Subklinische Hyper- und Hypothyreose und kardiovaskuläre Morbidität - Kantonsspital St.Gallen
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Subklinische Hyper- und Hypothyreose
und kardiovaskuläre Morbidität
Peter Kopp, MD
Médecin chef
Service d’endocrinologie, diabétologie et métabolisme
Centre hospitalier universitaire Vaudois
peter.kopp@chuv.ch
Editor-in-Chief Emeritus, Thyroid
President Elect, American Thyroid Association
Faculté de biologie et de médecine
The content of this talk is protected by copyright by the presenter. Copying, sharing, or reuse without authorization are not permitted.
Bisschop PH, van Trotsenburg A. N Engl J Med 370:1237-1237, 2014.
Das Myxödemherz
Vor Behandlung 4 Wochen 8 Wochen
Thyreoiodin Thyreoiodin
• Zondek H. Das Myxödemherz. Münch Med Wochenschr 43:1180–1182, 1918
• Kopp P. Das Myxödemherz: The Myxedema Heart. Herman Zondek 1887–1979. Thyroid 28: 1079-1080, 2018
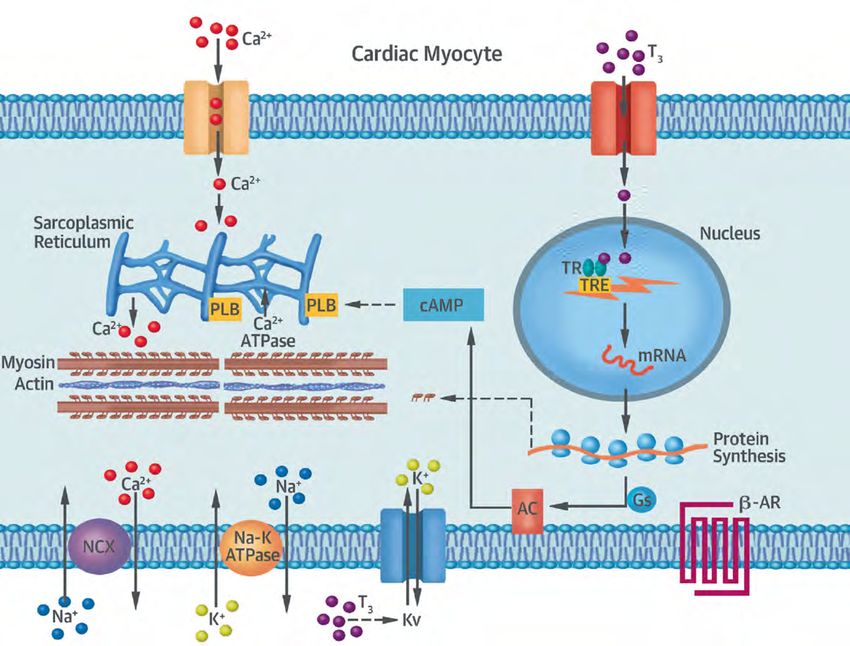
Thyroid Hormone Action in the Heart
TR-independent TH signaling
avβ3
T3
T3
TR
PI3K
p85α
T3
S T4
Akt/PKB 1
S
TR-dependent P P
2
signaling of TH
without Type 3
DNA binding
Type 4
p85
P I3
α
K
ER
K 1/
2
Thyroid Hormone Action in the Heart Razvi S et al. J Am Coll Cardiol 71:1781-1796, 2018
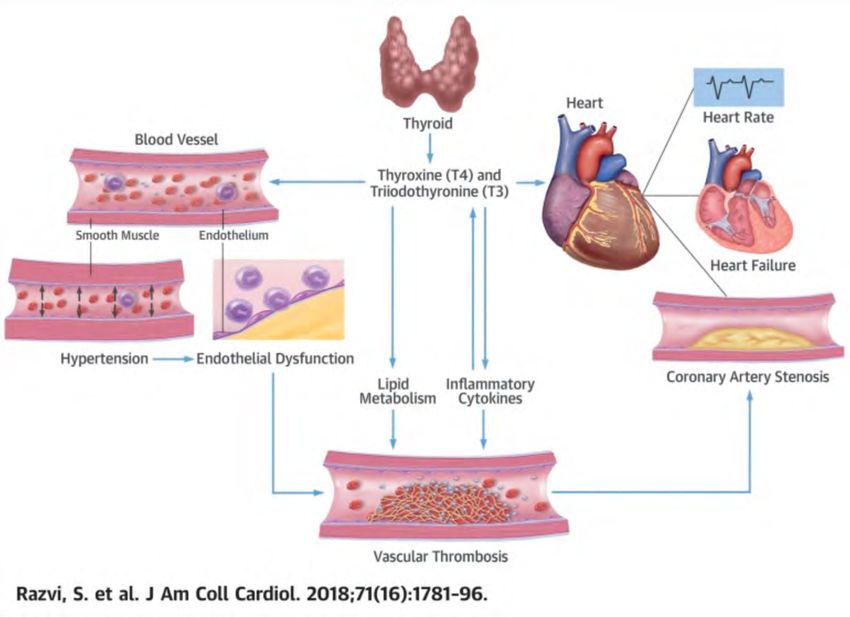
Thyroid Hormones and Cardiovascular
Function and Diseases
Razvi S et al. J Am Coll Cardiol 71:1781-1796, 2018
What is a normal TSH?

Normal TSH Frequency Using Different Methods
25 18
Behring 16 DPC
20 14
12
15
10
Frequency
8
10
6
5 4
2
0 0
0.3 0 1.0 2.0 4.0 0.3 1.0 2.0 4.0
35 40
30 Corning 35 Ortho
25 30
25
20
Frequency 20
15
15
10 10
5 5
0 0
0.3 1.0 2.0 4.0 0.3 1.0 2.0 4.0
TSH mU/L
Spencer C. NACB Guidelines 2002.
TSH Distribution in NHANES III
50
45
Black non-Hispanic
40 Mexican American
35
White non-Hispanic
30
Percent
25
20
15
10
5
0
0.1 to 0.2 0.21 to 0.3 0.31 to 0.5 0.51 to 1 1.1 to 2 2.1 to 3 3.1 to 5.0 5.1 to 10 10 to 20 20 to 50
Serum TSH (mU/L)
Note: Intervals on horizontal axis are not equal
Mean 1.4 mU/l
2.5 = 97.5th %ile
Modified after:
Hollowell, J. G. et al. J Clin Endocrinol Metab 2002;87:489-499
0.45-4.12 mU/lAge-Specific Distribution of Serum Thyrotropin and
Antithyroid Antibodies in the U.S. Population: Implications
for the Prevalence of Subclinical Hypothyroidism
97.5% iles
Surks MI and Joseph G. Hollowell JG. J Clin Endocrinol Metab 92: 4575–4582, 2007Age-Related Changes in Thyroid Function: A Longitudinal
Study of a Community-Based Cohort
• Longitudinal changes in thyroid function in 781 participants.
• Mean serum TSH increased from 1.49 to 1.81 mU/liter, a change
in mean TSH (DTSH) of 0.32 mU/liter
• [95% confidence interval (CI) 0.27, 0.38,PPrevalence of Thyroid Dysfunction
Canaris GJ. Arch Intern Med 160: 526, 2000
Total subjects 25,862
Euthyroid 22,842 (88.3%)
Hypothyroid 114 (0.4%)
Subclinical hypothyroid 2336 (9.0%)
Hyperthyroid 35 (0.1%)
Subclinical hyperthyroid 535 (2.1%)
Among patients not taking thyroid medication
8.9% elevated TSH
1% decreased TSH
9.9% unrecognized thyroid disorderPrevalence of Thyroid Dysfunction
Male
24
Female
Elevated TSH Level, % of Subjects
22
20
18
16
14
12
10
8
6
4
2
0
18-24 15-34 35-44 45-54 55-64 65-74 >74
Age years
Canaris GJ. Arch Intern Med 160: 526, 2000Subclinical Hyperthyroidism
Subclinical Hyperthyroidism:
Definition
q Suppressed TSH, with normal FT4 and T3
• Mild: TSH 0.1 – 0.39 mU/L (Grade 1)
• Severe: TSHSubclinical Hyperthyroidism and the Heart
Increase in:
Mean heart rate
Risk of atrial fibrillation
LV mass index
Heart failure
Cardiovascular mortalityAssociation Between Serum Free Thyroxine Concentration and Atrial Fibrillation Gammage MD et al. Arch Intern Med167:928-934, 2007
Thyroid status, cardiovascular risk, and
mortality in older adults
q Cardiovascular Health Study, a large, prospective cohort study.
q 3233 US community-dwelling individuals aged 65 years or older
Atrial Fibrillation
All subjects with subclinical hyperthyroidism
HR 1.98; (95% CI, 1.29-3.03)
Cappola AR et al. JAMA 295:1033-1041, 2006The Thyroid Studies Collaboration: Subclinical hyperthyroidism and incident atrial fibrillation q Individual data on 52,674 participants were pooled from 10 cohorts. q Incident AF was analyzed in 8711 participants from 5 cohorts. q In age-and sex-adjusted analyses, subclinical hyperthyroidism was associated with increased risk of AF (HR, 1.68; 95% CI, 1.16–2.43). Collett TH et al. Arch Intern Med 28: 799-809, 2012
The Thyroid Studies Collaboration:
Heart Failure Events According to TSH Levels
q 25,390 participants with 216,248 person-years of follow-up
q 648 had subclinical hyperthyroidism (2.6%)
q 2068 had subclinical hypothyroidism (8.1%)
Gencer B et al. Circulation 126:1040-1049, 2012The Thyroid Studies Collaboration:
Subclinical hyperthyroidism and CHD events
q Individual data on 52,674 participants were pooled from 10 cohorts.
q Coronary heart disease events were analyzed in 22,437 participants from 6
cohorts with available data.
q In age-and sex-adjusted analyses, subclinical hyperthyroidism was associated
with increased risk of CHD events (HR, 1.21; 95% CI, 0.99–1.46).
Collett TH et al. Arch Intern Med 28: 799-809, 2012The Thyroid Studies Collaboration:
Subclinical hyperthyroidism and CHD mortality
q Individual data on 52,674 participants were pooled from 10 cohorts.
q Coronary heart disease events were analyzed in 52,633 participants from 10
cohorts with available data.
q In age-and sex-adjusted analyses, subclinical hyperthyroidism was associated
with increased risk of CHD mortality (HR, 1.29; 95% CI, 1.02–1.62).
Collett TH et al. Arch Intern Med 28: 799-809, 2012Conclusion
Subclinical hyperthyroidism is associated with
increased risks of:
q Total mortality
q CHD mortality
q CHD events
q Incident AF
q The highest risks of CHD mortality and AF occur
with TSH levels below 0.10 mIU/L.Treatment of Subclinical Hyperthyroidism
ATA and ETA Guidelines
Serum TSH ( mU/L)
age 65 yrs)
disease,
osteoporosis)
Probably treat if
Younger symptomatic or with No indication to treat
comorbidities
• Ross DS et al. Thyroid 26:1343-1421, 2016
• Biondi B et al. Eur Thyroid J 4:149-163, 2015Subclinical Hyperthyroidism:
Important Clinical Points
q Over-replacement with thyroid hormone is the most
common cause of subclinical hyperthyroidism.
q In particular older patients with subclinical
hyperthyroidism have an increased risk of CV death,
atrial fibrillation and CHF.
q Treatment of subclinical hyperthyroidism is warranted if
the TSH isSubclinical Hypothyroidism
Patient S.H., , 79 o A 79 year old woman has mild fatigue. She also complains of depression. o The physical exam is normal, but her BP is 135/93 mmHg. Her thyroid is not enlarged. o A serum TSH is obtained and is 7.9 mU/l (0.4-4.0). The FT4 is 0.9 ng/dl (0.7-1.5). o Her LDL cholesterol is 157 mg/dl (4.26 mmo/L). o The Anti-TPO antibodies are negative. o To treat or not to treat?
Etiology and Presentation q The most common cause of SCH is chronic autoimmune thyroiditis associated with antithyroid peroxidase antibodies (Hashimoto’s thyroiditis). q Individuals with SCH are often asymptomatic, but clinical manifestations can include non-specific complaints or symptoms similar to those seen in overt hypothyroidism, such as fatigue, weakness, weight gain, cold intolerance, and constipation. Biondi B, Cooper DS. The clinical significance of subclinical thyroid dysfunction. Endocr Rev 29: 76-131, 2008
Progression to Overt Hypothyroidism q Individuals with subclinical hypothyroidism are at risk for progression to overt thyroid dysfunction with an average yearly progression rate of 2% to 6%. q The risk is increased in females, individuals with higher levels of TSH, and in the presence of antithyroid peroxidase antibodies. q Those without antithyroid peroxidase antibodies have also a higher risk of progression. Vanderpump MP et al. The incidence of thyroid disorders in the community: a twenty-year follow-up of the Whickham Survey. Clin Endocrinol 43: 55-68, 1995.
Progression to Overt Hypothyroidism
TPOAb Elevation
Activation of
autoimmune
process TSH Elevation
Subclinical
Hypothyroidism
Environmental
Factors Low FT4
Overt
Hypothyroidism
Genetic
Predisposition
5% per year
AgeSpontaneous TSH Normalization q In contrast, TSH levels normalize in 15% to 65% of those with a single elevated TSH without treatment, over follow-up periods going from 1 to 6 years. q The likelihood of spontaneous recovery is higher with TSH levels
Overt Hypothyroidism and CVD
Overt
Hypothyroidism
Atherogenic Hypercoagulable Abnormal Impaired
lipid profile state Hemodynamics endothelial Abnormal
Enddiastolic function nontraditional
dysfunction risk factors:
Lp(a), CRP,
homocysteine,
LDL particle sizeOvert Hypothyroidism and CVD Razvi S et al. J Am Coll Cardiol 71:1781-1796, 2018
Subclinical Hypothyroidism and CVD
Subclinical
Hypothyroidism
Atherogenic Hypercoagulable Abnormal Impaired
lipid profile state Hemodynamics endothelial Abnormal
Enddiastolic function nontraditional
dysfunction risk factors:
Lp(a), CRP,
homocysteine,
LDL particle sizeCardiovascular Risk and Heart Failure
q SCH can lead to impaired systolic and diastolic cardiac
function, and vascular dysfunction with increased
vascular stiffness and endothelial dysfunction.
• Monzani F et al. Effect of levothyroxine on cardiac function and structure in
subclinical hypothyroidism: a double blind, placebo-controlled study. J Clin
Endocrinol Metab. 86: 1110-1115, 2001.
• Razvi S et al. The beneficial effect of L-thyroxine on cardiovascular risk factors,
endothelial function, and quality of life in subclinical hypothyroidism:
randomized, crossover trial. J Clin Endocrinol Metab. 92: 1715-1723, 2007.The Epidemiology of CVD in Subclinical
HypothyroidismIncident CVD in Subclinical Hypothyroidism
Effect of SH on
Prospective Studies Comment
Incident CHD
Hak et al. 2000
No Mean age 69
Rotterdam study
Imaizumi et al. 2004
Yes Mean age 58; men only
Atomic Bomb Survivors
Gussekloo et al. 2004
No Age >85
Leiden Plus Study
Walsh et al. 2005
Yes Mean age 50
Busselton study
Rodondi et al. 2005
No Mean age 75; increased risk of CHF
Health Aging Study
Asvold et al. 2012 Increased mortality in women only;
Yes
The HUNT study mean age 54
Hyland et al. 2012
No Age >65
Cardiovascular Health Study
Tseng et al. 2012 Increased CV and all cause mortality;
Yes
Taiwan Study age 40s
LeGrys et al. 2013
No No increased with TSH >7
WHIIncident CVD in Subclinical Hypothyroidism
Effect of SH on
Prospective Studies Comment
Incident CHD
Hak et al. 2000
No Mean age 69
Rotterdam study
Imaizumi et al. 2004
Yes Mean age 58; men only
Atomic Bomb Survivors
Gussekloo et al. 2004
No Age >85
Leiden Plus Study
Walsh et al. 2005
Yes Mean age 50
Busselton study
Rodondi et al. 2005
No Mean age 75; increased risk of CHF
Health Aging Study
Asvold et al. 2012 Increased mortality in women only;
Yes
The HUNT study mean age 54
Hyland et al. 2012
No Age >65
Cardiovascular Health Study
Tseng et al. 2012 Increased CV and all cause mortality;
Yes
Taiwan Study age 40s
LeGrys et al. 2013
No No increased with TSH >7
WHIIncident CVD in Subclinical Hypothyroidism
Effect of SH on
Prospective Studies Comment
Incident CHD
Hak et al. 2000
No Mean age 69
Rotterdam study
Imaizumi et al. 2004
Yes Mean age 58; men only
Atomic Bomb Survivors
Gussekloo et al. 2004
No Age >85
Leiden Plus Study
Walsh et al. 2005
Yes Mean age 50
Busselton study
Rodondi et al. 2005
No Mean age 75; increased risk of CHF
Health Aging Study
Asvold et al. 2012 Increased mortality in women only;
Yes
The HUNT study mean age 54
Hyland et al. 2012
No Age >65
Cardiovascular Health Study
Tseng et al. 2012 Increased CV and all cause mortality;
Yes
Taiwan Study age 40s
LeGrys et al. 2013
No No increased with TSH >7
WHIThe Thyroid Studies Collaboration:
Heart Failure Events According to TSH Levels
q 25,390 participants with 216,248 person-years of follow-up
q 648 had subclinical hyperthyroidism (2.6%)
q 2068 had subclinical hypothyroidism (8.1%)
Gencer B et al. Circulation 126:1040-1049, 2012The Thyroid Studies Collaboration:
SCH and the risk of coronary heart disease and mortality
q SCH has been associated with an increased risk of fatal
and non-fatal coronary heart disease (CHD) events.
q Analysis of 55,000 subjects showed an age and sex-
adjusted HR of 1.89 (95% CI 1.28–2.80) for CHD events
in persons with TSH levels above 10 mIU/l.
q CHD mortality showed a HR of 1.58 (95% CI 1.10–2.27).
q Risks were not increased for participants with TSH
levelsThe Thyroid Studies Collaboration:
SCH and the risk of coronary heart disease and mortality
• Rodondi N et al. Subclinical hypothyroidism and the risk of coronary heart
disease and mortality. JAMA 304: 1365-1374, 2010Cardiovascular Risk and Heart Failure
q The Leiden 85+ Study showed a reduced risk of
cardiovascular and overall mortality in subclinically
hypothyroid individuals aged 85 years (1).
• Gussekloo J et al. Thyroid status, disability and cognitive function, and survival
in old age. JAMA 292: 2591-2599, 2004.Cardiovascular Risk and Heart Failure: Intervention q In a small RCT, normalization of TSH levels by thyroxine replacement therapy led to an improvement in cardiac function (1). q Retrospective administrative data suggest that thyroxine treatment leads to a reduction in ischemic heart disease in younger individuals, but not in persons aged 70 years or older (2). 1. Monzani F et al. Effect of levothyroxine on cardiac function and structure in subclinical hypothyroidism: a double blind, placebo-controlled study. J Clin Endocrinol Metab. 86: 1110-1115, 2001. 2. Razvi S et al. Levothyroxine treatment of subclinical hypothyroidism, fatal and nonfatal cardiovascular events, and mortality. Arch Intern Med 172: 811-817, 2012.
Mortality and Longevity
SCH:hypothyroidism:
Subclinical Mortality and Longevity
mortality
q Grossman et al.: 1956 subjects > 65 years with SCH:
SCH (HR, 1.75; confidence interval [CI], 1.63-1.88) was
associated with significantly increased mortality
(univariate and multivariate analyses). TSH ≥6.38 mIU/L
was associated with the highest mortality after
multivariate adjustment (HR, 1.708; CI, 1.38-2.12).
q Kovar et al: 3934 subjects with SCH (868 male, 3066
females, median age 48 years). Multivariate Cox
regression model adjusted for age and sex: TSH levels
associated with dose-dependent all-cause mortality.
• Grossman A et al. Subclinical Thyroid Disease and Mortality in the Elderly: A
Retrospective Cohort Study. Am J Med 129: 423-430, 2016.
• Kovar FM et al. Subclinical hypothyroidism and mortality in a large Austrian
cohort: a possible impact on treatment? Wien Klin Wochenschr 127: 924-930,
2015.SCH: Mortality and Longevity
q Leiden 85-Plus Study: 599 participants were followed up
from age 85 years through age 89 years. The hazard
ratio for mortality per SD increase of 2.71 mIU/L of
thyrotropin was 0.77 (95% confidence interval [CI], 0.63-
0.94; P = .009). Elderly individuals with abnormally high
TSH levels may have a prolonged life span.
q Atzmon et al.: Ashkenazi Jews with exceptional
longevity (centenarians; median age, 98 yr) compared
to two control groups. TSH was significantly higher in
centenarians [1.97 (0.42-7.15) mIU/liter].
• Gussekloo J et al. Thyroid status, disability and cognitive function, and survival in
old age. JAMA 292: 2591-2599, 2004.
• Atzmon G et al. Extreme longevity is associated with increased serum thyrotropin.
J Clin Endocrinol Metab 94: 1251-1254, 2009.
• Atzmon G et al. Genetic predisposition to elevated serum thyrotropin is
associated with exceptional longevity. J Clin Endocrinol Metab 94: 4768-4775,
2009.Cardiovascular Disease Risk and Age in SCH
+
Risk
50 60 70 80 90 years
-
Modified from: Biondi B, Cooper DS. Endocr Rev 29:76-131, 2008To Treat or Not to Treat?
Treat Don’t
TreatThe Problem
q Despite the large prevalence of SCH, evidence on
screening and the benefits and risks of treatment
remain controversial.
• Villar HC et al. Thyroid hormone replacement for subclinical hypothyroidism. The
Cochrane database of systematic reviews. 2007(3):CD003419. Epub 07/20/2007
• Rugge B et al. Screening and treatment of subclinical hypothyroidism or
hyperthyroidism. Comparative Effectiveness Reviews, No.24. Rockville (MD):
Agency for Healthcare Research and Quality (US). 2011.
• Cooper DS, Biondi B. Subclinical thyroid disease. Lancet 379: 1142-1154, 2012.
• Rodondi N et al. Subclinical hypothyroidism and the risk of coronary heart
disease and mortality. JAMA 304: 1365-1374, 2010.
• Gencer B et al. Subclinical thyroid dysfunction and the risk of heart failure events:
an individual participant data analysis from 6 prospective cohorts. Circulation
126: 1040-1049, 2012.Recommendations for Treatment q Due to the paucity of large-scale RCTs examining relevant clinical outcomes, current screening and treatment recommendations are principally based on observational data, small clinical trials with short follow-up durations and expert opinions. q Screening recommendations vary widely across different medical societies and expert groups.
Recommendations for Treatment
q A Cochrane Systematic Review published in 2007
concluded that evidence suggests a beneficial effect of
thyroid hormone replacement on surrogate markers for
cardiovascular risk, such as improved serum
cholesterol levels and cardiac function, but the impact
on clinical outcomes could not be assessed given the
current data.
• Villar HC et al. Thyroid hormone replacement for subclinical hypothyroidism. The
Cochrane database of systematic reviews. 2007(3):CD003419. Epub 07/20/2007Subclinical Hypothyroidism in Older Adults
TRUST Trial
• Stott DJ et al. N Engl J Med 376: 2534-2544, 2017Subclinical Hypothyroidism in Older Adults
q Double-blind, randomized, placebo-controlled,
parallel-group trial involving 737 adults who were at
least 65 years of age (mean age 74.4 years, 53.7%
women.
q SCH (TSH 4.6 to 19.99 mU/l, normal FT4).
q 368 treated with levothyroxine, 369 patients on placebo.
q The two primary outcomes at 1 year were:
• Change in the Hypothyroid Symptoms score
• Tiredness Score on a thyroid-related quality-of-life
questionnaire
• Stott DJ et al. N Engl J Med 376: 2534-2544, 2017Subclinical Hypothyroidism in Older Adults q No differences in the mean change at 1 year in the Hypothyroid Symptoms score. q No beneficial effects of levothyroxine were seen on secondary-outcome measures. q Conclusion: LT4 provided no apparent benefits in older persons with SCH. • Stott DJ et al. N Engl J Med 376: 2534-2544, 2017
Subclinical Hypothyroidism in the Elderly Numerous open questions/critiques: q Small number of patients, limited follow-up q Underpowered: statements on secondary endpoints (cardiovascular, bone) not conclusive, q No FT4 levels on treatment. q Overall modest decrease in TSH. q No lipid levels reported. • Stott DJ et al. N Engl J Med 376: 2534-2544, 2017
Recommendations for Treatment
q Most experts and societies suggest treatment of
subclinical hypothyroidism if TSH levels are >10 mIU/l
based on the available evidence.
q For persons with moderately elevated TSH
concentrations between 4.5–10 mIU/l, treatment remains
controversial. There is consensus that TSH levels
should be monitored every 6 to 12 months.
• Pearce SHS et al. ETA Guideline: Management of sublinical hypothyroidism. Eur
Thyroid J 2: 215-228, 2013.
• Jonklaas J et al. Guidelines for the treatment of Hypothyroidism. Thyroid 23:
1670-1751, 2014.
• Lazarus et al. 2014 European Thyroid Association guidelines for the management
of subclinical hypothyroidism in pregnancy and in children. Eur Thyroid J 3: 76-
94, 2014.Recommendations for Treatment Biondi B, Cooper DS. The clinical significance of subclinical thyroid dysfunction. Endocr Rev 29: 76-131, 2008
Levothyroxine Treatment of Subclinical Hypothyroidism,
Fatal and Nonfatal Cardiovascular Events, and Mortality
Patients with Subclinical Hypothyroidism Patients with Subclinical Hypothyroidism
(TSH 5-10 mU/l) Aged 40-70 (TSH 5-10 mU/l) Aged >70
Ischemic heart disease events Ischemic heart disease events
Treatment of SCH with LT4 was associated with fewer IHD events in
younger individuals, but this was not evident in older people.
• Razvi S et al. Arch Intern Med 172:811-817, 2012Subclinical thyroid disease
Minor biochemical
abnormality?
Potential hidden
impact on quality of life
and survival?Faculté de biologie et de médecine
You can also read