Tamiflu and transparency - Some general thoughts on data access and decision making Mike Clarke
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Tamiflu and transparency
Some general thoughts on data
access and decision making
January 28 2010
Mike Clarke
UK Cochrane Centre
School of Nursing and Midwifery,
Trinity College Dublin
“Oseltamivir 150 mg daily is effective in preventing lower respiratory tract complications in influenza cases (OR 0.32, 95% CI 0.18 to 0.57), especially bronchitis (OR 0.40, 95% CI 0.21 to 0.76) and pneumonia (OR 0.15, 95% CI 0.03 to 0.69), but not in ILI cases (OR 0.21, 95% CI 0.02 to 2.04). Both NIs are effective in preventing complications of all types in the intention-to-treat (ITT) population (OR 0.49, 95% CI 0.38 to 0.62), although these observations are based on single studies (Kaiser 2003; Makela 2000) the combined denominator is fairly substantial (2991).”

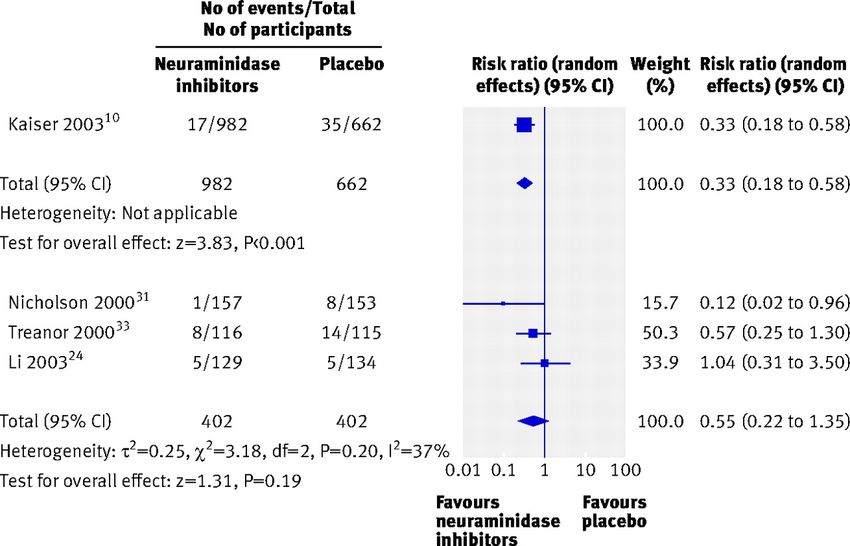
Oseltamivir did not reduce influenza lower respiratory tract complications (risk ratio 0.55, 95% CI 0.22 to 1.35),
“Data on the effectiveness of oseltamivir against the complications of influenza are confusing…. The remaining published evidence is insufficient to answer the question about the effectiveness of either neuraminidase inhibitor on reducing the complications of lower respiratory tract infection, antibiotic use, or admissions to hospital.”
The Background April 2009 Reports of Mexican or swine flu (H1N1) June 2009 WHO declares pandemic July/August 2009 NIHR commission a series of research studies, including the updating of relevant Cochrane reviews Billions of Euros spent on Tamiflu
Tamiflu and influenza symptoms Neuraminidase inhibitors have modest effectiveness. They shorten the duration of symptoms by one to day days, when taken within 48 hours of onset.
Tamiflu and complications: certainty
• Roche [roche.com] (2005): "Tamiflu delivers ... [a] 67% reduction in
secondary complications such as bronchitis, pneumonia and sinusitis in
otherwise healthy individuals"
• Kaiser et al (2003): "Our analysis found that early treatment of influenza
illness with the neuraminidase inhibitor oseltamivir significantly reduced
influenza-related LRTCs, associated antibiotic use, and the risk of
hospitalization. This effect was observed in both at-risk subjects and
otherwise healthy individuals."
• EU EMEA (2009): "The proportion of subjects who developed specified
lower respiratory tract complications (mainly bronchitis) treated with
antibiotics was reduced from 12.7% (135/1063) in the placebo group to
8.6% (116/1350) in the oseltamivir treated population (p = 0.0012)."
• US CDC (2008): "In a study that combined data from 10 clinical trials, the
risk for pneumonia among those participants with laboratory-confirmed
influenza receiving oseltamivir was approximately 50% lower than among
those persons receiving a placebo and 34% lower among patients at risk for
complications (pTamiflu and complications: uncertainty
• Roche [tamiflu.com] (2009): "Treatment with TAMIFLU has not been proven
to have a positive impact on [asthma, emphysema, other chronic lower
respiratory diseases, pneumonia, other respiratory diseases, pneumonitis,
and influenza-related death].”
• US FDA (2008): "Serious bacterial infections may begin with influenza-like
symptoms or may coexist with or occur as complications during the course
of influenza. TAMIFLU has not been shown to prevent such complications."
• Burch et al (2009): "Overall, little information was available on the effects of
either drug on the incidence of complications, and there were very few
events, in both the healthy adult and at-risk populations. Furthermore,
weaknesses in the available evidence limit the reliability and the ability to
generalise any results relating to the effect of these drugs on the rates of
complications."
• Canadian Coordinating Office for Health Technology Assessment (2002):
"There is insufficient evidence to show that oseltamivir reduces
complications, hospitalizations or death when used to treat: normally
healthy people suspected of having influenza, or; those who are at risk for
developing complications."What would you do?
Updating the Cochrane review Feedback from Keiji Hayashi (July 14 2009) The complications data in the Cochrane review were from a single peer-reviewed study by Kaiser et al, which had meta-analysed ten manufacturer funded trials from the late 1990s. Two of these were published in peer reviewed journals. Eight were apparently either unpublished or published only in abstract form. Plan by the Cochrane authors Try to verify the data on all ten trials and to do their own meta-analysis.
What would you do?
Timeline August 2009 Lead author, Tom Jefferson, wrote to the authors of Kaiser et al, but was told that they no longer had the files and to contact Roche. He also wrote to authors of the two published trials. One responded, directing him to the manufacturer. September 2009 Tom asks Roche for data.
Timeline October 2 2009 Roche indicated a willingness to share data, but sent Tom a "confidentiality agreement," containing a clause saying that he agrees "not to disclose ... the existence and terms of this Agreement“. October 3 2009 Tom doesn’t sign but asks for clarification. October 7 2009 Roche ask Tom to restate which data he was seeking. He does. Roche replies that it is unable to provide data because it had already provided it for a similar meta-analysis being started by an independent expert influenza group. They say that the Cochrane request might conflict with that review.
Timeline October 13 2009 Tom asked Roche to outline its concerns and explain why sending data to multiple groups of independent researchers should pose a problem. Roche did not answer these questions. October 21 2009 Roche emailed Tom excerpts of company reports from all clinical trials used by Kaiser et al. Jefferson wrote to Roche explaining that the files were insufficient to verify the effects on complications claims in Kaiser et al and the methods used in the trials. October 28 2009 Roche said it would send more information the following week. Tom told them that the deadline was now past, but that the Cochrane reviewers would accept any additional information for future updates.
What would you do?
Fig 6 Effect of oseltamivir compared with placebo on complications (including pneumonia,
bronchitis, or "other lower respiratory tract infections") requiring antibiotics in laboratory
confirmed influenza, based on study by Kaiser et al and three other studies (complications
included pneumonia, bronchitis, otitis media, and sinusitis). Unpublished studies were
excluded
Jefferson, T. et al. BMJ 2009;339:b5106
Copyright ©2009 BMJ Publishing Group Ltd.What would you do?
Implications Independent trials The only trials were done or sponsored by the manufacturer. Unpublished trials Most of the trials had not been published in full Access to raw data Some of the authors had not seen the data. None of the lead authors seemed able to provide it, or new analyses.
Trust • Much of the evidence on drug safety and effectiveness is taken on trust. • Governments and international bodies have relied heavily on Kaiser et al and on observational studies to justify the stockpiling and widespread use of oseltamivir. • They probably assumed that others had looked critically and comprehensively at the complete dataset. Those others might include drug regulators and health technology assessors such as NICE, as well as journal editors and Cochrane reviewers. • Unfortunately, that might not be the case.
Conclusion The current system isn’t working. Worse than that, it gives a false sense of security. The system’s failures have left a legacy of drug evaluations for which, in the absence of better information, we must assume the same levels of confusion and uncertainty as for oseltamivir. The drug industry directly or indirectly undertakes the majority of all drug evaluations, so most of the evidence used to support drug policy and treatment remains shrouded in secrecy. In only a minority of cases will the data have been subject to full independent analysis and interpretation. In many if not most cases, the only people who have seen the entire dataset are company employees.
What needs to be done?
• We need more publicly funded trials and the drug industry should
fund independent trials for licensing their drugs.
• Governments should enact relevant laws.
• Researchers who said in their protocols that they would do certain
analyses should be required to do them or explain why they have
not done so, and to make the results available.
• Authors should state who saw the full primary dataset and who saw
only summary data, who decided what analyses to do and report,
and who is the "custodian" for the data. The custodian should be
able and willing to show the full dataset to systematic reviewers and
other researchers.
• Journals should consider adopting a policy of independent statistical
review and should push for independent, individual patient data
meta-analyses wherever possible, especially for drugs to be used in
common conditions and purchased in large quantities to protect the
public’s health.What would you do?
You can also read