The Cost-effectiveness of Subcutaneous Semaglutide 2.4 mg Injection for Chronic Weight Management in Canada: A Societal Perspective
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
The Cost-effectiveness of Subcutaneous Semaglutide 2.4 mg Injection for
Chronic Weight Management in Canada: A Societal Perspective
Anamaria-Vera Olivieri
IQVIA
Sergey Muratov
IQVIA
Sara Larsen
Maria Luckevich ( mlvh@novonordisk.com )
Novo Nordisk Canada Inc.
Katalina Chan
Novo Nordisk Canada Inc.
Mark Lamotte
IQVIA
David Lau
University of Calgary
Article
Keywords: Canada, Core Obesity Model, Cost-effectiveness, Obesity, Semaglutide 2.4 mg
Posted Date: October 11th, 2022
DOI: https://doi.org/10.21203/rs.3.rs-2135939/v1
License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License
Page 1/14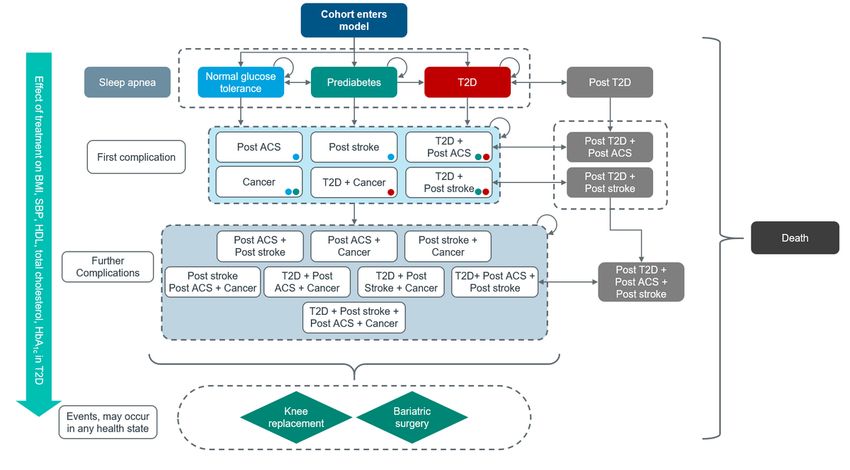
Abstract
OBJECTIVES: This study assessed the cost-effectiveness of once-weekly semaglutide 2.4mg injection as adjunct to reduced-calorie meals and
increased physical activity (diet and exercise, D&E), in adult patients with obesity (body mass index [BMI] of ≥30 kg/m2) or overweight (BMI 27-30
kg/m2) in the presence of ≥1 weight-related comorbidity, by comparing it with D&E alone or D&E in combination with liraglutide 3.0mg, orlistat, or
naltrexone 32mg/bupropion (NB32).
METHODS: The safety and efficacy of semaglutide 2.4mg and D&E were sourced from the STEP 1 and STEP 2 trials, while a network meta-analysis
informed the relative efficacy vs. other comparators. The Core Obesity Model was used to extrapolate costs and health outcomes (both discounted at
1.5% annually) over 40 years for a cohort with starting age 50 years and starting BMI 37.5 kg/m2, taking D&E alone or in combination with other
pharmacotherapies for 1 year. Costs were analyzed from a societal perspective, including publicly and privately funded health expenses, patient co-
payments, and indirect costs.
RESULTS: Semaglutide 2.4mg reduced weight and reverted prediabetes prevalence more than alternative therapies. This translated into delays in the
occurrence of weight-related complications, and gains in life-expectancy between 0.081 years vs. D&E (maximum gain) and 0.030 years vs. liraglutide
3.0mg (minimum gain), and quality-adjusted life-years (QALYs) between 0.103 vs. D&E and 0.039 vs. liraglutide 3.0mg, at additional costs. The
incremental cost-utility ratios were 29,677 Canadian dollars (CAD)/QALY gained vs. D&E, CAD12,369/QALY gained vs. liraglutide 3.0mg,
CAD25,663/QALY gained vs. orlistat and CAD25,003/QALY gained vs. NB32. The cost-effectiveness acceptability curve showed a high likelihood of
subcutaneous semaglutide 2.4 mg injection being considered cost-effective, at willingness-to-pay thresholds of CAD50,000/QALY and beyond.
CONCLUSION: Based on this analysis, the use of semaglutide 2.4mg injection can be considered a cost-effective alternative compared with D&E alone,
or D&E in combination with other pharmacotherapies.
Introduction
Obesity is classified as a body mass index (BMI) of 30 kg/m² or above for White, Hispanic, and Black individuals and > 25 kg/m² in Asian populations,
according to the World Health Organization (WHO) [1]. Many international organizations including Obesity Canada, Canadian Medical Association,
American Medical Association, World Obesity Federation and WHO view obesity as a complex chronic disease mediated by genetic, physiological,
environmental, and psychological factors [2–5]. According to the WHO (2016), nearly 2 billion adults are overweight and 650 million are obese [6].
Canadian data shows that 26.8% adults (7.3 million adults) are categorized as having obesity and another 36.3% adults (9.9 million adults) as
overweight [7]. Obesity increases the risk of type 2 diabetes (T2D) [7], hypertension, stroke, dyslipidemia, osteoarthritis, and certain cancers [8]. Indeed,
63.1% of Canadian adults are at increased risk of complications due to excess weight [7].
Obesity increases the economic burden on the individuals affected, their caregivers, healthcare system, and society. The Canadian Community Health
Survey, the National Population Health Survey, and the Economic Burden of Illness in Canada estimated that the total annual economic burden of
obesity in Canada increased by $735 million, from $3.9 to $4.6 billion between 2000–2008 [9]. The annual direct healthcare cost of obesity (including
physician, hospitalization, and medication costs) has been projected to reach 9 billion by 2021 [4].
Personalized care plans should be offered to adults with obesity to address root causes of obesity and provide a proactive health management through
medical nutrition therapy, exercise therapy, and psychological and behavior interventions [10]. However, when these are not sufficient, pharmacological
interventions for chronic weight management should be offered. Addition of pharmacological interventions may enhance adherence to behavioral
changes, improve physical functioning, and alleviate comorbidities [10]. There are currently three pharmacological agents approved for chronic obesity
management by Health Canada, all of which are being recommended for use in addition to medical nutrition and exercise therapy, i.e., diet and exercise
(D&E): liraglutide 3.0 mg (Saxenda®), naltrexone 32 mg/bupropion (NB-32) in a combination (Contrave®), and orlistat (Xenical®) [11–13]. Bariatric
surgery is considered an effective treatment for obesity. However, it is only reserved for individuals with BMI ≥ 40 kg/m2 or BMI ≥ 35 kg/m2 with
obesity-related diseases, such as T2D or hypertension [14].
Subcutaneous semaglutide 2.4 mg injection (Wegovy®) is a long-acting glucagon-like peptide-1 (GLP-1) receptor agonist approved for the treatment of
obesity in Canada [15]. Approximately 5 000 patients were enrolled in the phase 3a Semaglutide Treatment Effect in People with obesity (STEP)
program [16]. Additionally, 17 500 patients were enrolled in a cardiovascular (CV) outcomes trial, the Semaglutide Effects on Heart Disease and Stroke
in Patients With Overweight or Obesity (SELECT, NCT03574597) completion of which is expected in September 2023 [17]. Across the seven completed
STEP trials, participants were randomly assigned to receive subcutaneous semaglutide 2.4 mg injection once-weekly (as well as semaglutide 1.7 mg in
STEP 6 and semaglutide 1.0 mg in STEP 2) in combination with D&E or placebo and D&E [16, 18–23]. STEP 8 additionally included participants on
once-daily subcutaneous liraglutide 3.0 mg [23]. Subcutaneous semaglutide 2.4 mg injection was noted to provide a significant reduction in weight in
all trials [18–23].
The aim of the current study was to assess the health economic value of subcutaneous semaglutide 2.4 mg injection as adjunct to a reduced calorie
diet and increased physical activity in the management of obesity in Canada, using results from STEP 1 and STEP 2, and a network meta-analysis
(NMA) and indirect comparison. Comparators were D&E alone (trial placebo), or in combination with pharmacological treatments currently approved by
Page 2/14
Health Canada: liraglutide 3.0 mg, orlistat, and NB-32. The cost-effectiveness analysis (CEA) was conducted using the COM, a validated model in
obesity [24, 25].
Methods
Perspective
The analysis was conducted from a societal perspective, including publicly and privately funded health expenses, patient co-payments, and indirect
costs, in line with the guidance provided by the Canadian Agency for Drugs and Technologies in Health and the Institut National d'excellence en Santé et
Services Sociaux [26, 27]. An annual discount rate of 1.5% was applied to both costs and health outcomes beyond the first year. All cost results were
reported in 2021 Canadian dollars (CAD).
Population. Adults with BMI ≥ 30 kg/m2 (obese) or 27–30 kg/m2 (overweight) and ≥ 1 weight-related co-existing condition, including T2D were
analyzed. Since no trial had investigated the efficacy and safety of subcutaneous semaglutide 2.4 mg injection in this population, a weighted average
approach was undertaken to derive baseline characteristics as well as treatment effects pertaining to two published subcutaneous semaglutide 2.4 mg
injection trials, STEP 1 [22] (in patients with normal glucose tolerance [NGT] and prediabetes) and STEP 2 [18] (in patients with T2D). Glycemic status
proportions were assigned to the cohort at baseline and were calculated to represent a real-life population in Canada expected to be eligible for
treatment with subcutaneous semaglutide 2.4 mg injection, assuming 26.0%, 46.4%, and 27.6% of Canadians living with obesity could have NGT,
prediabetes, and T2D, respectively, based on published estimates [7, 28–31].
Other baseline characteristics (e.g., age, gender, and cardiometabolic risk factors such as BMI, systolic blood pressure [SBP], lipids, and glycated
hemoglobin [HbA1c] level [for those with T2D]) by glycemic subgroup and weighted average are reported in Supplementary Table 1. The starting mean
age of the analyzed cohort was 50 years, and 67% were females. Mean starting BMI was 37.5 kg/m2. In cohort with T2D at baseline, the average
duration of diabetes was 8 years, and mean HbA1c was 8.1%.
Clinical efficacy and safety. Changes vs. baseline in BMI, proportion of patients with ≥ 5% weight loss (responders), SBP, glycemic status change for
subcutaneous semaglutide 2.4 mg injection and D&E (Table 1), total cholesterol, and high-density lipoprotein cholesterol (Supplementary Table 2) were
taken from the STEP 1 and STEP 2 trials as observed at weeks 28 and 68. For all base-case analyses, the treatment policy estimand (intention to treat,
ITT) was used. Relative efficacy for other available pharmacological treatments was informed via NMA. The NMA generated estimates of treatment
effects for subcutaneous semaglutide 2.4 mg injection relative to pharmacological comparators approved for weight management in adults with BMI
27–30 kg/m2 and ≥ 1 weight-related comorbidity or BMI ≥ 30 kg/m2 among subgroups: NGT, prediabetes, and T2D. A systematic literature review was
conducted to inform the development of a base-case evidence network of all relevant randomized control trials to the total populations (Supplementary
Fig. 1). The comprehensive networks were generated by considering outcome data reported at 52–68 weeks (overall 52 weeks maintenance treatment
across all studies after variable titration periods across trials).
Page 3/14Table 1
Percent changes in weight, systolic blood pressure and prediabetes reversal vs. baseline by glycemic status subgroup.
S.C. semaglutide 2.4 mg inj. FAS Diet & exercise Liraglutide 3.0 mg ER Orlistat NB-32 mg ER
FAS FAS
Mean SEM Mean SEM Mean SEM Mean SEM Mean SEM
Weight gain (%)
Subgroup: normal glucose tolerance at baseline
Cycle 2 & 3 -11.8 0.2 −2.6 0.3 −5.5 0.7 −2.0 1.2 −6.2 1.3
Cycle 4 −15.9 0.3 −2.4 0.5 −10.5 0.7 −6.1 1.2 −11.2 1.3
Scenarios: 2 and 3 years
Cycle 5 & 6 −15.9 0.3 −2.4 0.5 −10.5 0.7 −6.1 1.2 −11.2 1.3
Subgroup: prediabetes at baseline
Cycle 2 & 3 −10.4 0.2 −2.6 0.3 −9.2 0.8 −0.6 1.2 −4.8 1.3
Cycle 4 −13.7 0.4 −2.4 0.5 −13.0 0.8 −3.9 1.2 −8.7 1.3
Scenarios: 2- and 3-years
Cycle 5 & 6 −13.7 0.4 −2.4 0.5 −13.0 0.8 −3.9 1.2 −8.7 1.3
Subgroup: type 2 diabetes at baseline
Cycle 2 & 3 −8.4 0.2 −2.6 0.2 −8.9 3.6 −3.5 2.9 −8.0 3.2
Cycle 4 −9.6 0.3 −3.1 0.3 −10.5 3.6 −4.8 2.9 −9.5 3.2
Scenarios: 2- and 3-years
Cycle 5 & 6 −9.6 0.3 −3.1 0.3 −10.5 3.6 −4.8 2.9 −9.5 3.2
Systolic blood pressure increase (%)
Subgroup: normal glucose tolerance at baseline
Cycle 2 & 3 −5.5 0.4 −0.3 0.6 −3.1 1.0 −5.5 0.0 0.0 2.4
Cycle 4 −6.4 0.4 −0.8 0.6 −4.4 1.0 −6.4 0.0 −1.2 2.4
Scenarios: 2- and 3-years
Cycle 5 & 6 −6.4 0.4 −0.8 0.6 −4.4 1.0 −6.4 0.0 −1.2 2.4
Subgroup: prediabetes at baseline
Cycle 2 & 3 −5.0 0.5 −0.3 0.7 −4.5 1.0 −5.0 0.0 0.7 2.4
Cycle 4 −5.8 0.5 −1.2 0.7 −5.1 1.0 −5.8 0.0 0.2 2.4
Scenarios: 2- and 3-years
Cycle 5 & 6 −5.8 0.5 −1.2 0.7 −5.1 1.0 −5.8 0.0 0.2 2.4
Subgroup: type 2 diabetes at baseline
Cycle 2 & 3 −4.6 0.6 −0.1 0.6 −5.7 1.6 −2.9 1.6 −2.2 1.6
Cycle 4 −3.9 0.6 0.0 0.6 −4.7 1.6 −2.2 1.6 −1.3 1.6
Scenarios: 2- and 3-years
Cycle 5 & 6 −3.9 0.6 0.0 0.6 −4.7 1.6 −2.2 1.6 −1.3 1.6
Prediabetes reversal (%), applied in the prediabetes at baseline subgroup only
Cycle 2 84.1 1.5 47.8 3.1 85.5 2.5 74.5 7.4 80.3 6.3
Probability early response (weight change of 5% or more vs. baseline, all patients)
Note: values applied in the model base-case cost-effectiveness analyses are highlighted in bold; SBP is expressed as absolute mean change, mmHg.
ER early responder, FAS full analysis set, Inj. injection, NA not applicable, NGT normal glucose tolerance, S.C. subcutaneous, SEM standard error of
mean, T2D, type 2 diabetes.
Page 4/14S.C. semaglutide 2.4 mg inj. FAS Diet & exercise Liraglutide 3.0 mg ER Orlistat NB-32 mg ER
FAS FAS
Mean SEM Mean SEM Mean SEM Mean SEM Mean SEM
Cycle 2 NA NA NA NA 68.2 NA NA NA 46.9 NA
Note: values applied in the model base-case cost-effectiveness analyses are highlighted in bold; SBP is expressed as absolute mean change, mmHg.
ER early responder, FAS full analysis set, Inj. injection, NA not applicable, NGT normal glucose tolerance, S.C. subcutaneous, SEM standard error of
mean, T2D, type 2 diabetes.
In addition, for treatments where a response assessment is recommended per product label, liraglutide 3.0 mg and NB-32, the relative efficacy
substantiated via the NMA was anchored to subcutaneous semaglutide 2.4 mg injection efficacy observed in a subset of patients who achieved a
decrease in BMI of 5% or more at 3 months. This is further referred to as early responder efficacy. On average 68.2 and 46.9% of patients on liraglutide
3.0 mg and NB-32, respectively were early responders. Non-responders to liraglutide 3.0 mg and NB-32 were assigned the efficacy observed with D&E.
For all other treatments, including subcutaneous semaglutide 2.4 mg injection, the efficacy observed in the ITT full analysis set was applied.
Adverse events (AEs) associated with obesity treatments (such as nausea, vomiting, diarrhea, constipation etc.) were not included in base-case
analyses because of their transitory nature, i.e., they typically occur during up-titration of doses in the first weeks of treatment, and level-off afterwards.
In addition, rates of non-severe hypoglycemic events and severe hypoglycemic events with liraglutide 3.0 mg and subcutaneous semaglutide 2.4 mg
injection were low-to-very low [22, 32]. Nevertheless, an exploratory scenario analysis was conducted including severe gastrointestinal AEs for all
pharmacological treatments, and hypoglycemic events, non-severe and severe, for liraglutide 3.0 mg and subcutaneous semaglutide 2.4 mg injection.
Modeling approach
The CEA was conducted using version 16.0 of the Core Obesity Model (COM), a validated Markov state-transition model (Fig. 1) [24, 25]. The model was
designed to evaluate the costs and health outcomes of developing known obesity complications in function of risk factors such as BMI, lipids, SBP and
glycemic levels/status, and has fully been described elsewhere [24, 25]. Briefly, the occurrence of chronic and/or recurring, weight-related complications
such as T2D, sleep apnea, cardio- and cerebrovascular disease like myocardial infarction (MI), unstable angina (UI), stroke, and transient ischemic
attacks, certain cancers (post-menopausal endometrial, post-menopausal breast and colon cancers) and knee replacement surgery following
osteoarthritis are predicted over a maximum time horizon of 40 years (Fig. 1).
Using a closed cohort approach, the cumulative incidence of complications, rates of clinical events, costs, life-years (LYs) gained and quality-adjusted
LYs (QALYs) gained are calculated. The cohort is defined as a set of average baseline characteristics, reflective of the target population, to which mean
treatment effects are applied for the duration of treatment. Treatment effects are applied for the duration of treatment, and are lost gradually thereafter,
according to a catch-up rate. The model has undergone several validations, including two published external validations [24, 25].
Model inputs
Transition probabilities and risk equations. Detailed information on the risk equations and transition probabilities has been provided in earlier
publications [24, 25]. Here, a short summary of the sources for derivation of probabilities used in the current analyses is provided. To predict the
incidence of T2D in individuals with NGT and prediabetes, QDiabetes equation, was used [33]. QRisk3 equation was used to predict CV-events in
NGT/prediabetes and T2D [34]. Recurrent CV-events in both NGT/prediabetes and T2D were predicted using the Framingham Recurrent Coronary Heart
Disease [35]. An alternative model for predicting first and recurrent CV-events in patients with T2D is the United Kingdom Prospective Diabetes Study
(UKPDS)82, and this was used in a scenario analysis [36, 37].
Changes in weight determine the prevalence of sleep apnea in the model based on data from a multicenter cohort, the Sleep Heart Health Study [38].
The baseline incidence of colon cancer, and its association with BMI were sourced from the Body Mass and Colorectal Cancer Risk in the NIH-AARP
Study [39]. The incidence of post-menopausal breast cancer and post-menopausal endometrial cancer and their association with BMI were sourced
from systematic review and meta-analyses [40, 41]. The incidence of knee replacement was predicted based on a case-control study [42].
Extrapolation of treatment effects beyond trials. Post-treatment, a catch-up rate was applied over 2 cycles (33% and 67%) to bring the values of BMI,
SBP and lipids back to their baseline value in the third cycle post-treatment stop, (i.e., catch-up 100%). Beyond catch-up, weight was assumed to
increase naturally with 0.145 kg/m2 and 0.175 kg/m2 per cycle (year) in males and females, respectively [43], up to a maximum age of 68 years. SBP
and lipids were assumed not to change further beyond catch-up. A summary of key modeling assumptions and justifications is provided in
Supplementary Table 3.
Mortality. Obesity is linked with an increased risk of mortality, particularly from CV-diseases and cancer [44, 45]. Overall, obesity is estimated to increase
the CV-mortality rate 4-fold and the cancer-related mortality rate 2-fold. People with severe obesity have 6- to 12-fold increase in the all-cause mortality
rate [46]. In the analyses conducted, mortality was accounted by using general population, all-cause age and gender annual probabilities of death
sourced from Canadian life tables [47, 48]. Life tables were adjusted to exclude deaths due to obesity complications, using mortality by cause of death,
and subtracting those from the all-cause mortality. The result of this was a non-disease-specific mortality applied in the model (Supplementary Table 4).
The non-disease specific mortality was then adjusted with hazard ratio per unit increase in BMI from a large study on the UK Clinical Practice Research
Page 5/14Datalink (N = 3.6 million adults) [49], to account for the additional mortality associated with overweight and obesity. The approach was described in
detail by Lopes et al [50]. Finally, case fatality rates associated with fatal events in the model-MI, UA, stroke, and knee replacement were applied in the
cycle the event occurred as well as hazard ratios for higher mortality post-acute coronary syndrome (ACS), stroke, and diabetes seen in the general
population with these diseases (Supplementary Table 5).
Costs. A societal perspective on costs was taken, meaning costs were included independent of whether they were covered by public or private
insurances, or paid out-of-pocket by patients. Work productivity losses were also included in this analysis. The list price of subcutaneous semaglutide
2.4 mg injection was provided by Novo Nordisk. Other drug prices used in the analysis were sourced from the IQVIA Delta PA and are detailed in
Supplementary Table 6. Disease monitoring costs were assumed to consist of four annual visits and two annual blood checks and were applied to all
patients in the analyzed cohorts. The cost of D&E was estimated as an average of four programs recommended by Canada Obesity Management
clinical guidelines [10] (Supplementary Table 7) and gym costs were accounted for as costs to private payers. These costs were applied to all treatment
arms. The costs of managing obesity complications, applied either as chronic recurring health states costs, or as one-off costs of events, were sourced
from the literature and the Ontario Care Costing Initiative (Supplementary Table 7) [51]. Where the same costs may be covered by both public and
private payers depending on individual coverage (e.g., costs of BP medication), these were included only once in the societal perspective. All costs
published prior to 2021 were inflated using the consumer price index to May 2021 (the latest published index as of July 2021).
Utilities. The association between BMI and health-related quality of life (QoL) as well as age and gender was informed via analysis of 36-Item Short
Form Survey (SF-36) data collected in STEP 1 mapped to European QoL 5-Dimensions 3-Level Version (EQ-5D-3L) utilities using UK general population
tariffs, regressing baseline EQ-5D-3L scores against baseline BMI (continuous), controlling for age, presence of coronary artery disease, prediabetes,
hypertension, and smoking status at baseline. The regression analysis followed the approach taken by Søltoft et al (similarly, separate models were
estimated for gender) [52]. The regression coefficients applied in the modeling analysis to derive BMI-dependent utility are shown in Supplementary
Table 8.
Event-specific disutilities are applied in the cycle when the events occur. Also, a per health state disutility is applied. These disutilities are subtracted
from the BMI, gender, and age-specific utility. The mentioned disutilities were sourced from published literature (Supplementary Table 9).
Analysis
The base-case analyses were conducted for a mixed population, with NGT, prediabetes or T2D at baseline. Treatment was assumed to last up to 1 year,
after which the cohort discontinued to receive D&E alone for the rest of the analysis time horizon. Scenario analyses were performed to assess the
overall impact of the discount rate on both costs and QALYs (0% and 3%), extension of treatment duration (2 and 3 years), changing the source of risk
equations (thus using UKPDS82 for incidence of first and recurrent CV-events in T2D, and using the Framingham Heart Study for incidence of CV-events
in NGT and the Framingham Offspring study for incidence of T2D), as well as including treatment-related AEs. To assess the impact of model input
uncertainty on cost-effectiveness results, probabilistic sensitivity analysis was performed, whereby standard error of the mean (SEM) was used, or an
assumed 25% variation when SEM was not available to create parameter distributions around means: a normal distribution was assumed for efficacy
parameters, gamma for costs, beta for utilities and probabilities and a joint Dirichlet distribution for proportions. Results are presented in the cost-
effectiveness plane and as cost-effectiveness acceptability curves.
Results
Base-case
Taking a societal perspective on costs, total per-arm costs, including treatment, disease management, health states and events costs with
subcutaneous semaglutide 2.4 mg injection, D&E alone, liraglutide 3.0 mg, orlistat, and NB-32 are CAD 231 142, CAD 228 097, CAD 230 662, CAD 229
197, and CAD 229 293, respectively. The average survival of patients in the model is approximately 25 years (undiscounted) and 21 years (discounted)
and is similar across arms. Total discounted QALYs by treatment arm are 17.723, 17.621, 17.684, 17.647, and 17.649 for subcutaneous semaglutide 2.4
mg injection, D&E alone, liraglutide 3.0 mg, orlistat, and NB-32 respectively. The resulting incremental cost-effectiveness ratios (ICERs) for subcutaneous
semaglutide 2.4 mg injection are: 29 677 CAD/QALY, 12 369 CAD/QALY, 25 663 CAD/QALY, and 25 003 CAD/QALY when compared with D&E alone,
liraglutide 3.0 mg, and orlistat and NB-32, respectively (Table 2).
Page 6/14Table 2
Base-case cost-effectiveness results for subcutaneous semaglutide 2.4 mg injection vs. other treatments from a societal perspective (2021 figures).
Semaglutide 2.4 mg D&E Liraglutide 3.0 mg Orlistat NB-32 mg
Total results per-arm (CAD)
Total costs 231 142 228 097 230 662 229 197 229 293
Obesity pharmacotherapy 4 360 0 3 422 1 812 1 719
Obesity monitoring + D&E 116 078 115 896 116 010 115 950 115 945
Blood pressure treatment 989 985 987 986 986
Complications: health states 99 047 100 460 99 543 99 714 99 903
Complications: events 10 667 10 757 10 699 10 734 10 740
Total QALYs 17.723 17.621 17.684 17.647 17.649
Total life-years 20.762 20.681 20.732 20.705 20.703
Incremental results for subcutaneous semaglutide 2.4 mg injection (CAD)
Costs 3 044 480 1 945 1 849
Obesity pharmacotherapy 4 360 938 2 548 2 641
Obesity monitoring + D&E 183 68 129 134
Blood pressure treatment 4 1 3 3
Complications: health states −1 412 −496 −667 −856
Complications: events −90 −32 −67 −72
QALYs 0.103 0.039 0.076 0.074
Life-years 0.081 0.030 0.057 0.059
CEA results (CAD)
ICER (cost/QALY) 29 677 12 369 25 663 25 003
Net monetary benefit 2 085 1 459 1 844 1 848
ICER (Cost/life-year) 37 520 15 862 34 024 31 109
BID twice daily, CEA cost-effectiveness analysis, CAD Canadian dollars, D&E diet and exercise, ICER incremental cost-effectiveness ratio, Inj. injection,
QALY quality-adjusted life-year, S.C. subcutaneous
Subcutaneous semaglutide 2.4 mg injection achieved greater weight reductions in non-T2D compared with all other treatments, and similar weight
reductions with liraglutide 3.0 mg in T2D. Prediabetes reversal was comparable with liraglutide 3.0 mg in non-T2D and superior to all other treatments.
These benefits result in delays in the occurrence of weight-related complications, mainly T2D (in patients free of T2D at baseline) and weight-
associated cancers (in those with T2D at baseline). A marked reduction in sleep apnea prevalence is also noted with subcutaneous semaglutide 2.4 mg
injection in the overall cohort. CV benefits predicted with the model for subcutaneous semaglutide 2.4 mg injection are small compared with those of
existing treatments. Equally, knee replacement events remained low and similar across treatment arms (Supplementary Table 10).
Over time, these clinical results translate into cost reductions from treating obesity-related diseases, which partially offset the higher drug acquisition
costs with subcutaneous semaglutide 2.4 mg injection. Indeed, the breakdown of cost results shows that the highest contributor to obesity cost offsets
with subcutaneous semaglutide 2.4 mg injection are costs associated with delay of T2D and cancer, followed by sleep apnea. When considering
discounted results, treatment with subcutaneous semaglutide 2.4 mg injection resulted in additional expenses of CAD 3 044, CAD 480, CAD 1 945, and
CAD 1 849 per patient when compared with D&E alone, liraglutide 3.0 mg, orlistat, and NB-32, respectively.
Scenarios
Longer treatment durations of up to 2 and 3 years provide additional benefits with subcutaneous semaglutide 2.4 mg injection, but treatment costs
increase more rapidly therefore resulting in increased ICERs compared with all other treatments vs. base-case. ICERs for longer treatment durations
remained below the willingness-to-pay (WTP) threshold of CAD 50 000/QALY, implicit in the Canadian Health Technology Assessment (HTA) [53]. Other
scenarios had a limited impact on the base-case results (Table 3).
Page 7/14Table 3
Scenario analyses, societal perspective (all costs included) (2021 figures).
Cost (CAD) Total costs Total QALYs ICER vs.:
Sema D&E Lira Orlistat NB- Sema D&E Lira Orlistat NB-32 D&E Lira Orlistat NB-
2.4 3.0 mg 32 2.4 mg 3.0 mg 3.0 mg 32
mg mg mg
Base-case 231 228 230 229 229 17.723 17.621 17.684 17.647 17.649 29 12 369 25 663 25
142 097 662 197 293 677 003
SA1: 233 227 231 228 229 17.840 17.677 17.776 17.721 17.727 37 29 337 41 525 33
Treatment 464 296 591 523 722 955 184
duration: 2
years
SA2: 235 226 232 228 230 17.954 17.732 17.865 17.793 17.803 38 32 856 41 573 32
Treatment 054 540 140 365 180 400 256
duration: 3
years
SA3: 230 227 229 228 228 18.208 18.123 18.175 18.146 18.150 35 13 617 29 906 30
cardiovascular 346 387 893 497 588 010 141
disease risk in
T2D based on
UKPDS
SA4: First 230 227 230 228 228 17.507 17.401 17.467 17.433 17.429 28 12 619 29 937 24
cardiovascular 725 731 221 504 850 207 118
event
Framingham,
T2D incidence
Framingham
Offspring
study
SA5: Include 231 228 230 229 229 17.723 17.621 17.684 17.647 17.649 29 11 602 25 766 25
treatment- 158 097 706 210 304 890 134
related
adverse event
SA6: Discount 295 292 294 293 293 21.595 21.468 21.548 21.502 21.503 23 9 742 21 282 20
rate 0% 259 278 797 291 424 563 022
SA7: Discount 186 182 185 184 184 14.867 14.781 14.834 14.803 14.805 36 15 357 30 342 30
rate 3% 009 893 508 065 132 359 504
BID twice daily, D&E diet and exercise, ICER incremental cost-effectiveness ratio; Inj. injection, Lira liraglutide, NB-32 naltrexone 32 mg /bupropion,
QALY quality-adjusted life-year, SA scenario analysis, Sema subcutaneous semaglutide, T2D type 2 diabetes, UKPDS UK Prospective Diabetes Study.
Probabilistic sensitivity analysis
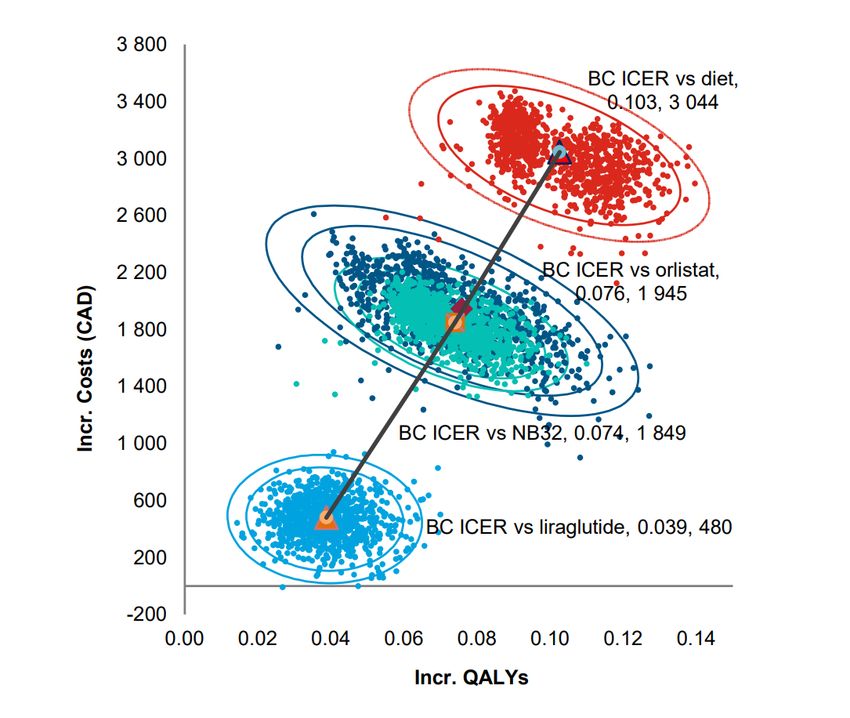
The cost-effectiveness plane displays 100% ICERs (cost/QALY) in the North-East quadrant, indicating little uncertainty with regards to the existence of
additional costs and additional QALY benefits with subcutaneous semaglutide 2.4 mg injection when comparing it with other treatments. There is some
uncertainty with the extent of the additional benefits (spread of ICERs along the X axis) and additional costs (on the Y axis) (Fig. 2).
The cost-effectiveness acceptability curve shows a high likelihood (80–100%) of subcutaneous semaglutide 2.4 mg injection being considered cost-
effective at thresholds of CAD 50 000/QALY and beyond (Fig. 3).
Discussion
The analyses estimated the long-term clinical benefits, costs, and cost-effectiveness of subcutaneous semaglutide 2.4 mg injection in a target
reimbursement population for chronic weight management in Canada, among obese and overweight adults with ≥ 1 weight-related comorbidity. The
analyses were conducted from the societal perspective using results of two head-to-head trials of subcutaneous semaglutide 2.4 mg injection and D&E,
[18, 22] informing the corresponding comparison, and results of an NMA comparing subcutaneous semaglutide 2.4 mg injection with liraglutide 3.0 mg,
orlistat, and NB-32 [18, 22, 54].
The base-case analyses showed that 1 year treatment with subcutaneous semaglutide 2.4 mg injection can be expected to result in delays in onset of
T2D, weight-associated cancers, and reductions in sleep apnea prevalence due to greater reductions in weight and SBP, and a better glycemic control
compared with all other approved treatments. This was achieved at higher treatment costs, but base-case results remained within acceptable WTP
thresholds in Canada of CAD 50 000/QALY gained. A cost-effectiveness in the US, using a 30-year time horizon, found long-term weight management
with subcutaneous semaglutide 2.4 mg injection to be cost-effective compared with no treatment, D&E alone, and all other anti-obesity medications
approved by the US Food and Drug Administration under a WTP threshold of US$ 150 000/QALY gained [55].
Page 8/14The present analysis has certain limitations. Firstly, the relative safety and efficacy vs. liraglutide 3.0 mg, orlistat, and NB-32 were sourced from indirect
comparisons and may thus be confounded by differences in trial design, trial populations, and time of efficacy assessment. These analyses may thus
be updated with direct evidence, such as the recent results of STEP 8 where subcutaneous semaglutide 2.4 mg was directly compared with liraglutide
3.0 mg in people with overweight or obesity without T2D [23]. Other limitations relate to structural uncertainty of the modeling exercise, inherent to the
nature of health economic modeling. First, it is uncertain whether a reduction in weight and other CV risk-factors for a given period (depending on the
treatment duration) would result in a reduction in the incidence of the modeled complications (CV-disease, cancer, osteoarthritis) and mortality in
patients who have suffered from obesity for a long-time. Nonetheless, evidence from the Swedish Obese Subjects trial points in this direction but the
weight loss achieved with bariatric surgery in this trial was, on average, − 23% after 2 years and maintained to a level of approximately − 18% up to 20
years from the initial surgery [56]. The association of weight reduction with many of the obesity complications herein modeled has been investigated in
other case-control studies [57], but a cause-effect relationship can only be determined via randomization. For some complications, highly prevalent in
the obese population, this evidence already exists. Such is the case of a causal effect on prediabetes reversal (shown in STEP 1 [22] and SCALE [32])
and reversal of sleep apnea [58]. Results of a CV risk-reduction trial with subcutaneous semaglutide 2.4 mg injection (SELECT) are expected in 2023. In
conclusion, the use of risk equations, assuming a causal relationship based on a demonstrated association, can be considered a valid approach for
health economic modeling, like its use in diabetes, hypercholesterolemia, and hypertension modeling. Moreover, this approach has been supported by
HTA agencies in their reviews, such as the one performed by the UK National Institute for Health and Care Excellence on Saxenda® (liraglutide 3.0 mg)
submission [59].
Second, limitations with regards to the model structure and cost inputs should be noted. It was not possible to include all complications related to
obesity in the model, and for reasons of simplicity only those with a relatively high prevalence, strong quantitative evidence of association, and
important cost and/or QoL implications were considered. Thus, the benefits and cost savings from weight loss may go beyond those herein considered,
and the presented ICERs for subcutaneous semaglutide 2.4 mg injection could be considered conservative. Even for the complications considered, it
was not possible to fully reflect their impact as it would have added excessive complexity and run time to the model. For example, it was not possible to
explicitly model all known microvascular complications following the development of T2D and worsening of beta-cell function resulting in insulin
resistance, neither the associated changes in costs nor QoL over time. As such, the model uses one cost input parameter and one QoL parameter for
microvascular complications related to T2D, which is applied throughout the analysis time horizon. This could have potentially produced an
overestimation of T2D costs in the first years of the analyses and an underestimation in the later years, potentially cancelling each other out. To
mitigate this uncertainty and others related to the cost inputs used, sensitivity analyses were conducted. Results remained highly consistent with the
ICERs found in the base-case analysis.
Conclusion
This CEA shows that once-weekly subcutaneous semaglutide 2.4 mg subcutaneous injection may be a cost-effective treatment option when compared
with D&E alone, liraglutide 3.0 mg, orlistat or NB-32 in Canadian settings using the WTP CAD 50 000/QALY gained. Subcutaneous semaglutide 2.4 mg
injection is associated with reduced obesity-related complications and costs, and higher utilities when compared to other obesity treatments in Canada.
Sensitivity and scenario analyses confirmed the robustness of the analyses.
Declarations
Funding source: This study was sponsored and funded by Novo Nordisk A/S in accordance with Good Publication Practice guidelines.
Conflict of interest: IQVIA, the employer of OAV, SM and MLa received consulting fees from Novo Nordisk for the development of the model and
conducting the analyses that are reported in this manuscript. SL, MLu and KC are full-time employees of Novo Nordisk. DCWL received consulting fees
from Amgen, Bayer, Boehringer Ingelheim, HLS Therapeutics, Eli Lilly, Novartis, Novo Nordisk, Pfizer and Viatris
Acknowledgment:
The authors wish to acknowledge Sarah Batson, Stephen Mitchell and Emily Hardy from Mtech Access for the systematic literature review and network
meta-analysis used for comparative outcomes used in the cost-effectiveness analysis, and the medical writing assistance and editorial support from
Sukanya Ghildiyal, who is an employee of IQVIA.
Data sharing statement
There is a restriction applied to the data that support the findings of this study and so are not publicly available. Data are however available from the
authors upon contracted agreement and with permission of Novo Nordisk. Please contact the corresponding author, M Luckevich
(MLVH@novonordisk.com) to request the data from this study.
References
1. World Health Organization. Obesity: preventing and managing the global epidemic. Report of a WHO consultation. 2000.
https://apps.who.int/iris/handle/10665/42330. Accessed 11 Mar, 2022.
Page 9/142. American Medical Association. Proceedings of the 2012 Annual Meeting of the American Medical Association House of Delegates. 2012.
https://www.ama-assn.org/sites/ama-assn.org/files/corp/media-browser/public/hod/a12-resolutions_0.pdf. Accessed 11 Apr, 2022.
3. Canadian Medical Association. Obesity in Canada: causes, consequences and the way forward. 2015.
https://www.cma.ca/sites/default/files/2018-11/BR2015-12.pdf. Accessed 21 Jun, 2022.
4. Obesity Canada. Obesity in Canada. 2022. https://obesitycanada.ca/obesity-in-Canada/. Accessed 29 Mar, 2022.
5. World Health Organization. Global strategy on diet, physical activity and health – 2004. 2004.
https://www.who.int/publications/i/item/9241592222. Accessed 11 Mar, 2022.
6. World Health Organization. Obesity and overweight. 2021. https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight. Accessed
11 Mar, 2021.
7. Statistics Canada. Health Fact Sheets. Overweight and obese adults, 2018. 2019. https://www150.statcan.gc.ca/n1/en/pub/82-625-
x/2019001/article/00005-eng.pdf?st=FRqwJKOe. Accessed 20 Jun, 2022.
8. Guh DP, Zhang W, Bansback N, Amarsi Z, Birmingham CL, Anis AH. The incidence of co-morbidities related to obesity and overweight: a systematic
review and meta-analysis. BMC Public Health. 2009;9:88.
9. Government of Canada. Obesity in Canada – health and economic implications. 2011. https://www.canada.ca/en/public-health/services/health-
promotion/healthy-living/obesity-canada/health-economic-implications.html. Accessed 22 Jun, 2022.
10. Wharton S, Lau DCW, Vallis M, Sharma AM, Biertho L, Campbell-Scherer D et al. Obesity in adults: a clinical practice guideline. CMAJ.
2020;192:E875–91.
11. Bausch Health Canada Inc. CONTRAVE® product monograph. 2020. https://pdf.hres.ca/dpd_pm/00056659.PDF. Accessed 21 Jun, 2022.
12. Cheplapharm Arzneimittel GmbH. XENICAL® product monograph. 2017. https://pdf.hres.ca/dpd_pm/00041463.PDF. Accessed 23 Feb, 2022.
13. Novo Nordisk Canada Inc. SAXENDA® product monograph. 2021.
https://www.novonordisk.ca/content/dam/nncorp/ca/en/products/Saxenda%20PM%20English%20-%20Marketed%20-
%2025%20February%202021.pdf. Accessed 10 Apr, 2022.
14. Biertho L, Hong D, Gagner M. Bariatric surgery: surgical options and outcomes. In: Canadian Adult Obesity Clinical Practice Guidelines, 2020.
15. Novo Nordisk Canada Inc. WEGOVY™ product monograph. 2022. https://www.novonordisk.ca/content/dam/nncorp/ca/en/products/Wegovy-
product-monograph.pdf. Accessed 10 Mar, 2022.
16. Kushner RF, Calanna S, Davies M, Dicker D, Garvey WT, Goldman B et al. Semaglutide 2.4 mg for the treatment of obesity: key elements of the STEP
trials 1 to 5. Obesity (Silver Spring). 2020;28:1050–61.
17. ClinicalTrials.gov. Semaglutide Effects on Heart Disease and Stroke in Patients With Overweight or Obesity (SELECT). 2022.
https://clinicaltrials.gov/ct2/show/NCT03574597. Accessed 24 Feb, 2022.
18. Davies M, Færch L, Jeppesen OK, Pakseresht A, Pedersen SD, Perreault L et al. Semaglutide 2·4 mg once a week in adults with overweight or
obesity, and type 2 diabetes (STEP 2): a randomised, double-blind, double-dummy, placebo-controlled, phase 3 trial. Lancet. 2021;397:971–84.
19. Kadowaki T, Isendahl J, Khalid U, Lee SY, Nishida T, Ogawa W et al. Semaglutide once a week in adults with overweight or obesity, with or without
type 2 diabetes in an east Asian population (STEP 6): a randomised, double-blind, double-dummy, placebo-controlled, phase 3a trial. Lancet
Diabetes Endocrinol. 2022;10:193–206.
20. Rubino D, Abrahamsson N, Davies M, Hesse D, Greenway FL, Jensen C et al. Effect of continued weekly subcutaneous semaglutide vs placebo on
weight loss maintenance in adults with overweight or obesity: the STEP 4 randomized clinical trial. JAMA. 2021;325:1414–25.
21. Wadden TA, Bailey TS, Billings LK, Davies M, Frias JP, Koroleva A et al. Effect of subcutaneous semaglutide vs placebo as an adjunct to intensive
behavioral therapy on body weight in adults with overweight or obesity: the STEP 3 randomized clinical trial. JAMA. 2021;325:1403–13.
22. Wilding JPH, Batterham RL, Calanna S, Davies M, Van Gaal LF, Lingvay I et al. Once-weekly semaglutide in adults with overweight or obesity. N Engl
J Med. 2021;384:989–1002.
23. Rubino DM, Greenway FL, Khalid U, O’Neil PM, Rosenstock J, Sørrig R et al. Effect of weekly subcutaneous semaglutide vs daily liraglutide on body
weight in adults with overweight or obesity without diabetes: the STEP 8 randomized clinical trial. JAMA. 2022;327:138–50.
24. Lopes S, Johansen P, Lamotte M, McEwan P, Olivieri AV, Foos V. External validation of the core obesity model to assess the cost-effectiveness of
weight management interventions. Pharmacoeconomics. 2020;38:1123–33.
25. Lopes S, Meincke HH, Lamotte M, Olivieri AV, Lean MEJ. A novel decision model to predict the impact of weight management interventions: the Core
Obesity Model. Obes Sci Pract. 2021;7:269–80.
26. Canada's Drug and Health Technology Agency. Guidelines for the economic evaluation of health technologies: Canada – 4th edition. 2017.
https://www.cadth.ca/node/101497. Accessed 15 Feb, 2022.
27. Institut national d’excellence en santé et en services sociaux. Guidance document for submitting a request to INESSS. 2018.
https://www.inesss.qc.ca/fileadmin/doc/INESSS/Inscription_medicaments/Fiches_inscription/en/Submission_guidance_document.pdf. Accessed
23 Jun, 2022.
28. Statistic Canada. Diabetes statistics in Canada. 2017. https://www150.statcan.gc.ca/n1/pub/82-625-x/2018001/article/54982-eng.htm. Accessed
10 Apr, 2022.
Page 10/1429. Twells LK, Janssen I, Kuk JL. Epidemiology of adult obesity. In: Canadian Adult Obesity Clinical Practice Guidelines, 2020.
30. Ivers NM, Jiang M, Alloo J, Singer A, Ngui D, Casey CG et al. Diabetes Canada 2018 clinical practice guidelines: key messages for family physicians
caring for patients living with type 2 diabetes. Can Fam Physician. 2019;65:14–24.
31. Rosella LC, Lebenbaum M, Fitzpatrick T, Zuk A, Booth GL. Prevalence of prediabetes and undiagnosed diabetes in Canada (2007–2011) according
to fasting plasma glucose and HbA1c screening criteria. Diabetes Care. 2015;38:1299–305.
32. Pi-Sunyer X, Astrup A, Fujioka K, Greenway F, Halpern A, Krempf M et al. A randomized, controlled trial of 3.0 mg of liraglutide in weight
management. N Engl J Med. 2015;373:11–22.
33. Hippisley-Cox J, Coupland C. Development and validation of QDiabetes-2018 risk prediction algorithm to estimate future risk of type 2 diabetes:
cohort study. BMJ. 2017;359:j5019.
34. Hippisley-Cox J, Coupland C, Brindle P. Development and validation of QRISK3 risk prediction algorithms to estimate future risk of cardiovascular
disease: prospective cohort study. BMJ. 2017;357:j2099.
35. D'Agostino RB, Russell MW, Huse DM, Ellison RC, Silbershatz H, Wilson PW et al. Primary and subsequent coronary risk appraisal: new results from
the Framingham study. Am Heart J. 2000;139:272–81.
36. Hayes AJ, Leal J, Gray AM, Holman RR, Clarke PM. UKPDS outcomes model 2: a new version of a model to simulate lifetime health outcomes of
patients with type 2 diabetes mellitus using data from the 30 year United Kingdom Prospective Diabetes Study: UKPDS 82. Diabetologia.
2013;56:1925–33.
37. Cederholm J, Eeg-Olofsson K, Eliasson B, Zethelius B, Nilsson PM, Gudbjörnsdottir S et al. Risk prediction of cardiovascular disease in type 2
diabetes: a risk equation from the Swedish National Diabetes Register. Diabetes Care. 2008;31:2038–43.
38. Young T, Shahar E, Nieto FJ, Redline S, Newman AB, Gottlieb DJ et al. Predictors of sleep-disordered breathing in community-dwelling adults: the
Sleep Heart Health Study. Arch Intern Med. 2002;162:893–900.
39. Adams KF, Leitzmann MF, Albanes D, Kipnis V, Mouw T, Hollenbeck A et al. Body mass and colorectal cancer risk in the NIH–AARP cohort. Am J
Epidemiol. 2007;166:36–45.
40. Renehan AG, Tyson M, Egger M, Heller RF, Zwahlen M. Body-mass index and incidence of cancer: a systematic review and meta-analysis of
prospective observational studies. Lancet. 2008;371:569–78.
41. Renehan AG, Zwahlen M, Egger M. Adiposity and cancer risk: new mechanistic insights from epidemiology. Nat Rev Cancer. 2015;15:484–98.
42. Wendelboe AM, Hegmann KT, Biggs JJ, Cox CM, Portmann AJ, Gildea JH et al. Relationships between body mass indices and surgical
replacements of knee and hip joints. Am J Prev Med. 2003;25:290–5.
43. Ara R, Blake L, Gray L, Hernández M, Crowther M, Dunkley A et al. What is the clinical effectiveness and cost-effectiveness of using drugs in treating
obese patients in primary care? A systematic review. Health Technol Assess. 2012;16:iii–xiv, 1–195.
44. Berrington de Gonzalez A, Hartge P, Cerhan JR, Flint AJ, Hannan L, MacInnis RJ et al. Body-mass index and mortality among 1.46 million white
adults. N Engl J Med. 2010;363:2211–9.
45. Prospective Studies Collaboration, Whitlock G, Lewington S, Sherliker P, Clarke R, Emberson J et al. Body-mass index and cause-specific mortality in
900 000 adults: collaborative analyses of 57 prospective studies. Lancet. 2009;373:1083–96.
46. Hamdy O, Uwaifo GI, Oral EA. Obesity. 2022. https://emedicine.medscape.com/article/123702-overview#a6. Accessed 27 Jun, 2022.
47. Statistics Canada. Life expectancy and other elements of the complete life table, three-year estimates, Canada, all provinces except Prince Edward
Island. Table 13-10-0114-01. 2022. https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310011401. Accessed 10 Apr, 2022.
48. Statistics Canada. Deaths and age-specific mortality rates, by selected grouped causes. Table 13-10-0392-01. 2022.
https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310039201. Accessed 10 Mar, 2022.
49. Bhaskaran K, Dos-Santos-Silva I, Leon DA, Douglas IJ, Smeeth L. Association of BMI with overall and cause-specific mortality: a population-based
cohort study of 3·6 million adults in the UK. Lancet Diabetes Endocrinol. 2018;6:944–53.
50. Lopes S, Grand T, Johansen P, Lamotte M, Olivieri AV. IDF21-0653 Exploring different ways to predict mortality in a cost-effectiveness model for
obesity. Diabetes Res Clin Pract. 2022;186:109756.
51. Ontario Ministry of Health and Long-Term Care Health Data Branch. Ontario Case Costing Initiative - data catalog (requires access rights). 2017.
https://hsim.health.gov.on.ca/hdbportal/. Accessed 10 Apr, 2022.
52. Søltoft F, Hammer M, Kragh N. The association of body mass index and health-related quality of life in the general population: data from the 2003
Health Survey of England. Qual Life Res. 2009;18:1293–9.
53. Griffiths EA, Vadlamudi NK. CADTH’s $50,000 cost-effectiveness threshold: fact or fiction? Value Health. 2016;19:A488–9.
54. Mtech Access Limited. Date on file: Semaglutide 2.4 mg for management of obesity - systematic review, meta-analysis feasibility assessment and
network meta-analysis report. In, 2021.
55. Kim N, Wang J, Burudpakdee C, Song Y, Ramasamy A, Xie Y et al. Cost-effectiveness analysis of semaglutide 2.4 mg for the treatment of adult
patients with overweight and obesity in the United States. J Manag Care Spec Pharm. 2022;28:740–52.
56. Sjöström L. Review of the key results from the Swedish Obese Subjects (SOS) trial – a prospective controlled intervention study of bariatric surgery.
J Intern Med. 2013;273:219–34.
Page 11/1457. Mariam A, Miller-Atkins G, Pantalone KM, Iyer N, Misra‐Hebert AD, Milinovich A et al. Associations of weight loss with obesity‐related comorbidities
in a large integrated health system. Diabetes Obes Metab. 2021;23:2804–13.
58. Foster GD, Borradaile KE, Sanders MH, Millman R, Zammit G, Newman AB et al. A randomized study on the effect of weight loss on obstructive
sleep apnea among obese patients with type 2 diabetes: the Sleep AHEAD study. Arch Intern Med. 2009;169:1619–26.
59. National Institute for Health and Care Excellence. Liraglutide for managing overweight and obesity. Technology appraisal guidance [TA664]. 2020.
https://www.nice.org.uk/guidance/ta664/evidence. Accessed 20 Jun, 2022.
Figures
Figure 1
Core Obesity Model structure. Reproduced/adapted from Lopes 2021[25] with permission from Wiley. ACS acute coronary syndrome, BMI body mass
index, HbA1c glycated hemoglobin, HDL high-density lipoprotein, SBP systolic blood pressure, T2D type 2 diabetes.
Page 12/14Figure 2
Cost-effectiveness plane subcutaneous semaglutide 2.4 mg injection vs. diet and exercise, liraglutide 3.0 mg, orlistat, and NB-32. BC base-case,
Incrincremental, ICER incremental cost-effectiveness ratio, NB-32 naltrexone 32 mg/bupropion, QALY quality-adjusted life-year.
Page 13/14Figure 3
Cost-effectiveness acceptability curve subcutaneous semaglutide 2.4 mg injection vs diet and exercise, liraglutide 3.0 mg, orlistat, and NB-32. NB-
32naltrexone 32 mg/bupropion,QALY quality-adjusted life-year.
Supplementary Files
This is a list of supplementary files associated with this preprint. Click to download.
Medicalwriterstatement.pdf
SupplMaterialTheCosteffectivenessofSubcutaneousSemaglutide2.4mgInjectionforChronicWeightManagementinCanadav7.0.docx
SupplFig.1.pptx
Page 14/14You can also read

















































