The COVID-19 Variants: What you need to know - Critical ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

4/13/2021 The COVID-19 Variants: What you need to know Gerald A. Evans, MD FRCPC Chair, Division of Infectious Disease Professor, Departments of Medicine, Biomedical & Molecular Sciences and Pathology & Molecular Medicine Queen’s University Kingston Health Sciences Centre April 1, 2021 1
4/13/2021 For those of you who have been away… Learning Objectives At the end of this session, the participant will have a working The WHO declared a COVID-19 a pandemic. knowledge of: 1. The epidemiology of the current variants of concern – March 11, 2020 2. The potential clinical relevance of VOCs 3. The potential impact of VOCs on vaccine effectiveness 2
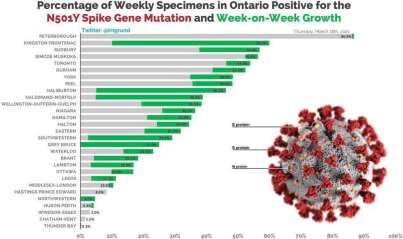
4/13/2021 Ontario Wave #3 • Primarily being driven by variants with increased transmissibility 92.1% • B.1.1.7 is dominating the rise • Vaccine rollout has been suboptimal to have a salutary effect Todate, only 8.6% of current variants have been full characterized Date March 30, 2021 3
4/13/2021 Weekly growth in Variants of Concern in Ontario matches other countries. 100% 90% % VOC by week (Countries aligned at VOC > 10%) 80% 70% 60% 50% 40% 30% 20% 10% 0% 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 Ontario Germany Netherlands Denmark Switzerland UK Data: PHO (Ontario), Robert Koch Institute (RKI), Rijksinstituut voor Volksgezondheid en Milieu (RIVM), Danish Covid-19 Consortium, SARS-CoV-2 Variants of Concern in Switzerland, Public Health England 4

4/13/2021 Case projections depend heavily on spread of variants Increase in Risks of COVID-19 Hospitalizations, ICU Admissions and Daily Cases Deaths with New VOCs as Compared to Scenarios based on 5 9,000 Early Variants (non-VOCs) models, 3-5 scenarios each. 8,000 7,000 Optimistic scenario reflects: 6,000 • Modeling approach 5,000 • Low increase of VOCs over time 4,000 • Low transmissibility of 3,000 VOCs 2,000 • Degree and timing of 1,000 relaxing public health - measures 01-01 01-08 01-15 01-22 01-29 02-05 02-12 02-19 02-26 03-05 03-12 03-19 03-26 04-02 ON - Daily ON - 7-Day Mean High Medium Low Predictions informed by modeling from COVID-19 ModCollab, Fields Institute, McMasterU, PHO, YorkU Data (Observed Cases): covid-19.ontario.ca Source: Risk of Hospitalization, ICU Admission and Death Associated with the New Variants of Concern – Ontario COVID-19 Science Advisory Table Brief March 29, 2021 5
4/13/2021 Influenza & SARS-CoV-2 – Analogies • Antigenic drift is a well-known mechanism in influenza • Small mutations in hemagglutinin and/or neuraminidase that results in antigenic changes within viral clades leading to seasonal epidemics • Mutations seen in SARS-CoV-2 produce a slower but perceptible antigenic drift in the spike protein creating ‘variants’ • These mutations are leading to both increasing transmissibility and immune escape SARS-CoV-2 Variants 6
4/13/2021 What generates Variants of SARS-CoV-2? Mutational Frequencies of SARS-CoV-2 SARS-CoV-2 • All viruses can develop • Nucleotide mutational mutations during viral frequency of six genomic replication segments of SARS-CoV-2 • The likelihood of mutation over an 11-week period arising is related to overall rates of viral replication • R5 (in yellow)is the • The more viral replication cycles genomic sequence that the more likely the occurrence of encompasses the Spike random mutations Protein of SARS-CoV-2 • Right now there is a lot of viral replication with COVID-19 worldwide SARS-CoV-2 in in this group of viruses Source: R Sanjuán & P Dominog-Calap Cell. Mol. Life Sci. (2016) 73:4433–4448 Source: N Kaushal et al Pathogens 2020, 9, 565; doi:10.3390/pathogens9070565 7
4/13/2021 WT-SARS-CoV-2 B117-SARS-CoV-2 VOC Evolution & Nomenclature Open Circles Amino acid deletion Diagram of the CORON AVIRU S Lineage Genomes Date range Comments GE NOM E Spike The root of the pandemic lies in this A 223 5 January–27 April 2020 lineage. Many Chinese sequences with global exports The base of this lineage lies in China, 24 December 2019–3 May with extensive global travel between CORONAVIRUS B 1,713 2020 multiple locations RNA genome Comprises the large Italian outbreak; it now represents many European B.1 7,438 24 January–10 May 2020 outbreaks, with travel within Europe and from Europe to the rest of the world Major European lineage; exports to the Red circles: B.1.1 6,286 15 February–9May 2020 rest of the world from Europe Amino acid Substitutions Start of 3 0 ,0 00 genom e RNA letters Connecting rays: Source: A Rambaut et al Nature Micro https://doi.org/10.1038/s41564-020-0770-5 MUTATIONS 8
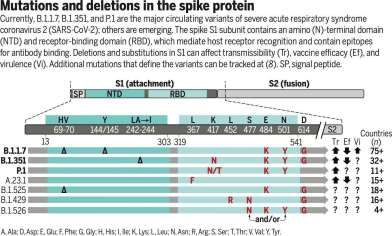
4/13/2021 Spike Protein Mutations • N501Y is the most common H69–V70 deletion Y144/145 • Increases avidity for ACE2 receptor • Likely main reason for increased transmissibility Coronavirus • Deletions like H69-70 and other mutations like spike gene, B. 1. 1. 7 N501Y mutation A570D E484K likely contribute to decrease binding by lineage P681H T716I neutralizing antibodies to spike protein • Other mutations being studied as to their S 9 82A implications D1118H • K417N • L452R The N501Y mutation is near the tip of the coronavirus spike, where it seems to change the shape of the protein to be a tighter fit with human cells 9
4/13/2021 The E484K mutation occurs near the top of the coronavirus spike, where it alters the shape of the protein. This change may help the spikes evade some types of coronavirus antibodies. 10
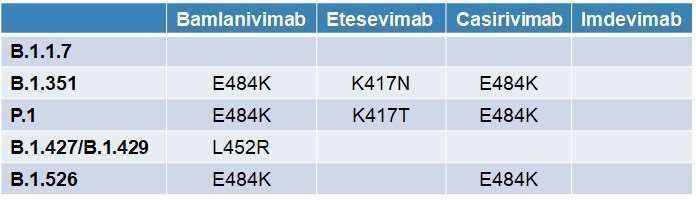
4/13/2021 Variants & Monoclonal Ab Selection 11
4/13/2021 Why are we concerned about Variants? Why are we concerned about Variants? • Worldwide spread following their • Possible consequences of emerging mutations emergence • More variants are continuing to 1. Increased transmissibility arise with uncontrolled numbers of cases around the world 2. Increased virulence • Without control on the numbers 3. Decreased protection from current vaccines or of cases, variants with better fitness will eventually previous natural infection predominate over the wild type strain of SARS-CoV-2 Source: https://nextstrain.org/ncov/global 12
4/13/2021 Current SARS-CoV-2 Variants of Concern (VOC) SARS-CoV-2 Variants of Interest (VOI) • The chief variants of concern presently are: • B.1.1.7 (UK origin) + E484K • B.1.1.7 (UK variant) • Bad combination due to potential for immune evasion • B.1.351 (South African variant) • P.2 (Brazilian origin) • B.1.128 aka P.1 (Brazilian variant) • Has E484K and V1176F • P.3 (Philippines origin) • B.1.427/429 (California origin) Variant Name Amino Acid Changes in Spike 20E (EU1) A222V-D614G 20A.EU2 S477N-D614G • Has L452R with potential for immune evasion to monoclonal Abs • B.1.525/526 (New York origin) N439K-D614G N439K-D614G Mink Cluster 5 Variant ∆H69∆V70-Y453F-D614G-I692V-M1229I B.1.1.7 ∆H69∆V70-∆Y144-N501Y-A570D-D614G-P681H- • Partial E484K T716I-S982A-D1118H • Double mutant reported in India (a.k.a., 20I/501Y.V1, VOC 202012/01) B.1.351 L18F-D80A-D215G-∆L242∆A243∆L244-R246I- (a.k.a., 20H/501Y.V2) K417N-E484K-N501Y-D614G-A701V • E484Q and L452R 13
4/13/2021 Transmission of SARS-CoV-2 Lineage B.1.1.7 in England B.1.1.7 Infectiousness A) B) Density Density • Mean duration of the proliferation phase • B117 = 5.3 days ● ●● ● ● ● ● ● ● ● ● ● ●●●●● ● ●●● ● ●●● ● ● ● ●●● ●●● ●●●●●●● ●●●●●● ●● ● ● ●● ● ● ● ● ● ● ● ●●● ●●●● ● ● ● ● ● ●●●● ● ● ● ●● ●●●● ● ● ●●●●● ●● ● ● ● ● ● ● ● ●● ● ● ● ● ● ● ● • Non-B117 = 2.0 days 106 107 108 109 1010 0 3 6 9 Mean peak RNA copies per ml Mean proliferation stage duration (days) C) D) • Mean duration of the clearance phase • B117 = 8.0 days Density Density • Non-B117 = 6.2 days • Mean overall duration of infection 0 3 ● ● ● ●● ●● ● ●●● ● ● ●●●●●●●●● ● ●● ● ● ● ● ● ●●● ● ● ●●● ● 6 ● ●●● ●● ●●● 9 ●● ● ● ● 12 0 ● 5 ● ● ●● ●●● ●● ● ●●●●● ●●●●●● ● 10 ●● ● ● ●●●● ● ● ● ● ●●●●●●● ● ●●●●● ● ● ● 15 ●● ● ● 20 (proliferation plus clearance) Mean clearance stage duration(days) E) Mean acute infection duration (days) • B117 = 13.3 days 15 • Non-B117 = 8.2 days 20 8 log10 RNA copies ml • Peak viral RNA Ct = 19.0 vs 20.2 25 Ct 6 30 35 4 40 −5 0 5 Days from peak Source: E Volz et al Preprint https://doi.org/10.1101/2020.12.30.20249034 Source: S Kissler et al https://nrs.harvard.edu/URN-3:HUL.INSTREPOS:37366884 14
4/13/2021 Data table – preliminary results Paper Method Sample Outcome Estimate of 95%CI Effect VOC Transmissibility B117 Mortality Imperial Non- parametric analysis: case- control weighting All samples, corrected for probability that S- gene negative samples are the VOC Ratio of S-negative to S-positive case fatality ratios 1.36 1.18-1.56 Imperial Non- All samples, Ratio of S-negative to 1.29 1.07-1.54 parametric corrected for S-positive case fatality analysis: probability that S- ratios standardised gene negative • B.1.1.7 – 40-50% more transmissible1 • UK data CFR samples are the VOC LSHTM Cox All samples, Hazard ratio for death 1.35 1.08-1.68 proportional adjusted for VOC-infected hazards model misclassification of individuals to non-VOC • B.1.427/B.1.429 – 20% more transmissible2 • On the outcome of COVID-19 case- LSHTM Cox proportional hazards model SGTF All samples, after 01.11.20 (not adjusted for infected individuals Hazard ratio death for VOC-infected individuals to non-VOC 1.28 1.06-1.56 • B.1.351 – 50% more transmissible3 fatality the estimated effect is 1.28 Exeter Matched case misclassification of SGTF) Samples since 01 infected individuals Hazard ratio death for 1.91 1.35-2.71 (95%CI 1.07-1.54) control study October, various VOC-infected adjustments individuals to non-VOC • B.1.128 - ? infected individuals CO-CIN Multinomial CO-CIN data from Odds ratio of death in 0.63 0.20-1.69 • On average a 28% higher risk for dying model a single trust hospitalised VOC- infected individuals to non-VOC infected • B.1.525/B.1.526 - ? individuals c/w non-VOC Wuhan SARS-CoV-2 PHE Retrospective matched cohort study Cases and comparators with at least 28 days Odds ratio of hospital admission in SGTF cases vs non-SGTF 1.07 0.86-1.33 infection (initial analysis) between specimen date and study end date cases • Is this real or related to higher PHE Retrospective Whole cohort Relative risk of death in 1.3 0.95-1.79 matched SGTF cases vs non- cohort study SGTF cases within 28 (initial analysis) days of a +ve result PHE Retrospective Cases and Relative risk of death in 1.00 0.58-1.73 infection rates from increased matched cohort study (initial analysis) comparators with at least 28 days between specimen SGTF cases vs non- SGTF cases within 28 days of a +ve result Sources: 1. NextTag transmission to vulnerable groups? PHE Retrospective matched date and study end date Whole cohort Relative risk of death in SGTF cases vs non- 1.65 1.21-2.25 2. Deng X, Garcia-Knight MA, Khalid MM, et al. Transmission, infectivity, and antibody neutralization of an emerging SARS-CoV-2 variant in California carrying a L452R spike protein cohort study (updated SGTF cases within 28 days of a +ve result mutation. MedRxiv 2021. doi: https://doi.org/10.1101/2021.03.07.21252647 analysis 19/01) 3. Mahase E. Covid-19: what new variants are emerging and how are they being investigated?BMJ. 2021;372:n158. Available from: https://doi.org/10.1136/bmj.n15 Source: P Horby et al NERVTAG note on B.1.1.7 severity SAGE Jan 21, 2021 15
4/13/2021 B117 Mortality B117 Mortality Risk – UK Risk – UK • From a dataset linking • From a dataset linking 2,245,263 positive SARS- 2,245,263 positive SARS- CoV-2 community tests CoV-2 community tests and 17,452 COVID-19 and 17,452 COVID-19 deaths in England from 1 deaths in England from 1 Sept 2020 to 14 Feb 2021 Sept 2020 to 14 Feb 2021 • SGTF vs non-SGTF • SGTF vs non-SGTF • Hazard of death with SGTF • Hazard of death with is 55% (95% CI 39–72%) SGTF is 55% (95% CI 39– higher after adjustment 72%) higher after adjustment Source: NG Davies et al Nature 2021 Source: NG Davies et al Nature 2021 https://doi.org/10.1038/s41586-021-03426-1 https://doi.org/10.1038/s41586-021-03426-1 16
4/13/2021 Risk of ICU Admission Associated with VOCs Compared Meta-Analysis of the with Early Variants by Time Since Diagnosis of COVID-19 Risk of COVID-19 Hospitalization, Intensive Care Unit Admission and Death Associated with new VOCs Compared to Early Variants Source: Risk of Hospitalization, ICU Admission and Death Associated with the New Variants of Source: Patone M, Thomas K, Hatch R, et al. Analysis of severe outcomes associated with the SARS-CoV-2 Variant of Concern 202012/01 in England using Concern – Ontario COVID-19 Science Advisory ICNARC Case Mix Programme and QResearch databases. medRxiv. Published online March 12, 2021:2021.03.11.21253364. Table Brief March 29, 2021 doi:10.1101/2021.03.11.21253364 17
4/13/2021 Risk of Death Associated with VOCs Compared with Risk of Death Associated with VOCs Compared with Early Variants by Time of Diagnosis of COVID-19 Early Variants by Time of Diagnosis of COVID-19 Source: Challen R, Brooks-Pollock E, Read JM, Dyson L, Tsaneva-Atanasova K, Danon L. Risk of mortality in patients infected with SARS- Source: Challen R, Brooks-Pollock E, Read JM, Dyson L, Tsaneva-Atanasova K, Danon L. Risk of mortality in patients infected with SARS- CoV-2 variant of concern 202012/1: matched cohort study.BMJ. 2021;372:n579. doi:10.1136/bmj.n579 CoV-2 variant of concern 202012/1: matched cohort study.BMJ. 2021;372:n579. doi:10.1136/bmj.n579 18
4/13/2021 Ontario Variants: Bottom Line • B.1.1.7, the VOC originally identified in the UK is now dominating the trajectory of the pandemic curve in NA & Europe • B.1.1.7 is associated with: • Increased transmission • Increased risk of hospitalization, ICU admission and death • In general, there is a 10-day time lag until the full increase in risk of death becomes apparent after the initial rise in cases SARS-CoV-2 Variants and Immune Escape 19
4/13/2021 Vaccine-induced Immunity to SARS-CoV-2 1. Protective immunity ✅ Good • Immunity protects the individual from more severe disease ↓ 2. Sterilizing immunity ❓→ ✅ Better • Immunity confers protection from infection ↓ 3. Transmission immunity ❓→ ✅ • Immune individuals do not transmit infection Best • Herd immunity when sufficient numbers vaccinated Source: C Chambers at https://healthydebate.ca/2021/03/topic/comparing-vaccines/?utm_source=mailpoet&utm_medium=email&utm_campaign=what-you- need-to-know-about-vaccines_6 20
4/13/2021 Time Periods for Pfizer & AZ & Vaccine RCTs Moderna Janssen Source: C Chambers at https://healthydebate.ca/2021/03/topic/comparing-vaccines/?utm_source=mailpoet&utm_medium=email&utm_campaign=what-you- need-to-know-about-vaccines_6 21
4/13/2021 Dynamics of the Adaptive Immune Response to Vaccines 22
4/13/2021 Functional T-cell responses modulate COVID-19 disease severity • Strong T cell responses in all trials seem to have led to prevention of severe disease • Even prior to vaccines, data indicating T-cell immunity from other coronaviruses led to milder SARS-CoV-2 infection • If you get re-infected after natural infection or vaccine (rare to date), it appears to be mild, if there has been a good T-cell response • Study from 1918 survivors of Spanish flu pandemic showed durable B-cell immunity (memory B-Ab) 90 years later 23
4/13/2021 South Africa AZ Vaccine Suspension South Africa AZ Vaccine Study 12.5 • Based on a study of around 2,000 participants whose median age was • MC DBRCT in South Africa of 100 31 HIV- subjects 80 10.0 • AstraZeneca vaccine had been showing a 75% efficacy against mild to • Participants 18-65 years of 7.5 Vaccine Cumulative Events age (mean age =31) 60 5.0 Placebo moderate COVID cases until the B.1.351 strain became dominant in • Placebo = 1010 40 2.5 South Africa • Vaccine = 1011 (%) 0.0 • After that, the efficacy dropped to just 22% percent, based on 42 • A 2-dose regimen of the 20 0 50 100 150 200 symptomatic cases ChAdOx1 nCoV-19 vaccine 0 did not show protection 0 50 100 150 200 • However, the number of cases involved was too small to draw firm against mild-to-moderate No. at Risk Vaccine 750 738 Days since Second Dose 674 137 0 conclusions COVID-19 due to the B.1.351 Placebo 717 707 632 124 0 variant Cumulative No.f Events Vaccine 0 2 6 14 19 Placebo 0 2 10 21 23 Source: S Mahdi et al NEJM 2021 DOI: 10.1056/NEJMoa210221 24
4/13/2021 Other Preliminary Reports on Vaccine AZ Vaccine Efficacy Variant N (%) ChAdOx1 Control VE 95%CI Effectiveness vs. B.1.351 against B.1.1.7 and Primary Symptomatic COVID-19 nCoV-19 • Preliminary data from non- B.1.1.7 strains B.1.1.7 Other variants 34 (14%) 86 (34%) 7/4236 12/4236 27/4270 74/4270 74.6% (41.6%, 88.9%) 84.1% (70.7%, 91.4%) J&J/Janssen® single-dose • Between 1st Oct 2020 No sequence result* Not sequenced** 25 (10%) 105 (42%) 5/4236 28/4236 20/4270 77/4270 75.4% (34.3%, 90.8%) 64.3% (44.9%, 76.8%) vaccine suggested it was 72% and 14th Jan 2021 Total cases 250 52/4236 198/4270 74.2% (65.0%, 81.0%) effective against moderate to Asymptomatic/Unknown infections severe COVID-19 in the U.S. • Similar to the efficacy of B.1.1.7 14 (7%) 6/4236 8/4270 26.5% (-112.0%, 74.5%) compared with 57% effective in the vaccine against other Other variants 30 (14%) 6/4236 24/4270 75.4% (39.9%, 89.9%) No sequence result 37 (18%) 21/4236 16/4270 -28.7% (-146.6%, 32.8%) South Africa non-B117 lineages Not sequenced 127 (61%) 63/4236 64/4270 3.1% (-37.3%, 31.6%) • Novavax® said the efficacy of • Reduction in the duration Total cases 208 96/4236 112/4270 15.7% (-10.7%, 35.8%) Any NAAT+ infection† its vaccine in studies from the of shedding and viral load B.1.1.7 51 (10%) 13/4236 38/4270 66.5% (37.1%, 82.1%) U.K. was 89% compared to 60% Other variants 128 (26%) 21/4236 107/4270 80.7% (69.2%, 87.9%) in South Africa No sequence result Not sequenced 69 (14%) 251 (50%) 29/4236 101/4236 40/4270 150/4270 28.8% (-14.9%, 55.9%) 33.8% (14.7%, 48.6%) Total cases 499 164/4236 335/4270 51.9% (42.0%, 60.1%) Source: KRW Emary et al Preprint 2021 https://ssrn.com/abstract=3779160 25
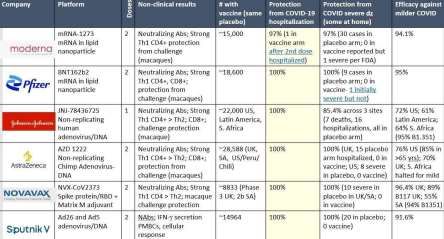
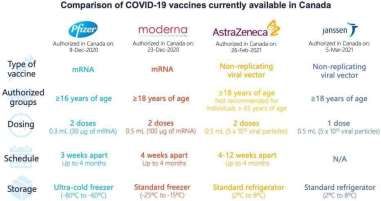
4/13/2021 Neutralizing Abs from Pfizer-BioNTech Vaccine vs. Clinical Efficacy of COVID-19 Vaccines Variants Vaccine Platform Doses Efficacy Efficacy Efficacy non-VOCs B.1.1.7 B.1.351 (Symptomatic) Pfizer-BioNTech mRNA 2 95% Unknown Unknown Moderna mRNA 2 94.5% Unknown Unknown Oxford/AZ AdV Vector 2 81.5% 70.4% 10-20% J&J/Janssen AdV Vector 1 72% Unknown 57% Novavax Recombinant subunit 2 95.6% 85.6% 60% • 20 serum samples obtained from 15 participants in the RCT • 2 or 4 weeks after the administration of the 2nd dose of BNT162b2 Sources: BMJ 2021;372:n597 | doi: 10.1136/bmj.n597 Lancet March 30, 2021 https://doi.org/10.1016/S0140-6736(21)00628-0 Source: Y Liu et al NEJM 2021 DOI: 10.1056/NEJMc2102017 26
4/13/2021 Moderna Neutralizing Antibody Titres from Vaccine Moderna Neutralizing Antibody Titres from Vaccine Recipients to B.1.1.7 Recipients to B.1.351 A D614G or Spike Mutations in B.1.1.7 B Matched Samples, D614G C D614G or Spike Mutations in B.1.351 D Matched Samples, D614G and B.1.1.7 and B.1.351 4 4 P=0.64 P=0.008 4 4 Reciprocal ID50 Titer (log10) Reciprocal ID50 Titer (log10) Reciprocal ID50 Titer (log10) Reciprocal ID50 Titer (log10) 3 3 3 3 2 2 2 2 1 1 1 1 Source: K Wu et al NEJM 2021 DOI: 10.1056/NEJMc2102179 Source: K Wu et al NEJM 2021 DOI: 10.1056/NEJMc2102179 27
4/13/2021 Summing up: Why are we concerned about COVID-19 Ontario – April 1, 2021 Variants? • Possible consequences of emerging mutakons • Where are we SARS-CoV-2 variants • Right now we’re in a 3rd wave and in 1. Increased transmissibility ✅ Ontario, mostly driven by SARS-CoV-2 variants 2. Increased virulence ✅ • Variants • A cause for concern due to increase in 3. Decreased proteckon from current vaccines or transmissibility and virulence previous natural infeckon ⚠ – with some • Vaccines and variants • They maintain effectiveness against B.1.1.7 but less so against B.1.351 likely due to the E484K mutation 28
4/13/2021 29
4/13/2021 30
You can also read

















































