The potential of serum neurofilament as biomarker for multiple sclerosis
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

doi:10.1093/brain/awab241 BRAIN 2021: 144; 2954–2963 | 2954
The potential of serum neurofilament as
biomarker for multiple sclerosis
Stefan Bittner,1 Jiwon Oh,2 Eva Kubala Havrdová,3 Mar Tintoré4 and Frauke Zipp1
Downloaded from https://academic.oup.com/brain/article/144/10/2954/6310737 by guest on 16 December 2021
Multiple sclerosis is a highly heterogeneous disease, and the detection of neuroaxonal damage as well as its quantifica-
tion is a critical step for patients. Blood-based serum neurofilament light chain (sNfL) is currently under close investiga-
tion as an easily accessible biomarker of prognosis and treatment response in patients with multiple sclerosis.
There is abundant evidence that sNfL levels reflect ongoing inflammatory-driven neuroaxonal damage (e.g. relapses or
MRI disease activity) and that sNfL levels predict disease activity over the next few years. In contrast, the association of
sNfL with long-term clinical outcomes or its ability to reflect slow, diffuse neurodegenerative damage in multiple scler-
osis is less clear.
However, early results from real-world cohorts and clinical trials using sNfL as a marker of treatment response in mul-
tiple sclerosis are encouraging. Importantly, clinical algorithms should now be developed that incorporate the routine
use of sNfL to guide individualized clinical decision-making in people with multiple sclerosis, together with additional
fluid biomarkers and clinical and MRI measures.
Here, we propose specific clinical scenarios where implementing sNfL measures may be of utility, including, among
others: initial diagnosis, first treatment choice, surveillance of subclinical disease activity and guidance of therapy
selection.
1 Department of Neurology, Focus Program Translational Neuroscience (FTN) and Immunotherapy (FZI), Rhine-Main
Neuroscience Network (rmn2), University Medical Center of the Johannes Gutenberg University Mainz, Mainz 55131,
Germany
2 Division of Neurology, Department of Medicine, St Michael’s Hospital, University of Toronto, Toronto, Ontario M5S
3H2, Canada
3 Department of Neurology and Center of Clinical Neuroscience, First Faculty of Medicine, Charles University and
General University Hospital, Prague 116 36, Czech Republic
4 Department of Neurology, Hospital General Universitari Vall D’Hebron, Cemcat, Barcelona 08035, Spain
Correspondence to: Stefan Bittner
University Medical Center of the Johannes Gutenberg University Mainz
Langenbeckstr. 1
Mainz 55131, Germany
E-mail: bittner@uni-mainz.de.
Correspondence may also be addressed to: Frauke Zipp
E-mail: zipp@uni-mainz.de
Keywords: biomarkers; neurofilament; prognosis; therapy response; multiple sclerosis
Abbreviations: CIS = clinically isolated syndrome; EDSS = Expanded Disability Status Scale; RRMS = relapsing-remit-
ting multiple sclerosis; sNfL = serum neurofilament light chain; SPMS = secondary progressive multiple sclerosis
Received March 5, 2021. Revised May 27, 2021. Accepted June 14, 2021. Advance access publication June 28, 2021
C The Author(s) (2021). Published by Oxford University Press on behalf of the Guarantors of Brain.
V
This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial License (https://creativecommons.org/licenses/
by-nc/4.0/), which permits non-commercial re-use, distribution, and reproduction in any medium, provided the original work is properly cited. For commercial
re-use, please contact journals.permissions@oup.comSerum NfL as biomarker for multiple sclerosis BRAIN 2021: 144; 2954–2963 | 2955
Introduction Serum NfL as a diagnostic biomarker in
Multiple sclerosis is a chronic inflammatory CNS disorder in which multiple sclerosis: distinct diagnostic
neuroaxonal damage is closely related to clinical and MRI events situations
and prognostication.1,2 Neurofilament light chain (NfL) is a major
Without considering any additional clinical context, sNfL alone is
component of neuronal and axonal cytoskeleton proteins, provid-
insufficient for a diagnosis of multiple sclerosis or for differentiat-
ing structural support in the central and peripheral nervous sys-
ing multiple sclerosis from other neuroinflammatory disorders
tems. Apart from inflammatory diseases, elevated NfL has among
with neuroaxonal damage and elevated sNfL levels,32 such as neu-
others been reported in neurodegenerative, traumatic and ischae-
romyelitis optica spectrum disorders or myelin oligodendrocyte
mic brain diseases.3–5 A comparison of CSF NfL levels across more
glycoprotein (MOG)-encephalomyelitis.33–35 However, in specific
than 30 different neurological disorders revealed increased levels
clinical situations, sNfL can contribute to differential diagnostics.
compared with healthy controls in most cases.6 High NfL levels are
As one example, patients developing progressive multifocal leu-
therefore a general reflection of axonal damage, independent of
koencephalopathy (PML) on natalizumab treatment had a steeper
underlying aetiology. However, the absolute values and/or tem-
sNfL increase than those with multiple sclerosis-related relapses.36
Downloaded from https://academic.oup.com/brain/article/144/10/2954/6310737 by guest on 16 December 2021
poral dynamics seem to reflect different competing aetiologies. In
A recent study took advantage of a unique prospective longitudin-
patients with multiple sclerosis, especially in cases where serum
al serum biobank effort with detailed clinical and demographic
NfL (sNfL) values are higher than expected in otherwise stable
data in the US Department of Defense Serum Repository. Sixty
patients, alternative causes and comorbidities such as head
individuals were identified who subsequently developed multiple
trauma, polyneuropathy or microvascular CNS lesions need to be
sclerosis and had previous serum collection in the years preceding
considered. Thus far, neuropsychiatric or cognitive symptoms are
diagnosis. sNfL levels were already elevated 6 years (range:
not related to sNfL levels according to results from a smaller co-
4–10 years) prior to disease onset and showed a further increase in
hort.7 With axonal damage, NfL proteins are not only released into the years leading up to the first clinical symptoms.37 Other studies
the CSF compartment, but also subsequently in low amounts have investigated patients with radiologically isolated syndrome,
(2%) into the peripheral blood.8,9 Research on neurofilament pro- who are clinically asymptomatic patients undergoing MRI exami-
teins has been performed for more than 20 years,10,11 but was ini- nations for other reasons with incidental multiple sclerosis-like
tially limited with respect to translational suitability due to the CNS lesions. In patients with radiologically isolated syndrome,
necessity of obtaining CSF samples. However, because of novel elevated sNfL levels indicate a higher risk for developing either
highly sensitive analytic methods (namely single molecule array, clinically isolated syndrome (CIS) or multiple sclerosis in the fu-
SIMOA, technology),12 minimal concentrations in the single-digit ture.38 These studies from presymptomatic patients with multiple
picogram/millilitre range can now be detected in serum or plasma sclerosis underscore the long prodromal phase of this disease prior
samples by specialized laboratories13 and, since c. 2017, are in- to the first clinical relapse with evident ongoing neurodegenera-
creasingly being used in multiple sclerosis research8 (Box 1). tive processes.
Correlations between CSF and blood values of NfL are high,14,15 MRI lesions and oligoclonal bands in the CSF are established
and thus assessment in the peripheral blood is presumed suffi- risk factors for a diagnosis of multiple sclerosis.39 In several stud-
cient, although a certain amount of uncertainty still exists as to ies performed in patients with CIS, elevated NfL values in the
whether this assumption can be generalized to all concentrations CSF40–42 or serum43,44 were an additional predictor of future relap-
and patient subgroups.16 The minimally invasive detection in ses. Importantly, studies mostly corrected for other known risk
blood samples can be considered a breakthrough for the potential factors (such as age, oligoclonal bands and T2 lesion numbers),
broader application of this marker in clinical practice. Herein, we highlighting the added value of sNfL as an independent risk factor.
will critically discuss the current progress and view regarding the In a cohort of more than 800 patients of the German Clinical
role of sNfL in answering essential clinical questions in patients Competence Network for Multiple Sclerosis (KKNMS), the role of
with multiple sclerosis (Box 2). early sNfL values for the diagnostic evaluation of patients was
Box 1 Neurofilament in a nutshell
Blood levels of sNfL, a neuron-specific cytoskeletal protein, have emerged as a biomarker able to capture neuronal damage in mul-
tiple sclerosis and a wide variety of neurological conditions. Following neuronal damage, sNfL is released into the CSF and subse-
quently into the blood, where it can be measured with current ultrasensitive assays (SIMOA), overcoming the problem of the inher-
ently invasive lumbar punctures needed for CSF-based markers. This simple approach to assessing the degree of ongoing neuronal
damage in the peripheral blood during standard patient care could greatly enhance clinical decision-making. One major advantage
of sNfL is that it shows high stability at room temperature and in frozen blood samples, and it is not affected by thawing cycles or
storage time,8,17,18 opening the door for broad application. Although many candidate biomarkers were in the past found to corres-
pond to existing clinical information, to add no additional information to MRI19,20 or to be too technically challenging to implement
in clinical practice, sNfL is not hampered by these issues. It is important to note when comparing different studies that the com-
mercially available SIMOA assay21,22 is known to produce lower absolute sNfL concentrations (by about 50%) compared to previous-
ly used assays with different protocols in earlier studies.23,24 Importantly, a recent multicentre study analysing identical serum
samples across 17 different international sites reported excellent inter-assay (56%) and inter-site (59%) coefficients of variation for
the most widely used commercial NF-lightTM assay.25–29 Inter- and intra-batch assay variability, as well as variability across differ-
ent newly emerging technical platforms (e.g. the ELLA system)30 are issues that still need to be addressed. Further international
efforts to standardize sNfL measures are ongoing.27,31 See Table 2 for recommendations on quality controls to be reported in publi-
cations. Furthermore, sNfL has thus far been investigated on a group level, whereas prospective use on an individual patient level
has not yet been established (see Fig. 1 for proposed clinical algorithms).2956 | BRAIN 2021: 144; 2954–2963 S. Bittner et al.
Box 2 Overview on the role of sNfL in multiple sclerosis
• Role in preclinical multiple sclerosis? Serum NfL is increased up to 6 years prior to first clinical symptoms and indicates a risk for
a first clinical event in patients with radiologically isolated syndrome, when it is increased.
• Role in diagnosis? At a group level, sNfL is higher in patients with RRMS than in healthy controls. sNfL thus indicates disease
versus functional symptoms and might improve differentiation between CIS and RRMS patients when included in current
diagnostic criteria.
• Role for prognosis? Elevated sNfL levels have predictive value for future relapses, new gadolinium-enhancing or T2 lesions and
future brain and spinal cord atrophy. With regard to clinical outcome, long-term predictions according to high sNfL levels is still
controversial, while the predictive value of short-term EDSS-deterioration is undisputed.
• Role for monitoring of disease activity? Levels of sNfL are associated with clinical and MRI parameters that indicate
inflammatory disease activity. Low or stable sNfL levels can exclude clinical or subclinical disease activity. Small increases in
Downloaded from https://academic.oup.com/brain/article/144/10/2954/6310737 by guest on 16 December 2021
sNfL levels may indicate progression in relapse-free phases.
• Treatment response? Levels of sNfL are decreased by effective treatment initiation in both clinical trials and real-world cohorts.
First studies suggest that sNfL levels might be able to differentiate between low and high efficacy treatments.
assessed.21 The inclusion of sNfL levels as an additional parameter probability of EDSS deterioration gradually increased with each cat-
into the current 2017 version of the McDonald criteria45 increased egory of higher sNfL level percentile.23 Notably, in a multivariable
the sensitivity and specificity of differentiating patients with CIS model, only sNfL predicted future brain volume loss in contrast with
and relapsing-remitting multiple sclerosis (RRMS).21 other parameters (T2 lesion volume, baseline normalized brain vol-
ume and contrast-enhancing lesions).23 Importantly, the central
messages of these studies only apply to a relatively small portion of
Serum NfL as a biomarker of disease patients with multiple sclerosis who have the highest sNfL levels. Of
activity in multiple sclerosis note, studies reported 46% of samples23 and 49% of samples8 from
patients with multiple sclerosis were above the 80th percentile and
Serum NfL, clinical activity and MRI: short-term
showed significantly more EDSS worsening in the following year.
A broad spectrum of clinical and MRI parameters linked to inflamma-
tory processes have demonstrated correlations to concurrently Serum NfL, clinical activity and MRI: long-term
assessed sNfL levels (Table 1). Large studies in 814 and 607 patients
clarified that the current Expanded Disability Status Scale (EDSS) A number of studies have confirmed that high sNfL levels have
score and sNfL levels are weakly, yet significantly, associated (12% predictive value for future MRI-based brain atrophy over the next
and 8% sNfL increase per EDSS step, respectively).21,23 Furthermore, 2–5 years23,46,49,51 and two studies have found predictive value for
sNfL levels were shown to correlate with concurrent relapses,8,21,23 brain atrophy in the longer-term at 10 and 12 years.24,52 In contrast,
the presence of gadolinium-enhancing lesions,8,9,21,43 the number of data concerning the longer-term predictive value of sNfL for dis-
gadolinium-enhancing lesions,14,15,23,47 the occurrence of new T2- ability progression are thus far less convincing. sNfL levels pre-
weighted lesions,9 the number of new T2-weighted lesions,21,23,43,46 dicted the transition from RRMS to secondary progressive multiple
the number and volume of cortical lesions,57 the presence of T1- sclerosis (SPMS) in two 5-year follow-up studies,51,53 whereas other
hypointense lesions in patients with CIS41 and T1 lesion volume46 as studies did not find a significant relationship between sNfL and
well as normalized brain volume, a cross-sectional measure of brain the risk of SPMS conversion.48,54 In three studies, sNfL was not
atrophy.23 Here it should be noted that sNfL levels are significantly associated with EDSS-progression over 5 years48 and 10 years24,53,
increased after a relapse or detection of a gadolinium-enhancing whereas a correlation was observed in other 5-year studies.53,60 In
lesion and can persist for some time (a few weeks to several a study of more than 120 patients, initial sNfL levels were not cor-
months).9,15,23,58 Other parameters thus far have demonstrated related with EDSS values after 10 years, but did predict T2 lesion
mixed results [e.g. (i) sNfL with T2 lesion volumes with significant8,47 load and brain atrophy rates.52 The patient cohort in this study,
and not significant23 correlations; and (ii) sNfL and deep grey-matter however, was rather benign, with only 11% of patients with mul-
structures with significant14,44,51 and not significant correlations] or tiple sclerosis reaching an EDSS score of 3.0 or more by 10 years
showed no correlation with sNfL values (e.g. the presence of oligoclo- (mean disease duration at first visit: 1.6 years). In contrast, another
nal bands or vitamin D3 levels).43,47 See also Table 1 for a summary study with a more aggressive disease cohort recruited in the era
of the relationships between sNfL and different clinical/MRI parame- before modern disease-modifying drugs (43% of patients reaching
ters. Despite differences in methodological approaches across stud- an EDSS score of 3.0 by 10 years; mean disease duration at first
ies, all findings support that sNfL levels provide a good reflection of visit: 3.1 years) showed that patients with the highest sNfL levels
ongoing inflammation-driven neuroaxonal damage. This is in line progressed most rapidly with an annual rate of increase in the
with positive correlations between the inflammatory activity of mul- EDSS score of 0.16 over a median follow-up of 19 years.55,56 In one
tiple sclerosis lesions and axonal damage.59 large study in 44000 patients and a median follow-up of 5 years,
Over a relatively short period, high sNfL levels were associated high sNfL levels were associated with the risk of reaching an EDSS
with an increased risk for relapses and/or EDSS deterioration over score of 3.0 and 4.0, but not 6.0.54 One plausible explanation for the
the next 1–3 years.8,21,23,48,49 In a study of patients with multiple discrepancies observed across these studies might be the fact that
sclerosis and healthy controls (n = 259 each), sNfL levels above the sNfL levels strongly reflect acute, focal inflammatory neuronal in-
90th percentile of healthy controls predicted EDSS worsening in jury due to relapses or subclinical MRI lesions in RRMS, and that
the subsequent year [odds ratio (OR) 2.8, confidence interval (CI) this might mask slowly progressing neurodegenerative processes.
1.61–4.83],23 which confirmed findings from an earlier study in 241 At this point, our assessment is based on the size of the cohort
patients with repeated serum sampling (OR 2.1, CI 1.03–4.29).8 The studies and comes with the knowledge that technical differencesSerum NfL as biomarker for multiple sclerosis BRAIN 2021: 144; 2954–2963 | 2957
Table 1 Current evidence on the correlation and prediction of clinical and MRI parameters by sNfL levels
Parameter Level of Key results
evidence
Cross-section correlation
+++
Relapses and T1-gadolinium Relapses and gadolinium-enhancing lesions causing acute neuronal damage are the
enhancing lesions most important driver of sNfL peaks. It is currently unclear whether blood-brain
barrier damage in acute lesions facilitates efflux of sNfL proteins into the peripheral
blood thereby resulting in higher absolute levels.8,9,15,21,23,43,44
++
EDSS Large well-powered studies have clarified that sNfL and current EDSS scores are weak-
ly, yet significantly correlated. Furthermore, multiple studies have confirmed higher
levels at later disease stages compared to earlier stable patients. Studies showing
no correlation are most likely underpowered.8,21,23
++
New T2 lesions Both the occurrence and number of new T2-weighted lesions raise sNfL levels.9,21,23,43
Downloaded from https://academic.oup.com/brain/article/144/10/2954/6310737 by guest on 16 December 2021
+
T1-hypointense lesions Not as well studied, but was positively correlated in a few smaller studies.9,46
+
Existing T2 lesion load sNfL and number or volume of existing T2 lesions were significantly correlated in
some studies, whereas no correlation was found in others. As sNfL indicates acute
ongoing axonal damage, existing lesions without ongoing pathology are less likely
to contribute to sNfL level increase.8,23,47
+++
Relapses and EDSS increase in High sNfL levels were consistently associated with an increased risk for relapses in
the next 1–3 years the next years. Some studies indicate that the sNfL percentile category reflects the
strength of this prediction.21,23,48–50
Prediction
++
Brain and spinal cord volume High sNfL levels are associated with future brain and spinal cord volume loss on a
loss in the next 2–5 years group level. It is plausible that high sNfL levels precede visual structural alterations
in MRI, while exact time frames are still unclear.46,49,51
+
Long-term EDSS progression The long-term predictive value of sNfL values is so far not consistent in all studies.
(45 years) and SPMS While it is likely that investigations from further studies will bring more clarity,
conversion sNfL will probably be more useful in clinical situations with regards to prediction of
the next 1–3 years.24,48,51–56
+ = non-replicated observations that require further study or conflicting evidence.
+ + = observations that have been replicated and/or supported by independent methods.
+ + + = high level of evidence from larger studies, consistently replicated.
in laboratories may still influence results (Box 1). Precisely defined Nevertheless, another study confirmed the main finding that CSF
progression states in large patient cohorts may clarify the exact NfL is higher in multiple sclerosis patients with cognitive impair-
value of sNfL, reflecting gradual degenerative processes, since ment and especially in those with impaired information process-
even patients classified as having RRMS can suffer from disability ing speed and verbal fluency, assessed by the Brief Repeatable
increase in relapse-free phases of the disease (so-called ‘progres- Battery of Neuropsychological Tests (BRBN).64 Another interesting
sion independent of relapse activity’, PIRA61). Overall, sNfL is most concept is that high sNfL might (probably due to relapses or new
likely a predictor for brain atrophy and a milder predictor for long- gadolinium-enhancing lesions) precede short-term changes in
term EDSS development over several years; however, so far, it is cognitive parameters: data from the phase III EXPAND trial (siponi-
not an irrefutable predictor for conversion to SPMS. mod versus placebo in patients with SPMS) showed that patients
with high baseline sNfL levels had a 40% greater risk of 6-month
SDMT worsening than patients with low sNfL values.65 Overall,
Relationship between serum NfL and while initial data do indeed point towards an association between
cognitive impairment sNfL and measures of cognitive impairment, sNfL as a marker of
axonal damage will probably not be useful as a singular specific
A limited number of studies thus far have investigated the associ-
marker for cognitive damage in patients with multiple sclerosis.
ation between NfL and cognition in multiple sclerosis. A small
This notion is further supported by pathological concepts prefer-
study in 27 patients did not find correlations between sNfL levels
entially linking grey matter damage and network dysfunction to
and symbol digit modalities test (SDMT) scores after 1 and 10 years,
cognitive impairment.66,67 Further studies should therefore focus
while other studies demonstrated an association between serum
on developing multi-modal approaches integrating sNfL levels
and CSF NfL levels and lower verbal fluency performance or SDMT
with MRI data and other molecular biomarkers indicative of grey
scores.52,62,63 In one larger study using BICAMS (Brief International
matter damage (see also below).
Cognitive Assessment for Multiple Sclerosis), cognitively impaired
patients with multiple sclerosis had higher sNfL levels and a
greater longitudinal sNfL increase compared with non-cognitively Combination of serum NfL with other
impaired patients.51 Limitations of this study include the heteroge-
neous study cohort (mixed CIS, RRMS and SPMS patients) with
markers
quite low inflammatory activity, the use of binary categorizations As sNfL specifically reflects neuroaxonal damage, the addition of
of both BICAMS and sNfL based on cut-off values (‘normal’ versus one or several other markers might give a broader view of the
‘not-normal’), and the fact that cognitively impaired and non- pathophysiological processes in multiple sclerosis. Indeed, a num-
cognitively impaired patients varied in a number of parameters ber of studies have started to investigate whether sNfL composite
that potentially impact sNfL levels (e.g. age and EDSS). scores are able to outperform single biomarkers.2958 | BRAIN 2021: 144; 2954–2963 S. Bittner et al.
Glial fibrillary acidic protein (GFAP) is the major cytoskeleton that sNfL is not impacted by sex in healthy cohorts or in patients
protein in astrocytes and released upon changes in cellular integrity. with multiple sclerosis.25 However, the physiological increase in
GFAP is drawing increased research interest as a second major blood sNfL levels seen with ageing in healthy individuals54,79,80 needs to be
biomarker that can reliably be measured in serum samples and that taken into consideration when interpreting sNfL data. The strength
is moderately correlated with sNfL.68,69 Early studies in patients of the association between age and sNfL levels seems to be depend-
with multiple sclerosis suggested that GFAP is not elevated in asso- ent on the specific age of the investigated cohort as well as the
ciation with acute relapses and focal inflammatory infiltrates, and underlying disease. In both a meta-analysis and independent cohort
hence could be used to elucidate the ongoing glial-driven neurode- studies in multiple sclerosis, no clear association between CSF NfL
generative pathology.68,70 Indeed, using diffusion tensor imaging as levels and age was observed for patients with multiple sclerosis, in
a means to assess diffuse neuroaxonal damage not visible in con- contrast with healthy controls or people with most neurodegenera-
ventional MRI, it has recently been shown that both T2 lesions and tive disorders.6,21,47,54 It is plausible that the increase in sNfL levels
diffuse damage contribute to sNfL levels, and that the latter was observed in healthy controls (e.g. due to age-related neuronal loss or
preferentially found in older patients with more advanced disease preclinical age-related disorders) is masked by the higher baseline
course.71 These concepts were further expanded by efforts combin- inflammatory activity regularly observed in younger patients with
Downloaded from https://academic.oup.com/brain/article/144/10/2954/6310737 by guest on 16 December 2021
ing sNfL with GFAP, emphasizing that a combination of both multiple sclerosis. Thus, compared with inflammatory-associated
markers might be useful in differentiating RRMS from SPMS elevations, the age-dependency of sNfL may not be a relevant con-
patients.69 This notion is supported by an independent report that founder in clinical practice in younger patients without comorbid-
assessed GFAP and chitinase-3-like protein 1 (CHI3L1) as markers of ities. Some studies took the approach of modelling the ‘normal’ sNfL
astrocytic and microglial activation. A simplified ‘glia score’ (GFAP distribution across different ages based on a matched healthy donor
CHI3L1 / sNfL) was higher in SPMS versus RRMS patients and corre- control cohort,8,23,79 but unfortunately, different normative sNfL
lated with EDSS values only in SPMS patients.72 These studies are values were reached in each study despite being from the same
also interesting as they are in line with the concept that glia activa- laboratory.
tion is closely linked with axonal damage and disability progression
in multiple sclerosis. Assessing both sNfL and GFAP simultaneously
might be useful for differentiating multiple sclerosis activity across Serum NfL as a biomarker of treatment
different stages of the disease. response in multiple sclerosis: towards
Other approaches have assessed the combination of sNfL and personalized immunotherapy
markers of B cell activity in light of the recent appreciation of
(intrathecal) B cells as drivers of multiple sclerosis pathology.73 In an early study, CSF NfL levels in patients with multiple sclerosis
Patients that are positive for oligoclonal bands have higher serum were reduced to the levels of healthy controls 6 to 12 months after
and CSF NfL levels in comparison with oligoclonal band-negative treatment initiation with natalizumab, providing for the first time
patients.74,75 In one study of 142 patients, sNfL values were associ- evidence that that: (i) NfL levels increase upon acute inflammatory
ated with CSF total CD80 + (i.e. B cells and myeloid cells) as well as attacks; and (ii) a subsequent control of inflammatory disease ac-
CD80 + CD19 + (i.e. B cells) frequency.47 Patients with early multiple tivity with an immunomodulatory drug reduces NfL levels back to
sclerosis were stratified into probable benign and aggressive dis- baseline levels.81 Since then, a broad number of studies have con-
ease courses based on MRI criteria, and the investigators found firmed that sNfL values from patients receiving immunomodula-
that combining sNfL with CD20 + /CD14 + ratios in the CSF tory drugs are generally lower than untreated patients and that
(i.e. increased B cell frequency) considerably improved distinction initiation of any treatment is associated with a decrease in sNfL
between the groups compared to sNfL alone.76 levels.8,9,15,21,24,82,83
As elaborated above, sNfL strongly reflects (focal) acute inflam- Early studies suggest that sNfL levels might be able to differenti-
matory axonal damage of the white matter and its clinical value ate between different treatments at a patient group level. In one
might be extended by combination with other biomarkers indicating study, patients who changed treatment between disease-modifying
gradual grey matter damage. Parvalbumin is a protein expressed in therapies with similar efficacy had stable sNfL concentrations, while
GABAergic interneurons and has been proposed as a marker of cor- patients who escalated to therapies with higher efficacies had
tical grey matter neurodegeneration in patients with multiple scler- decreased sNfL concentrations after a median follow-up of
osis.77,78 A reduction in CSF parvalbumin correlated with meningeal 12 months.15 However, it should be noted that this study cohort of
inflammation, cortical lesion load, cortical thickness and cognitive multiple sclerosis patients was quite heterogeneous and that no
impairment; all of which possibly showed a better correlation of data on T2 lesions was available. Confirming and extending these
gradual degenerative pathology than NfL levels. Extending these findings, patients starting highly active immunotherapies have
findings in larger, multicentre longitudinal studies is warranted to higher sNfL levels at treatment initiation than those starting on
assess a possible combination of both biomarkers. mild/moderate therapies, leading to a larger relative decrease after
In summary, combining sNfL with other biomarkers reflecting commencing therapy.21,24,63 The number of future therapy changes,
glial activation, intrathecal inflammation or grey matter pathology as well as treatment escalations were predicted by baseline sNfL lev-
is highly promising. The integration of a multi-modal biomarker els.21,24 Another well-powered study assessed registry data from
assessment of multiple sclerosis pathology must still be investi- 1261 patients on different disease-modifying therapies and after
gated in large cohorts and in international efforts. using inverse propensity score weighting to correct for differences
in baseline factors, confirmed a similar picture: patients starting
alemtuzumab displayed the highest reduction and lowest on-treat-
Serum NfL in multiple sclerosis: ment sNfL levels, while patients on teriflunomide started from
considerations of age as a potential lower levels, had a smaller decrease in sNfL and higher on-treat-
ment levels.63 These studies underscore that repetitive measure-
confounder ments and evaluating longitudinal changes in sNfL will likely be an
An important point that needs to be considered when implementing important part of supporting and managing therapy decisions.
the use of sNfL in clinical practice is the difficulty in developing nor- After broadly introducing SIMOA assays, sNfL levels were analysed
mative values. Reassuringly, consistent reports have demonstrated retrospectively from stored samples of completed randomized clinicalSerum NfL as biomarker for multiple sclerosis BRAIN 2021: 144; 2954–2963 | 2959
trials. In phase 3 trials of fingolimod, natalizumab and alemtuzumab, sNfL is that it is stable in fresh and frozen blood samples and is
sNfL reflected the same benefit with therapy initiation as clinical and not affected by thawing cycles or storage time, opening the door
MRI parameters.56,84 Subsequently, a recent study simulated whether for a broad range of applications. From a technical viewpoint, the
sNfL could serve as an end point in phase 2 studies in patients with next challenges in the sNfL field are to establish age- and comor-
multiple sclerosis. Assuming typical features of a phase 2 trial in bidity-adjusted normative values and to ensure methodological
RRMS (6 months, 90% power, 5% significance level) and taking into ac- harmonization across different laboratories (see Box 3 and Table 2
count sNfL data from the FREEDOMS trial, between 28 and 143 sub- for recommendations on quality controls). From a clinical point of
jects per arm would have been needed to show a 20–40% reduction in view, the two questions ‘When’ and ‘How’ are of utmost relevance:
sNfL levels.85 Although the calculated numbers sound realistic, no tri- When should sNfL be measured and how should findings be inte-
als utilizing such a design have been performed to date, but this may grated into clinical decision-making? Because of the high inter-in-
change in the near future. In the ASCLEPIOS trial (ofatumumab versus dividual distribution of sNfL levels, we postulate longitudinal
teriflunomide), sNfL was included for the first time prospectively as a intra-individual changes being the most appropriate application
secondary end point in a phase 3 multiple sclerosis trial. Interestingly, for assessing clinical activity and treatment responses. Given the
sNfL levels were significantly different between both groups, whereas ongoing expansion of the therapeutic landscape in multiple scler-
Downloaded from https://academic.oup.com/brain/article/144/10/2954/6310737 by guest on 16 December 2021
brain atrophy rates were not, raising questions about the underlying osis, sNfL could support individualized decision-making. From a
causes for this discrepancy.86 It is plausible that short-term sNfL clinical standpoint, longitudinal sNfL assessments of patients with
changes might rather reflect inflammatory processes in multiple RRMS can support therapeutic decisions in key areas including:
sclerosis and changes are therefore evident earlier than MRI-based (i) initial classification of CIS versus RRMS; (ii) choice of initial
brain atrophy. As sNfL is included in most upcoming larger clinical tri- treatment; (iii) evaluation of subclinical disease activity in parallel
als, more insight will be obtained in the future. with MRI measurements; (iv) treatment escalation in clinically ac-
tive patients; and (v) treatment de-escalation or treatment cessa-
tion (Fig. 1 and Table 3). Importantly, sNfL measurement needs to
Conclusions and future directions be considered in a comprehensive and context-specific manner to-
In recent years, numerous studies have linked sNfL with outcomes gether with clinical information and other MRI markers of disease
related to disease activity, disability progression, treatment re- activity. While sNfL may indeed become the first blood biomarker
sponse and prognosis in patients with multiple sclerosis, generat- with relevance in multiple sclerosis monitoring, multimodal com-
ing convincing evidence that sNfL may soon be broadly used as posite indices integrating existing or other emerging markers
the first blood-based biomarker monitoring disease activity and could enable increasingly precise individualized treatment
treatment responses in clinical practice. One major advantage of decisions.
Box 3 Key challenges
• To clarify when and how often sNfL should be measured to assess subclinical disease activity and guide therapeutic decisions.
• To define the threshold that constitutes a clinically meaningful change in longitudinal measurements.
• To clarify whether absolute values are comparable in standardized investigations.
• To implement the standardization of neurofilament measures and values across different assays and laboratories.
• To take confounding factors (e.g. age and other comorbidities) into account. It should be clarified whether it is sufficient to
consider age exclusively in elderly cohorts (460 years) as the association with sNfL is weak in younger patients with RRMS.
Table 2 Suggested quality criteria to support the validity of measurements
Checkpoint Quality criteria
Replicate measurements Calibrators and samples should be measured at least in duplicates. Samples with a missing result for a repli-
cate or a CV of duplicate determination 420% should be measured again. The number of samples with
repeated measurements due to quality criteria should be reported in the method section.
Intra-assay precision Mean CV of duplicate determinations should be reported. Intra-assay CVs below 10% can usually be
achieved.
Control samples Three (pre-characterized) control samples with low, medium and high NfL concentrations should be
included in each run to monitor any matrix effects and to determine the inter-assay CV. Control samples
should preferably be derived from the same material as samples (e.g. serum, plasma or CSF).
Inter-assay precision Inter-assay CV should be reported. Values below 10% can usually be achieved and may reduce the risk of
reporting plate effects instead of true group effects.
Different LOTs or assay versions Inter-LOT effects should be negligible. However, caution is advised with different assay versions. If different
LOTs were used this should be announced in the method section and the inter-LOT CV should be
reported.
Blinding Individuals performing the NfL measurements should be blinded to clinical data.
Note that the recommendations apply to the first broadly used commercially available platform (NfL-lightTM assays, Quanterix, HD-1/HD-X). CV = coefficient of variation.2960 | BRAIN 2021: 144; 2954–2963 S. Bittner et al.
Downloaded from https://academic.oup.com/brain/article/144/10/2954/6310737 by guest on 16 December 2021
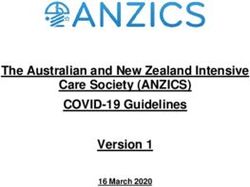
Figure 1 Potential sNfL decision concepts in clinical practice. (A) Longitudinal sNfL assessment algorithm guiding treatment optimization in RRMS.
Red fields mark four areas using sNfL for guiding decisions in (i) initial diagnosis of multiple sclerosis; (ii) choice of initial treatment; (iii) evaluation of
subclinical disease activity; and (iv) treatment optimization in clinically active patients. (B) An sNfL assessment algorithm in patients undergoing
treatment cessation or de-escalation, stratifying patients with stable disease course and those in need of therapy reinitiation or re-escalation. Note
that First, no randomized controlled trials have directly addressed the question of whether or when to discontinue treatment in RRMS patients who
have no evidence of relapses, no disability progression and stable MRI parameters. Especially in patients on higher-efficacy therapies (e.g. natalizu-
mab or fingolimod), the risk of return of disease activity or rebound when stopping treatment has been well documented. In agreement with the
European and American Academy of Neurology (AAN) guidelines,87 this algorithm is not suggesting treatment cessation in specific patient cohorts,
but rather is an approach to implement sNfL in ongoing follow-ups and periodic re-evaluations when treatment cessation occurs for clinical reasons.
Second, the suggested differentiation into NfLHIGH, NfLINTERMEDIATE and NfLLOW is a rough estimation based on our datasets and data from Table 3.
These values apply to RRMS patients (age 18 to 40–50 years) without comorbidities and are currently only partially validated within international
efforts. Older age groups still have to be compared to normal cohorts, since the age-associated sNfL increase seems to be markedly steeper beyond
about 50 years of age and is less studied up to date. cMRI = cranial MRI; NEDA = no evidence of disease activity; OCB = oligoclonal bands; RIS = radio-
logically isolated syndrome; sMRI = spinal cord MRI.Serum NfL as biomarker for multiple sclerosis BRAIN 2021: 144; 2954–2963 | 2961
Table 3 Corrected reference values for sNfL levels for two clinically relevant scenarios
Parameter Reported values Corrected values
MS versus healthy controls 9.7 pg/ml (age 18–40 years; sNfL 495th percentile of healthy cohort)26 9.7 pg/ml
29.3 pg/ml (age 30 years, sNfL 4 95th percentile of healthy cohort)23 14.7 pg/mla
27.9 pg/ml (age 30 years, sNfL 4 95th percentile of healthy cohort)8 14.0 pg/mla
14.4 pg/ml versus 8.5 pg/ml (pooled study data patients versus healthy 14.4 pg/ml versus 8.5 pg/ml
controls)84
11.4 pg/ml versus 7.5 pg/ml (MS patients versus healthy controls)54 14.3 pg/ml versus 9.4 pg/mlb
17.0 pg/ml versus 8.2 pg/ml (MS patients versus healthy controls)88 17.0 pg/ml versus 8.2 pg/ml
10.1 pg/ml versus 7.3 pg/ml (MS patients versus healthy controls)55 10.1 pg/ml versus 7.3 pg/ml
Serum NfL comparisons indi- 25.0–45.1 pg/ml (median; presymptomatic to symptomatic)37 12.5–22.5 pg/mla
cating disease activity in MS 29.6–43.4 pg/ml (median; no Gd + lesion to Gd + lesion)8 14.8–21.7 pg/mla
patients 28.9–39.3 pg/ml (median; no relapse to recent relapse 560 days)8 14.5–20.0 pg/mla
Downloaded from https://academic.oup.com/brain/article/144/10/2954/6310737 by guest on 16 December 2021
9.9–16.1 pg/ml (median; no Gd + lesion to Gd + lesion)21 9.9–16.1 pg/ml
28.1–63.2 pg/ml (median, no Gd + lesion to Gd + lesion)44 14.1–31.6 pg/mla
Note that when considering published data, there is a significant variation in data analysis procedures, making it difficult to systematically compare different studies. To
name a few challenges: published datasets have used mean, median, geomean, different parametric or non-parametric tests and cross-sectional or longitudinal analyses.
Analyses are performed either on raw data (non-parametric tests) or in log-transformed data in order to use parametric tests. While age-adjusted z-scores of log-transformed
data might indeed be the optimal statistical approach,26 this is challenging to implement in a broad clinical setting. Therefore, only reports publishing absolute values with
cut-offs were included. The presented data are only meant as a simplified approach for a rough range of expected values in two clinically relevant scenarios and not as vali-
dated cut-offs. Gd + = gadolinium-enhancing lesions; MS = multiple sclerosis.
a
Because of technical differences between different protocols, values are reduced by 50% to give a rough estimation. For full values and more details (e.g. interquartile range),
see the original publications.
b
Plasma concentrations are 25% lower than serum concentration (Thebault et al.26 and own experience), values were increased accordingly.
Search strategy and selection criteria Pharmaceuticals. M.T. is co-editor of Multiple Sclerosis Journal-
ETC. F.Z. has recently received research grants and/or consultation
We searched PubMed and Web of Science for articles on neurofila-
funds from DFG, BMBF, PMSA, MPG, Genzyme, Merck Serono,
ment published between 1 January 2018 and 15 May 2021. Search
Roche, Novartis, Sanofi-Aventis, Celgene, ONO and Octapharma.
terms were ‘neurofilament’, ‘neurofilaments’, ‘neurofilament light
chain’, ‘NfL’, ‘sNfL’, ‘PML’ and all combinations of these phrases with
‘multiple sclerosis’, ‘MS’ and ‘neuroinflammation’. The final reference References
list was generated based on novelty and relevance to this review.
1. Reich DS, Lucchinetti CF, Calabresi PA. Multiple sclerosis. N Engl
J Med. 2018;378(2):169–180.
Acknowledgements 2. Suthiphosuwan S, Kim D, Bharatha A, Oh J. Imaging markers for
monitoring disease activity in multiple sclerosis. Curr Treat
The authors thank Dr Cheryl Ernest for proofreading and editing the
Options Neurol. 2017;19(5):18.
manuscript. The thumbnail image was created with BioRender.com.
3. Khalil M, Teunissen CE, Otto M, et al. Neurofilaments as biomarkers
in neurological disorders. Nat Rev Neurol. 2018;14(10):577–589.
Funding 4. Uphaus T, Bittner S, Groschel S, et al. NfL (neurofilament light
chain) levels as a predictive marker for long-term outcome after
This work was supported by the German Research Council (DFG,
ischemic stroke. Stroke. 2019;50(11):3077–3084.
CRC-TR-128 to F.Z. and S.B.), Hertie-Stiftung (myLab to S.B.), the
5. Moseby-Knappe M, Mattsson N, Nielsen N, et al. Serum neurofi-
Progressive Multiple Sclerosis Alliance (PMSA, BRAVEinMS PA-
lament light chain for prognosis of outcome after cardiac arrest.
1604-08492 to F.Z.), and the German Federal Ministry of Education
JAMA Neurol. 2019;76(1):64–71.
and Research (BMBF, VIP + HaltMS to F.Z.). 6. Bridel C, van Wieringen WN, Zetterberg H, et al.; the NFL Group.
Diagnostic value of cerebrospinal fluid neurofilament light pro-
Competing interests tein in neurology: A systematic review and meta-analysis.
JAMA Neurol. 2019;76(9):1035.
S.B. has received honoraria and compensation for travel from 7. Aktas O, Renner A, Huss A, et al. Serum neurofilament light
Biogen Idec, Merck Serono, Novartis, Sanofi-Genzyme and Roche. chain: No clear relation to cognition and neuropsychiatric
J.O. has received funding from the MS Society of Canada, the symptoms in stable MS. Neurol Neuroimmunol Neuroinflamm.
National MS Society, Brain Canada, EMD-Serono, Roche and 2020;7(6):e885.
Biogen-Idec. J.O. has also received compensation for consulting or 8. Disanto G, Barro C, Benkert P, et al.; the Swiss Multiple Sclerosis
speaking engagements from Alexion, EMD-Serono, Sanofi- Cohort Study Group. Serum neurofilament light: A biomarker of
Genzyme, Biogen-Idec, Novartis, BMS, and Roche. E.K.H. has neuronal damage in multiple sclerosis. Ann Neurol. 2017;81(6):
received honoraria/research support from Biogen, Merck Serono, 857–870.
Novartis, Roche and Teva; has served as a member of advisory 9. Varhaug KN, Barro C, Bjornevik K, et al. Neurofilament light
boards for Actelion, Biogen, Celgene, Merck Serono, Novartis and chain predicts disease activity in relapsing-remitting MS. Neurol
Sanofi Genzyme; and has been supported by the Czech Ministry of Neuroimmunol Neuroinflamm. 2018;5(1):e422.
Education research, project PROGRES Q27/LF1. M.T. has received 10. Rosengren LE, Karlsson JE, Karlsson JO, Persson LI, Wikkelso C.
compensation for consulting services and speaking honoraria Patients with amyotrophic lateral sclerosis and other neurode-
from Almirall, Bayer Schering Pharma, Biogen-Idec, Genzyme, generative diseases have increased levels of neurofilament pro-
Merck-Serono, Novartis, Roche, Sanofi-Aventis, Viela Bio and Teva tein in CSF. J Neurochem. 1996;67(5):2013–2018.2962 | BRAIN 2021: 144; 2954–2963 S. Bittner et al.
11. Lycke JN, Karlsson JE, Andersen O, Rosengren LE. Neurofilament 31. Freedman M, Gnanapavan S. Letter to the Editor: Consensus
protein in cerebrospinal fluid: potential marker of activity in mul- statement on neurofilament proteins in multiple sclerosis
tiple sclerosis. J Neurol Neurosurg Psychiatry. 1998;64(3):402–404. under development by Consortium of Multiple Sclerosis
12. Rissin DM, Kan CW, Campbell TG, et al. Single-molecule enzyme- Centers (CMSC) expert panel. Int J MS Care. 2020;22(6):294.
linked immunosorbent assay detects serum proteins at subfem- 32. Chitnis T. Serum NFL levels should be used to monitor multiple
tomolar concentrations. Nat Biotechnol. 2010;28(6):595–599. sclerosis evolution-Commentary. Mult Scler. 2020;26(1):21–22.
13. Kuhle J, Barro C, Andreasson U, et al. Comparison of three analyt- 33. Kim H, Lee EJ, Kim S, et al. Serum biomarkers in myelin oligo-
ical platforms for quantification of the neurofilament light chain dendrocyte glycoprotein antibody-associated disease. Neurol
in blood samples: ELISA, electrochemiluminescence immuno- Neuroimmunol Neuroinflamm. 2020;7(3):e708.
assay and Simoa. Clin Chem Lab Med. 2016;54(10):1655–1661. 34. Peng L, Bi C, Xia D, Mao L, Qian H. Increased cerebrospinal fluid
14. Kuhle J, Barro C, Disanto G, et al. Serum neurofilament light neurofilament light chain in central nervous system inflamma-
chain in early relapsing remitting MS is increased and corre- tory demyelinating disease. Mult Scler Relat Disord. 2019;30:
lates with CSF levels and with MRI measures of disease severity. 123–128.
Mult Scler. 2016;22(12):1550–1559. 35. Watanabe M, Nakamura Y, Michalak Z, et al. Serum GFAP and
Downloaded from https://academic.oup.com/brain/article/144/10/2954/6310737 by guest on 16 December 2021
15. Novakova L, Zetterberg H, Sundstrom P, et al. Monitoring dis- neurofilament light as biomarkers of disease activity and dis-
ease activity in multiple sclerosis using serum neurofilament ability in NMOSD. Neurology. 2019;93(13):e1299–e1311.
light protein. Neurology. 2017;89(22):2230–2237. 36. Dalla Costa G, Martinelli V, Moiola L, et al. Serum neurofila-
16. Myhr KM, Torkildsen O. Serum NFL levels should be used to ments increase at progressive multifocal leukoencephalopathy
monitor multiple sclerosis evolution-No. Mult Scler. 2020;26(1): onset in natalizumab-treated multiple sclerosis patients. Ann
19–21. Neurol. 2019;85(4):606–610.
17. Altmann P, Leutmezer F, Zach H, et al. Serum neurofilament 37. Bjornevik K, Munger KL, Cortese M, et al. Serum neurofilament
light chain withstands delayed freezing and repeated thawing. light chain levels in patients with presymptomatic multiple
Sci Rep. 2020;10(1):19982. sclerosis. JAMA Neurol. 2019;77(1):58.
18. Keshavan A, Heslegrave A, Zetterberg H, Schott JM. Stability of 38. Matute-Blanch C, Villar LM, Alvarez-Cermeno JC, et al.
blood-based biomarkers of Alzheimer’s disease over multiple Neurofilament light chain and oligoclonal bands are prognostic
freeze-thaw cycles. Alzheimers Dement (Amst). 2018;10:448–451. biomarkers in radiologically isolated syndrome. Brain. 2018;
19. Comabella M, Montalban X. Body fluid biomarkers in multiple 141(4):1085–1093.
sclerosis. Lancet Neurol. 2014;13(1):113–126. 39. Miller DH, Chard DT, Ciccarelli O. Clinically isolated syndromes.
20. Housley WJ, Pitt D, Hafler DA. Biomarkers in multiple sclerosis. Lancet Neurol. 2012;11(2):157–169.
Clin Immunol. 2015;161(1):51–58. 40. Arrambide G, Espejo C, Eixarch H, et al. Neurofilament light
21. Bittner S, Steffen F, Uphaus T, et al.; KKNMS Consortium. chain level is a weak risk factor for the development of MS.
Clinical implications of serum neurofilament in newly diag- Neurology. 2016;87(11):1076–1084.
nosed MS patients: A longitudinal multicentre cohort study. 41. van der Vuurst de Vries RM, Wong YYM, Mescheriakova JY, et
EBioMedicine. 2020;56:102807. al. High neurofilament levels are associated with clinically def-
22. Bsteh G, Berek K, Hegen H, et al. Serum neurofilament levels inite multiple sclerosis in children and adults with clinically
correlate with retinal nerve fiber layer thinning in multiple isolated syndrome. Mult Scler. 2019;25(7):958–967.
sclerosis. Mult Scler. 2019;26(13):1682–1690. 42. Teunissen CE, Iacobaeus E, Khademi M, et al. Combination of
23. Barro C, Benkert P, Disanto G, et al. Serum neurofilament as a CSF N-acetylaspartate and neurofilaments in multiple sclerosis.
predictor of disease worsening and brain and spinal cord atro- Neurology. 2009;72(15):1322–1329.
phy in multiple sclerosis. Brain. 2018;141(8):2382–2391. 43. Dalla Costa G, Martinelli V, Sangalli F, et al. Prognostic value of
24. Canto E, Barro C, Zhao C, et al. Association between serum neu- serum neurofilaments in patients with clinically isolated syn-
rofilament light chain levels and long-term disease course dromes. Neurology. 2019;92(7):e733–e741.
among patients with multiple sclerosis followed up for 12 years. 44. Siller N, Kuhle J, Muthuraman M, et al. Serum neurofilament
JAMA Neurol. 2019;76(11):1359. light chain is a biomarker of acute and chronic neuronal dam-
25. Barro C, Chitnis T, Weiner HL. Blood neurofilament light: a crit- age in early multiple sclerosis. Mult Scler. 2019;25(5):678–686.
ical review of its application to neurologic disease. Ann Clin 45. Zipp F, Oh J, Fragoso YD, Waubant E. Implementing the 2017
Transl Neurol. 2020;7(12):2508–2523. McDonald criteria for the diagnosis of multiple sclerosis. Nat
26. Thebault S, Booth RA, Rush CA, MacLean H, Freedman MS. Rev Neurol. 2019;15(8):441–445.
Serum neurofilament light chain measurement in MS: hurdles 46. Srpova B, Uher T, Hrnciarova T, et al. Serum neurofilament light
to clinical translation. Front Neurosci. 2021;15:654942. chain reflects inflammation-driven neurodegeneration and
27. Kapoor R, Smith KE, Allegretta M, et al. Serum neurofilament predicts delayed brain volume loss in early stage of multiple
light as a biomarker in progressive multiple sclerosis. Neurology. sclerosis. Mult Scler. 2021;27(1):52–60.
2020;95(10):436–444. 47. Uher T, McComb M, Galkin S, et al. Neurofilament levels are
28. Kuhle J, Barro C, Hrusovsky K, Chang L, Jeromin A. International associated with blood-brain barrier integrity, lymphocyte ex-
multi-site analytical validation of the Simoa NF-light assay in travasation, and risk factors following the first demyelinating
human serum samples from multiple sclerosis patients. Mult event in multiple sclerosis. Mult Scler. 2020;27(2):220–231.
Scler. 2018;24:249–251. 48. Sellebjerg F, Royen L, Soelberg Sorensen P, Oturai AB, Jensen
29. Sharma A, Petrillo M, Zhao G, Unkown A, Unkown A. Strategic PEH. Prognostic value of cerebrospinal fluid neurofilament light
platform selection and validation of biomarker assays to meas- chain and chitinase-3-like-1 in newly diagnosed patients with
ure serum neurofilament light and heavy chain in multiple multiple sclerosis. Mult Scler. 2019;25(11):1444–1451.
sclerosis. Mult Scler. 2018;24:660–661. 49. Kuhle J, Nourbakhsh B, Grant D, et al. Serum neurofilament is
30. Gauthier A, Viel S, Perret M, et al.; OFSEP Investigators. associated with progression of brain atrophy and disability in
Comparison of Simoa(TM) and Ella(TM) to assess serum neuro- early MS. Neurology. 2017;88(9):826–831.
filament-light chain in multiple sclerosis. Ann Clin Transl Neurol. 50. Disanto G, Adiutori R, Dobson R, et al.; International Clinically
2021;8(5):1141–1150. Isolated Syndrome Study Group. Serum neurofilament lightSerum NfL as biomarker for multiple sclerosis BRAIN 2021: 144; 2954–2963 | 2963
chain levels are increased in patients with a clinically isolated 70. Norgren N, Sundstrom P, Svenningsson A, Rosengren L,
syndrome. J Neurol Neurosurg Psychiatry. 2016;87(2):126–129. Stigbrand T, Gunnarsson M. Neurofilament and glial fibrillary
51. Jakimovski D, Kuhle J, Ramanathan M, et al. Serum neurofilament acidic protein in multiple sclerosis. Neurology. 2004;63(9):
light chain levels associations with gray matter pathology: a 5- 1586–1590.
year longitudinal study. Ann Clin Transl Neurol. 2019;6(9):1757–1770. 71. Saraste M, Bezukladova S, Matilainen M, et al. High serum neu-
52. Chitnis T, Gonzalez C, Healy BC, et al. Neurofilament light chain rofilament associates with diffuse white matter damage in MS.
serum levels correlate with 10-year MRI outcomes in multiple Neurol Neuroimmunol Neuroinflamm. 2021;8(1):e926.
sclerosis. Ann Clin Transl Neur. 2018;5(12):1478–1491. 72. Huss A, Otto M, Senel M, Ludolph AC, Abdelhak A, Tumani H. A
53. Bhan A, Jacobsen C, Myhr KM, Dalen I, Lode K, Farbu E. score based on NfL and glial markers may differentiate between
Neurofilaments and 10-year follow-up in multiple sclerosis. relapsing-remitting and progressive MS course. Front Neurol.
Mult Scler. 2018;24(10):1301–1307.
2020;11:608.
54. Manouchehrinia A, Stridh P, Khademi M, et al. Plasma neurofi-
73. Bittner S, Ruck T, Wiendl H, Grauer OM, Meuth SG. Targeting B
lament light levels are associated with risk of disability in mul-
cells in relapsing-remitting multiple sclerosis: from patho-
tiple sclerosis. Neurology. 2020;94(23):e2457–e2467.
physiology to optimal clinical management. Ther Adv Neurol
Downloaded from https://academic.oup.com/brain/article/144/10/2954/6310737 by guest on 16 December 2021
55. Thebault S, Abdoli M, Fereshtehnejad SM, Tessier D, Tabard-
Disord. 2017;10(1):51–66.
Cossa V, Freedman MS. Serum neurofilament light chain pre-
74. Engel S, Steffen F, Uphaus T, et al. Association of intrathecal
dicts long term clinical outcomes in multiple sclerosis. Sci Rep.
pleocytosis and IgG synthesis with axonal damage in early MS.
2020;10(1):10381.
Neurol Neuroimmunol Neuroinflamm. 2020;7(3):e679.
56. Leppert D, Kuhle J. Blood neurofilament light chain at the door-
75. Farina G, Magliozzi R, Pitteri M, et al. Increased cortical lesion
step of clinical application. Neurol Neuroimmunol Neuroinflamm.
2019;6(5):e599. load and intrathecal inflammation is associated with oligoclo-
57. Magliozzi R, Howell OW, Nicholas R, et al. Inflammatory intra- nal bands in multiple sclerosis patients: a combined CSF and
thecal profiles and cortical damage in multiple sclerosis. Ann MRI study. J Neuroinflammation. 2017;14(1):40.
Neurol. 2018;83(4):739–755. 76. Engel S, Friedrich M, Muthuraman M, et al. Intrathecal B-cell ac-
58. Rosso M, Gonzalez CT, Healy BC, et al. Temporal association of cumulation and axonal damage distinguish MRI-based benign
sNfL and gad-enhancing lesions in multiple sclerosis. Ann Clin from aggressive onset in MS. Neurol Neuroimmunol Neuroinflamm.
Transl Neurol. 2020;7(6):945–955 2019;6(5):e595.
59. Dutta R, Trapp BD. Mechanisms of neuronal dysfunction and de- 77. Magliozzi R, Howell OW, Durrenberger P, et al. Meningeal inflam-
generation in multiple sclerosis. Prog Neurobiol. 2011;93(1):1–12. mation changes the balance of TNF signalling in cortical grey mat-
60. Jakimovski D, Zivadinov R, Ramanthan M, et al. Serum neurofi- ter in multiple sclerosis. J Neuroinflammation. 2019;16(1):259.
lament light chain level associations with clinical and cognitive 78. Magliozzi R, Pitteri M, Ziccardi S, et al. CSF parvalbumin levels
performance in multiple sclerosis: A longitudinal retrospective reflect interneuron loss linked with cortical pathology in mul-
5-year study. Mult Scler. 2019;26(13):1670–1681. tiple sclerosis. Ann Clin Transl Neurol. 2021;8(3):534–547.
61. Kappos L, Wolinsky JS, Giovannoni G, et al. Contribution of re- 79. Khalil M, Pirpamer L, Hofer E, et al. Serum neurofilament light
lapse-independent progression vs relapse-associated worsen- levels in normal aging and their association with morphologic
ing to overall confirmed disability accumulation in typical brain changes. Nat Commun. 2020;11(1):812.
relapsing multiple sclerosis in a pooled analysis of 2 random- 80. Vagberg M, Norgren N, Dring A, et al. Levels and age depend-
ized clinical trials. JAMA Neurol. 2020;77(9):1132–1140. ency of neurofilament light and glial fibrillary acidic protein in
62. Quintana E, Coll C, Salavedra-Pont J, et al. Cognitive impairment healthy individuals and their relation to the brain parenchymal
in early stages of multiple sclerosis is associated with high cere- fraction. PLoS One. 2015;10(8):e0135886.
brospinal fluid levels of chitinase 3-like 1 and neurofilament 81. Gunnarsson M, Malmestrom C, Axelsson M, et al. Axonal dam-
light chain. Eur J Neurol. 2018;25(9):1189–1191. age in relapsing multiple sclerosis is markedly reduced by nata-
63. Delcoigne B, Manouchehrinia A, Barro C, et al. Blood neurofila-
lizumab. Ann Neurol. 2011;69(1):83–89.
ment light levels segregate treatment effects in multiple scler-
82. Sejbaek T, Nielsen HH, Penner N, et al. Dimethyl fumarate
osis. Neurology. 2020;94(11):e1201–e1212.
decreases neurofilament light chain in CSF and blood of treat-
64. Gaetani L, Salvadori N, Lisetti V, et al. Cerebrospinal fluid neuro-
ment naive relapsing MS patients. J Neurol Neurosurg Psychiatry.
filament light chain tracks cognitive impairment in multiple
2019;90(12):1324–1330.
sclerosis. J Neurol. 2019;266(9):2157–2163.
83. Preziosa P, Rocca MA, Filippi M. Current state-of-art of the appli-
65. Kuhle J, Kropshofer H, Barro C, Unkown A, Unkown A. The pre-
cation of serum neurofilaments in multiple sclerosis diagnosis
dictive value of neurofilament light chain levels in blood for
and monitoring. Expert Rev Neurother. 2020;20(8):747–769.
cognitive impairment in patients with secondary progressive
84. Kuhle J, Kropshofer H, Haering DA, et al. Blood neurofilament
multiple sclerosis (S12.009). Neurology. 2019;92:S12.009
66. Fleischer V, Muthuraman M, Anwar AR, et al. Continuous reorgan- light chain as a biomarker of MS disease activity and treatment
ization of cortical information flow in multiple sclerosis: A longitu- response. Neurology. 2019;92(10):e1007–e1015.
dinal fMRI effective connectivity study. Sci Rep. 2020;10(1):806. 85. Sormani MP, Haering DA, Kropshofer H, et al. Blood neurofila-
67. Geurts JJ, Calabrese M, Fisher E, Rudick RA. Measurement and ment light as a potential endpoint in phase 2 studies in MS. Ann
clinical effect of grey matter pathology in multiple sclerosis. Clin Transl Neurol. 2019;6(6):1081–1089.
Lancet Neurol. 2012;11(12):1082–1092. 86. Fyfe I. Trials take MS treatment forward. Nat Rev Neurol. 2019;
68. Abdelhak A, Huss A, Kassubek J, Tumani H, Otto M. Serum GFAP 15(11):620.
as a biomarker for disease severity in multiple sclerosis. Sci Rep. 87. Bittner S, Zipp F. AAN unveils new guidelines for MS disease-
2018;8(1):14798. modifying therapy. Nat Rev Neurol. 2018;14(7):384–386.
69. Hogel H, Rissanen E, Barro C, et al. Serum glial fibrillary acidic 88. Piehl F, Kockum I, Khademi M, et al. Plasma neurofilament light
protein correlates with multiple sclerosis disease severity. Mult chain levels in patients with MS switching from injectable
Scler. 2020;26(2):210–219. therapies to fingolimod. Mult Scler. 2018;24(8):1046–1054.You can also read