The role of the surgeon in the management of melanoma
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
MINERVA CHIR 2006;61:141-54
The role of the surgeon in the management
of melanoma
M. S. SABEL, A. ARORA
While multimodality therapy has become the Department of Surgery, University of Michigan
standard for most solid tumors, the mainstay of Comprehensive Cancer Center
therapy for melanoma remains surgical. This Ann Arbor, MI, USA
includes not only early stage disease, but
advanced melanoma as well. The surgical
approach to melanoma has changed dramati-
cally, with a trend towards less aggressive resec-
tion of the primary tumor, and towards a more ment of melanoma. Similarly, despite a
aggressive approach to regional and metastat- tremendous interest in their potential for treat-
ic disease. Melanoma surgery has been altered
by our knowledge of the biology of the disease, ment, biologic and immunologic therapies
and the results of well-designed, prospective have not to date significantly impacted out-
randomized trials. Conversely, new surgical comes in melanoma. Surgery thus remains
approaches have expanded our understand- the primary treatment for both thin, local-
ing of melanoma biology, and new random- ized malignant melanoma as well as for
ized trials are needed to further define the opti- advanced melanoma.
mal surgical approach. This article will review
the evolution of melanoma surgery and the While the need for surgery has remained
evidence behind today’s recommendations. constant, the nature of that surgery has
Key words: Melanoma - Surgery - Sentinel lymph changed considerably over that time. It cur-
node - Lymph node biopsy. rently targets 3 arms of treatment: the pri-
mary tumor, the nodal basin, and when fea-
sible, stage IV disease. Historically, treatment
of the primary tumor began with narrow exci-
C ancer has evolved over the past century
from existing as primarily a surgical dis-
ease to one treated in this day by a multidis-
sion. Review of outcomes, and high rates of
local and regional recurrence, led next to
ciplinary approach. Today, few solid tumors, wide radical excisions, but failure to improve
with the exception of the earliest-stage dis- overall survival led to a reversion back to
ease, are treated by surgery alone. Melanoma moderate margins. Management of the
stands out as an exception at all stages. regional nodal basin has also evolved and
Mainstays in the therapy of most malignan- continues to be a source of controversy
cies, chemotherapy and radiation therapy among clinicians. Even further, the role of
play extremely limited roles in the manage- surgery in stage IV disease is expanding
beyond palliation towards curative extirpa-
tion.
Address reprint requests to: M. S. Sabel, MD, FACS 3304 These changes in the surgical management
Cancer Center, 1500 East Medical Center Drive, Ann Arbor, MI
48109. E-mail: msabel@umich.edu of melanoma have been the result of both
Vol. 61, N. 2 MINERVA CHIRURGICA 141SABEL THE ROLE OF THE SURGEOAN IN THE MANAGEMENT OF MELANOMA
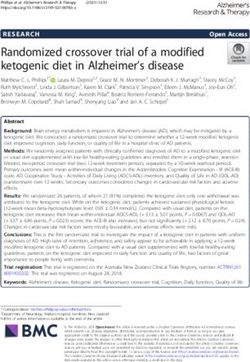
TABLE I.—Randomized trials of wide versus narrow excision for malignant melanoma.
Trial Author No. Breslow depth Arms Follow-up Outcomes
World Health Organization, Veronesi 9, 10 612 ≤2 mm 1 cm vs 3 cm 8 years NSD
Melanoma Program 10 OS, DFS, LRR
Intergroup Melanoma Surgical Trial Balch 11, 12 486 1-4 mm 2 cm vs 4 cm 10 years NSD
OS, LRR
Swedish Melanoma Group Ringborg 13, 14 989 0.8-2 mm 2 cm vs 4 cm 11 years NSD
OS, DFS, LRR
United Kingdom Melanoma Thomas 15 900 > 2 mm 1 cm vs 3 cm 5 years NSD OS
Study Group
? LRR with
1 cm (P=0.05)
HR=1.26
French Cooperative Group Banzet 16 319 ≤2 mm 2 cm vs 5 cm 4 NSD
OS, DFS
OS: overall survival; DFS: disease-free survival; LRR: local-regional recurrence; NSD: no significant difference; HR: hazard ratio
our increased knowledge of the natural biol- including the fascia with the resection spec-
ogy of this disease and prospective, ran- imen.
domized trials designed to answer specific The definition of an adequate margin for
questions regarding specific treatment wide radical excision has changed over time.
options. This article will review the role of In 1907, Handley recommended a margin of
surgery in the management of cutaneous 1 inch. This was based both on the failure of
melanoma, the evidence behind our current the present approaches to cure the disease
practice, and the questions that remain. and on microscopic examination of strips of
adjacent tissue from autopsy studies.5, 6 In
the later half of the 20th century, the recom-
Surgery and the primary melanoma mended margins increased to 4 or 5cm based
on the discovery of melanocytes and
Excisional biopsy of melanoma with nar- microsatellites beyond the excision site.7, 8 In
row and negative margins is inadequate treat- some cases, this involved a radical en bloc
ment, associated with local recurrence rates resection of the regional nodal basins.
in the range of 30% to 60%.1 Since first This radical excision, despite the morbidity
described by William Norris in 1857, the wide involved, remained the treatment for
radical excision has remained the mainstay of melanoma until an interest in gathering sci-
therapy for localized melanoma.2 Wide rad- entific data to support these recommenda-
ical excision consists of excising an adequate tions via clinical trials emerged. Five ran-
margin of normal appearing skin down to domized trials demonstrated no difference in
underlying fascia. Historically, the muscular survival between conservative margins and
fascia was excised with the specimen. There wide margins (Table I 9-16). However, the stud-
existed some belief, however, that removing ies differed greatly in both the entry criteria and
the fascia might promote the dissemination of the margins of excision. Three trials compared
tumor cells and increase the recurrence rate.3 2 cm margins to either 4 cm or 5 cm margins,
Although this has never been addressed in a while 2 trials compared 1 cm margins with 3
prospective trial, a retrospective trial of 202 cm margins. Our present recommendations
patients showed no difference in recurrence are based on the data from these randomized
with the removal of the fascia.4 Current prac- trials, with the margin of excision based on
tice involves dissection down to, but not the Breslow thickness of the primary tumor.
142 MINERVA CHIRURGICA Aprile 2006THE ROLE OF THE SURGEOAN IN THE MANAGEMENT OF MELANOMA SABEL
Resection margins for thin (2 mm
612 patients with melanomas less than 2 mm randomized between 1 and 3 cm margins
thick to receive excision with either 1 cm performed by the UK Melanoma Study
(narrow) or 3 cm (wide) margins.9, 10 In the Group, the British Association of Plastic
group of patients who had melanoma 2 mm risk of locoregional recurrence with 1 cm
Most of the trials included thicker margins. It also suggested that this margin
melanomas. A multi-institutional prospective may be associated with increased mortality.
randomized trial from France demonstrated Based on these results, the trial concluded
no difference in either local recurrence rate that a margin of 1 cm is inadequate for
or survival between patients who had a 5 cm melanomas greater than 2 mm in Breslow
margin or a 2 cm margin.16, 17 This trial includ- thickness. Notably, though, the increased
ed 319 patients with melanomas 2 mm or recurrence rate was primarily restricted to
greater in thickness. regional recurrences in the draining nodal
The Intergroup Melanoma Committee con- basin. It is unclear whether this risk would still
ducted a randomized prospective study eval- exist today with the routine application of
uating 2 cm versus 4 cm margins in 468 lymphatic mapping and sentinel lymph node
patients with intermediate thickness melano- biopsy (SLNB).
mas (1-4 mm).11, 12 There was a statistically The margins of excision necessary for
significant difference in the need for skin melanomas greater than 4 mm remains con-
grafts between the groups, with 46% of the 4 troversial, as this population was not repre-
cm group requiring skin grafts versus 11% of sented in the randomized trials. While a more
the 2 cm group. With a ten-year median fol- aggressive surgical resection may be war-
low-up, there was no significant difference in ranted given the known biologic aggressive-
recurrence between the groups. ness of thick melanomas, this must be tem-
The Swedish Melanoma Study Group com- pered against the higher propensity of these
pared 2 cm versus 5 cm margins of excision lesions to have already metastasized, mini-
in 989 patients with melanomas between 0.8 mizing the impact of local control on overall
and 2 mm thick. There were local recurrences survival. The optimum approach for this
in 1% of patients, equally distributed between group has yet to be well determined, but the
the 2 study arms, and no differences in recur- present recommendations are margins of at
rence-free or overall survival.13 least 2 cm.
Cumulatively, these studies all demonstrate
that a 2 cm margin for intermediate-thick-
Resection margins for melanoma between 1
ness melanomas (1-4 mm) is appropriate to
and 2 mm
significantly minimize the risks of both recur-
rence and the need for skin grafting. These The randomized trials demonstrate that
studies do not, however, answer the question melanomas less than 1 mm can be safely
Vol. 61, N. 2 MINERVA CHIRURGICA 143SABEL THE ROLE OF THE SURGEOAN IN THE MANAGEMENT OF MELANOMA
TABLE II.—Recommended margins of excision for pri- diagnosis.18 Patients who have previously
mary melanoma. undergone a wide excision may recur with
Melanoma in situ 0.5 cm palpable adenopathy evident on exam, and
Less than or equal to 1 mm 1 cm occasional patients present with nodal metas-
1 to 2 mm 1 to 2 cm tases in the absence of a detectable primary
2 to 4 mm 2 cm
> 4 mm at least 2 cm
melanoma. Palpable enlarged nodes (gener-
ally 1-1.5 cm in maximum diameter), or nodes
that are hard or fixed to adjacent structures
must be considered suspicious for metastat-
resected with a 1 cm margin, and that ic involvement. Metastatic nodal involvement
melanomas >2 mm should be resected with should be verified with a fine needle aspira-
a minimum of a 2 cm margin. What about tion (FNA) biopsy. Excisional biopsy is
melanoma between 1 and 2 mm? While the reserved for those situations where the lymph
studies show that 2 cm margins are appro- node is clinically suspicious but the FNA
priate, there is little data to answer whether biopsy results are inconclusive.
1 cm margins would be appropriate. The Complications of an open biopsy (sero-
only study of 1 cm versus 3 cm margins that ma, infection, scarring) can interfere with the
included patients with melanoma between performance of the subsequent lymph node
1 and 2 mm melanoma was the World Health dissection. Previous interventions in the
Organization Melanoma Group trial. As regional basin have also been associated with
described above, this trial included patients
an increase in melanoma recurrence after
melanomas less than 2 mm thick to receive
radical dissection.19 For both oncologic and
excision with either 1 cm (narrow) or 3 cm
functional reasons, if an excisional biopsy is
(wide) margins.9, 10 While there were no local
performed, the incision should be oriented in
recurrences among patients with melanomas
a way that it can be readily re-excised duringTHE ROLE OF THE SURGEOAN IN THE MANAGEMENT OF MELANOMA SABEL
PET scanning is superior to CT scans, while removal of the fat pad improves survival, this
others have suggested the false-positive rates procedure is not routinely recommended.
for PET imaging is too high to make it a reli- Lymphedema remains the most common
able choice. CT scanning has the additional complication of ALND. While many surgeons
advantage of providing additional anatomic skeletonize the axillary vein during the dis-
information that the surgeon may find useful section, others have suggested that this may
to plan the dissection. One example in par- increase the rate of lymphedema. Lawton et
ticular would be the presence of enlarged al.27 proposed preservation of the fascia from
pelvic lymph nodes; this finding might well the pectoralis and latissimus dorsi muscles
convert an inguinal node dissection to an ili- to decrease postoperative lymphedema.
ac-inguinal node dissection. Definitive studies addressing variations in
technique and their impact on outcome have
AXILLARY LYMPH NODE DISSECTION not been performed. In experienced hands,
the lymphedema rate after ALND should be
For patients with palpable disease in the between 5% and 12%.24, 28, 29
axilla, the axillary lymph node dissection
(ALND) should include levels I, II, and III
GROIN DISSECTION
nodes to provide the best regional control.
Some surgeons, however, include level III Groin dissections are associated with a
only when suspicious nodes are present.23-25 In much higher overall complication rate; 50%
a thin patient, with adequate mobilization and to 64% compared to 14% to 17% for axillary
anterior retraction of the pectoralis major and lymph node dissection.30, 31 More than 20% of
minor muscles, it may be possible to ade- patients will have chronic lymphedema.32-34
quately dissect the level III nodes without Wound complications, including skin flap
dividing the pectoralis minor muscle. This may necrosis, wound dehiscense and surgical site
involve dissection between the pectoralis infections, are quite common.
major and minor muscles to adequately For patients with inguinal disease, the
include the level III nodes, which lie medial to extent of lymphadenectomy is more contro-
the pectoralis minor muscle. In most patients, versial. Whether simply an inguinofemoral
however, it is necessary to divide the pec- dissection (superficial) should be performed
toralis minor muscle. The extent of dissection, (with the inguinal ligament being the supe-
as measured by the number of nodes rior boundary of dissection) or the iliac nodes
removed, has been correlated with improved should be included is a matter of debate giv-
five-year survival in one retrospective study.26 en the higher rate of complications involved
Other variations in technique affect both with the pelvic dissection. Some surgeons
the regional recurrence rate and the mor- advocate routinely performing the addition-
bidity of axillary dissection. Preservation of al iliac dissection (deep) for patients with
the long thoracic and thoracodorsal nerves is clinically apparent inguinal disease. Others
considered routine, and injury to these nerves limit iliac dissection to only patients with a
should be extremely rare in experienced positive Cloquet’s node or multiple (3 or
hands. The intercostobrachial nerves may more) involved nodes. The drawback of
also be preserved, however most surgeons using Cloquet’s node as a deciding factor for
routinely resect these when the dissection is dissection boundaries is its limited ability to
being performed for palpable disease. Some predict the involvement of pelvic lymph
authors have advocated a more extensive nodes.35 Still others do not perform an iliac
dissection, including removal of the supra- dissection unless there is radiographic evi-
axillary fat pad, although this greatly increas- dence of pelvic adenopathy.
es the morbidity by exposing the brachial A retrospective review of 104 patients who
plexus. Brachial plexus injuries, although underwent superficial versus superficial plus
rare, can be devastating complications of this deep dissection demonstrated no influence of
procedure. Because there is no evidence that the deep dissection on locoregional recur-
Vol. 61, N. 2 MINERVA CHIRURGICA 145SABEL THE ROLE OF THE SURGEOAN IN THE MANAGEMENT OF MELANOMA
rence or survival.36 Another retrospective for patients with clinically evident disease,
study of 227 patients who had either super- the optimal management of patients without
ficial or superficial and deep dissections also clinically evident disease remains controver-
failed to demonstrated a survival advantage sial. Prior to the advent of SLNB, many advo-
associated with the extent of surgery, prompt- cated the performance of an elective lymph
ing the conclusion that pelvic dissection node dissection (ELND) for patients without
should be limited to patients with clinical clinical evidence of nodal metastases in order
evidence of disease.37 Five-year survival rates to assess for microscopic metastatic disease.
of 24% to 35% have been reported for Although ELND provides important prog-
patients with pelvic involvement who under- nostic information, this is only of benefit if
go superficial and deep dissection.37, 38 there are adjuvant therapies to offer the
If an iliac dissection is to be performed patient who is found to harbor metastases.
with the inguinofemoral dissection, this can Given the high rate of complications associ-
be accomplished through one skin incision by ated with ELND, the morbidity of it is hard-
obliquely dividing the external and internal ly justified on the basis of accurate staging
oblique muscles to expose the pelvic alone.
retroperitoneum, or alternatively by dividing The management of patients with melano-
the inguinal ligament. This may be particu- ma changed considerably after SLNB was
larly useful in cases of disease low in the described by Morton et al.42 There now exists
pelvis along the distal external iliac vessels. a reliable method for the identification and
The inguinal ligament may be divided either removal of the primary lymph node drain-
over the femoral vessels, which is technical- ing the site of a cutaneous melanoma, one
ly simpler, or at the anterior superior iliac that accurately determines whether tumor
spine, which may be associated with better cells have metastasized to that respective
wound healing. lymph node basin.43-45 Regional recurrence
after sentinel node biopsy is infrequent, and
CERVICAL DISSECTION has a greatly decreased morbidity as com-
pared to ELND. 46, 47
The gold standard for treating regional dis- SLNB possesses the further advantage of
ease in the neck has been the radical neck allowing for a more detailed histological
dissection (RND); removal of levels I-V as well examination than ELND. Identification of
as the sternocleidomastoid muscle, internal micrometastases in sentinel nodes is carried
jugular vein and spinal accessory nerve. Given out by careful sectioning of the node (step-
the extent of the structures removed, RND can sectioning) as well as the use of immuno-
be associated with significant morbidity. A histochemical staining with anti-S-100, anti-
modified radical neck dissection (MRND), also MART-1, or HMB-45 (anti-gp100) antibod-
described as a functional neck dissection, ies.48 Clinically, even microscopic foci of
includes preservation of any or all of those melanoma detected only by immunohisto-
structures. Several authors have reported no chemical staining are significant. With this
appreciable difference in the risk of regional increased sensitivity, sentinel lymph node
recurrence with MRND versus RND.39-41 A status is the most important predictor of sur-
more selective approach has therefore been vival for patients with melanoma. Patients
advocated, basing the dissection on the loca- with a negative sentinel node are over 6 times
tion of the involved nodes or primary lesion.41 more likely to survive than those with a pos-
itive sentinel lymph node (SLN), making the
predictive impact of sentinel node status
Sentinel lymph node biopsy as a much greater than any other prognostic fac-
staging procedure tor.49
SLNB plays a central role in staging the
While there is little argument as to the regional lymph nodes and is the standard of
potential benefit of a lymph node dissection care in many major melanoma centers.44, 50
146 MINERVA CHIRURGICA Aprile 2006THE ROLE OF THE SURGEOAN IN THE MANAGEMENT OF MELANOMA SABEL
Currently, the compelling prognostic value ing ELND theorized that of the patients with
of the nodal status makes SLNB indispensable occult metastases in the regional basin, some
for accurate staging, and thus obligates it to may have no distant disease at diagnosis, but
be a key component of future studies exam- could develop secondary metastases from
ining adjuvant therapy. Which patients should occult lymph node metastases during the
undergo SLNB? Cascinelli et al.50 reported interval between diagnosis of the primary
SLN positivity rates of 16% in lesions thicker melanoma and progression to clinically evi-
than 1 mm. Among the 829 patients in a dent nodal disease. Eradicating that micro-
WHO study, positivity rates of 2% (3 mm) were reported. In addition to tumor ment of distant disease and thereby improve
thickness, other factors such as tumor ulcer- survival. The exact impact of lymph node
ation, young patient age, and mitotic rate dissection on survival, however, would
have been shown to be associated with SLN depend on the size of the target population.
positivity.49, 51, 52 Based on these data, as well If a large percentage of patients with micro-
as on additional corroborating studies, the scopic nodal disease already have concomi-
SLNB procedure should be routinely consid- tant distant disease at diagnosis, or con-
ered for primary melanomas deeper than 1 versely, if only a small percentage of patients
mm. It may be selectively applied for tumors with microscopic disease go on to develop
1 mm or less, when other worrisome fea- secondary metastases, then the impact on
tures are present. survival would be quite small. As only
The same arguments against ELND may approximately 20% of patients are node pos-
be made against SLNB: the cost and morbid- itive, the impact of ELND on these subjects
ity, albeit lower, are not justified simply to would have to be quite large in order to see
obtain accurate staging information. Since a survival benefit for the entire group.
the introduction of SLNB, however, adjuvant The argument for ELND was fueled by ret-
therapy in the form of high-dose interferon rospective data suggesting a survival benefit
(HDI) has become available for the treatment existed. Two retrospective reviews compared
of high-risk melanoma. Although the use of survival statistics for patients with localized
HDI is controversial, the available evidence melanomas (stage I and II) who underwent
demonstrates an improvement in disease- wide excision alone with those who under-
free survival as well as a likely improvement went wide excision plus ELND.58, 59 Both
in overall survival.53-56 Justification of its use reviews suggested that patients who under-
and appropriate patient selection are issues went wide excision plus ELND had a signif-
beyond the scope of this article. If the patient icantly higher survival rate than those who
is a candidate for adjuvant interferon or par- had wide excision alone, even after the analy-
ticipation in a clinical trial for other adjuvant sis was stratified for tumor sites. As with all
therapies, SLNB is certainly justified in order retrospective research, though, any number
to identify high-risk individuals. Regardless, of unknown variables may have played a
the primary argument in favor of SLNB is the role in the choice between ELND and obser-
potential improvement in long-term outcome vation.
associated with the early eradication of micro- This data prompted 2 large prospective,
scopic disease. randomized trials to answer the question of
whether ELND provides a survival benefit.
The WHO Melanoma Group randomized 2
Lymph node dissection for groups of patients to receive either wide exci-
microscopic disease sion plus ELND (n=267) or wide excision
with subsequent therapeutic lymphadenec-
Complete lymph node dissection in tomy if clinically indicated (n=286).60 Analysis
patients without nodal disease was first advo- of these data revealed no difference in sur-
cated by Snow in 1892.57 The argument favor- vival between the 2 groups. With follow-up
Vol. 61, N. 2 MINERVA CHIRURGICA 147SABEL THE ROLE OF THE SURGEOAN IN THE MANAGEMENT OF MELANOMA now at greater than 20 years, the WHO Trial follow-up data was presented at the American still shows no statistical improvement in either Society of Clinical Oncology (ASCO) meeting survival or disease-free interval.17 The largest in Orlando, Florida in May, 2005.63 The inter- trial to examine the issue was the Intergroup im results compared only those patients with Melanoma Surgical Program, which ran- positive SLN, either those found to be posi- domized 740 stage I and II melanoma patients tive on SLNB or those who recurred after to ELND or observation.61 Overall, there again wide local excision alone. The seven-year was no significant difference between the 2 melanoma specific survival for patients who groups. Long-term results confirmed no sig- had completion lymph node dissection nificant ten-year survival difference between (CLND) for a positive SLN was 69%, com- ELND or observation (77% vs 73%, P=0.12).31 pared to 48% for patients undergoing delayed On the surface, this would seem to end CLND after nodal relapse (P=0.0034, RR=0.53, the discussion on whether we should be per- 95% CI 0.33,0.84). forming ELND, or even SLNB, for melanoma. The evidence to date suggests that per- Further assessment of the data, however, sug- forming SLNB plus CLND for a positive SLN gests that there are subsets of patients who do is unlikely to result in a survival advantage benefit from ELND. when all patients are compared, but will In the Intergroup trial, a significant reduc- improve survival among the subset of patients tion in mortality with ELND was seen for with occult lymph node metastases. Whether patients with nonulcerated melanomas, this approach is worth the added cost will tumors between 1 and 2 mm, and limb require maturation of the data. When ana- melanomas. It is possible that these subsets lyzed along with the use of adjuvant inter- represent patients who are less likely to have feron, it does appear to be cost-effective. 64 distant disease in the presence of regional But is the completion node dissection nec- disease, and thus might benefit from early essary? It is possible that SLNB alone will lymph node dissection. Further evidence is identify patients at high risk, and in the sub- provided from the WHO Program 14 Trial, set of patients for whom the SLN is the only which compared ELND to observation for node that harbors disease, it in itself is ther- patients with truncal melanomas. When the apeutic. Additional positive non-sentinel survival of patients in the WHO Program 14 lymph nodes (NSN) are found in only 7-33% Trial with microscopic disease at ELND was of patients with a positive sentinel node. compared with those who had regional recur- Unfortunately, predicting which patients will rences during observation, the survival was have residual disease in the NSN has proven significantly improved in the former group difficult.65-67 Even patients with the most (48.2% vs 26.6%, P=0.04). 62 favorable primary melanomas have a sub- This data suggests, but does not prove, stantial risk of additional disease in the basin. that lymph node dissection may benefit The on-going Multicenter Selective Lympha- patients with microscopic disease in the denectomy Trial-II will help answer this ques- lymph nodes, but not all clinically node neg- tion by randomizing patients with a positive ative patients. The SLN has provided a selec- SLN to CLND or observation. Until the final tive approach to complete lymph node dis- results from these 2 trials are available, CLND section, sparing node-negative patients the for a positive SLN remains the standard morbidity of the procedure, while offering approach. improved regional control and any potential survival benefit to the node-positive patient. The Multicenter Selective Lymphadenec- Surgery for stage IV melanoma tomy Trial-I is the only current prospective randomized trial that specifically compares The management of metastatic disease wide excision alone to wide excision plus from most cancers rarely falls into the domain SLNB, with complete node dissection for of the surgeon. Notable exceptions include patients with a positive SLN. The most recent liver resection for colorectal metastases and 148 MINERVA CHIRURGICA Aprile 2006
THE ROLE OF THE SURGEOAN IN THE MANAGEMENT OF MELANOMA SABEL
pulmonary resection for sarcoma metastatic who is >2 years out from initial resection is an
to the lung, both of which may be associat- ideal candidate for resection. The patient
ed with long-term survival. Distant site recur- with multiple metastases shortly after prima-
rences of melanoma are unpredictable, ry therapy presumed to have more aggressive
though, and can occur in almost every major disease and is very unlikely to benefit from
organ or tissue. While most patients with surgical resection; other treatment options
metastatic melanoma will not be candidates should be explored. For patients on the fence,
for curative resection, complete surgical resec- one option is to treat the patient with sys-
tion of melanoma metastases may be associ- temic therapy for 2 to 3 months and then re-
ated with an improvement in long-term sur- evaluate the patient. Patients who have a
vival. response or remain stable may then proceed
to resection.
Selection of patients for curative resection Preoperative evaluation begins with a thor-
ough history and physical examination,
The five-year survival for patients with including a complete review of systems
stage IV melanoma is approximately 10%. designed to elicit signs and symptoms of
Not all stage IV disease is equivalent in prog- additional metastatic disease. Blood count,
nosis, however, so careful selection of stage metabolic profile and serum LDH should be
IV melanoma patients for consideration of obtained. Although LDH is clearly associated
metastatectomy is imperative. Five-year sur- with prognosis, it is unclear whether an ele-
vival rates as high as 35% have been report- vated LDH in a patient with what appears to
ed with proper patient selection. Several fac- be resectable disease should preclude
tors should be weighed into the decision to surgery.68 A thorough search for the extent of
resect metastatic disease, foremost being the metastatic disease must be undertaken. Any
initial site of metastases. The new American symptoms suggestive of metastatic disease
Joint Committee on Cancer (AJCC) staging should prompt the appropriate additional
system groups metastatic melanoma into 3 studies, such as MRI for symptoms consis-
subsets. M1a disease is defined as nonvis- tent with brain metastases. Asymptomatic
ceral metastases such as skin, subcutaneous patients have typically been evaluated with a
tissue or lymph nodes outside of the draining CT scan of the chest, abdomen and pelvis.
basins. Patients with M1a disease have a 5 However, recent studies have suggested that
year melanoma specific survival rate of 18-flourodeoxyglucose positron emission
approximately 19%.68 M1b disease is defined tomography (FDG-PET) should be obtained
as pulmonary metastases, and M1c disease to detect occult metastatic disease, and would
includes all nonpulmonary visceral metas- be the imaging study of choice in this situa-
tases. The survival rate for visceral disease tion.22, 69, 70
is lower than for M1a disease, at approxi-
mately 7% for M1b and 9% for M1c disease.
Resection of M1a disease
All patients with metastatic melanoma should
have a serum LDH level drawn, as this cor- The most common site of distant metas-
relates with distant disease. If elevated, it tases are to remote areas of skin and soft tis-
leads to a classification of M1c disease regard- sues, as well as to lymph nodes outside of the
less of the site of distant disease. draining basins. Patients with a solitary metas-
Other factors that deseve consideration tasis to dermal or subcutaneous tissue have
include the likelihood of a complete resec- a reasonable long-term prognosis. There
tion, the number of metastatic foci, the initial should be no hesitancy to resect these
stage of disease and the interval between pri- patients if the work-up reveals no addition-
mary therapy and distant recurrence. The al areas of disease. Patients with more exten-
patient’s performance status, co-morbidities sive M1a disease must be evaluated on a indi-
and life expectancy are also considered. The vidualized basis, taking into account both
patient with the solitary, easily resected lesion the number and location of metastases and
Vol. 61, N. 2 MINERVA CHIRURGICA 149SABEL THE ROLE OF THE SURGEOAN IN THE MANAGEMENT OF MELANOMA
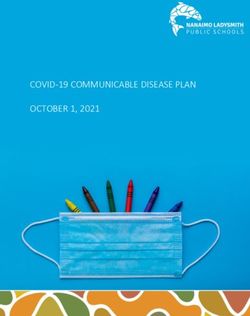
TABLE III.—Survival after complete resection of M1a TABLE IV.—Survival after complete resection of M1b
disease. disease.
Author Year No. Site 5-year survival Author Year No. 5-year survival
(%) (%)
Markowitz 71 1991 72 Lymph nodes 38 Wong 75 1988 38 31
Markowitz 71 1991 60 Soft tissue 49 Gorenstein 76 1991 59 25
Gadd 72 1992 190 All 14 Harpole 77 1992 98 20
Karakousis 73 1994 23 Lymph nodes 22 Karakousis 73 1994 39 14
Karakousis 73 1994 27 Subcutis 33 Tafra 78 1995 106 27
Meyer 74 2000 45 Lymph nodes 20 La Hei 79 1996 83 22
Meyer 74 2000 30 Skin/subcutis 17.8 Leo 80 2000 282 22
the disease-free interval. Several series have tion may be appropriate for highly selected
reported impressive five-year survivals after patients. Although it is one of most common
resection of M1a disease (Table III 71-74). malignancies to metastasize to the gastroin-
Resection of these lesions may also be pal- testinal tract, this is in actuality a relatively
liative, so erring on the side of an aggressive rare occurrence. Patients with gastrointesti-
surgical approach may be reasonable in the nal tract involvement are usually symptomatic,
appropriate setting. with pain/obstruction, bleeding/anemia and
weight loss. Surgery is primarily palliative,
Resection of M1b disease but may offer long-term survival (five-year
survivals of 5% to 10%).81-85 One series
Fifteen percent to 30% of metastases from demonstrated that long-term palliation could
malignant melanoma will occur in the lungs, be achieved in a majority of patients, and
typically asymptomatically, and is detected patients who underwent complete resection
by either chest radiography or computed had a longer median survival than patients
tomography (CT). Most will not be candi- who could not.86 Factors associated with a
dates for surgical resection because of either poor outcome include short disease-free inter-
multiple lesions or the presence of extrapul- val or elevated serum LDH.83 Resection of
monary disease. The patient with the soli- metastases to the spleen or liver have also
tary pulmonary metastasis, in the absence of been described, although only rare patients
additional disease discovered on CT or PET are candidates for that surgery. 87, 88
scan, should undergo resection. It is impor- Brain metastases are common in melanoma
tant to remember that in the patient with a patients and are associated with an extreme-
history of melanoma and the new solitary ly poor prognosis. Patients may present with
pulmonary nodule, this may not be a metas- headaches, focal neurologic deficits or
tases but a new primary lung cancer. When seizures; if left untreated they will experi-
more than one lesion is present, the deci- ence rapid deterioration and death. Palliation
sion to perform a pulmonary metastatectomy often involves whole brain irradiation, though
necessitates consideration of the ability to surgery or radiosurgery have been used with
achieve a complete resection. The pulmonary reasonable results. Not only is palliation
function and comorbidities of the patient as achieved in a significant number of patients,
well as the disease-free interval also play a but several series describe median survivals
heavy role in this decision. In selected of 6 to 18 months, depending on the selection
patients, five-year survivals of 15% to 15% criteria.89-94 Whether surgical resection should
may be achievable (Table IV73, 75-80). be followed by whole-brain irradiation
remains controversial. The criteria used to
select patients include the number of lesions
Resection of M1c disease
and their accessibility. Patients with deep-
Visceral recurrences outside of the lung are seated or multifocal lesions, while not good
less likely to benefit from surgery, but resec- surgical candidates, may be candidates for
150 MINERVA CHIRURGICA Aprile 2006THE ROLE OF THE SURGEOAN IN THE MANAGEMENT OF MELANOMA SABEL
stereotactic radiation techniques (gamma ottimale. Questo articolo rivede l’evoluzione della
knife). These consist of multiple convergent chirurgia del melanoma e sottolinea le evidenze che
beams that deliver a single high dose of radi- sono alla base delle raccomandazioni attuali.
ation to the lesion(s). 95, 96 Parole chiave: Melanoma - Chirurgia - Linfonodo sen-
tinella - Biopsia linfonodale.
Conclusions References
In summary, surgery remains the corner- 1. Chang AE, Johnson TM, Rees R. Cutaneous Neoplasms.
In: Greenfield LJ, Mulholland MW, Oldham KT,
stone of therapy for the treatment of both Zelenock GB editors. Surgery: Scientific Principles and
primary and metastatic melanoma. It offers a Practice. Philadelphia: Lippincott-Raven; 1997. p. 2231-
cure for primary melanoma when appropri- 46.
2. Essner R. Surgical treatment of malignant melanoma.
ate resection margins are taken. Surgery also Surg Clin N Am 2003;83:109-56.
plays a substantial role in the diagnosis and 3. Olsen G. Some views on the treatment of melanomas
of the skin. Arch Chirurg Neerl 1970;22:79-90.
treatment of regional disease, a role that has 4. Kennedy DE, Brown BW, McBride CM. Excision of
changed significantly since the advent of underlying fascia with a primary malignant melanoma:
SLNB. Even when the spread of disease has effect on recurrence and survival rates. Surgery
1982;92:615-8.
exceeded microscopic levels, surgery can not 5. Handley WS. The Hunterian lectures on the pathology
only provide palliation, but prolong survival of melanotic growths in relation to their operative treat-
if metastectomy is applied to an appropri- ment. Lancet 1907;1:996-1003.
6. Handley WS. The pathology of melanotic growths in
ately selected patient population. The future relation to their operative treatment. Lancet 1907;1:
of melanoma therapy is hopeful; it holds 927-33.
7. Wong CK. A study of melanocytes in the normal skin
promise for adjuvant or neoadjuvant treat- surrounding malignant melanomata. Dermatologica
ments in the form of vaccines, new chemo- 1970;141:215-25.
therapies and biologic agents. The objectives 8. Kelly JW, Sagebiel RW, Calderon W, Murillo L, Dakin RL,
Blois MS. The frequency of local recurrence and
and outcomes of surgical intervention will microsatellites as a guide to re-excision margins for
continue to change dramatically as these oth- cutaneous malignant melanoma. Ann Surg 1984;200:
759-63.
er therapies demonstrate their potential. Until 9. Veronesi U, Cascinelli N. Narrow excision (1-cm mar-
those roles are better defined and bear out gin). A safe procedure for thin cutaneous melanoma.
success, however, surgical therapy remains Arch Surg 1991;126:438-41.
10. Veronesi U, Cascinelli N, Adamus J, Balch C, Bandiera
the foundation of treatment for melanoma. D, Barchuk A et al. Thin stage I primary cutaneous
malignant melanoma: comparison of excision with
margins of 1 or 3cm. N Engl J Med 1988;318:1159-62.
11. Balch CM, Urist MM, Karakousis CP, Smith TJ, Temple
Riassunto WJ, Drzewiecki K et al. Efficacy of 2cm surgical mar-
gins for intermediate thickness melanomas (1 to 4
mm): results of a multi-institutional randomized surgi-
Il ruolo del chirurgo nella gestione del melanoma cal trial. Ann Surg 1993;218:262-7.
Mentre la terapia multidisciplinare è diventata lo 12. Balch CM, Soong SJ, Smith T, Ross MI, Urist MM,
standard per la maggior parte dei tumori solidi, per il Karakousis CP et al. Long-term results of a prospective
melanoma il trattamento è ancora imperniato sull’in- surgical trial comparing 2cm vs 4cm excision margins
for 740 patients with 1-4mm melanomas. Ann Surg
tervento chirurgico. Questo è vero non solo per le fasi Oncol 2001;8:101-8.
precoci della malattia ma anche per quelle avanzate. 13. Cohn-Cedermark G, Rutqvist LE, Andersson R, Breivald
L’approccio chirurgico al melanoma è mutato radi- M, Ingvar C, Johansson H et al. Long term results of a
calmente, indirizzandosi verso un’asportazione meno randomized study by the Swedish Melanoma Group on
aggressiva del tumore primario, accompagnata, però, 2cm vs 5 cm resection margins for patients with cuta-
neous melanoma with a tumor thickness of 0.8-2.0
da un approccio più aggressivo nei confronti delle mm. Cancer 2000;89:1495-501.
metastasi. La chirurgia del melanoma è stata influen- 14. Ringborg U, Andersson R, Eldh J, Glaumann B,
zata dalla comprensione dei meccanismi biologici Hafstrom L, Jacobsson S et al. Resection margins of 2
della malattia e dai dati emersi dagli studi clinici pro- versus 5 cm for cutaneous malignant melanoma with a
spettici e randomizzati appositamente disegnati. tumor thickness of 0.8 to 2.0mm. A randomized study
Viceversa, i nuovi approcci chirurgici ci hanno con- by the Swedish Melanoma Study Group. Cancer
1996;77:1809-14.
sentito di comprendere meglio la biologia del mela- 15. Thomas JM, Newton-Bishop J, A’Hern R, Coombes G,
noma, ma sono necessari ulteriori studi randomizza- Timmons M, Evans J et al. Excision margins in high-risk
ti per definire ulteriormente l’approccio chirurgico malignant melanoma. N Engl J Med 2004;350:757-66.
Vol. 61, N. 2 MINERVA CHIRURGICA 151SABEL THE ROLE OF THE SURGEOAN IN THE MANAGEMENT OF MELANOMA
16. Banzet P, Thomas A, Vuillemin E. Wide versus narrow Morton DL et al. Is the node of Cloquet the sentinel
surgical excision in thin (THE ROLE OF THE SURGEOAN IN THE MANAGEMENT OF MELANOMA SABEL
52. Bleicher RJ, Essner R, Foshag LJ, Wanek LA, Morton DL. 70. Krug B, Dietlein M, Groth W, Stutzer H, Psaras T,
Role of sentinel lymphadenectomy in thin invasive Gossmann A et al. Flouro-18-flourodeoxyglucose
cutaneous melanomas. J Clin Oncol 2003;21:1326-31. positron emission tomography (FDG-PET) in malig-
53. Sabel MS, Sondak VK. Pros and cons of adjuvant inter- nant melanoma: diagnostic comparison with conven-
feron in the treatment of melanoma. Oncologist tional imaging methods. Acta Radiol 2000;41:446-52.
2003;8:451-8. 71. Markowitz JS, Cosimi LA, Carey RW, Kang S, Padyk C,
54. Kirkwood JM, Manola J, Ibrahim JG, Sondak V, Ernstoff Sober AJ et al. Prognosis after initial recurrence of cuta-
MS, Rao U. A pooled analysis of Eastern Cooperative neous melanoma. Arch Surg 1991;126:703-7.
Oncology Group and Intergroup trials of adjuvant high- 72. Gadd MA, Coit DG. Recurrence patterns and outcome
dose interferon for melanoma. Clin Cancer Res in 1019 patients undergoing axillary or inguinal lym-
2004;10:1670-7. phadenectomy for melanoma. Arch Surg 1992;127:
55. Wheatley K, Ives N, Hancock BW, Gore M, Eggermont 1412-6.
A, Suciu S. Does adjuvant interferon alfa for high risk 73. Karakousis CP, Velez A, Driscoll BA, Takita H.
melanoma provide a worthwhile benefit? A meta-analy- Metastatectomy in malignant melanoma. Surgery 1994;
sis of the randomised trials. Cancer Treat Rev 115:295-302.
2003;29:241-52. 74. Meyer T, Merkel S, Goehl J,Hohenberger W. Surgical
56. Lens MB, Dawes M. Interferon alfa therapy for malig- therapy for distant metastases of malignant melanoma.
nant melanoma: a systematic review of randomized Cancer 2000;89:1983-91.
controlled trials. J Clin Oncol 2002;20:1818-25. 75. Wong JH, Euhus DM, Morton DL. Surgical resection
57. Snow H. Melanotic cancerous disease. Lancet for metastatic melanoma to the lung. Arch Surg
1892;2:872. 1988;123:1091-5.
58. Balch CM, Cascinelli N, Milton GW. Elective node dis- 76. Gorenstein LA, Putnam JB, ANatarajan G, Balch CA,
section: pros and cons. In: Balch CM, Milton GW edi- Roth JA. Improved survival after resection of pulmonary
tors. Cutaneous melanoma: clinical management and metastases from malignant melanoma. Ann Thorac
treatment results worldwide. Philadelphia: J.B. Surg 1991;52:204-10.
Lippincott, 1985. p. 131. 77. Harpole DH, Johnson CM, Wolfe WG, George SL,
59. Balch CM. The role of elective lymph node dissection Seigler HF. Analysis of 945 cases of pulmonary metasta-
in melanoma: rationale, results and controversies. J tic melanoma. J Thorac Cardiovasc Surg 1992;103:743-
Clin Oncol 1988;6:163-72. 8; discussion 748-50.
60. Veronesi U, Adamus J, Bandiera DC, Brennhovd O, 78. Tafra L, Dale PS, Wanek LA, Ramming KP, Morton DL.
Caceres E, Cascinelli N et al. Delayed regional lymph Resection and adjuvant immunotherapy for melanoma
node dissection in stage I melanoma of the skin of the metastatic to the lung and thorax. J Thorac Cardiovasc
lower extremities. Cancer 1982;49:2420-30. Surg 1995;110:119-28.
61. Balch CM, Soong SJ, Bartolucci AA, Urist MM, 79. La Hei ER, Thompson JF, McCaughan BC, Petersen-
Karakousis CP, Smith TJ et al. Efficacy of an elective Schaefer K, Ramanaden D, Coates AS. Surgical resec-
regional lymph node dissection of 1 to 4 mm thick tion of pulmonary metastatic melanoma: a review of 83
melanomas for patients 60 years of age and younger. thoracotomies. Asia Pacific Heart J 1996;5:111-4.
Ann Surg 1996; 224:255-66. 80. Leo F, Cagini L, Rocmans P, Cappello M, Geel AN,
62. Cascinelli N, Morabito A, Santinami M, MacKie RM, Maggi G et al. Lung metastases from melanoma: when
Belli F. Immediate or delayed dissection of regional is surgical treatment warranted? Br J Cancer 2000;83:
nodes in patients with melanoma of the trunk: a ran- 569-57.
domized trial. Lancet 1998;351:793-6. 81. Klasse JM, Kroon BB. Surgery for melanoma metasta-
63. Morton DL. Interim results of the Multicenter Selective tic to the gastrointestinal tract. Br J Surg 1990;77:60-1.
Lymphadenectomy Trial (MSLT-I) in clinical stage I 82. Caputy GG, Donohue JH, Goellner JR, Weaver AL.
melanoma. 2005 American Society of Clinical Oncology Metastatic melanoma of the gastrointestinal tract. Results
Annual Meeting, 2005, May 13-17, Orlando, FL. of surgical management. Arch Surg 1991;126:1353-8.
64. Wilson LS, Reyes CM, Lu C, Lu M, Yen C. Modelling the 83. Ricaniadis N, Konstadoulakis MM, Walsh D, Karakousis
cost-effectiveness of sentinel lymph node mapping CP. Gastrointestinal metastases from malignant
and adjuvant interferon treatment for stage II melanoma. Surg Oncol 1995;4:105-10.
melanoma. Melanoma Res 2002;12:607-17. 84. Ollila DW, Essner R, Wanek LA, Morton DL. Surgical
65. Sabel MS, Griffith KA, Sondak VK, Lowe L, Schwartz JL, resection for melanoma metastatic to the gastroin-
Cimmino VM. Predictors of nonsentinel lymph node testinal tract. Arch Surg 1996;131:975-9.
positivity in patients with a positive sentinel node for 85. Agrawal S, Yao TJ, Coit DG. Surgery for melanoma
melanoma. J Am Coll Surg 2005;201:37-47. metastatic to the gastrointestinal tract. Arch Surg
66. Wagner JD, Gordon MS, Chuang T-Y, Coleman JJ 3rd, 1999;131:975-9.
Hayes JT, Jung SH et al. Predicting sentinel and resid- 86. Panagiotou I, Brountzos EN, Babloukos D, Stoupis C,
ual lymph node basin disease after sentinel lymph Brestas P, Kelekis DA. Malignant melanoma metastat-
node biopsy for melanoma. Cancer 2000;89:453-62. ic to the gastrointestinal tract. Melanoma Res
67. McMasters KM, Wong SL, Edwards MJ, Chao C, Ross MI, 2002;12:169-73.
Noyes RD et al. Frequency of nonsentinel lymph node 87. De Wilt JH, McCarthy WH, Thompson JF. Surgical treat-
metastasis in melanoma. Ann Surg Oncol 2002;9: ment of splenic metastases in patients with melanoma.
137-41. J Am Coll Surg 2003;197:38-43.
68. Balch CM, Buzaid AC, Soong S-J, Atkins MB, Cascinelli 88. Rose DM, Essner R, Hughes TS, Tang PC, Bilchik A,
N, Coit DG et al. Final version of the American Joint Wanek LA et al. Surgical resection for metastatic
Committee on Cancer staging system for cutaneous melanoma to the liver: the John Wayne Cancer Institute
melanoma. J Clin Oncol 2001;19:3635-48. and Sydney Melanoma Unit experience. Arch Surg
69. Gulec SA, Faries MB, Lee CC, Kirgan D, Glass C, Morton 2001;136:950-5.
DL et al. The role of flourine-18-deoxyglucose positron 89. Hagen NA, Cirrincione C, Thaler HT, DeAngelis LM. The
emission tomography in the management of patients role of radiation therapy following resection of single
with metastatic melanoma: impact on surgical deci- brain metastases from melanoma. Neurology 1990;
sion making. Clin Nucl Med 2003;28:961-5. 40:158-60.
Vol. 61, N. 2 MINERVA CHIRURGICA 153SABEL THE ROLE OF THE SURGEOAN IN THE MANAGEMENT OF MELANOMA
90. Saha S, Meyer M, Krementz ET, Hoda S, Carter RD, with brain metastases from malignant melanoma. J
Muchmore J et al. Prognostic evaluation of intracra- Neurosurg 1998;88:11-20.
nial metastasis in malignant melanoma. Ann Surg Oncol 94. Wronski M, Arbit E. Surgical treatment of brain metas-
1994;1:38-44. tases from melanoma: a retrospective study of 91
91. Salvati M, Cervoni L, Caruso R, Gagliardi FM. Solitary patients. J Neurosurg 2000;93:9-18.
cerebral metastasis from melanoma: value of the ‘en 95. Yu C, Chen JCT, Apuzzo MLJ, O’Day S, Giannotta SL,
bloc’ resection. Clin Neurol Neurosurg 1996;98:12-4. Weber JS et al. Metastatic melanoma to the brain: prog-
92. Skibber JM, Soong SJ, Austin L, Balch CM, Sawaya RE. nostic factors after gamma knife radiosurgery. Int J
Cranial irradiation after surgical excision of brain metas- Radiat Oncol Biol Phys 2002;52:1277-87.
tases in melanoma patients. Ann Surg Oncol 1996;3: 96. Gerosa M, Nicolato A, Foroni R. The role of gamma
118-23. knife radiosurgery in the treatment of primary and
93. Sampson JH, Carter JH, Friedman AH, Seigler HF. metastatic brain tumors. Curr Opin Oncol 2003;15:
Demographics, prognosis, and therapy in 702 patients 188-96.
154 MINERVA CHIRURGICA Aprile 2006You can also read