THYROID CANCER Joseph P. Cleaver MD Medical Director November, 2011
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
THYROID CANCER Joseph P. Cleaver MD Medical Director November, 2011
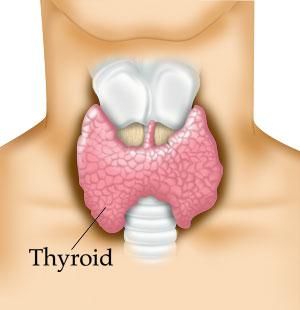
THE THYROID GLAND AND ITS FUNCTIONS
THYROID GLAND
• Under the influence of the hypothalmus and the pituitary gland, the thyroid produces the
following
• T4 (thyroxine) – constitutes 80% of thyroid hormone produced and is a prohormone.
• T3 (Triidothyronine) – constitutes 20% and is the active hormone
• Calcitonin- ( produced by C- cells) – helps regulate calcium level
• T4 is converted to the active form T3 by iodothyronine deiodinaseTHYROID STUDIES
• 80% of T4 and T3 is bound by thyroglobulin, a protein made by the thyroid gland and is
metabolically inactive
• Therefore, measure free T4, and free T3 is most accurate
• Thyroglobulin – tumor marker for thyroid Ca
• TSH (thyroid stimulating hormone)- pituitary
• Measures thyroid dysfunction when elevated.THYROID FUNCTION • The thyroid gland impacts every function in the body because it controls metabolism
THYROID DEFICIENCY SYMPTOMS • Cold intolerance, cold hands, feet • Fatigue • Dry skin • Constipation • Depression • Resistant to wt loss • Dry rough skin • Hoarseness • Tiredness, fatigue • Lower body temp • Brain fog • Fluid retention
40 YEAR OLD FEMALE • Presents with a solitary firm 2.0 cm nodule on annual exam by her personal physician • TSH = 3.4 Free T4 = 1.4 Free T3= 4.4 • BIOPSY – ? • THYROID ULTRASOUND – COMPLEX CYST • BIOPSY – BENIGN by FNA • RISK?
BENIGN THYROID NODULES - TYPES • Macrofollicular ( colloid) • Normofollicular (simple) • Microfollicular (fetal) • Trabecular (embryonal) • Hurthle cell (oxyphil – cell) adenoma
THYROID NODULES • 1/15 women • 1/40 men • Solitary nodule higher risk of malignancy then multiple nodules • Usually asymptomatic • May be cystic – ultrasound to evaluate • Fluid filled simple cysts are usually benign • Complex cysts composed of fluid and solid components occasionally are malignant
FEATURES THAT INCREASE SUSPICION OF MALIGNANCY • Age 70 • Irregular, firm or fixed nodule • solid or complex on ultrasound • Nodule size >4 cm • “cold “ nodule • Cervical lymphadenopathy • Previous hx of thyroid cancer • hx of external neck radiation • Family hx of thyroid ca or MEN 2
SOLITARY THYROID NODULE
BIOPSY – AMERICAN THYROID ASSOCIATION
THYROID CANCER • Approximately 50,000 new cases annually, mostly in women • Overall five year survival is 97% • Most cases between the ages of 20 and 50
RISK FACTORS FOR THYROID CANCER
• Women are 3X greater lifetime risk then men
• Most cancers occur between the ages of 20 and 60. (risk peaks in women (40s and 50s)
earlier then men)
• Dietary risks – iodine (too high too low)
• Radiation exposure – young age, dose dependent
• Family historyHEREDITARY CONDITIONS • FMTC – Familial medullary thyroid carcinoma • APC gene – Familial adenomatous polyposis • PTEN gene – Cowden disease – thyroid, endometrial, breast
40 YEAR OLD FEMALE • Presents with solitary nodule on annual exam by her private physician • TSH = 4.0 Free T4 = 1.4 free T3 = 4.4 • Mass is hard and fixed • Ultrasound shows solid mass at 1.4 cm • FNA shows follicular cell tumor • lymph nodes are negative, no capsular invasion • Total thyroidectomy and treatment with I131 in 2008 • Thyroid scans and thyroglobulin negative since 2009 • Current exam reveals no recurrence • Stage ? • Risk?
UNDERWRITING THYROID NODULES • Solitary or multiple nodules (solitary fixed or movable) • Cystic or solid (simple or complex) • Capsule invasion • Hot or cold nodule on thyroid scan
STAGES AND RATINGS
RATING
STAGES TNM A B
In situ Tis 0 0
Single nodule, 1 cm or less, without invasion of T1 Class 6 Class 5
capsule
With mobile regional lymph nodes T1, N1-2 Class 4 Class 3
With fixed regional lymph nodes T1, N3 Class 3 Class 2
Single nodule, more than 1 cm,
without invasion of capsule
With mobile regional lymph nodes Class 4 Class 3
With fixed regional lymph nodes Class 3 Class 2
Multiple nodules, isthmus nodule, Class 3 Class 2
without invasion of capsule
With regional lymph nodes Class 2 Class 1
Tumor invasion of capsule and beyond Class 1 RNA
Distant metastases RNA RNA
Undifferentiated and Anaplastic Carcinomas RNA RNA
Persistent elevated calcitonin level RNA RNABenign Tumors
The most common benign tumor is the adenoma. Other tumors include
follicular adenoma (sometimes called colloid adenomas), fetal tumors, Hurthle-
cell adenomas and the extremely rare teratoma.
Present
Single, firm or hard nodule
0–1 year PP
1–2 years +50–100 up WP:No ADB:Yes
Multinodular
Small, asymptomatic 0 WP:Yes ADB:Yes
Large, symptomatic +50–100 up WP:No ADB:Yes
History of
Surgically removed, benign 0 WP:Yes ADB:Yes
Malignant Tumors
Differentiated Tumors
A) Papillary carcinoma
B) Follicular Carcinoma
Hurthle Cell Carcinoma
Medullary (C-Cell) CarcinomaRATING CLASS
Time since Rating Class
complete surgical
removal or radiation 1 2 3 4 5 6
cure
0–1 year RNA RNA PP PP $10.00 for 4 $5.00 for 3
1–2 years RNA RNA PP $10.00 for 5 $ 7.00 for 3 $5.00 for 2
2–3 years RNA PP $12.00 for 5 $ 7.00 for 4 $ 5.00 for 2 $5.00 for 1
3–4 years PP $15.00 for 5 $10.00 for 4 $ 7.00 for 3 $ 5.00 for 1
4–5 years PP $10.00 for 4 $10.00 for 3 $ 7.00 for 2
5–6 years $20.00 for 5 $10.00 for 3 $ 5.00 for 2 $ 5.00 for 1
6–7 years $20.00 for 4 $10.00 for 2 $ 5.00 for 1
7–8 years $15.00 for 3 $ 5.00 for 1
8–9 years $15.00 for 2
9–10 years $15.00 for 1APPROACH TO THYROID CANCER
• Pathology
• Stage
• Treatment – I131 ablation
• Follow up
• I131 scans
• Thyroglobulin levelsTHYROID CANCER CLASSIFICATION • Follicular carcinoma • Papillary carcinoma • Medullary carcinoma • Anaplastic carcinoma • Primary thyroid lymphoma • Metastatic carcinoma (breast, renal cell, others)
FINE NEEDLE ASPIRATION - FNA
• Benign
• Malignant – follicular and Hurthle cell carcinoma need surgical bx to make diagnosis
• Suspicious –need surgical excision to determine 25% found to be malignant and usually
follicular or hurthle cel neoplasm
• Non-diagnostic – insufficient number of cellsULTRASOUND – WHAT TO LOOK FOR
• Most likely benign
• Cystic and fluid filled
• Sharp edges
• Multiple nodules
• No blood flowing through it (usually a cyst)THYROID SCAN
• COLD – decreased uptake usually benign
• 20% still malignant and still need biopsy to rule out malignancy
• HOT – increased uptake of isotope almost always benign
• Biopsy not needed
• Associated with hyperthyroidismFOLLICULAR CANCER • 12% of thyroid cancers • More aggressive than papillary ca • Higher mortality if diagnosed after age 40 • Treatment is total thyroidectomy and I131 therapy • Metastasis can be treated with additional I131 therapy
PAPILLARY CANCER • Most common type, 60-70% • Commonly spreads to cervical lymph nodes • Treatment is thyroidectomy and I131 therapy • Prognosis is best under 40
MEDULLARY CANCER • 5-8% of thyroid cancer • Originates from the C cells – calcitonin producing cells • Higher incidence of metastasis to lymph nodes • Tx is complete thyroidectomy and neck dissection • Can’t use I131 post sx to assess post surgical follow up • Lower cure rate than papillary and follicular neoplasms
HURTHLE CELL CANCER • 4% of thyroid cancers • Follicular cancer variant, much higher risk of metastasis and recurrence • Difficult to differentiate between benign and malignant tumor on frozen section • Need thyroidectomy if path report indicates Hurthle cell metaplasia • Hurthle cells are less likely to take up iodine • Good prognosis if diagnosed early
SURVIVAL
Medullary thyroid cancer**
Stage 5-Year Relative
Survival Rate
I near 100%
II 98%
III 81%
IV 28%SURVIVAL
Follicular thyroid cancer*
Stage 5-Year Relative
Survival Rate
I near 100%
II near 100%
III 71%
IV 50%
Papillary thyroid cancer*
Stage 5-Year Relative
Survival Rate
I near 100%
II near 100%
III 93%
IV 51%THYROID CANCER MORTALITY
FOLLOW UP THYROID CANCER
• Post thyroidectomy I131 therapy
• Must eradicate all thyroid tissue so can later scan for abnormal recurrence
• Six months after initial treatment – rescan entire body
• If no uptake then no additional tx needed
• If present then retreat with I131
• Two consecutive negative scans at six month intervals – remission
• Thyroglobulin levels checked post op and every six months until scan is negative, then
annuallyFOLOW UP THYROID CANCER
• IF THERE IS ANY RESIDUAL THYROID TISSUE ON RADIOACTIVE THYROID SCAN,
OR THYROGLOBULIN IS ELEVATED, POSTPONE FOR FURTHER EVALUATION AND
TREATMENTSTAGING
THANK YOU
You can also read