Update on the Diagnosis and Treatment of Narcolepsy - Michael Thorpy M.D. Sleep-Wake Disorders Center
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Update on the Diagnosis and Treatment
of Narcolepsy
Michael Thorpy M.D.
Sleep-Wake Disorders Center
Department of Neurology
Montefiore Medical Center
and
The Albert Einstein College of Medicine
Bronx, New York
Narcolepsy Network NYC Meeting, November, 2019
Narcolepsy and Variant Disorders Narcolepsy Type I (Narcolepsy with cataplexy) Narcolepsy Type 2 (Narcolepsy without cataplexy) Idiopathic Hypersomnia
Definition - Narcolepsy
A Neurologic disorder characterized by:
Excessive Daytime Sleepiness
Continual sleepiness (background)
Voluntary sleep episodes (naps)
Involuntary sleep episodes (sleep attacks)
Wakeful sleep (automatic behavior, microsleeps)
REM-related phenomena
Cataplexy ~ 60%
Hallucinations ~ 67%
Sleep paralysis ~ 64%
Disturbed Nocturnal sleep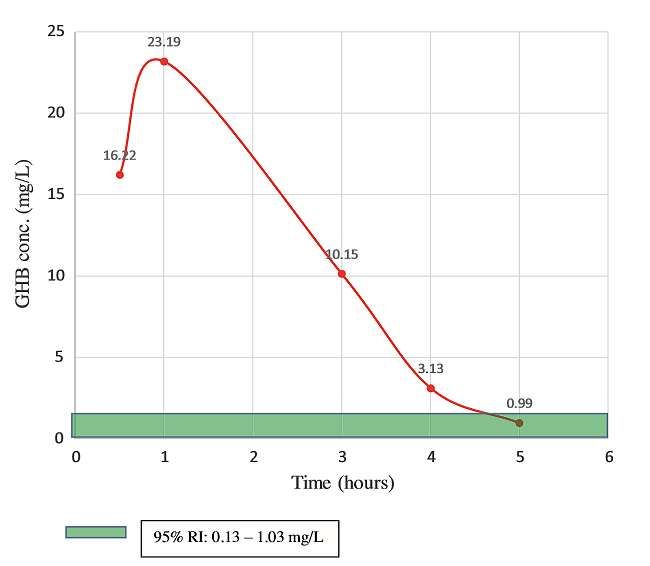
Narcolepsy Diagnosis Criteria ICSD-3
ICSD-3 (2014)
Narcolepsy Type 1 (narcolepsy with cataplexy)
•Chronic EDS (daily for at least 3 months) and
•Presence of 1 or both of the following:
– Cataplexy + mean sleep latency ≤ 8 minutes and ≥ 2 SOREMPs on MSLT*
– Low CSF hypocretin-1 level (either ≤ 110 pg/mL or < 1/3 of mean values)
Narcolepsy Type 2 (narcolepsy without cataplexy)
•Chronic EDS (daily—at least 3 months)
•Mean sleep latency ≤ 8 minutes and ≥ 2 SOREMPs on MSLT*
•Cataplexy absent
•CSF hypocretin-1 concentration not measured or CSF hypocretin-1 level is > 110
pg/mL or > 1/3 mean values
*A SOREMP on the preceding night's polysomnograpm may substitute for 1 of the SOREMPs on MSLT.
a. American Academy of Sleep Medicine. The International Classification of Sleep Disorders. 3rd ed. 2014; b. American Psychiatric 4
Association. Diagnostic and Statistical Manual of Mental Disorders – Fifth Edition. 2015.Limitations of the MSLT
False positives
≥2 SOREMS occur in 13% of men and 6% of women.
≥2 SOREMs and MSL latency < 8 min occurs in 6% of men and
1% of women.
False negatives
MSLT can be falsely negative 7-20% of the time (anxiety, meds,
age, environmental factors)
With advanced age, number of SOREMP decreases by 1 and
mean sleep latency increases ~2 min
Poor test-retest reliability
In 18 N-C patients with 2 MSLT’s, the MSLT was positive
in < 50%.
(Okun, et al, 2002; Mignot, et al, 2006; Dauvilliers et al, 2001; Dauvilliers, et al, 04;
Furuta, et al, 2001; Andlauer, et al, 2012; Trotti, et al 2013)Cataplexy in Narcolepsy
Facial sagging
Eyelids and twitching
Head drop Slurred speech
Jaw weakness
Pathognomonic for narcolepsy
Weakness
Sudden and transient loss or reduction of in arms,
muscle tone shoulders,
or hands
Triggered by strong emotions
Laughter, elation, surprise, anger
Typically partial or localized (~75%)
Usually short duration (seconds to
minutes) Buckling
Frequency varies widely (yearly to daily) of knees
Partial
or 75%
Localize
d
1. American Academy of Sleep Medicine. The International Classification of Sleep Disorders. 2nd ed.; 2005.
2. Overeem S et al. Sleep Med. 2011;12(1):12-18.
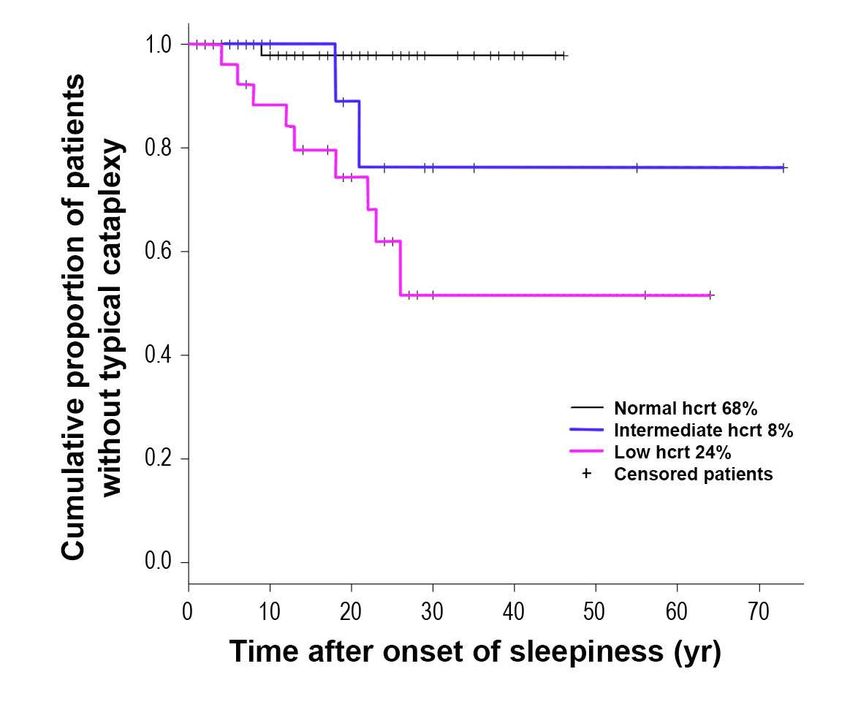
3. Ahmed I, Thorpy M. Clin Chest Med. 2010;31(2)371-381.Development of cataplexy over time
n=127 narcolepsy without cataplexy patients
Andlauer, et al, 2012REM Sleep Abnormalities Atonia occurs during wakefulness (cataplexy). REM sleep intrudes into wakefulness during the daytime (soremps). Sleep paralysis occurs in the transitions to and from sleep, often in association with dreams or hallucinations (40-80%). Compoents of REM sleep in wakefulness leads to visual and even auditory hallucinations (40-80%). Frequent, vivid, frightening and bizarre dreams, nightmares, lucid dreams, delusional dreams, out-of-body experiences and dreams of flying often occur. REM sleep behavior, can cause of bodily injury to the patient and potentially the bed partner. Ahmed I, Thorpy M. Clinical features, diagnosis and treatment of narcolepsy. Clin Chest Med. 2010 Jun;31(2):371-81.
Dreams in Narcolepsy
Hypnagogic hallucinations occur in 59% of NC (28% NwoC)
Dreams tend to be frequent, vivid, emotional and more easily recalled .
Dreams often occur in naps.
Lucid dreams more common.
88% delusional dreams in narcolepsy (cf 15% norms).
Dreams of flying, or out-of-body experiences, where dreams of seeing
themselves asleep, are more common in narcolepsy.
Flying 67%
Being chased 61%
Nightmares 54 %
Presence of a person in the room 31%
Monsters 19 %
Out-of-body experiences 18%
Leu-Semenescu et al. Sleep Med 2011 9120: 497-504;Wamsley E, et al.. Sleep. 2014 Feb 1;37(2):419-22.; Sturzenegger et al. J.
Sleep Res. (2004) 13, 395–406. Pisko et al 2014Idiopathic Hypersomnia Diagnostic Criteria (ICSD3 2014)
A. The patient has daily periods of irrepressible need to sleep or daytime
lapses into sleep occurring for at least 3 months.
B. Cataplexy is absent.
C. An MSLT performed according to standard techniques shows fewer than
2 sleep-onset REM periods or no SOREMPs if the REM latency on the
preceding nocturnal PSG was less than or equal to 15 minutes.
D. The presence of at least one of the following:
1. The MSLT shows a mean sleep latency of < 8 minutes.
2. Total 24-hour sleep time is >660 minutes (typically 12-14 hours
on a 24- hour polysomnographic monitoring (performed after
correction of chronic sleep deprivation), or by wrist actigaphy in
association with a sleep log (averaged over at least seven days with
unrestricted sleep).
American Academy of Sleep Medicine. The International Classification of Sleep
Disorders. 3rd ed.; 2014CSF hypocretin (pg/mL) Hypocretin/orexin Levels
600
500
400 47 10 18 28
300
200
3 0 1
100
88 3 0
0
Control Narcolepsy Narcolepsy Idiopathic
(n=47) with without Hypersomnia
Cataplexy Cataplexy (n=28)
(n=101) (n=21)
Mignot et al. 2002Progressive Narcolepsy
Years After EDS
2 4 6
Onset
PSG SOREMP
3 2 1
(mins)
ESS 19 16 18
MSLT MSL 6.9 5.4 3.6
MSLT SOREMPs
0 3 5
Csf Hct pg/ml 128 56.4
At age 39 female presented with excessive sleepiness, hypnogogic hallucinations, sleep
paralysis, nightmares.
Age 45 onset of cataplexy.
Dx: Idiopathic hypersomnia – Type 2 Narcolepsy – Type 1 narcolepsy
Pizza F et al. Primary progressive narcolepsy Type1. Neurology 2014; 83: 2189-2190Narcolepsy Spectrum Disorder IH NT2 NT1 Resolve Variable Stable
Precipitation of Narcolepsy
Streptoccocus
Lymes Disease
Infectious Mononucleosis
Influenza Virus
H1N1vaccination
Koepsell TD, Ton TG, Longstreth WT Jr. Medical exposures in youth and the frequency of narcolepsy with cataplexy: a
population-based case-control study in genetically predisposed people. J. Sleep Res; 19:80-86, 2010Narcolepsy
An autoimmune disorder in genetically predisposed
people probably precipitated by an infection with a
loss of hypocretin cells in the CNSGoals of Treatment
Reduce daytime sleepiness
Control ancillary symptoms:
Cataplexy
Nightmares and hallucinations
Sleep paralysis
Disturbed nocturnal sleep
Improve psychosocial and work functioning
Improve safety of patient and publicAASM Practice Parameters for Narcolepsy:
Excessive Sleepiness (Recommendations 2007)
Recommendation
Agent Indication Based on:
Level
Modafinil Narcolepsy: Standard 4 level 1 studies
EDS 2 Level 2 studies
Narcolepsy: EDS, Standard 3 level 1 studies
Sodium Oxybate
2 Level 2 studies
Amphetamine Narcolepsy: Guideline 3 level 2B studies
Methamphetamine EDS 4 level 5C studies
d-amphetamine
Methylphenidate
Selegiline Narcolepsy: EDS, Option 2 level 2B studies
Cataplexy 1 level 4C studies
Ritanserin Narcolepsy: EDS Option 2 level 2B studies
Morgenthaler TI, et al. Practice parameters for the treatment of narcolepsy and other hypersomnias of central origin. Sleep. 2007
Dec 1;30(12):1705-11.AASM Practice Parameters for Narcolepsy:
Ancillary Symptoms (Recommendations 2007)
Recommendation
Agent Indication Based on:
Level
Standard 3 level 1 studies
Sodium Oxybate
Cataplexy, 2 Level 2 studies
Disrupted sleep
Hypnagogic Halluc.
Option
Sleep paralysis
Tricyclic antidepressants, cataplexy Guideline 1 level 2 study
SSRIs, venlafaxine 1 Level 4 study
and reboxetine 1 level 5 study
Tricyclic antidepressants, Sleep paralysis
SSRIs, venlafaxine Option
Hypnagogic halluc.
and reboxetine
Morgenthaler TI, et al. Practice parameters for the treatment of narcolepsy and other hypersomnias of central origin.
Sleep. 2007 Dec 1;30(12):1705-11.Therapeutic Interventions for Narcolepsy
Alerting Medications
Medication Mechanism of action
Caffeine[a] Adenosine receptor antagonist
Sympathomimetic; enhance neurotransmission of
Methylphenidate[b]*, amphetamines[c]*
dopamine, norepinephrine, serotonin
Modafinil[d]*, armodafinil[e]* Dopamine reuptake inhibitor
Sodium oxybate[f]* GABAB agonist
Solriamfetol[g]* Dopamine-norepinephrine reuptake inhibitor
Pitolisant[h]* Histamine H3 antagonist/inverse agonist
TAK-925[i]† Hypocretin receptor agonist
*FDA approved to treat excessive sleepiness associated with narcolepsy.
†Investigational;
not FDA-approved for any indication.
a. Aldosari MS, et al. Clin Nutr. 2018;37:S208; b. Ritalin® (methylphenidate) PI 2019; c. Adderall® (amphetamine and dextroamphetamine) PI 2007; d. Provigil® (modafinil) PI
19
2015; e. Nuvigil® (armodafinil) PI 2018; f. Xyrem® (sodium oxybate) PI 2018; g. Sunosi™ (solriamfetol) PI 2019;
h. Kimura H, et al. An orexin 2 receptor-selective agonist,]. Sleep. 2019;42(suppl 1):A23.Sodium Oxybate
Improves nocturnal sleep;
Increases slow wave sleep
Reduces arousals and awakenings
Can eliminate cataplexy
Reduces vivid dreams, nightmares and hallucinations
Reduces sleep paralysis
Improves overall cognitive functioning
The only medication that can treat all symptoms of
narcolepsyArmodafinil
Longer acting isomer of modafinil (R-(-)-modafinil)
Half life approximately 3 x S-(-)-modafinil (approx 15
hrs)
Once per day formulation
Dose: 50mg – 250 mg (eqiv 400mg modafinil)
No effect on cataplexy
Reduces efficacy of oral contraceptives
Increases metabolism of ethinylestradiol
Can cause serious rashes and allergic reactions$65.8 million class action settlement for
purchases or modafinil
Provigil or its generic equivalent
Violation of antitrust and consumer protection laws by
delaying availability of less expensive generic
versions on Provigil
June 24, 2006 through August 8, 2019
Not a class member if you were insured and paid a
flat co-pay that was the same dollar amount as for
brand drug purchases and purchased only generic
pursuant to a fixed co-pay applicable to generic
drugs.
Claim by January, 2020Adderall
(mixed amphetamine salts)
Four amphetamine salts:
racemic amphetamine aspartate monohydrate,
racemic amphetamine sulfate,
dextroamphetamine saccharide,
dextroamphetamine sulfate
A dopamine and norepinephrine releasing agent, mildly
serotonergic.
Available in two formulations:
IR (Instant Release) and XR (Extended Release).
The IR is indicated for narcolepsy,
the XR formulation is not indicated for narcolepsy.
Dosage: 5 – 60mgSolriamfetol (Sunosi)
Selective dopamine-norepinephrine reuptake inhibitor (DNRI)
with robust wake-promoting effects1,2
Low binding affinity and selective for DAT and NET2
Inhibits DAT and NET reuptake2
Negligible interactions at SERT2
Does not produce rebound hypersomnia2
Human pharmacokinetics show3,4:
Rapid uptake (median Tmax 2-3 hours)
Renal clearance as unchanged drug with a t1/2 of ~6 hours
Bioequivalence of the fed and fasted conditions
FDA approved March 21, 2019
1. Hasan S, et al. Neuropsychopharmacology. 2009;34:1625-1640. 2. Carter L, et al. Presented at: 49th Winter Conference on Brain Research; January 23–28,
2016; Breckenridge, CO. Poster Su23. 3. Zomorodi K et al. Clin Pharmacol Drug Dev. 2017;6(S1):5 (abstract). 4. Zomorodi K et al. Sleep. 2017;40
(suppl):A382-383 (abstract). 5. Bogan R, et al. Sleep Med. 2015;16:1102-1108. 6. Ruoff C, et al. Sleep. 2016;39:1379-1387Sunosi (Solriamfetol)
Dopamine Norepinephrine Reuptake Inhibitor (DNRI). Schedule IV
Available in 75mg scored or 150mg tablets.
Approved for adults: Narcolepsy: 75mg to 150mg, OSA: 37.5mg to 150mg
Can be taken with or without food on awakening
Contraindicated with MAOIs
Renal excretion (95%): reduced dose in renal disease
Can cause increased BP and HR, no effect on QTc
Avoid use in unstable cardiovascular disease
Can cause anxiety, insomnia and irritability
Half-life 7 hours, Tmax 2 hours
No evidence of dependence or withdrawal
Drug liking similar to or lower than phentermine
No effect on O/Cs
No evidence of increase pregnancy risk
No data on breast milk (present in rat milk)
No effect on cataplexy
FDA approved March 21, 2019, available July 8, 2019
Thorpy MJ, et al. A randomized study of solriamfetol for excessive sleepiness in narcolepsy. Ann Neurol. 2019 Mar;85(3):359-370.Pitolisant
Dosing Warning and precautions
Recommended dosage Increases QTc interval; avoid
range: 17.8 mg to 35.6 mg use in patients
once daily Taking other drugs that
Adjustments in patients with prolong QTc interval
hepatic or renal impairment or With risk factors for
poor metabolizers of CYP2D6 prolonged QTc interval
Contraindications Pregnancy and lactation
Patients with severe hepatic Unknown (present in rat milk)
impairment Alternative non-hormonal
contraceptive method during
FDA approved for the treatment of and for at least 21 days after
EDS in adults with narcolepsy on discontinuation of treatment
August 14, 2019
Available November 4, 2019
Not controlled, non scheduled
a. Romigi A, et al. Drug Des Devel Ther. 2018;12:2665-2675; b. Wakix® (pitolisant) PI 2015; c. ClinicalTrials.gov. NCT03433131.Medications for Cataplexy
Sodium oxybate
Histamine H3 receptor antagonist/agonist:
pitolisant*
Antidepressants*:
TCA’s: anafranil, clomipramine, protripyline
SSRIs: fluoxetine, paroxetine
NERI’s: venlafaxine, atomoxetine, reboxetine
* Not FDA approved for cataplexyAntidepressants for Cataplexy Can be effective for cataplexy NERIs most effective; e.g., venlafaxine, atomoxetine Can cause sexual side effects Can disturb nocturnal sleep Not effective for other REM phenomena; SP, HH Not effective for sleepiness
Narcolepsy and Pregnancy
Avoiding all medications during conception and pregnancy is the usual
recommendation.
If medications have to be taken then the lowest effective dose should be taken.
The modafinils should be avoided in pregnancy.Medications and Pregnancy
Category C: Animal reproduction studies have shown an adverse effect on the fetus and there are no adequate
and well-controlled studies in humans, but potential benefits may warrant use of the drug in pregnant women
despite potential risks.
Hoque R and Chesson A. Conception, Pregnancy, Delivery, and Breastfeeding in a Narcoleptic Patient
with Cataplexy. Journal of Clinical Sleep Medicine, p.601-603, 4:6, 2008Medications and Pregnancy
In 2015 the FDA replaced the A, B, C, D and X risk categories, in use
since 1979, with narrative sections and subsections to include:
Pregnancy (includes Labor and Delivery):
Pregnancy Exposure Registry
Risk Summary
Clinical Considerations
Data
Lactation (includes Nursing Mothers)
Risk Summary
Clinical Considerations
Data
Females and Males of Reproductive Potential
Pregnancy Testing
Contraception
Infertility
FDA/CDER SBIA Chronicles. Drugs in Pregnancy and Lactation: Improved Benefit-Risk Information. Accessed
August 1, 2019 at https://www.fda.gov/files/drugs/published/%22Drugs-in-Pregnancy-and-Lactation--Improved-
Benefit-Risk-Information%22-January-22--2015-Issue.pdfModafinil and Pregnancy:
Post marketing surveys have shown that modafinil
increases the risk of fetal malformations.
Fetal malformations 17.3%, and cardiac anomalies 4%
(cf 3% and 1%).
Canadian Product Monograph (CPM) included a
contraindication to the use of modafinil in pregnancy,
Teva Canada, Pregnancy Registry 2018 ReportComplications During Pregnancy: Summary There are no clinically significant increased complications in pregnancy in narcolepsy patients.
Narcolepsy and Delivery:
Most narcolepsy patients have vaginal delivery without
complications.
Rarely, patients may have cataplexy that interferes with
delivery.
If caesarian is required there are no increased
anaesthetic or surgical risks.Medications and the Fetus in Narcolepsy:
Summary
The perceived risks of narcolepsy medication during
pregnancy to mother and fetus are usually overestimated.
The most vulnerable period to the fetus from medications is
after 18-60 days of conception.
The risk of teratogenic effects from narcolepsy medications,
other than modafinil, in therapeutic doses is essentially
nonexistent.Medications and Breast Feeding in
Narcolepsy: Summary
Hypnotics should not be used.
Newer antidepressants generally are safe to use.
Stimulants in therapeutic doses are unlikely to adversely affect
the infant.
Sodium oxybate may have a sedative effect on the infant and is
best avoided.
Ultra caution: timing express breast milk after or before dosing.GHB and Breast Milk
32 year old female, 9th week of lactation, 4.5 gms sodium oxybate
Blood Concentrations Breast Milk Concentrations
GHB is eliminated from breast milk 5 hours after ingestion
Busardò FP, et al. Determination of GHB levels in breast milk and
correlation with blood concentrations. Forensic Sci Int. 2016 Feb 17;265:172-181.Agents Under Investigation New Forms of Sodium Oxybate Once a night formulation - Avadel Low sodium formulation - Jazz GABA-A antagonists Clarithromycin Flumazanil Pentetrazole (BTD-001) - Balance Therapeutics GABA–B receptor agonists Baclofen Norepinephrine Reuptake Inhibitors (NERIs) Reboxetine - Axsome H3R inverse agonists SUVN-3031 - Suven
Narcolepsy Treatment
• First line: sodium oxybate; narcolepsy NT1 and NT2:
Sodium oxybate is the most effective medication for cataplexy and the only
medication that can treat all the symptoms of narcolepsy.
• Second line: Sleepiness/cataplexy: pitolisant
Sleepiness: modafinil / armodafinil, solriamfetol
Cataplexy: venlafaxine or atomoxetine
• Third line: Methylphenidate, amphetamines
The combination of sodium oxybate and modafinil produces the most
effective treatment of excessive sleepiness.Treatment Algorithm
• Trial of sodium oxybate (SXB) in all NT1 and NT2 patients if
acceptable to patient and no contraindications.
• If SXB not fully effective for EDS then add solriamfetol.
• If SXB not fully effective for cataplexy then add pitolisant.
• If unable to take SXB: Trial of pitolisant (Pit).
• If Pit not fully effective for EDS then add solriamfetol.
• If Pit not fully effective for cataplexy then add venlafaxine.
• If Pit contraindicated or unacceptable, then use solriamfetol.
• If cataplexy is present, after stabilizing on solriamfetol, add a
NERI, such as venlafaxine.
• Rationale: SXB and Pit are the only medications that treat
both REM abnormalities and EDS.Conclusion
Narcolepsy with cataplexy is an autoimmune disorder associated with
hypocretin loss.
Narcolepsy without cataplexy may be due to subtle loss of hypocretin.
Idiopathic hypersomnia may be a variant of narcolepsy.
An infection may be the commonest cause of precipitating narcolepsy
Sodium oxybate is the most effective medication in narcolepsy
Alternative treatments are: pitolisant, solriamfetol, armodafinil,
norepinephrine reuptake inhibitors.
Narcolepsy medications (other than modafinil) in therapeutic doses have
not been shown to be harmful to the mother or fetus.You can also read