Vertebrae and Vertebral column
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Lecture 04
Development of the
Vertebrae
and
Vertebral column
By
Dr Farooq Khan Aurakzai
Dated: 01.03.2021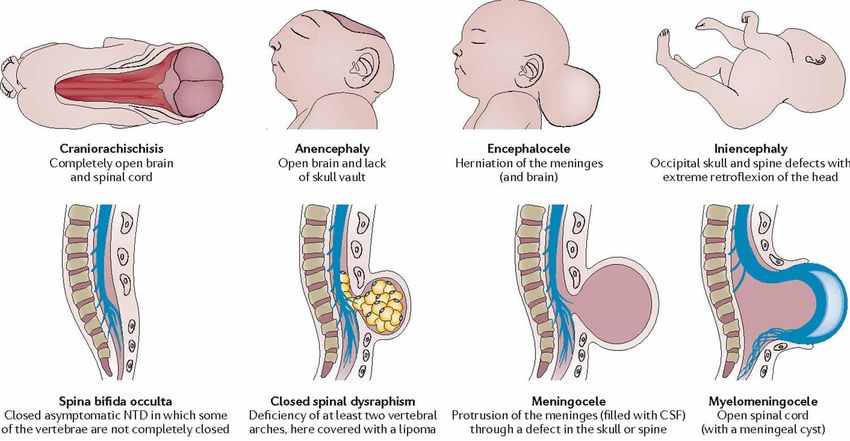
INTRODUCTION
Development of vertebrae
By about 28 days, the notochord
fully demarcates the midline of the
embryo and induces the formation
of the vertebral column around it.
Dorsal to the notochord, the
ectoderm forms the neural tube,
which differentiates into the brain
and spinal cord.
INTRODUCTION
development of vertebrae…….con’t
On each side of the notochord, the
mesoderm of the embryo is thickened to
form a longitudinal mass known as
the paraxial mesoderm.
By the 21st day of development, the paraxial
mesoderm starts to be marked by transverse
clefts across its dorsal surface.
These clefts separate the paraxial mesoderm
into segments called somites.
The first somites appear in the region of the
head, and others appear successively
caudally.
By about the 30th day of embryonic Figure showing:
development, a total of 42–44 somites are A dorsal view of an embryo with 10 somites.
formed.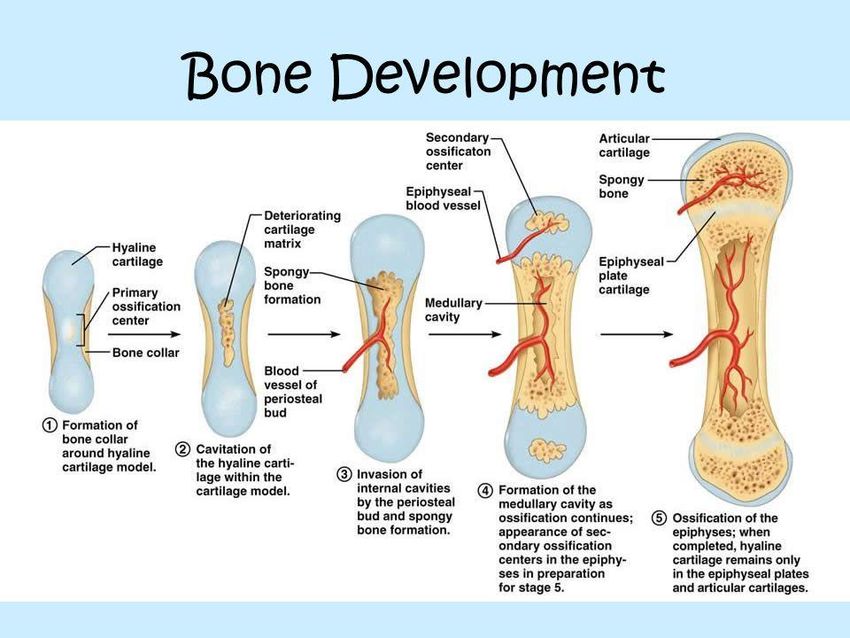
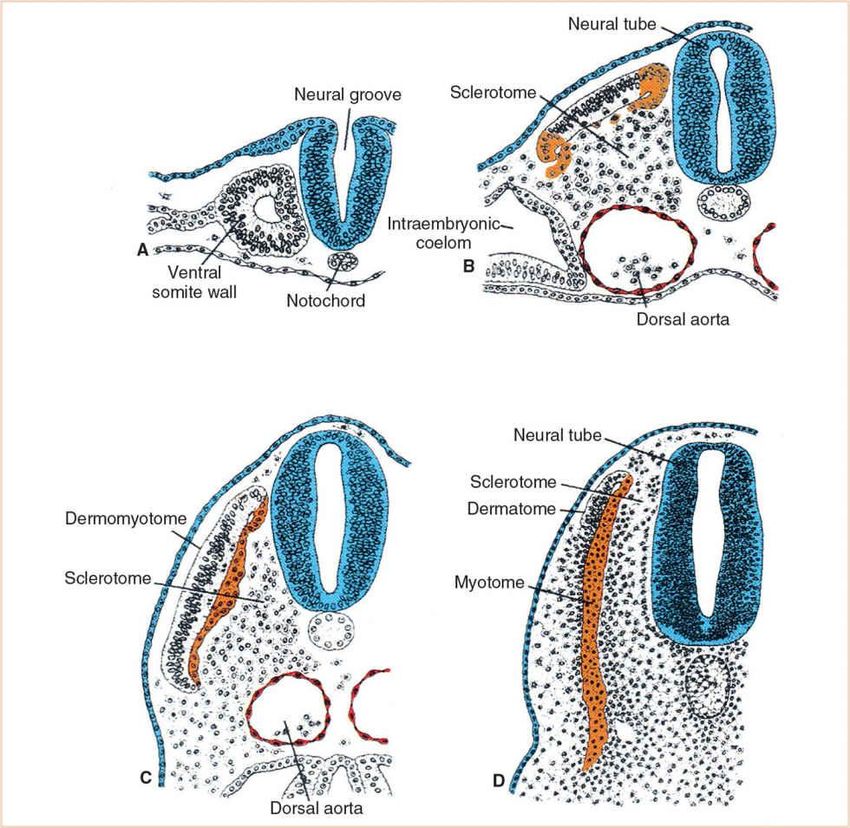
Skeletal System All skeletal tissue arises from cells with a Mesenchymal morphology. Origin of the mesenchyme: Paraxial mesoderm Somatic layer of lateral plate mesoderm. Neural crest

PARAXIAL MESODERM Somitomeres (in head region)and somites (from occipital region caudally. Somites differentiate into: Sclerotome And Dermo-myotomes.
Derivatives of the PARAXIAL mesoderm
SCLERETOME Form loosely woven tissue, the MESENCHYME Mesenchymal cells can migrate and differentiate in many ways(fibroblasts, chondroblast or osteoblasts) Forms: Base of occipital bone (in part), vertebral column and ribs.
LATERAL PLATE mesoderm (Somatic layer) Contributes mesenchyme to the formation of the shoulder and pelvic girdles and bones of the limbs
Neural crest mesenchyme Forms bones of the face and skull. Occipital somites and somitomeres also contribute to part of the vault and base of skull.
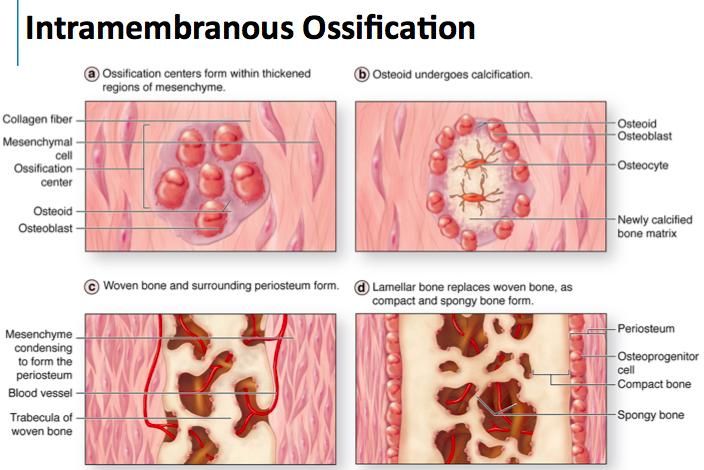
OSSIFICATION INTRAMEMBRANOUS OSSIFICATION: First membranous sheets which later are ossified. ENDOCHONDRAL OSSIFICATION: First a cartilaginous model, then ossification starts.
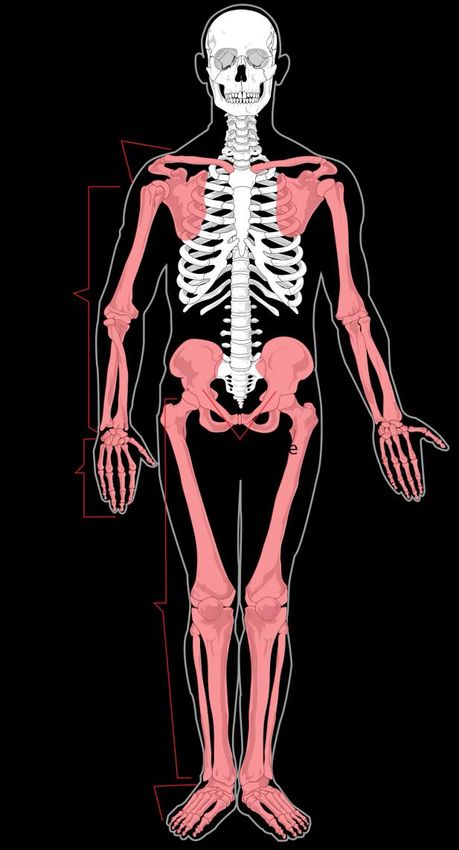
Vertebrae and Vertebral Column Composed of 33 vertabrae and divided inti: CERVICAL REGION: Include highly specialized atlas and axis that link the vertebral column to the skull. THORACIC REGION: Form which the ribs arise. LUMBER REGION: SACRAL REGION: Vertebrae are fused into a single sacrum and CAUDAL REGION: Represents the tail in most mammals and the rudimentary coccyx in humans.
Vertebrae and Vertebral Column They are: Separated by Fibrocartilaginous INTERVERTEBRAL DICS secured to each other by: Interlocking processes and Binding of ligaments. This structural arrangements permits only limited movement between adjacent vertebrae but extensive movement for the vertebral column as a whole. Between the vertebrae are opening called intervertebral foramina that allow passage of spinal nerves.
CURVATURES of Vertebral Column A Striking feature is the presence of curves. There are four of these in the Sagittal plane. PRIMARY CURVES: concave forward in the thoracic and sacral region. SECONDARY or COMPENSATORY CURVES: Convex in the cervical and lumber regions. These four vertebral curves are not present in a newborn.
CURVATURES OF THE VERTEBRAL COLUMN CERVICAL CURVE: Begins to develop at 03 months as the baby begins holding up its head , and it becomes more pronounced as the baby learns to sit up. LUMBEDR CURVE: Results from the assumption of upright sitting posture, and is further accentuated when he learns to walk.
CURVATURES OF THE VERTEBRAL COLUMN In PRIMARY CURVES----difference between the front and back height of the bodies of their respective vertebrae while in COMPENSATORY CURVES, the bend is accounted for mainly by corresponding difference in height in the intervertebral discs. The most anterior part of the cervical convexity is the front of the body of C4. The body of T7 0r T8 usually forms the point of greatest posterior projection in the curve. Sacrum in women is turned back to a greater extent. This would make a more prominent lumbosacral angle, but it is modified by the lumber curve becoming more pronounced: thus in women the 4th lumber is usually more prominent forward than in men.
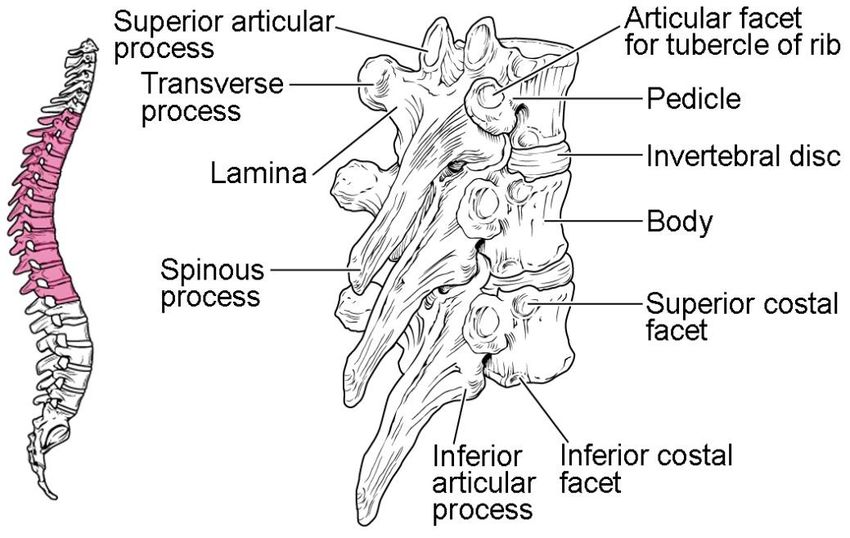
GENERAL STRUCTURE OF VERTEBRAE
INTERVERTEBRAL DISCS Two components: NUCLEUS PULPOSES: Central, gel like , 80 -90 % water and 15- 20% collagen fibrils and GAGS. ANNULUS FIBROSUS: Peripheral, Fibrocartilaginous material, 50- 60% collagen. Allows flexibility between vertebrae for movements of the entire spin al column. Disc is Avascular and Aneural so healing of a damaged disc is unpredictable and not promising Disc rarely fails under compression. Vertebral body will usually fracture before damage to disc occurs.
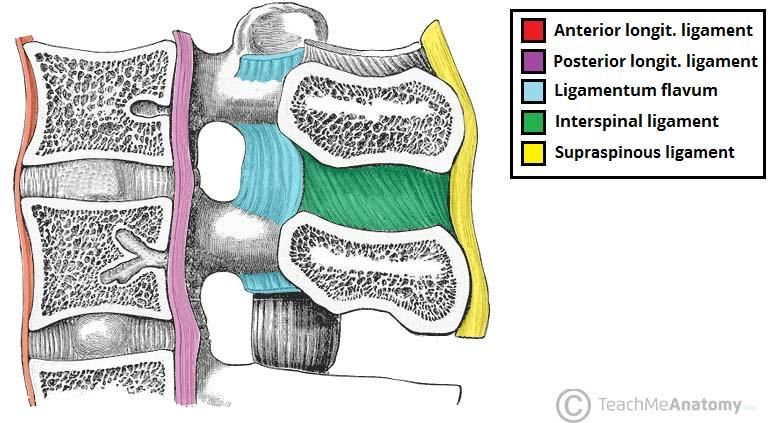
JOINTS & LIGAMENTS JOINTS: Symphysial Synovial Fibrous LIGAMENTS: Anterior Longitudinal Posterior Longitudinal Ligamentum flavum: aids in extension following flexion of the trunk Interspinous Supraspinous Inter transverse
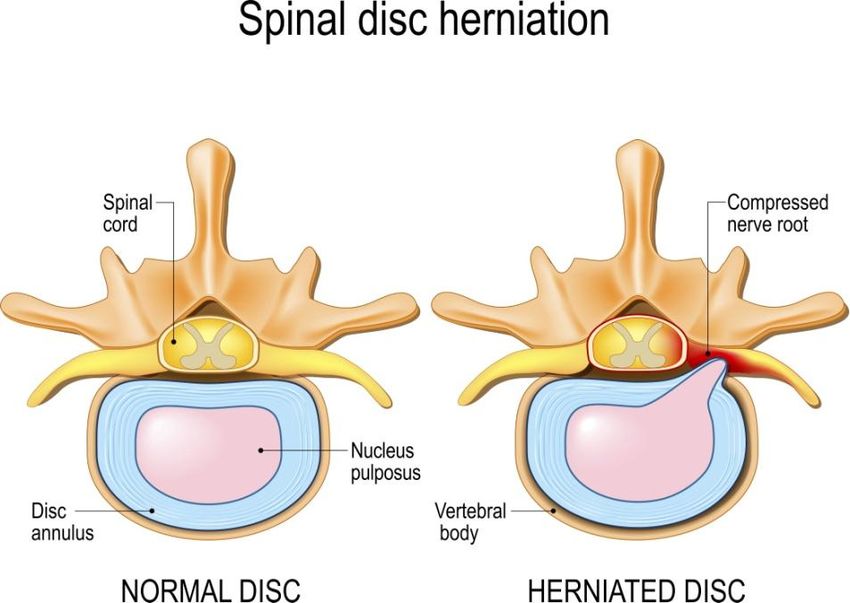
Herniated Discs NP protrudes out from between the vertebrae Nerves are impinged by the bulging NP. Lead to numbness /pain
DEVELOPMENT of Vertebrae Vertebrae are formed from the sclerotome component of the somites. SHH and Noggin gene Pax 1 VENTRAL PORTION OF THE SCLEROTOME surrounds the notochord and forms the CENTRUM, the rudiment of the vertebral body. DORSAL COLUMN OF THE SCLEROTOME surrounds the neural tube and forms the NEURAL ARCH, the rudiment of the vertebral arch.
MOLECULAR REGULATION OF SOMITE
DIFFERENTIATION
1. The secreted protein products of
the noggin gene and sonic hedgehog
(SHH), produced by the notochord
and floor plate of the neural tube,
induce the ventromedial portion of
the somite to become
SCLEROTOME.
2. SCLEROTOME cells express the
transcription factor PAX1, initiating
cascade of cartilage and bone forming
genes for vertebral formation.Development of spinal nerve The spinal nerves develop segmentally; i.e:, each spinal nerve emerges at the same level as the corresponding somite., Then how the spinal nerves escape from the developing vertebrae?? A related question is why eight cervical sclerotome produce seven cervical vertebrae, whereas in the rest of the vertebral column there is a one to one correspondence of sclerotome to vertebrae.
Development of spinal nerve The answer to these questions is that the sclerotome split and recombine to produce vertebral rudiments that lie intersegmentaly. Each sclerotome splits into a loose cranial half and a compact caudal half.
development of spinal nerve…..con’t As the segmental spinal nerves grow out to innervate the myotomes the caudal half of each sclerotome fuses with the cranial half of the succeeding sclerotome. The resulting composite structure produces a vertebra that lies intersegmentaly.
DEVELOPMENT Seven cervical vertebrae form from eight cervical somites because the : Cranial half of C1 sclerotome fuses with the caudal half of the 0ccipital sclerotome and contributes to the formation of the base of the skull. The caudal half of the C1 sclerotome then fuses with the cranial half of the C2 sclerotome to form the first cervical vertebra (the Atlas), and so on down the spine. The C8 sclerotome contributes its cranial half to the C7 vertebra and its caudal half to T1 vertebra.
DEVELOPMENT of IV disk The notochord degenerates and disappears where it is surrounded by the developing vertebral bodies. Between the developing vertebral bodies the notochord expands to form the gelatinous center of intervertebral disc- the NUCLEUS PULPOSUS. This nucleus is later surrounded by fibres that form the ANNULUS FIBROSUS. NP and AF together contribute the IV DISC.
OSSIFICATION OF VERTEBRAL COLUMN Each typical vertebra has 03 primary ossification centers. One for CENTRUM One for each half of the NEURAL ARCH. 05 secondary ossification centers develop during puberty in each typical vertebra. One for tip of spinous process. One for the tip of each transverse process. 02 Annular Epiphyses (ring epiphyses)– one on superior and one on inferior edge of the Centrum. Unite with vertebral body in early adulthood.
NEURAL TUBE DEFECTS
SPINAL DYSRAPHISM
• Spinal dysraphism is a generic term covering a wide rang of developmental abnormalities
of the vertebral column and spinal cord characterized by a failure of fusion of midline
structure.
• The spectrum of defects includes:
• Non fusion of the entire neural tube with no vertebral arch development (CRANIO-
RACHISCHISIS).SPINAL DYSRAPHISM Non fusion of the rostral portion of the neural tube with no calvarial or occipital development (ANENCEPHALY); and Non fusion of caudal portions of the neural tube and local failure of vertebral arch development (SPINA BIFIDA). Spina bifida may be obvious at birth of before (e.g)SPINA BIFIDA CYSTICA or SPINA BIFIDA APERTA), or not obvious at birth (SPINA BIFIDA OCCULTA).
NTDs related to spinal cord NTDs originate during 3rd week of development. A failure of part of the neural tube to close not only disrupts the differentiation of the CNS but also disrupts the induction of the overlying vertebral arches, so that the arches remain underdeveloped and fails to fuse along the dorsal midline to enclose the vertebral canal. The resulting open vertebral canal is a condition called SPINA BIFIDA. In some cases of spina bifida, the contents of the vertebral canal bulge into a membranous sac (cele) that is continuous with the surrounding skin.
SPINA BIFIDA OCCULTA The mildest defect in this spectrum. Vertebral arches of a single vertebra fail to fuse, but the underlying neural tube differentiates normally and does not protrude from the vertebral canal . This condition, known as spina bifida occulta, may occur anywhere along the spinal cord bit is most common at lower lumbar or sacral levels.
SPINA BIFIDA OCCULTA The location of the defect is frequently indicated by a tuft of hair induced by the underlying abnormality, or by an angioma, pigmented nevus or a dimple. Spina bifida occulta usually produces no clinical symptoms. A small percentage of affected infants have functionally significant defects of the underlying spinal cord and dorsal roots.
SPINA BIFIDA CYSTICA(APERTA {Open- up})
Collectively covers the more severe forms of
this defect.
MENINGOCELE:
The dura and the arachnoid protrude from the
vertebral canal in the affected region.
MYELOMENINGOCELE:
If neural tiissue as well as Meninges protrudes.
The neural tube defects in this series may not be fatal,
but when they are severe, the spinal cord and spinal
nerves involved in a myelomeningocele, for example,
often fail to develop normally, resulting in dysfunction
of pelvic organs and legs.Different types of meningoceles.
MYELOSCHISIS or RACHISCHISIS The most severe defects of neural tube development are those in which the neural folds not only fail to fuse but also fail to differentiate, inviginate and finally separate from the surface ectoderm, failure of the neural tube to close at one or several levels in the spinal cord region results in an anomaly called MYELOSCHISIS. It is rare, but serious condition, and results in paralysis.
Anencephaly and cranio-rachishisis Means “lack of brain” occurs when the cranial neuropore fails to close Neural tissue fails to differentitate and the vault of skull does not close over it. This condition is called exencephaly, anencephaly or craniorachishisis. Anencephalic embryos have prominent eyes lying at the base of the skull, often survive to late fetal life or to term but invariably die with in a few hours or days after birth.
THANK YOU…..
You can also read