Viral-vector based immunotherapies to transform the fight against cancer and infectious diseases - January, 2019 - Transgene
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Viral-vector based immunotherapies
to transform the fight against cancer
and infectious diseases
January, 2019
Disclaimer
This presentation contains forward-looking statements, which are subject to numerous risks and uncertainties,
which could cause actual results to differ materially from those anticipated. There can be no guarantee that (i) the
results of pre-clinical work and prior clinical trials will be predictive of the results of the clinical trials currently
under way, (ii) regulatory authorities will agree with the Company’s further development plans for its therapies, or
(iii) the Company will find development and commercialization partners for its therapies in a timely manner and on
satisfactory terms and conditions, if at all. The occurrence of any of these risks could have a significant negative
outcome for the Company’s activities, perspectives, financial situation, results and development.
For a discussion of risks and uncertainties which could cause the Company's actual results, financial condition,
performance or achievements to differ from those contained in the forward-looking statements, please refer to the
Risk Factors (“Facteurs de Risques”) section of the Document de Référence, available on the AMF website
(http://www.amf-france.org) or on Transgene’s website (www.transgene.fr). Forward-looking statements speak
only as of the date on which they are made and Transgene undertakes no obligation to update these forward-
looking statements, even if new information becomes available in the future.
2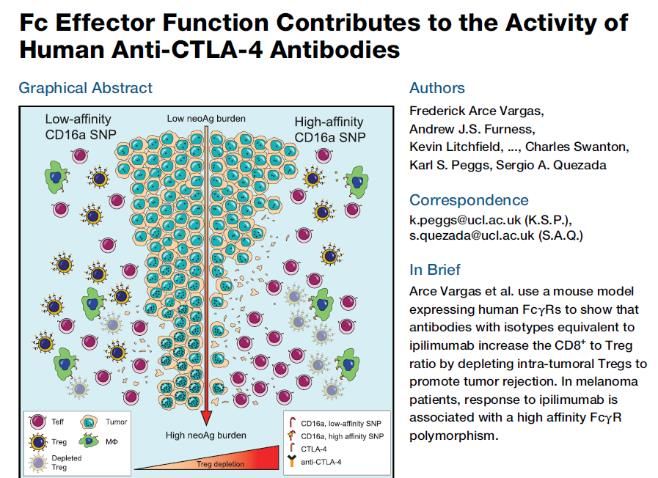
Focused on enhancing our leadership in viral vector-based
immunotherapies
Mature Clinical Assets Early-Stage Clinical Technology Platforms
Assets
TG4010 TG4001
TG6002
Pexa-Vec TG1050
First candidates
in clinic in 2019 3
World leader in viral-vector based immunotherapies
Experience driven innovation
Clinical pipeline Our new cutting edge
technology platforms
TG 4010
THERAPEUTIC
TG 4001
VACCINES
TG 1050 WORLD
Informed LEADING
decisions
SCIENCE
ONCOLYTIC PEXA-VEC
VIRUSES TG6002
First candidates in
clinic in 2019
4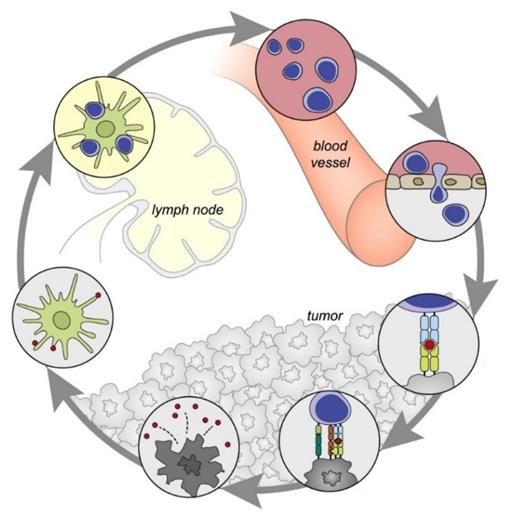
Broad pipeline of clinical-stage immunotherapies
Transgene strategic trials are poised to deliver key read out in 2019
Preclinical Clinical Phase
Product Indication
Phase 1 Phase 2 Phase 3 Next Key Milestone
THERAPEUTIC VACCINES
Non-small cell lung cancer –
*
2H 2019:
TG4010 1st line + nivolumab (ICI) + CT
ORR (35 patients)
Recurrent HPV-positive head 2H 2019:
TG4001 and neck cancers
*
+ avelumab (ICI) First efficacy date
TG1050 Chronic hepatitis B + antiviral **
Potential partnership
ONCOLYTIC VIRUSES
Advanced HCC – 1st line
2H 2019:
+ sorafenib
Pexa-Vec (PHOCUS) *** Intermediary readout
Mid 2019:
Advanced HCC – 1st line + nivolumab (ICI)
ORR (15 patients)
TG6002 Colorectal cancer ** TBC
* Clinical collaboration / ** Rights acquired for Greater China
***Transgene has commercial rights to Pexa-Vec in Europe and additional selected countries. 5
Therapeutic Vaccines Pioneering virus-based immunotherapeutics
Lung cancer | Better therapeutic options still needed
for non-responders (ICIs)
≈30 % of 1L patients whose tumor
cells express high levels
of PD-L1 (≥ 50 %)
➔ Pembrolizumab registered
Most patients still diagnosed since 2016
at late stages, with dismal
Non-small cell lung cancer ≈70 % of 1L patients whose tumor
prognosis cells express no or low levels of PD-L1
First-line therapy
Min. 350 K patients * (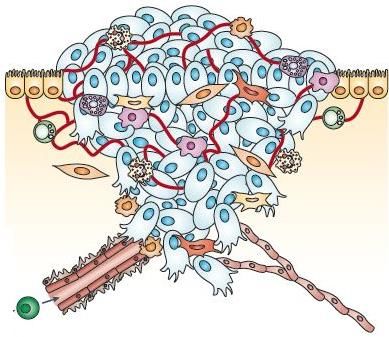
TG4010 | Compelling lung cancer clinical data
Improved response rate & duration of response
SUCCESSFUL PHASE 2B TRIAL (RANDOMIZED, PLACEBO-CONTROLLED, 222 PATIENTS)
TG4010 in combination with chemotherapy for 1st line NSCLC
TG4010 Placebo
TG4010 + chemotherapy
40.9 [23.9 – 54.1] wks + CT + CT
Non-squamous (n) 98 98
ORR 40% 28%
Median duration of response (wks) 41 18
Chemotherapy (n=27)
18.1 [13.7 – 36.4] wks ✓ Improved response rate
Placebo + chemotherapy
18.1 [13.7 – 36.4] wks
& duration of response
✓ Good safety profile
Source: Quoix, E. et al., TG4010 immunotherapy and first-line chemotherapy for advanced non-small-cell lung cancer (TIME): results from the phase 2b part of a
randomised, double-blind, placebo-controlled, phase 2b/3 trial, The Lancet Oncology, Dec. 2015, (17:212) 8
TG4010 | Compelling lung cancer clinical data
Well positioned for further development in NSCLC
SUCCESSFUL PHASE 2B TRIAL (RANDOMIZED, PLACEBO-CONTROLLED, 222 PATIENTS)
TG4010 in combination with chemotherapy for 1st line NSCLC
Progression-free survival (months) Overall survival (months)
Patients with non sq. tumors (n=196) Patients with non sq. tumors (n=196)
✓ Significant improvements
in PFS and OS in patients
in patients with non sq.
tumors
35%
36% ✓ Clinical efficacy
19%
in both PD-L1 negative
TG4010 + chemotherapy
Placebo + chemotherapy
TG4010 + chemotherapy
20%
and PD-L1 positive
Placebo + chemotherapy
patients
Source: Quoix, E. et al., TG4010 immunotherapy and first-line chemotherapy for advanced non-small-cell lung cancer (TIME): results from the phase 2b part of a
randomised, double-blind, placebo-controlled, phase 2b/3 trial, The Lancet Oncology, Dec. 2015, (17:212) 9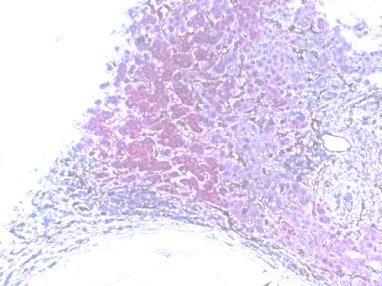
TG4010 1L | To increase ORR with triple combination regimen in patients with non sq. NSCLC expressing low levels of PD-L1 (
TG4001 | HPV-positive Head & Neck Cancers (HNSCC)
Phase 1b/2 in combination with avelumab (Bavencio®)
MVA encoding for HPV16 E6 & E7 and IL-2
In collaboration with
Endpoints (Phase 2 part)
• Primary endpoint: Objective response rate (ORR)
• Secondary endpoints: progression-free survival (PFS), overall
survival (OS), duration of response and safety
• First patient treated in September 2017
Principal Investigator • Following positive safety evaluation,
• Pr Christophe Le Tourneau, Institut Curie Phase 2 part ongoing and additional sites being activated
Protocol
• Up to 50 patients (France)
• Multi-center, single-arm, open label trial Phase 1 results in 4Q 2018 (n=9 patients)
• Metastatic or refractory/recurrent HPV-16+ head & Next clinical readout expected in 2H 2019
neck cancer, after failure of standard therapy
11TG1050 | Positive Phase 1 results (safety and immunogenicity)
Adeno encoding for 3 HBV antigens Phase 1 results presented at AASLD 2018
(n=48 patients)
Principal investigator
• Prof Fabien Zoulim, Hospices civils, Lyon (France) ✓ Primary endpoint met: good safety profile confirmed
• Participating countries: Canada, France, Germany ✓ TG1050 triggers T cell-based immune responses, specific
Protocol of all 3 encoded HBV antigens
• Up to 48 patients ✓ Intermediate dose (1010 vp) consistently immunogenic
• Randomized safety and dose-finding study (≈70% of patients)
• Patients currently being treated with SoC antiviral ✓ New preclinical data support further investigation in
therapy combination with antivirals and immunomodulators
Rights for Greater China acquired
by Tasly Pharmaceuticals (July 2018)
12TG1050 | Key findings of the positive Phase 1 trial
Safety: Clinical trial primary end-point reached. Subcutaneous SD & MD injections of TG1050 in Number of patients
NUC-suppressed CHB patients is well tolerated over the 3 DLs. No negative impact on disease with low anti-Ad5 pre-
control, especially in the sensitive part of patients with no pre-immunity against the adenoviral immunity per dose
vector, reinforces the robust safety profile of TG1050. group responding to at
Immunogenicity: TG1050 induces HBV-specific cellular immunity (IFN-g cells) in NUC-suppressed least 1, 2 or 3 antigens
0
CHB patients without or with low anti-Ad5 pre-immunity. Induced responses are specific of single
or multiple antigens expressed by TG1050 (Core/Pol & Env). Detection of Env-specific responses is
encouraging in a highly tolerogenic context for this antigen. Responses are detected following
single and multiple injections: Intermediate dose 1010 vp is consistently immunogenic (~70% of
patients).
HBsAg evolution: HBsAg decline reaches ≈0.4 log over time in 2 patients of 1010 vp group.
Heatmap of ELISpot
responses. Patients
with low anti-Ad5
pre-immunity are
listed as lines and
test conditions as
columns
Individual evolution of ELISpot responses over time in patients with low anti-Ad5 pre-immunity
Detectable responses in
both SD & MD cohorts at
1010 & 1011 vp doses ;
Env-specific responses
detected despite
TG1050 encoding for
only small domains of
Env/HBsAg as well as the
very high tolerance
against HBsAg
characterizing CHB
carriers.Entering the field of individualized immunotherapies using our unique proven MVA based platform
myvacTM |Individualized immunotherapy platform
Targets patients’ neoantigens
Immunotherapy MVA-based therapeutic vaccine
Safety Therapeutic class with established track-record
Efficacy Proven anti-tumor activity
Individualized One cancer, One patient, One vaccine
The advantages of
personalised treatment Flexible Versatile platform and AI integration
without the drawbacks of
autologous approaches Clinical First trials will start in 2019
15myvacTM | Transgene’s vaccine expertise provides the insights
needed to leverage multiple cutting edge technologies
Artificial
Intelligence
Gene
editing
Genome
sequencing
16myvacTM | Targeting unique patient specific set of mutations
• Because of deficient repair mechanisms and rapid proliferation,
tumor cells accumulate DNA mutations
• Some mutations lead to the generation of non-self proteins (therefore
immunogenic)
• These neoantigens are more immunogenic than “classical” tumor associated
antigens
Transgene’s myvac vaccines against neoantigens are expected
to induce broader and stronger T cell responses
17myvac™ network combines bioengineering & digital transformation
Identify patients eligible Manufacture
Secure and exploit Select the most Realize clinical
for individualized myvac™ product in
genomic data relevant neo-antigens proof of concept
immunotherapies controlled time and cost
100
Percent survival
50
Vaccin
Placebo
0
0 50 100 150
Time (days)
World renown US
and UK clinical
centers
18| Clinical protocols being finalized with 2 international KOLs
Dr Christian Ottensmeier presenting at SITC 2018 HPV negative
After surgery
head and neck
and adjuvant therapy
cancers
After surgery
Ovarian cancer and adjuvant
chemotherapy
Trials are expected to start in 2019
(Europe & USA)
19Oncolytic Viruses – Pioneered by Transgene A new and highly promising therapeutic class in the fight against cancer. Transgene leading the development of multifunctional OVs for the enhanced modulation of the TME via a single therapeutic.
Pexa-Vec | Lead oncolytic virus
Global
clinical development plan
Transgene owns development
HCC 1L Other solid tumors
and commercialization rights
in Europe • Global Phase 3 trial • Exploratory Phase 2 trials
• Combination Phase 2 trial conducted by Transgene
Licensor: SillaJen conducted by Transgene • Exploratory Phase 1 trials
(KOSDAQ: 215600) led by SillaJen (RCC 2L,
CRC 2L/3L)
21Pexa-Vec | Large unmet medical need in HCC
First-line therapy
• Sorafenib - modest activity
– ORR: 2% ; median OS: 10.7 months
Dismal prognosis
• Lenvatinib recently approved with non-inferiority results (USA, EU, Japan)
• Nivolumab could become a new therapeutic option: Promising activity
Better therapeutic in Phase 3 (still ongoing)
options needed
Second-line therapy
25,000 eligible patients • Regorafenib
– ORR: 10%; median OS: 10.6 months
in Europe*
• Nivolumab approved by FDA (2017)
– ORR: 18%; median OS: 15.6 months
• Pembrolizumab approved by FDA (2018)
– ORR: 17%, median OS: 12.9 months
* Source: Globocan, Company estimates
22Pexa-Vec | Key Phase 2 clinical trial results
Clinical activity demonstrated in multiple trials
Trials with >300 patients treated with Pexa-Vec in variety of tumor types, including
liver, colorectal and kidney
Proof of concept for MOA: active immunotherapy
30-patient dose-finding Phase 2 trial in HCC
(80% of patients first-line)
• OS results - high dose versus low dose
– Median OS: 14.1 (high dose) vs. 6.7 months (low dose)
– Hazard Ratio = 0.39
– p = 0.020
Nature Medicine, Volume 19, Issue 2, February 2013
23Pexa-Vec | Triggers antitumor immunity after single IV administration
Prior to planned surgery of locally advanced, poor prognosis or metastatic cancers
Single IV Pexa-Vec
Pexa-Vec shown to Surgery Post-surgery
• Selectively target tumor tissue after single IV administration d1 d2 d3 d5 d14 ± 4d 1m 3m
• Stimulate the adaptive and innate anti-tumor immune response
Peripheral blood samples collected
• Induce expression of PD-L1 and PD-1 pathways
n = 8 ; 3 with metastatic melanoma and 5 with colorectal cancer metastases to the liver (CRLM)
One complete and one partial tumor pathological response PBMCs exhibited robust activation by 24 hrs post-infusion
at the time of surgery on four evaluable CRLM patients • Expression of CD69 (an early activation marker) was
enhanced on effector cell populations, notably NK & T cells
Tumor-specific adaptive T cell
responses (T cell Elispot) • Expression of PD-L1 was increased
Presence of Pexa-Vec
in tumor tissue Patient : Mel. CRLM CD69 PD-L1
TAA : MART1 CEA
Normal tissue
Pre-
infusion
CRLM tissue showing expression of 1 month
Pexa-Vec, signs of inflammation and post-
fibrosis, necrotic cells infusion
Data support ongoing development of Transgene’s Vaccinia virus-based oncolytics
Source: Samson, A. et al, Single intravenous preoperative administration of the oncolytic vaccinia virus Pexa-Vec to prime anti-tumor immunity, ASCO 2018, June 2018 24Pexa-Vec | Clinical development plan in HCC - 1st line
Pivotal Phase 3 and combination Phase 2
➔Position Pexa-Vec with current and future standard of care
Advanced HCC Conducted by Advanced HCC Pexa-Vec Conducted by
Pexa-Vec
1st line 1st line + Opdivo®
+ sorafenib Phase 1/2 (nivolumab)
Phase 3
• Multi-center Phase 3 trial in Europe, USA, Asia • Multi-center Phase 1/2 trial in France, Italy, USA
• Randomized, two-arm trial • Open-label, single-arm trial
• Ongoing global recruitment
• First patient included in China in Sept. 2018
• Safety review committee expected before
year-end 2018
First data (efficacy vs SoC) expected in 2019 • Interim analysis (15 patients) expected
mid-2019 (primary endpoint ORR)
25Next Generation of Oncolytic Viruses Transgene’s novel Oncolytic Viruses are based on its optimal Vaccinia virus backbone armed with either chemo or immuno payloads
Oncolytic viruses | Three complementary ways to act on the tumor
Oncolysis
Specific replication in tumor cells, and
direct lysis of infected cells
Immune response
Induction of immunogenic cell death,
engagement of both innate and
adaptive anti-tumor immunity
Immuno-modulating payloads delivery
Many routes to Targeted delivery of anti-tumor
reach the tumor modalities, synergistic with other
(i.e. IV, IT)
MOAs (e.g. targeted CT, or immune
modulation of TME)
27Vaccinia virus (VV) | The optimal oncolytic backbone
• Excellent Oncolytic activity of the Copenhagen vaccinia strain
• Good immunological balance (Th1 vs Th2, anti-tumor vs anti-
viral responses, etc.)
• Large genome capacity (up to 25 kb), to accommodate
multiple transgenes
• Tumor selective replication in numerous cancer cell types, and
good safety profile
• Pure cytoplasmic replication (no risk for genome integration
or mutagenesis)
• Well-established processes for GMP manufacturing
28VVCOPTK-RR- | Targets a large spectrum of human tumors
Replication Oncolytic activity
20 tumor cell lines, MOI 10-3, 48 hrs post-infection 10 cell lines, MOI variable, day 5 post-infection
100
105
Magnitude of replication
104 80
% surviving cells
103 60
102 40
10 20
0
MIA
Hela
HepG2
U87MG
A549
SKOV3
PaCa2
U118MG
SNU5
CAL33
HCT116
SK-Mel1
PANC1
Hs746T
UMUC3
SW780
LoVo
OE21
OE19
OVCAR3
KATO3
29TG6002 Our VV oncolytic backbone enhanced by tumor targeted chemotherapy
TG6002 | Advanced OV already in the clinic
Viral oncolysis + local production of chemotherapy
Multiple Advantages:
1. Excellent oncolytic properties
2. Highly tumor selective
3. IV delivery
4. Targeted chemotherapy with FCU1 gene
- allowing the production of 5-FU in the tumor
TG6002
FCU1 gene
• Unique and proprietary • No FCU1 related safety issue
• High 5-FC to 5-FU conversion rate • Preclinical results confirm potency
Greater China rights acquired by Tasly Biopharmaceuticals as part of a $48 million (July 2018)
31TG6002 | Significant anti-tumor activity in multiple human cell lines
Example: Evaluation of systemic injection of TG6002 in the colorectal cell line (LoVo)
P < 0,05
P < 0,005
TG6002+5-FC
• Mice: n=12
Similar results with other cell lines:
pancreas (MiaPaca2); glioblastoma (U-87MG), esophaegal (OE19), stomach (HS746T), hepatocarcinoma (Hep G2)
32TG6002 | In Phase 1/2a GI cancer clinical study
Viral oncolysis + local production of chemotherapy administered IV
Gastro-intestinal adenocarcinoma with liver metastasis (colon cancer)
(Tumors known to be 5-FU sensitive)
Protocol Regimen
• Multi-center Phase 1/2a trial • TG6002 IV: D1, D8, D15 + 200 mg/kg/day
• Phase 1 part (dose escalation): up to 24 patients • Oral 5-FC prior to TG6002
• Phase 2a part (efficacy): 35 patients • Additional cycles until disease progression
• Trial will include biodistribution analysis
Principal investigator • INDs granted in Belgium, Spain, France
• Prof Philippe Cassier, centre Léon Bérard
(Lyon, France)
• First patients recruited in Q4 2018
• Expected Ph 1 Readout: H2 2019
33Our new generation oncolytic products The Invir.IOTM Platform: Immuno-armed Vaccinia Virus (VV)
Multiple options for immune modulation of the tumor
micro-environment via immuno-armed oncolytic VVs
Chemokines
Favoring tumor infiltration
Undisclosed sdAbs
Unlocking local immunosuppression
Better release of tumor Ags,
Local expansion, and
and of related immuno-
activation of APC and
stimulatory molecules
effectors cells Degradation of immunosuppressive
hCD Cytokines
metabolites and cells in the TME
TNFR-Ls Undisclosed enzyme
TCEs ICIs
Agonistic sdAbs Anti-CTLA-4
35OV encoding for anti-CTLA-4 mAb
Improving on validated MoA of ipilimumab
Preclinical PoC Building a potent multifunctional OV
• Transgene’s OVs deliver functional mAb in the TME(1) Improved efficacy compared to combination of
separate Ab and OV (1)
• BioInvent’s full length human recombinant anti-CTLA-4
Abs promote depletion of intratumoral Treg cells (2) Longer duration of expression
Expected improved tolerability owing to lower
systemic antibody exposure in peripheral non-
tumor compartments
Indications: multiple solid cancers
In late stage preclinical development
(1) Kleinpeter P. et al., Vectorization in an oncolytic vaccinia virus of an antibody, a Fab and a scFv against programmed cell death -1 (PD-1) allows their intratumoral
delivery and an improved tumor-growth inhibition, OncoImmunology, Oct. 2016 (5:10)
(2) Vargas F. et al., Fc Effector Function Contributes to the Activity of Human Anti-CTLA-4 Antibodies, Cancer Cell, April 2018 (33: 1-15) 36Transgene to deliver multiple value- enhancing clinical data readouts and preclinical milestones in 2019
Significant anticipated value-creating news flow
Portfolio to deliver news flow in the near-term
1H 2019 2H 2019
TG4010 1L NSCLC TG4010 1L NSCLC
Recruitment ORR on 35 patients
completed
Pexa-Vec + nivo 1L HCC TG6002
Phase 1 clinical readout
Safety review
committee Pexa-Vec + nivo 1L HCC
TG4001 SCCHN
Interim analysis (ORR) on 15 patients
First efficacy readout
Pexa-Vec Phase 3 1L HCC Pexa-Vec Phase 3 1L HCC
Futility analysis Interim analysis
1st product in clinic
1st product in clinic
Clinical results Clin. trial milestone Next generation platforms 38Company funded to deliver multiple value generating milestones
Key figures Key shareholders
As of December 31, 2018
Cash and cash equivalents
€ 26.6 million
as of September 30, 2018
Operating revenues
€ 37.5 million as of September 30, 2018 57 %
(incl. the sale of the TG1050 rights in China for €35.6 million)
Free float
43 %
€ 25 million Expected cash burn for 2018
• Market capitalization:
Financial visibility to end September 2019 ~ $200 million as of December 31, 2018
(excl. the potential monetization of the Tasly • 62.3 million shares outstanding
Biopharmaceuticals shares - $48 million) + 0.7 million options and restricted stocks
• Listed on Euronext Paris
• ISIN: FR0005175080 - Ticker: TNG
39Transgene| A world leader in viral-vector based immunotherapies
• Strong late stage clinical pipeline of therapeutic vaccines
• multiple value adding milestones expected in 2019
• Novel myvac – individualised immunotherapy platform results from Transgene’s
significant clinical vaccine expertise
• First clinical trials to start in 2019
• Well positioned to be a best-in-class in oncolytic viruses via the further
development of TG6002 and our Invir.io platform
• Both are based on our proprietary large capacity VVCOPTK-RR- backbone
• First Invir.io product to enter the clinic in 2019
• Adequate financial resources to fund business
40Contact
Jean-Philippe Del
investorrelations@transgene.fr
@TransgeneSA Transgene
400 Boulevard Gonthier d’Andernach - Parc d’Innovation - CS80166
67405 Illkirch Graffenstaden Cedex France
Tél.: + 33 (0)3 88 27 91 21 www.transgene.frYou can also read

















































