Migraine Surgery at the Frontal Trigger Site: An Analysis of Intraoperative Anatomy - Harvard ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Migraine Surgery at the Frontal Trigger
Site: An Analysis of Intraoperative Anatomy
The Harvard community has made this
article openly available. Please share how
this access benefits you. Your story matters
Citation Ortiz, Ricardo. 2020. Migraine Surgery at the Frontal Trigger Site: An
Analysis of Intraoperative Anatomy. Doctoral dissertation, Harvard
Medical School.
Citable link https://nrs.harvard.edu/URN-3:HUL.INSTREPOS:37364944
Terms of Use This article was downloaded from Harvard University’s DASH
repository, and is made available under the terms and conditions
applicable to Other Posted Material, as set forth at http://
nrs.harvard.edu/urn-3:HUL.InstRepos:dash.current.terms-of-
use#LAAScholarly Report submitted in partial fulfillment of the MD Degree at Harvard Medical
School
Date: 27 September 2019
Student Name: Ricardo Ortiz, BSc
Scholarly Report Title: Migraine Surgery at the Frontal Trigger Site: An Analysis of
Intraoperative Anatomy
Mentor Name(s) and Affiliations: William G. Austen Jr., MD, Division of Plastic and
Reconstructive Surgery, Massachusetts General Hospital
Collaborators, with Affiliations: Lisa Gfrerer, MD PhD1; Marek A. Hansdorfer, MD1;
Kassandra P. Nealon, BSc1; Jonathan Lans, MD, Massachusetts General Hospital, Division of
Plastic and Reconstructive Surgery, Boston, MA
Link to and Citation for any publications that you wrote on your scholarly project:
Ortiz R, Gfrerer L, Hansdorfer M, Nealon K, Austen WG. Migraine Surgery at the Frontal
Trigger Site: An Analysis of Intraoperative Anatomy. Plast. Reconstr. Surg. In Press.
1Table of Contents
Abstract: ........................................................................................................................................3
Glossary of Abbreviations .............................................................................................................4
Description of Scholarly Work .....................................................................................................5
Specific aims and significance.........................................................................................5
Student and Collaborator Contributions ......................................................................5
Main Text ....................................................................................................................................6
Introduction.......................................................................................................................6
Methods..............................................................................................................................7
Results............................................................................................................................... 9
Discussion........................................................................................................................ 14
Limitations...................................................................................................................... 15
Conclusions..................................................................................................................... 16
References ...................................................................................................................................17
2Abstract
Purpose
The development of migraine headaches may involve the entrapment of peripheral
craniofacial nerves at specific sites. Cadaveric studies in the general population have confirmed
potential compression points of the supraorbital (SON) and supratrochlear (STN) nerve at the
frontal trigger site. Our aim was to describe the intraoperative anatomy of the SON and STN at
the level of the supraorbital bony rim in patients undergoing frontal migraine surgery and to
investigate associated pain.
Methods
Patients scheduled for frontal site surgery were prospectively enrolled. The senior author
evaluated intraoperative anatomy and recorded variables using a detailed form and operative
report. The resulting data was analyzed.
Results
118 sites among 61 patients were included. The SON traversed a notch in 49%, foramen
in 41%, notch plus foramen in 9.3%, and neither a notch nor foramen in one site. The senior
author noted macroscopic nerve compression at 74% of sites. Reasons included a tight foramen
in 24%, notch with a tight band in 34%, STN and SON emerging via the same notch in 7.6% or
via the same foramen in 4.2%. Preoperative pain at a site was significantly associated with nerve
compression by a foramen.
Conclusions
The intraoperative anatomy and etiology of nerve compression at the frontal trigger site
varies greatly among patients. We report a SON foramen prevalence of 50.3%, which is greater
than previous cadaver studies of the general population. Lastly, the presence of pain at a specific
site is associated with macroscopic nerve compression.
3Glossary of Abbreviations
CT…………………………………………........ Computed tomography
IQR…………………………………………...... Interquartile range
MH…………………………………………....... Migraine Headache
MHI…………………………………………..... Migraine headache index
SD…………………………………………........ Standard deviation
SON………………………………………...….. Supraorbital nerve
STN…………………………………………...... Supratrochlear nerve
4Description of Scholarly Work
Specific aims and significance
Migraine headaches (MH) affect an estimated 28 million people in the United States and
costs an estimated 11 billion dollars to the healthcare system, not including indirect costs from
reduced productivity and missed workdays1,2.
In the last two decades, surgery for migraine headache (MH) has emerged as an effective
modality to treat MH in select patients1-3. Although the use of surgery to treat migraines is not an
entirely new concept, it has only just emerged as an evidence-based treatment in the last 20 years
or so. Dr. Bahman Guyuron, a plastic surgeon regarded as the inventor and pioneer of modern
migraine surgery, discovered its therapeutic potential serendipitously after many of his forehead
rejuvenation patients stated that their migraines had improved postoperatively. This early clue to
its therapeutic potential would later be bolstered by several studies showing its efficacy,
including a randomized placebo-controlled trial that showed complete migraine elimination in
57.1 percent of the surgical arm and in 3.8 percent of the sham operations4-7.
Today there have been thousands of patients who have undergone migraine surgery, but
further research is warranted to fully investigate its effects. The efficacy of surgery for MH
suggests a structural trigger of migraine in these patients, but these specific structural causes
have yet to be fully described anatomically. Previous literature has reported anatomic variation in
the regions around trigger sites4,5, but these variations have not been studied in patients with MH.
Through this study, we aim to describe the intraoperative anatomy associated with migraines at
trigger site I (frontal), a common MH trigger site that is found in 65.6% of patients undergoing
surgery for MH6.
Student and Collaborator Contributions
I was involved in this project from start to finish. I was intimately involved with writing
the protocol with guidance from Dr. Austen and Dr. Lisa Gfrerer, a resident physician who
assisted by overseeing the project. I submitted the study as an amendment to a previous study in
IRB and responded to any IRB-related queries. My role included generating data collection tools
(i.e. the RedCAP surveys) and maintaining the data in a secured, password protected device. I
also oversaw any junior staff or students who assist with the project and communicated with
them to ensure data is collected and maintained in a standardized manner. I performed all
statistical analyses and took the lead on writing the manuscript. Lastly, I was involved in all of
the peer-review steps that occurred as a result of journal submission.
Project Timeline
This research project took several months to complete and will take about one year or
longer to be published in a peer-reviewed journal. The steps I took to bring this project to
completion were the following: protocol design, generation of data collection tools, institutional
review board process, collection and organization of data, analysis of data, the writing process,
and finally the submission process.
5Introduction
Previous studies have suggested that the development of migraine headaches (MH)
involves entrapment of peripheral craniofacial nerves at specific trigger sites1-5. A common
location is the frontal trigger site (site I), which is implicated in almost two-thirds of patients
undergoing MH surgery6. Studies have suggested that pain at the frontal site involves
compression of the supraorbital (SON) and supratrochlear (STN) nerves, and release of these
nerves has been shown to reduce MH pain, duration, and frequency1-5,7-10.
Both the SON and STN arise from the frontal nerve, which is a branch of the trigeminal
nerve’s ophthalmic division. Typically, both nerves emerge from the supraorbital region via their
own notch or bony foramen before branching through the glabellar muscle group11.
While the early literature on MH surgery focused on distal compression points of the
SON/STN, such as the entrance and exit of the corrugator supercilii muscle, more recent studies
have investigated the role of other more proximal compression points, such as bony SON/STN
foramina and tight fascial bands at the supraorbital rim5,10,12-14. Cadaveric studies of the general
population have confirmed foramina and fascial bands across the supraorbital notch as potential
compression points12,13. Janis et al. revealed three points of potential compression for the
supratrochlear and supraorbital nerve: entrance into the corrugator muscle, exit through the
corrugator muscle, and nerve emergence from either a notch or foramen12. Fallucco et al.
reported a supraorbital foramen prevalence of 27% among cadavers of the general population
and devised a classification system of the supraorbital notch fascial band13. The presence of a
supraorbital foramen versus a notch is clinically relevant in the development of MH pain since
performing a foraminotomy in addition to myectomy has been shown to improve outcomes as
compared to myectomy alone5.
As summarized above, the SON and STN course and compression points have been
detailed in cadaveric studies sampled from the general population. MH surgery patients are a
very select group that may differ from this sample. To our knowledge, there have been no reports
to investigate the intraoperative anatomy of patients undergoing surgery for MH at the frontal
site. The aim of this study was to describe the intraoperative anatomy of the SON and STN at the
level of the supraorbital bony rim and to identify which anatomic features are associated with
frontal trigger site pain.
6Methods
Institutional review board approval was obtained at the Massachusetts General Hospital
in Boston, Massachusetts. Patients undergoing MH surgery at the frontal trigger site between
2013 and 2018 by the senior author (W.G.A.) were prospectively enrolled following their written
informed consent. Inclusion criteria were a diagnosis of chronic MH by a board-certified
neurologist and failure of conservative management prior to presentation. Exclusion criterion
was incomplete intraoperative data. At the preoperative clinic visit, trigger sites were identified
using a combination of history, physical examination, and nerve block, as described in previous
publications8,15. Patients were asked to complete a detailed MH history and the Migraine
Headache Index (MHI) online using REDCap electronic data capture tools hosted at
Massachusetts General Hospital prior to surgery16. Preoperative pain location was determined by
pain pattern forms and physical examination (Fig. 1).
Figure 1: An example of a pain pattern form that a patient was asked to complete preoperatively
in order to describe where their pain starts (black x) and to where it radiates (red x). This pattern
is typical for isolated frontal trigger site pain.
7The senior author (W.G.A.) performed all surgical procedures using a nonendoscopic
approach, as previously described8. In all cases, the corrugator supercilii and portions of the
depressor supercilii and procerus were resected. Depending on the anatomy, tight fascial bands
were released, and/or a foraminotomy was performed using a 2mm osteotome. The senior author
evaluated frontal trigger site anatomy intraoperatively and findings were recorded using an
intraoperative anatomy form. Similar to prior studies, a notch was defined as a supraorbital bony
opening without an inferior bony border, whereas a foramen was defined as a supraorbital bony
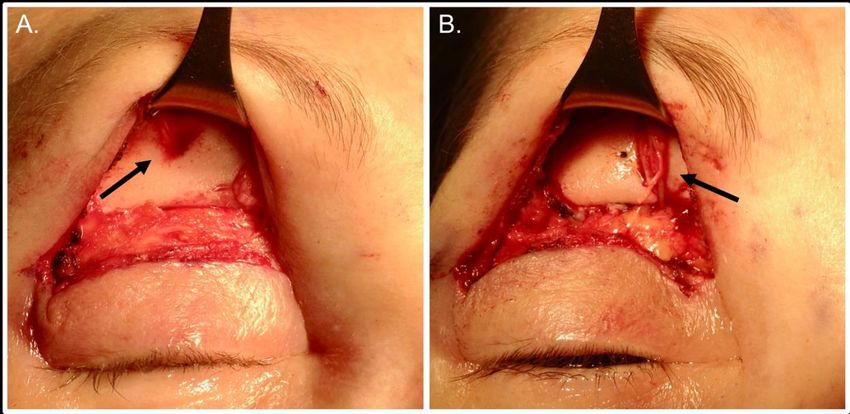
opening with a complete circumferential bony border (Fig. 2)13,14,17. The presence of nerve
compression was noted when visible macroscopic evidence of compression, including nerve
edema, flattening, or discoloration was observed.
Figure 2: A supraorbital foramen before foraminotomy (A) and after foraminotomy (B).
In order to compare the prevalence of SON notches and foramina in our MH patients to
that found in the general population, we conducted a systematic literature review in January of
2019 using the PubMed, Ovid, and Web of knowledge databases. The following keywords were
used: “supraorbital” AND (“notch” OR “notches”) AND (“cadaver” OR “cadavers” OR
“cadaveric” OR “hemiface” OR “hemifaces” OR “hemi-face” OR “hemi-faces”). Inclusion
criteria included English language articles that detailed the proportion of supraorbital notches
8and foramina in cadaveric heads. Information on author, number of cadaveric heads or hemi-
faces, and proportion of foramina and notches was collected.
Data were analyzed with STATA Version 13.0 (StataCorp, College Station, Texas).
Descriptive statistics were computed for all variables. Categorical variables were described using
frequencies and percentages. Associations between dichotomous variables, such as the presence
of pain at a supraorbital region and presence of nerve compression at that same region, were
analyzed using Chi-square and Fisher’s Exact test. Continuous parametric variables were
described using means and standard deviations (SD). Continuous nonparametric variables were
described with medians and interquartile ranges (IQR). A value of PThere were four patients for which only a single frontal site was operated on. All of these
patients presented with unilateral pain and preferred unilateral surgery despite being aware of the
risks of asymmetry. Thus, a total of 118 frontal sites (left plus right) were included for analysis.
Intraoperatively, a SON notch was found at 49% (n=58) of sites (Table 2). One site was
found to have two separate notches. In this case, the SON bifurcated into a deep and superficial
branch before exiting through two notches. A SON foramen was encountered in 41% (n=48) of
sites. Three sites (2.5%) had two foramina, and, similar to the double notch, the SON bifurcated
prior to emerging through either foramen. Eleven (9.3%) sites had a notch plus foramen. In all of
these sites, the superficial branch of the SON traversed the notch while a deep branch traversed
the foramen. One site (0.80%) had neither a notch nor a foramen. Instead, the SON traveled
inferiorly around the orbital rim without coming through a notch or foramen.
Table 2. SON Emergence Routes per site
n= 118 No, (%)
Notch 58 (49%)
One notch 57 (48%)
Double notch with SON split 1 (0.80%)
Foramen 48 (41%)
One foramen 45 (38%)
Double foramen with SON split 3 (2.5%)
Notch plus foramen 11 (9.3%)
Neither notch nor foramen 1 (0.80%)
Per individual, the most common anatomic configuration was a bilateral notch (n=18,
32%), followed by notch on one side, foramen on the other side (n=14, 25%), and bilateral
foramen (n=13, 23%). Twenty-one percent of patients (n=12) had one of six other arrangements
(Table 3). The presence of a notch on one side was associated with a contralateral notch
(PTable 3. SON Emergence Routes per patient
n= 57* No, (%)
Bilateral notch 18 (32%)
Notch and foramen 14 (25%)
Bilateral foramen 13 (23%)
Other 12 (21%)
Notch plus foramen and notch 5 (8.8%)
Notch plus foramen and notch plus foramen 2 (3.5%)
Notch plus foramen and double foramen 1 (1.8%)
Double foramen and foramen 2 (3.5%)
Double notch and notch 1 (1.8%)
Neither and foramen 1 (1.8%)
*Excludes patients who only had one frontal site operated on (n=4)
During surgery, the SON and/or STN appeared macroscopically compressed in 95% of
patients (n=58) and at 74% of sites (n=87) as indicated by nerve edema, flattening, or
discoloration (Table 4). The SON was visibly compressed at 66% of sites (n=78), whereas the
STN was compressed at 39% of sites (n=45). Etiology of compression included a tight fascial
band across the SON notch in 34% (n=40) of sites, tight SON foramen in 24% (n=28), tight
periorbital fascia compressing the SON not associated with a notch in 3.4% (n=4), tight fascial
band enclosing the STN in 30% (n=35), SON and STN emerging from one notch in 7.6% (n=9),
and SON and STN emerging from one foramen in 4.2% (n=5) (note: reasons for compression
were not mutually exclusive).
The presence of preoperative pain in a supraorbital region was not significantly
associated with the presence of a foramen (P=0.64), notch plus foramen (P=0.28), or any other
frontal anatomic configuration (P=0.99) (Table 5). There was, however, a significant correlation
between the presence of preoperative pain in a supraorbital region and presence of intraoperative
SON compression (Pcompression. The presence of macroscopic nerve compression was not associated with a history
of head or neck injury (P=0.52), type of injury (P=0.60). or years living with migraine (P=0.80).
Table 4. Macroscopic Nerve Compression
n= 118 No, (%)
Any nerve compression (SON or STN) 87 (74%)
SON compression total 78 (66%)
Causes of SON compression
Tight fascial band enclosing notch 40 (34%)
Tight foramen 28 (24%)
Tight fascial band without notch 4 (3.4%)
SON and STN within same notch 9 (7.6%)
SON and STN within same foramen 5 (4.2%)
Tight fascial band surrounding STN 35 (30%)
*Note: Reasons for compression were not mutually exclusive
Table 5. Associations between supraorbital pain and intraoperative anatomy
Proportion of supraorbital regions with
anatomical variable
Anatomical variable Pain (%) No pain, (%) P-value
SON notch 56% 68% 0.31
SON foramen 52% 41% 0.34
Any nerve compression 81% 41% < 0.001***
SON compression 74% 32% < 0.001***
STN compression 43% 24% 0.11
Tight fascial band enclosing SON notch 37% 23% 0.21
SON tight foramen 28% 4.5% 0.018*
Tight fascial band without notch 4.2% 0% 0.33
SON and STN emerging via same notch 8.4% 4.5% 0.54
SON and STN emerging via same foramen 5.3% 0% 0.58
12Our systematic literature review of cadaveric studies reporting the proportion of
supraorbital notches versus foramina yielded a total of eight studies 12,13,18-23. A total of 521
supraorbital regions among the eight studies were analyzed (Table 6). Foramina were found at
22% of supraorbital regions, including sites with an isolated foramen (18%), sites with a notch
plus a foramen (2.3%), and sites with double foramina (1.5%).
Table 6: Systemic Literature Review of Foramina Prevalence Among Cadaveric Samples
SON SON
Number of SON SON Double Notch Plus
Author Supraorbits Notches Foramina Foramina Foramin
Andersen et al. 2001 20 6 6 6 2
Aziz et al. 2000 94 70 24 - -
Cutright et al. 2003 160 148 12 - -
Falluco et al. 2012 60 44 10 0 6
Fatah et al. 1991 20 19 1 - -
Janis et al. 2013 27 16 11 - -
Malet et al. 1997 40 26 8 2 4
Saylam et al. 2003 100 77 23 - -
Total (%) 521 406 (78) 95 (18) 8 (1.5) 12 (2.3)
Lastly, we investigated for any associations between anatomy and migraine severity
using the MHI. Preoperatively, there were no significant differences in mean MHI between
patients with SON foramina on either side (125±90) versus those without foramina on either side
(100±58) (P=0.33). At one year postoperatively, there was an 82% response rate (n=50) to
follow-up surveys. Analyses suggested no difference in mean postoperative MHI between
patients with SON foramina (39±65) versus those without (32±63) (P=0.71). Between patients
with foramina versus those without, there was also no significant difference in the number of
patients achieving a 50% reduction (84% versus 74%, P=0.38) or 80% reduction (74% versus
63%, P=0.41), respectively.
13Discussion
Anatomic studies at the frontal trigger site have been conducted in cadavers resembling
the general population11-13,24. This study explored the intraoperative anatomy observed in MH
surgery patients undergoing frontal release surgery. We demonstrated 1) that the intraoperative
anatomy and etiology of nerve compression at the frontal trigger site varies greatly among
patients undergoing MH surgery and 2) there is a higher rate of SON foramina as compared to
previous cadaveric studies of the general population. Further, some anatomic features in patients
undergoing MH surgery and the general population were identical. This prompts the question of
which features are causal for pain. We found that the presence of pain at a specific supraorbital
side was not associated with a specific anatomic feature (notch or foramen), but was associated
with macroscopically-visible nerve compression on that same side. This suggests that locations
with pain will often have evidence of nerve compression, although this is not uniformly the case.
The hypothesis that a supraorbital foramen increases the risk of nerve compression
compared to a supraorbital notch has been suggested previously by the literature5,14. In the
current study, we found a higher prevalence of SON foramina (50.3%, including supraorbital
regions with a foramen plus notch and regions with double foramina) as compared to prior
cadaveric studies (22%)13,18-20. A recent CT study in patients undergoing surgery at the frontal
site revealed a 30% prevalence of foramina14. However, this proportion was not compared with
intraoperative data.
While the presence of a supraorbital foramen did not predict MH pain, a tight foramen
resulting in macroscopic nerve compression did correlate with pain at a given site. This finding
suggests that a foramen is not enough to trigger MH pain but that it must also be sufficiently
narrow to entrap the nerve. This notion is accordant with the fact that 22% of the general
population have supraorbital foramina but do not have MH pain. Despite this finding, we would
currently recommend foraminotomy for MH surgery patients with supraorbital foramina. For
one, it is unclear if patients with foramina that show no current macroscopically visible nerve
compression will develop symptoms in the future. Further, current technology does not allow
intraoperative evaluation of nerves to screen for microscopic injuries. This argument is further
supported by CT imaging findings of Pourtaheri et al. who found that MH patients undergoing
surgery have foramina that are 34-42% smaller as compared to the general population. In
addition, previous studies have shown that patients with supraorbital foramina exhibit higher
14baseline MHI scores and that performing foraminotomy improves outcomes in comparison with
myectomy alone5,14.
While our findings revealed that a tight supraorbital foramen resulting in macroscopic
nerve compression is associated with MH pain, it is important to consider that our study did not
investigate all anatomic features that may be relevant, such as the nerve branching patterns
through muscle, muscular hypertrophy, or muscular hyperactivity. Interestingly, a recent study
using CT imaging analyzed the size of the corrugator muscle in patients with frontal MH pain
and found that MH patients do not exhibit muscular hypertrophy as compared to the general
population25. The authors concluded that pain is thus more likely from corrugator hyperactivity
rather than hypertrophy 26-30. It is important to consider all anatomic elements when treating MH
surgery candidates at the frontal site.
As with most research inquiries, it is likely that the answers to our questions are even
more complex than initially apparent. Among patients with MH pain, it is likely that there are
multiple points of nerve compression. The “double crush” hypothesis has been well described in
the context of other entrapment neuropathies31,32. Simply stated, it posits that if a nerve is
compressed at one location, the disturbance in axoplasmic flow will render the nerve more
vulnerable to subsequent compression at other locations. When multiple compression points
exist, their effects can be summative and cause clinical dysfunction whereas a single point of
compression would not have. Patients in our study could very well have multiple points of
compression that we are not able to identify by mere observation. While we did not find
significant associations with pain and tight fascial bands, it is possible that our sample size
lacked the power to elucidate this relationship. As we move closer to understanding the complex
pathways of MH pain development, it will also become critical to investigate beyond
macroscopic anatomy and into molecular pathophysiology and microscopic pathology33.
We caution readers of this study to interpret the reported results with an understanding of
its limitations. First, the presence of nerve compression is not objectively quantifiable during
surgery and is based on the experience and observation of a single surgeon who was not blinded
to the pain patterns of the subjects. While there is an inherent risk of observer bias in any non-
blinded study, the current authors emphasize that the existence of nerve compression was only
noted when there was macroscopic evidence of nerve compression such as nerve discoloration,
flattening, or edema.
15This study reveals that the supraorbital rim anatomy of the frontal trigger site varies
greatly among patients undergoing MH surgery. We also report the most common suspected
causes of SON and STN compression in MH surgery patients, which often include a tight band
and tight foramen, the latter of which is significantly associated with MH pain. It is of great
importance for surgeons performing MH surgery to be aware of the anatomic variability they
will encounter and to ensure complete decompression of frontal nerves during surgery.
16References
1. Guyuron B, Varghai A, Michelow BJ, et al. Corrugator supercilii muscle resection and
migraine headaches. Plast Reconstr Surg. 2000;106(2):429-434; discussion 435-427.
2. Guyuron B, Tucker T, Davis J. Surgical treatment of migraine headaches. Plast Reconstr
Surg. 2002;109(7):2183-2189.
3. Guyuron B, Reed D, Kriegler JS, et al. A placebo-controlled surgical trial of the
treatment of migraine headaches. Plast Reconstr Surg. 2009;124(2):461-468.
4. Janis JE, Dhanik A, Howard JH. Validation of the peripheral trigger point theory of
migraine headaches: single-surgeon experience using botulinum toxin and surgical
decompression. Plast Reconstr Surg. 2011;128(1):123-131.
5. Chepla KJ, Oh E, Guyuron B. Clinical outcomes following supraorbital foraminotomy
for treatment of frontal migraine headache. Plast Reconstr Surg. 2012;129(4):656e-662e.
6. Seyed Forootan NS, Lee M, Guyuron B. Migraine headache trigger site prevalence
analysis of 2590 sites in 1010 patients. J Plast Reconstr Aesthet Surg. 2017;70(2):152-
158.
7. Kurlander DE, Ascha M, Sattar A, et al. In-Depth Review of Symptoms, Triggers, and
Surgical Deactivation of Frontal Migraine Headaches (Site I). Plast Reconstr Surg.
2016;138(3):681-688.
8. Gfrerer L, Maman DY, Tessler O, et al. Nonendoscopic deactivation of nerve triggers in
migraine headache patients: surgical technique and outcomes. Plast Reconstr Surg.
2014;134(4):771-778.
9. Janis JE, Barker JC, Javadi C, et al. A review of current evidence in the surgical
treatment of migraine headaches. Plast Reconstr Surg. 2014;134(4 Suppl 2):131S-141S.
10. Hagan RR, Fallucco MA, Janis JE. Supraorbital Rim Syndrome: Definition, Surgical
Treatment, and Outcomes for Frontal Headache. Plast Reconstr Surg Glob Open.
2016;4(7):e795.
11. Janis JE, Ghavami A, Lemmon JA, et al. The anatomy of the corrugator supercilii
muscle: part II. Supraorbital nerve branching patterns. Plast Reconstr Surg.
2008;121(1):233-240.
1712. Janis JE, Hatef DA, Hagan R, et al. Anatomy of the supratrochlear nerve: implications for
the surgical treatment of migraine headaches. Plast Reconstr Surg. 2013;131(4):743-750.
13. Fallucco M, Janis JE, Hagan RR. The anatomical morphology of the supraorbital notch:
clinical relevance to the surgical treatment of migraine headaches. Plast Reconstr Surg.
2012;130(6):1227-1233.
14. Pourtaheri N, Guyuron B. Computerized tomographic evaluation of supraorbital notches
and foramen in patients with frontal migraine headaches and correlation with clinical
symptoms. J Plast Reconstr Aesthet Surg. 2018;71(6):840-846.
15. Guyuron B, Nahabet E, Khansa I, et al. The Current Means for Detection of Migraine
Headache Trigger Sites. Plast Reconstr Surg. 2015;136(4):860-867.
16. Harris PA, Taylor R, Thielke R, et al. Research electronic data capture (REDCap)--a
metadata-driven methodology and workflow process for providing translational research
informatics support. J Biomed Inform. 2009;42(2):377-381.
17. Beer GM, Putz R, Mager K, et al. Variations of the frontal exit of the supraorbital nerve:
an anatomic study. Plast Reconstr Surg. 1998;102(2):334-341.
18. Malet T, Braun M, Fyad JP, et al. Anatomic study of the distal supraorbital nerve. Surg
Radiol Anat. 1997;19(6):377-384.
19. Saylam C, Ozer MA, Ozek C, et al. Anatomical variations of the frontal and supraorbital
transcranial passages. J Craniofac Surg. 2003;14(1):10-12.
20. Aziz SR, Marchena JM, Puran A. Anatomic characteristics of the infraorbital foramen: a
cadaver study. J Oral Maxillofac Surg. 2000;58(9):992-996.
21. Andersen NB, Bovim G, Sjaastad O. The frontotemporal peripheral nerves. Topographic
variations of the supraorbital, supratrochlear and auriculotemporal nerves and their
possible clinical significance. Surg Radiol Anat. 2001;23(2):97-104.
22. Fatah MF. Innervation and functional reconstruction of the forehead. Br J Plast Surg.
1991;44(5):351-358.
23. Cutright B, Quillopa N, Schubert W. An anthropometric analysis of the key foramina for
maxillofacial surgery. J Oral Maxillofac Surg. 2003;61(3):354-357.
24. Janis JE, Ghavami A, Lemmon JA, et al. Anatomy of the corrugator supercilii muscle:
part I. Corrugator topography. Plast Reconstr Surg. 2007;120(6):1647-1653.
1825. Hsu JJ, Stasiak AM, Ranganathan K, et al. Morphometric Evaluation of the Frontal
Migraine Trigger Site. Plast Reconstr Surg. 2018;141(5):726e-732e.
26. Aurora SK, Dodick DW, Turkel CC, et al. OnabotulinumtoxinA for treatment of chronic
migraine: results from the double-blind, randomized, placebo-controlled phase of the
PREEMPT 1 trial. Cephalalgia. 2010;30(7):793-803.
27. Diener HC, Dodick DW, Aurora SK, et al. OnabotulinumtoxinA for treatment of chronic
migraine: results from the double-blind, randomized, placebo-controlled phase of the
PREEMPT 2 trial. Cephalalgia. 2010;30(7):804-814.
28. Liu MT, Armijo BS, Guyuron B. A comparison of outcome of surgical treatment of
migraine headaches using a constellation of symptoms versus botulinum toxin type A to
identify the trigger sites. Plast Reconstr Surg. 2012;129(2):413-419.
29. Nahabet E, Janis JE, Guyuron B. Neurotoxins: Expanding Uses of Neuromodulators in
Medicine--Headache. Plast Reconstr Surg. 2015;136(5 Suppl):104S-110S.
30. Janis JE, Barker JC, Palettas M. Targeted Peripheral Nerve-directed Onabotulinumtoxin
A Injection for Effective Long-term Therapy for Migraine Headache. Plast Reconstr Surg
Glob Open. 2017;5(3):e1270.
31. Upton AR, McComas AJ. The double crush in nerve entrapment syndromes. Lancet.
1973;2(7825):359-362.
32. Mackinnon SE. Double and multiple "crush" syndromes. Double and multiple entrapment
neuropathies. Hand Clin. 1992;8(2):369-390.
33. Guyuron B, Yohannes E, Miller R, et al. Electron microscopic and proteomic comparison
of terminal branches of the trigeminal nerve in patients with and without migraine
headaches. Plast Reconstr Surg. 2014;134(5):796e-805e.
19You can also read

















































