Effect of Preoperative Intravenous Methocarbamol and Intravenous Acetaminophen on Opioid Use After Primary Total Hip and Knee Replacement
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
■ Feature Article
Effect of Preoperative Intravenous
Methocarbamol and Intravenous
Acetaminophen on Opioid Use After
Primary Total Hip and Knee Replacement
THOMAS D. LOOKE, MD, PHD; CAMERON T. KLUTH, MBA
gical site injections, designed by physi-
abstract cians at the Florida Hospital Winter Park
campus have evolved over the past sever-
Between 2010 and 2011, a perioperative pain protocol for primary total hip and al years. No standardized protocol exist-
knee replacement at one Florida medical center replaced preoperative oral an- ed prior to 2006. In 2006, the anesthesia
algesics with intravenous methocarbamol and intravenous acetaminophen. This department offered regional anesthesia
is a retrospective cohort study of 300 patients, with 150 patients using the new to all total knee patients. By mid-2008,
pain protocol and 150 patients using a 2008 pain protocol that did not include anesthesiologists at Florida Hospital
these medications. The 2 cohorts were similar in patient gender, age, and body Winter Park offered every total knee pa-
mass index. Opioid consumption was evaluated for a period of 48 hours after tient a femoral nerve sheath catheter with
incision and was divided into 3 separate time intervals, as well as total 48-hour
consumption. Mean opiate use decreased significantly from 2008 to 2011 in
all time intervals and total consumption (7.5⫾3.4 mg to 6.1⫾3.0 mg; P⬍.01). The authors are from the Florida Hospital De-
partment of Anesthesiology and Florida Hospital,
Subgroup analysis suggested that changes to the hip protocol were responsible Winter Park Division, Office of Orthopedic Research
for decreased opioid use in the operating room and the postanesthesia care unit, (TDL); and from the University of Central Florida
and changes to the knee protocol were responsible for decreased opioid use on College of Medicine (CTK), Orlando, Florida.
the hospital floor and total consumption. The difference between the 2 protocol Dr Looke received investigator-initiated study
grant support paid to his institution from Cadence
groups was not due to differences in individual surgeon practice patterns. Physical Pharmaceuticals, Inc., and was compensated by
therapy progress of knee flexion, average walking distance, and maximum walk- SLACK Incorporated for his contribution to this
ing distance were significantly improved. Hospital discharge was shorter in the manuscript. Mr Kluth received travel reimburse-
2011 group (4.0⫾1.1 days in 2008 group and 3.6⫾1.0 days in 2011 group). This ment from the University of Central Florida College
of Medicine.
study shows significant improvement in patient care from 2008 to 2011 that is at The authors thank Gwen Certain and Cecille
least partially due to the change to the use of preoperative intravenous methocar- Brocato for sharing their extensive knowledge and
bamol and intravenous acetaminophen. experience as certified pain nurses and for providing
their invaluable assistance with data collection; and
Dr Julie W. Pepe with Florida Hospital Office of Re-
search Administration for her biostatistics expertise.
I
n the United States, more than perform more than 2100 primary total hip The authors also thank the leadership team at Flor-
600,000 total knee replacements and and knee replacements each year at the ida Hospital Winter Park for providing equipment,
285,000 total hip replacements are 7 campuses in the greater Orlando area. office space, and logistical support for this project.
Correspondence should be addressed to: Thom-
performed each year.1,2 At Florida Hos- Perioperative pain management proto- as D. Looke, MD, PhD, 4609 Jetty St, Orlando, FL
pital, a 4415 bed hospital system with cols, which include oral and parenteral 32817 (tdlooke@hotmail.com).
22 campuses in central Florida, surgeons analgesics, regional anesthetics, and sur- doi: 10.3928/01477447-20130122-54
FEBRUARY 2013 | Volume 36 • Number 2/SUPPLEMENT 25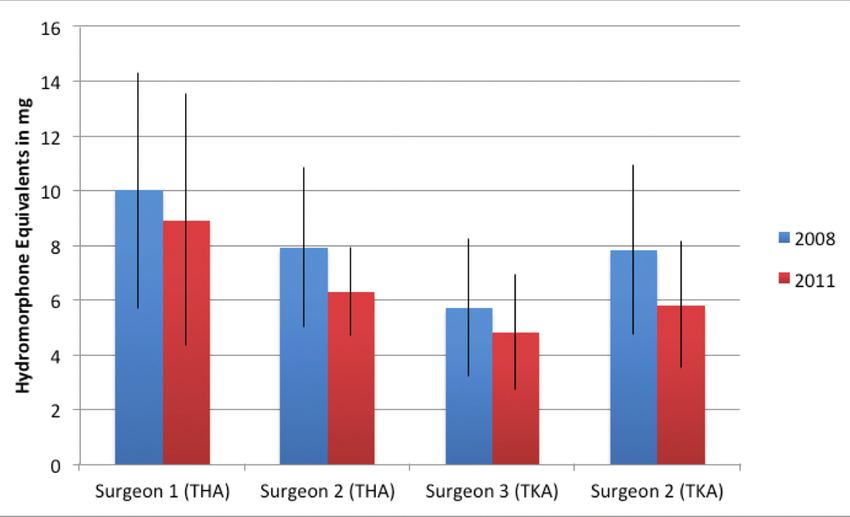
■ Feature Article
48 hours of continuous regional anesthe- opioid rescue, VAS pain scores, physical and 50 using the 2008 control protocol
sia for postoperative pain management. therapy progress, and hospital discharge each) and 2 surgeons performing hips
By 2010, the use of postoperative opioids times. This was considered a pilot study (25 using the 2011 study protocol and 25
after total knee surgery decreased signifi- to determine if a prospective, random- using the 2008 control protocol each). In
cantly, and patient-controlled analgesia ized, controlled clinical trial would likely total, the study included patients from 3
delivery of intravenous hydromorphone show any benefit from expanding the use surgeons, because the second most pro-
was replaced with nursing administration of these 2 intravenous medications from lific knee surgeon was also the second
of oral oxycodone plus acetaminophen 1 preoperative dose to regular dosing for most prolific hip surgeon. More empha-
or intravenous hydromorphone at patient the first 48 hours. sis was placed on limiting the number of
request only. In addition, preoperative surgeons rather than anesthesiologists,
treatment with oral analgesics (a sur- MATERIALS AND METHODS because the number of patient-care items
geon-ordered combination of 1 or more The Institutional Review Boards of left to the discretion of the surgeon is
of celecoxib, oxycodone plus acetamino- Florida Hospital and the University of greater than those left to the discretion
phen, or pregabalin) was replaced with Central Florida approved this retrospec- of the anesthesiologist. In addition, the
intravenous methocarbamol (Robaxin In- tive 2 cohort study with HIPAA and in- team wanted to determine whether those
jection; Baxter Healthcare Corporation, formed consent waivers for 300 patients. items left to surgical discretion, such as
Deerfield, Illinois). The goals with this One hundred fifty patients were included intraoperative surgical site injections and
medication were to reduce oral loading in the study group (using the 2011 proto- perioperative analgesic adjunct selection,
preoperatively and reduce recovery room col with preoperative intravenous metho- influenced primary outcome differences.
discharge delays due to muscle spasm carbamol and intravenous acetamino- Patients were evaluated from 2011
pain. At that time, no reports existed on phen), and 150 patients in the control (study) and 2008 (control) protocol
the effectiveness of intravenous metho- group (using the 2008 protocol without groups in the order described above and
carbamol postoperatively for total joint these 2 medications). The patient popula- included those patients, between the ages
surgery. Two studies of its use after breast tion was identified from anesthesia bill- of 18 and 85, who had an American Soci-
augmentation had been performed,3-5 but ing records, including all patients from ety of Anesthesiologists (ASA) physical
this medication was ignored by most of Florida Hospital Winter Park who had status of 1 to 3. Patients were excluded
the anesthesia pain literature.6 primary unilateral total knee arthroplasty if they had chronic pain with patient
In 2011, intravenous acetaminophen (CPT 27447) or primary total hip arthro- reported opioid use 1 month preopera-
(OFIRMEV; Cadence Pharmaceuticals, plasty (CPT 27130) between January 1, tively; had taken centrally acting muscle
Inc., San Diego, California) was added to 2009, and October 12, 2011. Patients relaxants 24-hours preoperatively; re-
the protocol. Physicians and nursing staff were grouped according to the periopera- ceived a regional anesthesia procedure
had anecdotally reported that the combi- tive pain protocol and excluded patients for postoperative pain control (other than
nation of intravenous methocarbamol and from the 2010 protocol who received in- a femoral nerve sheath catheter for knees
intravenous acetaminophen improved the travenous methocarbamol but not intra- or fascia iliaca block for hips); did not
early postoperative recovery after total venous acetaminophen. receive both of the study medications;
hip and knee replacement. Although in- Within each protocol group, patients and if there was a notable surgical com-
travenous acetaminophen had been stud- were also grouped first by surgeon (from plication as defined by the surgeon’s op-
ied for use in major orthopedic surgery,7,8 greatest to least surgical volume), next erative report. Data was collected for 300
it had not been studied when added to a by anesthesiologist (from greatest to patients. During the data analysis phase,
perioperative pain protocol that included least volume), and finally by date of 1 total hip patient in the 2008 protocol
long acting peripheral regional anesthet- surgery (in reverse chronologic order). group, whose opioid consumption ex-
ics and other intravenous adjuncts. Since the total knee arthroplasty volume ceeded 5 standard deviations above the
Our retrospective study compares a co- at Florida Hospital Winter Park (700 in mean, was also excluded from analysis,
hort of patients from 2011, who received 2011) is approximately twice that of total based on a history of chronic pain that
preoperative intravenous methocarbamol hip arthroplasty volume (375 in 2011), had been missed in the initial assessment.
and intravenous acetaminophen, with a the team decided, a priori, to include Thus, 299 patients with a primary total
cohort of patients using the 2008 pain 100 knees and 50 hip patients from each knee or total hip replacement were in-
protocol, who did not receive these med- protocol group. This made it possible to cluded in the study.
ications. The outcome measures studied limit the study to 2 surgeons performing For the study time periods, the sur-
were opioid consumption, time to first knees (50 using the 2011 study protocol gical incision was defined as time zero.
26 ORTHOPEDICS | Healio.com/Orthopedics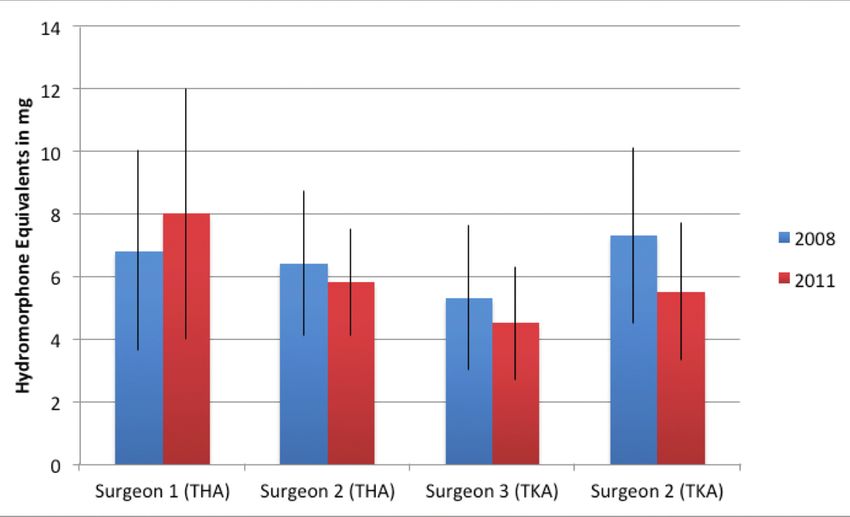
EFFECT OF METHOCARBAMOL AND ACETAMINOPHEN ON OPIOID USE AFTER THA AND TKA | LOOKE & KLUTH
time (in minutes from incision to first
Table 1 request for opioid medication); physical
Opiate Equivalency Table Used to Convert Opiates Encountered therapy progress (range of motion after
During the Study to Hydromorphone Equivalents total knee in degrees of flexion and ex-
tension, and ambulation in feet after both
Opiate Generic Name Route Equivalent Dose total hip and total knee) recorded by a
Fentanyl Intravenous 100 mcg physical therapist once or twice daily;
Hydrocodone Oral 30 mg PACU discharge time (in minutes from
Hydromorphone Intravenous 1.5 mg time of arrival to the time that PACU
Hydromorphone Oral 7.5 mg discharge criteria was met); and hospital
discharge time (in days from time of inci-
Meperidine Intravenous 75 mg
sion to time officially recorded as end of
Morphine Intravenous 10 mg
hospital admission).
Morphine Oral 30 mg
Statistical analysis used a chi-square
Oxycodone Oral 20 mg test for each categorical variable (gender
Propoxyphene Oral 150 mg and ASA class) and considered noncat-
egorical variables to be continuous. The
team then evaluated noncategorical vari-
ables using either parametric or nonpara-
Table 2
metric tests depending on whether the
Demographics of Study Patients data were found to be normally or non-
normally distributed. Parametric tests
Sex, No.(%) ASA Class No. (%)
Age, y, BMI, included an independent 2-sample t test
Group Female Male Mean (SD) Mean (SD) 1 2 3 for the primary group (protocol) compar-
All 174 (58) 125 (42) 65.5 (9.8) 30.8(5.9) 23 (8) 190 86 isons and analysis of variance (ANOVA)
(63) (29)
for the multiple subgroup comparisons.
2008 84 (56) 65 (44) 66.1 (9.4) 30.8(5.4) 5 (3) 95 49 The team used Levene’s test of equality
(64) (33)
of error variances for the ANOVA com-
2011 90 (60) 60 (40) 64.9 (10.3) 30.9(6.3) 18 95 37
(12) (63) (25) parisons to determine if the subgroup
P value .559 .276 .959 .011a
populations had comparable statistics.
A significant Levene’s test result means
Abbreviations: ASA class, American Society of Anesthesiology physical status; BMI, body mass
index. that subgroup populations have different
a
Meets criteria for significance at P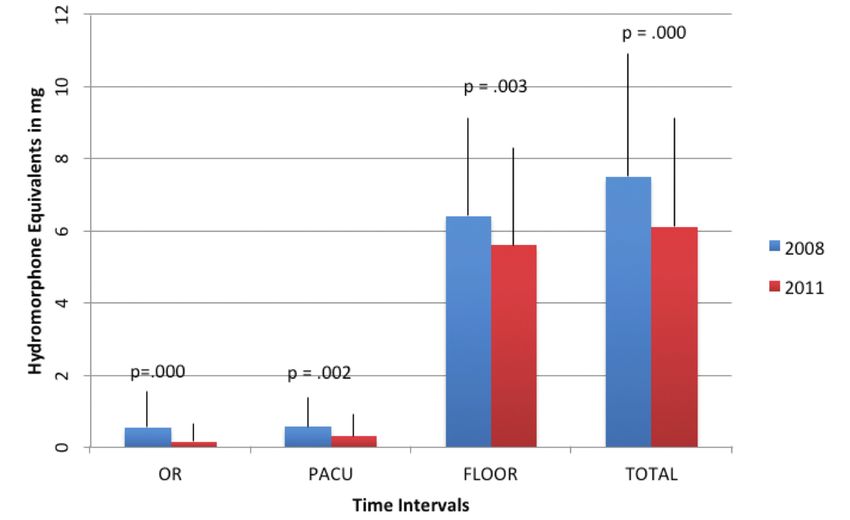
■ Feature Article
Table 3
Opiate Use by Time Period for Protocol and Subgroupa
Group ORb PACUc FLOORd TOTALe
Protocol group
2008 .53 (.99) mg .56 (.80) mg 6.4 (2.7) mg 7.5 (3.4) mg
2011 .16 (.49) mg .30 (.60) mg 5.6 (2.7) mg 6.1 (3.0) mg
NP P valuef .000 .002 .003 .000
Total Hip Arthroplasty Only
2008 1.24 (1.20) mg 1.10 (.92) mg 6.6 (2.7) mg 8.9 (3.8) mg
2011 .19 (.54) mg .54 (.79) mg 6.9 (3.3) mg 7.6 (3.6) mg
f
NP P value .000 .001 .978 .074
Total Knee Arthroplasty Only
2008 .18 (.65) mg .29 (.58) mg 6.3 (2.7) mg 6.8 (3.0) mg
2011 .15 (46) mg .17 (.43) mg 5.0 (2.0) mg 5.3 (2.2) mg
f
NP P value .572 .179 .000 .000
Subgroup Analysis by Surgery Type, Surgeon, and Protocol Group
THA, surgeon 1
2008 6.8 (3.2) mg 10.0 (4.3) mg
2011 8.0 (4.0) mg 8.9 (4.6) mg
THA, surgeon 2
2008 6.4 (2.3) mg 7.9 (2.9) mg
2011 5.8 (1.7) mg 6.3 (1.6) mg
ANOVA P valuesg
Surgeon vs surgeon .024 .002
2008 protocol vs 2011 protocol .604 .067
Surgeon influence on protocol .143h .717h
TKA, surgeon 3
2008 5.3 (2.3) mg 5.7 (2.5) mg
2011 4.5 (1.8) mg 4.8 (2.1) mg
TKA, surgeon 2
2008 7.3 (2.8) mg 7.8 (3.1) mg
2011 5.5 (2.2) mg 5.8 (2.3) mg
ANOVA P valuesg
Surgeon vs surgeon .000 .000
2008 protocol vs 2011 protocol .000 .000
Surgeon influence on protocol .146h .134h
Abbreviations: ANOVA, analysis of variance; NP, nonparametric; OR, operating room; PACU, postanesthesia care unit; THA, total hip arthroplasty;
TKA, total knee arthroplasty.
a
Analysis given as mean (standard deviation) in hydromorphone equivalent mg.
b
OR time period is defined as incision time to PACU admission time.
c
PACU time period is defined as PACU admission time to PACU discharge time.
d
FLOOR time period is defined as PACU discharge to 48 hours after incision.
e
TOTAL time period is defined as incision time to 48 hours after incision time.
f
NP P value refers to nonparametric test of significance (Mann-Whitney U test) with .05 considered significant, subgroup analysis by surgeon only
completed for FLOOR and TOTAL time periods.
g
ANOVA P values for surgeon subgroup analysis show that for THA there was a statistically significant difference between the 2 surgeons but not the 2
protocol groups and that differences between the surgeons did not significantly influence analysis of the protocol groups; for TKA, statistically significant
differences were found between the surgeons and the protocol groups but the surgeon differences did not significantly impact the protocol groups.
h
Levene’s test of equality of error variances was positive when comparing hip surgeons. Therefore, comparing the hip surgeon populations by ANOVA
may not be valid due to significant differences in the population characteristics in the 2 protocol groups.
28 ORTHOPEDICS | Healio.com/OrthopedicsEFFECT OF METHOCARBAMOL AND ACETAMINOPHEN ON OPIOID USE AFTER THA AND TKA | LOOKE & KLUTH
Opiate Use in OR by Protocol Group
2008 Protocol (Blue) 2011 Protocol (Green)
2
Figure 2: Opiate usage by time interval and protocol group. OR is the time period in
1 the operating room from time of incision to time of PACU admission; PACU is time
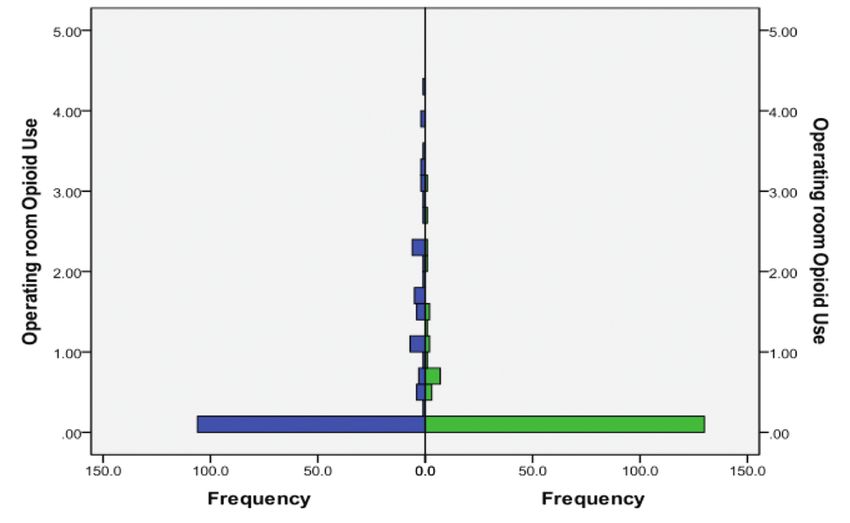
Figure 1: Demonstration of skewed opiate data. The vast majority of patients in postanesthesia care unit from time of admission to time of discharge from PACU;
receive no opiate medication in the operating room. The y-axis is opioid use in FLOOR is the time period from PACU discharge to 48 hours after incision; and TO-
hydromorphone equivalent mg. The x-axis, labeled Frequency, shows number TAL is the combined period from incision time to 48 hours after incision. The height
of patients receiving the amount of hydromorphone in the interval shown with of the bars represents mean with error line (standard deviation) rising above mean
the bottom interval (highest frequency) being the number of patients receiving demonstrating that data is not normally distributed (skewed left). Mann-Whitney U
hydromorphone 0 to 0.2 mg. test P values shown above each time interval.
3 4
Figure 3: FLOOR opiate use by surgeon. Comparison of 2008 and 2011 protocol Figure 4: Comparison of 2008 and 2011 protocol groups total opiate use broken
groups opiate use on the FLOOR (after discharge from PACU) broken down by down by surgeon. The height of the bars (error lines) represent mean (standard
surgeon. The height of the bars (error lines) represent mean (standard deviation) deviation) opiate use in hydromorphone equivalent mg. Table 4 gives ANOVA P
opiate use in hydromorphone equivalent mg. Table 4 gives ANOVA P values. For values. For THA, Surgeon 1 and 2 populations have different opiate needs but the
THA, Surgeon 1 and 2 populations have different opiate needs but the combined combined protocol groups are similar and the differences between the surgeons
protocol groups are similar and the differences between the surgeons did not did not significantly affect protocol group changes. For TKA, Surgeon 3 and 2 popu-
significantly affect protocol group changes. For TKA, Surgeon 3 and 2 popula- lations have different opiate needs, combined 2008 and 2011 protocol groups have
tions have different opiate needs, combined 2008 and 2011 protocol groups have different needs, but the difference between the surgeons did not impact the differ-
different needs, but the difference between the surgeons did not impact the dif- ence between the protocol groups.
ference between the protocol groups.
Continued from page 27 time periods. Even with patients in both proved adequate for all time periods for
FLOOR intervals (as described above) protocol groups requiring minimal opi- both hip and knee surgeries and showed
into 1, a necessary adjustment due to spo- oids in the OR and PACU (Figure 1, for the same skew to the left as the full pro-
radic FLOOR data. The TOTAL period the OR), nonparametric analysis showed tocol groups, necessitating a nonparamet-
combined all data for the 48-hour period significant reduction of opioid use in the ric approach for this analysis as well. The
starting with incision time. 2011 protocol group in all time periods 2011 protocol group demonstrated signifi-
Our patient population demonstrated a (Figure 2). cantly reduced opioid use in the OR and
non-normally distributed opioid use that The results were also analyzed focus- PACU time periods after hip surgery but
was heavily skewed to the left with the ing on surgery type (hip or knee) and not knee surgery. There was significantly
median much greater than the mean in all surgeon (Table 3). For surgery type, data reduced opioid use on the FLOOR and
FEBRUARY 2013 | Volume 36 • Number 2/SUPPLEMENT 29■ Feature Article
TOTAL in the knee surgery group but not
the hip surgery group. Examining the in- Table 4
dividual surgeons (identified only as sur- Secondary Outcome Variablesa
geons 1, 2, and 3), FLOOR and TOTAL
opiate use were normally distributed data 2008 Protocol 2011 Protocol
Group Group P
and ANOVA was used to determine if
changes in opioid use (FLOOR and TO-
Pain; all periods b
4.9 (1.0) VAS 5.5 (1.2) VASEFFECT OF METHOCARBAMOL AND ACETAMINOPHEN ON OPIOID USE AFTER THA AND TKA | LOOKE & KLUTH
surgery, which may provide 12 hours of
Table 5 postoperative pain relief. We are not able
Changes in Intraoperative Anesthesia Preference for Total Hip Surgery to determine if the increased use of spi-
nal morphine or fascia iliaca blocks to
2008 2011 the 2011 THA protocol contributed to the
a b
No. GA Spinal Both No. GA Spinala Bothb findings. It is possible that a statistically
Surgeon 24 24 0 0 25 13 17 5 significant increase in FLOOR opioid
1, No(%) (100) (52) (68) (20) use was averted by these techniques.
Surgeon 25 15 16 6 25 5 23 3 Other changes in the use of patient-
2, No(%) (60) (64) (24) (20) (92) (12)
controlled analgesia, preoperative oral
Total, 49 39 16 6 50 18 40 8 analgesics, and surgical site injections
No(%) (80) (33) (12) (36) (80) (16)
may have influenced the results. Ten
Abbreviation: GA, general anesthesia. months after initiating the 2008 protocol,
a
Single injection of spinal anesthesia.
b
Patient received both spinal and GA. Reason for receiving both was unspecified but could be failed or most total knee patients who received spi-
slow onset spinal or other patient factors, such as patient preference, morbid obesity, or sleep apnea). nal anesthesia and a femoral nerve cath-
eter controlled their postoperative pain
with only PRN oral opioids. The patient-
Table 6 controlled analgesia for total knee sur-
Use of Patient-controlled Analgesia Postoperatively gery postoperatively was phased out over
the next year. In the 2008 protocol group,
by Surgery Type, Surgeon, and Protocol Group
33% of patients (who had their surgery in
2008 2011 2009 and early 2010) received a patient-
Procedure PCAa No PCA PCA No PCA controlled analgesia, and with the 2011
protocol, no patients (except chronic pain
THA
patients) received a patient-controlled
Surgeon 1 (n=49) 14 10 12 13
analgesia. This was also phased out for
Surgeon 2 (n=50) 25 0 0 25
total hip patients, with 80% receiving
Total, No.(%) 39 (80%) 10 (20%) 12 (24%) 38 (76%) patient-controlled analgesias in the 2008
TKA protocol group and only 24% receiving
Surgeon 3 (n=100) 12 38 0 50 patient-controlled analgesias in the 2011
Surgeon 2 (n=100) 21 29 0 50 protocol group (Table 6). There was a
Total, No.(%) 33 (33%) 67 (67%) 0 100 significant reduction in late opiate use
All (n=299), No.(%) 72 (48%) 77 (52%) 12 (8%) 138 (92%) (FLOOR and TOTAL) and a concomitant
increase in average pain scores (Table 4).
Abbreviations: N, number of patients; PCA, patient-controlled analgesia; THA, total hip arthroplasty;
TKA, total knee arthroplasty. This may be related to eliminating the
a
Numbers given in PCA columns represent the number of patients with documented initiation of a PCA patient-controlled analgesia. The pres-
in nursing records; totals given as number (%). ence of a patient-controlled analgesia is
an independent (second only to pain it-
self) driver of opioid consumption and
desired result is less time in the PACU but not statistically less (P=.074). In the its elimination will decrease opioid use
adjusting for inadequate or excessive 2008 total hip protocol, 33% of patients without significantly changing patient
opiate loading in the OR and less opiate (all from surgeon 2) also received spinal satisfaction. Thus, we were surprised to
use overall. The increased use of spinal morphine, but this increased to 80% of see a 12% increase in pain scores and are
anesthesia from 2008 to 2011 certainly patients in the 2011 hip protocol (from uncertain if the increase in average pain
contributed to the significant reduction in both surgeons). The expected benefit is 6 scores from 4.9 to 5.5 is accompanied
OR and PACU opioid use in the total hip to 12 hours of postoperative pain relief. with reduced patient satisfaction.
subgroup (Table 3) and probably to the None of the knee patients received spi- In the 2008 protocol, both knee sur-
slight (insignificant) increase in opioid nal morphine. Ultrasound-guided fascia geons (surgeon 2 and surgeon 3), routinely
use on the floor. Overall, the TOTAL opi- iliaca blocks were also added to all pa- ordered preoperative and postoperative
ate use after hip surgery was numerically, tients in the 2011 protocol for total hip oral analgesics, including celecoxib and a
FEBRUARY 2013 | Volume 36 • Number 2/SUPPLEMENT 31■ Feature Article
combination oxycodone-acetaminophen The study found no difference in PACU REFERENCES
tablet. In the 2011 protocol, both surgeons discharge times but a significant decrease 1. Total knee replacement. American Academy
eliminated these medications and added in hospital length of stay. This may be re- of Orthopaedic Surgeons Web site. http://
orthoinfo.aaos.org/topic.cfm?topic=a00389.
oral methocarbamol (500 mg 3 times daily) lated to the difference in ASA grades in the Updated December 2011. Accessed October
to the postoperative routine. This change 2 groups, or a possible change in round- 20, 2012.
may also have contributed to the lower opi- ing patterns by the hospitalists. However, 2. Total hip replacement. American Academy
of Orthopaedic Surgeons Web site. http://
ate use on the floor for total knee surgery there was no evidence other than improved
orthoinfo.aaos.org/topic.cfm?topic=a00377.
postoperatively. Another variable evaluated pain control to explain the decreased length Updated December 2011. Accessed October
was intraoperative surgical site injections, of stay. There was no change in physical 20, 2012.
as both total knee surgeons routinely in- therapy practice between the 2 cohorts and 3. Hidalgo DA, Pusic AL. The role of methocar-
bamol and intercostal nerve blocks for pain
jected either the “subcutaneous tissues” or improved pain control seems to be respon- management in breast augmentation. Aesthet
the “posterior capsule.” Surgeon 3 used the sible for improvements in knee flexion and Surg J. 2005; 25(6):571-575.
same formula in both 2008 and 2011: bu- walking distances. 4. Schneider MS. Methocarbamol: adjunct ther-
pivacaine 0.25% 50 mL, preservative-free apy for pain management in breast augmen-
tation. Aesthet Surg J. 2002; 22(4):380-381.
morphine 5 mg, and ketorolac 30 mg. Sur- CONCLUSION
5. Schneider MS. Pain reduction in breast aug-
geon 2 injected bupivacaine 0.25% 50 mL This retrospective 2-cohort pilot study mentation using methocarbamol. Aesthetic
and preservative-free morphine 5 mg in showed that the addition of preoperative Plast Surg. 1997; 21(1):23-24.
2008 and bupivacaine 0.25% 50 mL alone intravenous methocarbamol and intrave- 6. White PF. The changing role of non-opioid
in 2011. Subgroup analysis focusing on nous acetaminophen led to significant im- analgesic techniques in the management
of postoperative pain. Anesth Analg. 2005;
the type of surgery subdivided by surgeon provements in the care of patients under- 101(5 Suppl):S5-22.
(Table 3; Figures 3,4) revealed that the opi- going total knee and hip surgery at Florida 7. Sinatra RS, Jahr JS, Reynolds LW, Viscusi
oid use group means were significantly dif- Hospital Winter Park. The expanded use ER, Groudine SB, Payen-Champenois C.
Efficacy and safety of single and repeated
ferent (surgeon 1 compared with surgeon 2 of these medications postoperatively for
administration of 1 gram intravenous acet-
for total hip and surgeon 3 compared with 48 hours should be studied in a prospec- aminophen injection (paracetamol) for pain
surgeon 2 for total knee). The ANOVA test tive, randomized, controlled clinical trial management after major orthopedic surgery.
Anesthesiology. 2005; 102(4):822-831.
to determine if the surgeon differences of total hip and knee patients. Based on
8. Sinatra RS, Jahr JS, Reynolds L, et al. Intra-
were responsible for overall group changes the data of this study, in order to reduce venous acetaminophen for pain after major
from 2008 protocol to 2011 protocol was opioid use by at least 10%, reduce pain orthopedic surgery: an expanded analysis.
not significant. Thus, the minor differences scores by at least 10%, and avoid con- Pain Pract. 2012; 12(5):357-365.
in surgeon practice probably influenced founding variables, the proposed 2-armed
the opioid use, but did not affect the out- randomized controlled trial would need
come changes and were not confounding 90 patients in each arm. This study is pres-
variables. ently in the planning stage.
32 ORTHOPEDICS | Healio.com/OrthopedicsYou can also read