WHo Global report on falls Prevention in older Age - WHO ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Ageing and Life Course, Family and Community Health
WHO Global Report
on Falls Prevention in Older Age
PAGE 1Ageing and Life Course, Family and Community Health
WHO Global Report
on Falls Prevention in Older AgeWHO Library Cataloguing-in-Publication Data
WHO global report on falls prevention in older age.
1.Accidental falls - prevention and control. 2.Risk factors. 3. Population dynamics. 4.Aged.
I.World Health Organization.
ISBN 978 92 4 156353 6 (NLM classification: WA 288)
© World Health Organization 2007
All rights reserved. Publications of the World Health Organization can be obtained from WHO
Press, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel.: +41
22 791 3264; fax: +41 22 791 4857; e-mail: bookorders@who.int). Requests for permission to
reproduce or translate WHO publications – whether for sale or for noncommercial distribution –
should be addressed to WHO Press, at the above address (fax: +41 22 791 4806; e-mail: permis-
sions@who.int).
The designations employed and the presentation of the material in this publication do not imply
the expression of any opinion whatsoever on the part of the World Health Organization concern-
ing the legal status of any country, territory, city or area or of its authorities, or concerning the
delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border
lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that
they are endorsed or recommended by the World Health Organization in preference to others of
a similar nature that are not mentioned. Errors and omissions excepted, the names of propri-
etary products are distinguished by initial capital letters.
All reasonable precautions have been taken by the World Health Organization to verify the
information contained in this publication. However, the published material is being distributed
without warranty of any kind, either expressed or implied. The responsibility for the interpreta-
tion and use of the material lies with the reader. In no event shall the World Health Organiza-
tion be liable for damages arising from its use.
Printed in France
Design: Langfeldesigns.com Marilyn Langfeld/Art Director, Adina Murch/Design,
© Ann Feild/Didyk Illustration
PAGE iiWho global report on falls prevention in older age
Contents
Chapter I
Magnitude of falls – A worldwide overview 1
1. Falls 1
2. Magnitude of falls worldwide 1
3. Population ageing 3
4. Main risk factors for falls 4
5. Main protective factors 6
6. Costs of falls 6
7. References 7
Chapter II
Active ageing: A Framework for the Global Strategy for the prevention of falls in older age 10
1. What is 'Active Ageing'? 10
2. References 12
Chapter III
Determinants of Active Ageing as they relate to falls in older age 13
1. Cross-cutting determinants: Culture and gender 13
2. Determinants related to health and social services 14
3. Behavioural determinants 15
4. Determinants related to personal factors 16
5. Determinants related to the physical environment 18
6. Determinants related to the social environment 18
7. Economic determinants 19
8. References 19
Chapter IV
Challenges for prevention of falls in older age 20
1. Changing behaviour to prevent falls 20
2. References 25
Chapter V
Examples of effective policies and interventions 26
1 Policy 26
2. Prevention 29
3. Practice – Interventions 32
4. Concluding remarks 33
5. References 33
Chapter VI
WHO falls prevention model within the Active Ageing framework 35
1. The need 35
2. The foundation 37
3. Three pillars of the WHO Falls Prevention Model 39
4. The way forward 47
PAGE iAcknowledgements
This global report is the product of the conclusions reached and recommenda-
tions made at the WHO Technical Meeting on Falls Prevention in Older Age which
took place in Victoria, Canada in February 2007. The report includes international
and regional perspectives on falls prevention issues and strategies and is based
on a series of background papers that were prepared by worldwide recognized ex-
perts. The papers are available at: http://www.who.int/ageing/projects/falls_pre-
vention_older_age/en/index.html
The report was developed by the Department of Ageing and Life Course (ALC)
under the direction of Dr Alexandre Kalache and the coordination of Dr Dongbo
Fu who was closely assisted by Ms Sachiyo Yoshida. ALC would like to thank three
institutions for their financial and technical support: the Division of Aging and
Seniors, Public Health Agency of Canada; the Department of Healthy Children,
Women and Seniors, British Columbia Ministry of Health and the British Columbia
Injury Prevention and Research Unit.
The contribution and input of the following experts are gratefully acknowledged:
Dr W. Al-Faisal (Syria), Ms Lynn Beattie (U.S.A), Dr Hua Fu (China), Dr K. James
(Jamaica), Dr S. Kalula (South Africa), Dr B. Krishnaswamy (India), Dr Nabil Kronfol
(Lebanon), Dr P. Marin (Chile), Dr Ian Pike (Canada), Dr Debra J. Rose (U.S.A.),
Dr Vicky Scott (Canada), Dr Judy Stevens (U.S.A), Prof. Chris Todd (the United
Kingdom), Dr G. Usha ( India ) and Dr Wojtek J. Chodzko-Zajko (U.S.A.).
Editing, layout and printing of the report was managed by Mrs Carla Salas-Rojas
(ALC).
PAGE iiWho global report on falls prevention in older age
Chapter I. Magnitude of falls – A worldwide
overview
1. Falls (5-7). The frequency of falls increases with
age and frailty level. Older people who are
Falls are prominent among the exter-
living in nursing homes fall more often
nal causes of unintentional injury. They
than those who are living in community.
are coded as E880-E888 in International
Approximately 30-50% of people living in
Classification of Disease-9 (ICD-9), and as
long-term care institutions fall each year,
W00-W19 in ICD-10, which include a wide
and 40% of them experienced recurrent
range of falls including those on the same
falls (8).
level, upper level, and other unspecified
falls. Falls are commonly defined as “in- The incidence of falls appears to vary
advertently coming to rest on the ground, among countries as well. For instance, a
floor or other lower level, excluding inten- study in the South-East Asia Region found
tional change in position to rest in furni- that in China, 6-31% (9-13) while another,
ture, wall or other objects”. found that in Japan, 20% (14) of older adults
fell each year. A study in the Region of the
a) Problems in defining falls. Americas (Latin/Caribbean region) found
The adoption of a definition is an the proportion of older adults who fell each
important requirement when studying year ranging from 21.6% in Barbados to 34%
falls as many studies fail to specify an in Chile (15).
operational definition, leaving room for
b) Fall injury rates.
interpretation to study participants. This
results in many different interpretations The rate of hospital admission due to falls
of falls. For example, older people tend to for people at the age of 60 and older in
describe a fall as a loss of balance, whereas Australia, Canada and the United Kingdom
health care professionals generally refer to of Great Britain and Northern Ireland (UK)
events leading to injuries and ill health (1). range from 1.6 to 3.0 per 10 000 population.
Therefore, the operational definition of a fall Fall injury rates resulting in emergency
with explicit inclusion and exclusion criteria, department visits of the same age group
is highly important. in Western Australia and in the United
Kingdom are higher: 5.5-8.9 per 10 000
population total.
2. Magnitude of falls worldwide
a) Frequency of falls.
Approximately 28-35% of people aged of
65 and over fall each year (2-4) increasing
to 32-42% for those over 70 years of age
PAGE 1c) Need of medical attention. d) Fall mortality rates.
Falls and consequent injuries are major Falls account for 40% of all injury deaths
public health problems that often require (27). Rates vary depending on the country
medical attention. Falls lead to 20-30% of and the studied population. Fall fatality
mild to severe injuries, and are underlying rate for people aged 65 and older in United
cause of 10-15% of all emergency depart- States of America (USA) is 36.8 per 100
ment visits (18). More than 50% of injury- 000 population (46.2 for men and 31.1 for
related hospitalizations among people women) (28) whereas in Canada mortality
over 65 years and older (19). The major rate for the same age group is 9.4 per 10 000
underlying causes for fall-related hospital population (29). Mortality rate for people
admission are hip fracture, traumatic brain age 50 and older in Finland is 55.4 for men
injuries and upper limb injuries. and 43.1 for women per 100 000 population
(30).
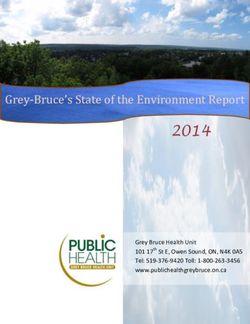
The duration of hospital stay due to falls
varies; however it is much longer than other Figure 1 (page 3) shows fatal falls by 5-year
injuries. It ranges from four to 15 days in age group and sex (31). Fatal falls rates
Switzerland (20), Sweden (21), USA (22), increase exponentially with age for both
Western Australia (23), Province of British sexes, highest at the age of 85 years and
Columbia and Quebec in Canada (24). In over. Rates of fatal falls among men exceed
the case of hip fractures, hospital stays that of women for all age groups in spite
extend to 20 days (25). With the increas- of the fewer occurrences of falls among
ing age and frailty level, older person are them. This is attributed to the fact that men
likely to remain in hospital after sustaining suffer from more co-morbid conditions
a fall-related injury for the rest of their life. than women of the same age (28). A similar
Subsequently to falls, 20% die within a year difference in mortality between men and
of the hip fracture (26). women has been reported following hip
fracture. The incidence of hip fracture is
In addition, falls may also result in a post-
greater among women while hip fracture
fall syndrome that includes dependence,
mortality is higher among men (32). One
loss of autonomy, confusion, immobiliza-
study found that men reported poorer
tion and depression, which will lead to a
health and a greater number of underlying
further restriction in daily activities.
conditions than women, which substan-
tially increased the impact of hip fracture
and consequently increased the risk of
mortality (33). Or is it not that men who fall
have more co-morbidity than other men in
general.
PAGE 2Who global report on falls prevention in older age
Figure 1. Fatal falls rate by age and sex group
Fatal falls rates
Men
200 Women
153.2
150
106.4
100
63.9
50 41.4
34
16 19
5.4 10.6 9.5
0
65-69 70-74 75-79 80-84 85+ Age group
In the U.S.A. 2001 Source : National Council on Ageing, 2005 (31)
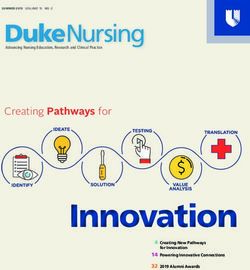
3. Population
30 ageing with a decreasing proportion of younger
population. The triangular population pyra-
"Population ageing is a triumph of human- mid of 2005 will be replaced with a more
ity but also a 24
challenge to society" (34). cylinder-like structure in 2025.
Worldwide, the number of persons over
60 years is growing faster than any other a) Impact of population ageing on falls.
18
age group. The number of this age group
Falls prevention is a challenge to popula-
was estimated to be 688 million in 2006,
12 to almost two billions tion ageing. The numbers of falls increase in
projected to grow
magnitude as the numbers of older adults
by 2050. By that time, the population of
increase in many nations throughout the
6 be much larger than that
older people will
world. Falls exponentially increase with
of children under the age of 14 years for
age-related biological change, therefore a
the first time in human history. Moreover,
0 pronounced number of persons over the age
the oldest segment0-9of population,
65-69 aged 80
of 80 years will trigger substantial increase
and over, particularly prone to falls and its
of falls and fall injury at an alarming rate. In
consequences is the fastest growing within
fact, incidence of some fall injuries, such as
older population expected to represent 20%
fractures and spinal cord injury, have mark-
of the older population by 2050 (35).
edly increased by 131% during the last three
Figure 2 illustrates the population pyramid decades (36). If preventive measures are not
in 2005 and 2025. It highlights the growing taken in immediate future, the numbers of
proportion of older population in parallel injuries caused by falls is projected to be
100% higher in the year 2030 (36).
PAGE 3This applies to many developing countries dimensions: biological, behavioural, envi-
where currently close to 70% of the elderly ronmental and socioeconomic factors.
population lives, and where population
Figure 3 encapsulates the risk factors and
ageing is occurring rapidly. “Unlike the
the interaction of them on falls and fall-
developed world that became richer before
related injuries. As the exposure to risk
getting older, developing countries are
factors increases, the greater becomes the
getting older before becoming richer” (37).
risk of falling and being injured.
This is reflected in the fact that health in
older age is neglected in some developing
countries. Falls prevention is one of the a) Biological risk factors
issues that have not been given a sufficient
Biological factors embrace characteristics
attention. For instance, there is a lack of
of individuals that are pertaining to the
epidemiological data in many regions of the
human body. For instance, age, gender and
developing world.
race are non-modifiable biological factors.
These are also associated with changes due
to ageing such as the decline of physical,
4. Main risk factors for falls cognitive and affective capacities, and the
Falls occur as a result of a complex interac- co-morbidity associated with chronic ill-
tion of risk factors. The main risk factors nesses.
reflect the multitude of health determi-
nants that directly or indirectly affect
well-being. Those are categorized into four
Figure 2. Global population pyramid in 2005 and 2025
Age group
Males Females
80+
70-74 2025
2005
60-64
50-54
40-44
30-34
20-24
10-14
0-4
400000 300000 200000 100000 0 100000 200000 300000 400000
Population in thousands
Source : UN, 2004 (35)
PAGE 4Who global report on falls prevention in older age
Figure 3. Risk factor model for falls in older age
Behavioural risk factors
-Multiple medication use
-Excess alcohol intake
-Lack of excercise
-Inappropriate footware
Environmental risk factors Biological risk factors
Falls and -Age, gender and race
-Poor building design
-Chronic illnesses (e. g. Parkinson,
-Slippery floors and stairs fall-related Arthritis, Osteoporosis)
-Looser rugs
-Insufficient lighting injuries -Physical, cognitive and affective
-Cracked or uneven sidewalks capacities decline
Socioeconomic risk factors
-Low income and education levels
-Inadequate housing
-Lack of social interactions
-Limited access to health and social services
-Lack of community resources
The interaction of biological factors with c) Environmental risk factors
behavioural and environmental risks
Environmental factors encapsulate the
increases the risk of falling. For example,
interplay of individuals' physical conditions
the loss of muscle strength leads to a loss
and the surrounding environment, includ-
of function and to a higher level of frailty,
ing home hazards and hazardous features
which intensifies the risk of falling due to
in public environment. These factors are
some environmental hazards (see Chapter 3
not by themselves cause of falls – rather,
for further information).
the interaction between other factors and
their exposure to environmental ones.
b) Behavioural risk factors
Home hazards include narrow steps, slip-
Behavioural risk factors include those pery surfaces of stairs, looser rugs and
concerning human actions, emotions or insufficient lighting (29). Poor building
daily choices. They are potentially modifi- design, slippery floor, cracked or uneven
able. For example, risky behaviour such as sidewalks, and poor lightening in public
the intake of multiple medications, excess places are such hazards to injurious falls
alcohol use, and sedentary behaviour can (see Chapter 3 for further information).
be modified through strategic interventions
for behavioural change (see Chapter 3 and 4
for further information).
PAGE 5d) Socioeconomic risk factors 6. Costs of falls
Socioeconomic risk factors are those The economic impact of falls is critical to
related to influence social conditions and family, community, and society. Health-
economic status of individuals as well as care impacts and costs of falls in older age
the capacity of the community to challenge are significantly increasing all over the
them. These factors include: low income, world. Fall-incurred costs are categorized
low education, inadequate housing, lack of into two aspects:
social interaction, limited access to health
and social care especially in remote ar- Direct costs encompass health care costs
eas, and lack of community resources (see such as medications and adequate services
Chapter 3 for further information) e.g. health-care-provider consultations in
treatment and rehabilitation.
Indirect costs are societal productivity
5. Main protective factors losses of activities in which individuals or
family care givers would have involved if
Protective factors for falls in older age are
he/she had not sustain fall-related injuries
related to behavioural change and environ-
e.g. lost income.
mental modification. Behavioural change
to healthy lifestyle is a key ingredient to This section briefly shows an overview of
encourage healthy ageing and avoid falls. health service impacts and costs of falls in
Non-smoking, moderate alcohol consump- some developed countries. This is due to
tion, maintaining weight within normal the lack of data in developing countries.
range in mid to older age, playing an ac-
ceptable level of sport protect older people a) Direct health system costs
from falling (38). Furthermore, self-health
The average health system cost per one fall
behaviour (e.g. proper level of simple …
injury episode for people 65 year and older in
walking) is integral to healthy ageing and
Finland and Australia was US$ 3611 (origi-
independence.
nally AUS$ 6500 in 2001-2002) and US$ 1049
One example of the environmental modi- (originally in €944 in 1999) respectively (23,
fications is home modification. It prevents 40).
older persons from hidden fall hazards in
daily activities at home. The modification
includes installation of stairway protec-
tive devices such as railings, grab bars and
slip-resistant surfacing in the bathroom
and provision of lighting and handrails (39).
Age-friendly design in public environment
is also critical factor to avoid falls among
older adults. (see Chapter 5 for further
information).
PAGE 6Who global report on falls prevention in older age
Among different cost items, hospital 7. References
inpatient services cost is the greatest cost,
accounting for about 50% of total cost of 1. Zecevic AA et al. (2006). Defining a fall and
falls (19, 22, 23). The cost of hospital inpa- reasons for falling: Comparisons among the
tient services includes the emergency and views of seniors, health care providers, and the
research literature. The Gerontologist, 46:367-
general holding ward cost, of those admit- 376.
ted to either the general holding ward or to
2. Blake A et al.(1988). Falls by elderly people at
hospital. The second highest is the long- home: prevalence and associated factors. Age
term care costs, contributing to 9.4% to 41% Ageing, 17:365-372.
of all health system costs (23, 25). 3. Prudham D, Evans J (1981). Factors associated
with falls in the elderly: a community study.
The average cost of hospitalization for fall re- Age Ageing, 10:141-146.
lated injury for people 65 year and older range 4. Campbell AJ et al. (1981). Falls in old age: a
study of frequency and related clinical factors.
from US$ 6646 in Ireland to US$ 17 483 in the Age Ageing, 10:264-270.
USA (22, 41). This cost are projected to in- 5. Tinetti ME, Speechley M, Ginter SF (1988).
crease to US$ 240 billion by year 2040 (42). Risk factors for falls among elderly persons
living in the community. New England
Where the cost of a visit to an emergency
Journal of Medicine, 319:1701-1707.
department varies widely across countries,
6. Downton JH, Andrews K (1991). Prevalence,
ranging from US$ 236 in the USA (based characteristics and factors associated with
on data collected in 1998) (22) to US$ 2472 falls among the elderly living at home. Aging
(Milano), 3(3):219-28.
in Western Australia (based on data col-
7. Stalenhoef PA et al. (2002). A risk model for
lected in 2001-2002) (23). the prediction of recurrent falls in community-
dwelling elderly: A prospective cohort study.
b) Indirect costs Journal of Clinical Epidemiology, 55(11):1088-
1094.
In addition to the substantial direct costs 8. Tinetti ME (1987). Factors associated with
outlined above, falls incur indirect costs that serious injury during falls by ambulatory
are critical to family e.g. the loss of produc- nursing home residents. Journal of the
American Geriatrics Society, 35:644-648.
tivity of family caregivers. The average lost
9. Wannian Liang, Ying Liu, e.a. Xueqing Weng
earnings could approximate US$ 40 000 per (2004). An epidemiological study on injury of
annum in the United Kingdom (25). Even the community-dwelling elderly in Beijing.
Chinese Journal of Disease Control and
when family caregivers are more morally Prevention, 8(6):489-492.
and culturally accepted, falls remain a sig- 10. Suzhen L, Jiping L, Y C (2004). Body function
nificant burden to household economy. and fall-related factors of the elderly in
community. Journal of Nursing Science,
19(6):5-7.
PAGE 711. Weiping M, Lihua Y (2002). Analysis of risk 23. Hendrie D et al. (2003). Injury in Western
factors for elderly falls. Chinese Journal of Australia: The health system costs of falls
Behavioural Medical Science, 11(6):697-699. in older adults in Western Australia. Perth,
12. Gang L, Sufang J, YS (2006). The incidence Western Australia, Western Australian
status on injury of the community-dwelling Government.
elderly in Beijing (in Chinese). Chinese Journal 24. Herman M, Gallagher E, Scott VJ (2006).
of Preventive Medicine, 40(1):37. The evolution of seniors' falls prevention in
13. Litao L, Shengyong W, Shong Y (2002). A British Columbia. Victoria, British Colombia,
British Columbia Ministry of Health http://
study on risk factors for falling down in elderly
www.health.gov.bc.ca/library/publications/
people of rural areas in Laizhou city. Chinese
year/2006/falls_report.pdf, accessed 27 August
Journal of Geriatrics, 21(5):370-372. 2007).
14. Yoshida H, Kim H (2006). Frequency of falls 25. The University of York (2000). The economic
and their prevention (in Japanese). Clinical cost of hip fracture in the U.K., Health
Calcium, 16(9):1444-1450. Promotion, England.
15. Reyes-Ortiz CA, Al Snih S, Markides KS 26. Zuckerman JD (1996). Hip fracture. New
(2005). Falls among elderly persons in Latin England Journal of Medicine, 334(23):1519-
America and the Caribbean and among elderly 1525.
Mexican-Americans. Revista Panamericana de
Salud Pública, 17(5-6):362-369. 27. Rubenstein LZ (2006). Falls in older people:
epidemiology, risk factors and strategies for
16. Stevens JA, Sogolow ED (2005). Gender prevention. Age Ageing, 35-S2:ii37-ii41.
differences for non-fatal unintentional fall
related injuries among older adults. Injury 28. Stevens JA et al. (2007). Fatalities and Injuries
Prevention, 11(2):115-119. From Falls Among Older Adults, United
States, 1993-2003 and 2001-2005. Journal of
17. Gregg EW et al. (2000). Diabetes and physical the American Medical Association, 297(1):32-
disability among older U.S. adults. Diabetes 33.
Care, 23(9):1272-1277.
29. Division of Aging and Seniors, PHAC. Canada
18. Scuffham P, Chaplin S, Legood R (2003). (2005). Report on senior's fall in Canada.
Incidence and costs of unintentional falls in Ontario, Division of Aging and Seniors. Public
older people in the United Kingdom. Journal of Health Agency of Canada.
Epidemiology and Community Health, 57:740-
744. 30. Kannus P et al (2005). Fall-induced deaths
among elderly people. American Public Health
19. Scott VJ (2005). Technical report: Association, 95(3):422-424.
hospitalizations due to falls among Canadians
age 65 and over. In Report on Seniors' falls in 31. National Council on Ageing (2005). Falls
Canada. Canada, Minister of Public Works and among older adults: risk factors and prevention
Government Services. strategies. In Fall free: promoting a national
falls prevention action plan. J.A. Stevens Eds..
20. Seematter-Bagnoud L et al. (2006). Healthcare
utilization of elderly persons hospitalized after 32. Fransen M et al. (2002). Excess mortality or
a noninjurious fall in a Swiss academic medical institutionalization after hip fracture: men
center. Journal of the American Geriatrics are at greater risk than women. Journal of the
Society, 4(6):891-897. American Geriatrics Society, 50(4):685-690.
21. Bergeron E et al. (2006). A simple fall in the 33. Hernandez JL et al. (2006). Trend in hip
elderly: not so simple. Journal of Trauma, fracture epidemiology over a 14-year period
60(2):268-273. in a Spanish population. Osteoporosis
International, 17: 464-470.
22. Roudsari B et al. (2005). The acute medical
care costs of fall-related injuries among the 34. World Health Organization (2002). Active
U.S. older adults. Injury, 36(11):1316-1322. Ageing: A Policy Framework. Geneva.
PAGE 8Who global report on falls prevention in older age
35. United Nations (UN) (2004). World Population 40. Nurmi I., Luthje P (2002). Incidence and
Prospects: The 2004 Revision. New York, USA. costs of falls and fall injuries among elderly
36. Kannus P et al. (2007). Alarming rise in the in institutional care. Scandinavian Journal of
number and incidence of fall-induced cervical Primary Health Care, 20(2):118-122.
spine injuries among older adults. Journal of 41. Carey D, Laffoy M (2005). Hospitalisations due
Gerontology: Biological Sciences and Medical to falls in older persons. Irish Medical Journal,
Sciences, 62(2):180-183. 98(6):179-181.
37. Kalache A, Keller I (2000). The greying world: a 42. Cummings SR, Rubin SM, Black D (1990).
challenge for the 21st century. Science Progress, The future of hip fractures in the United
83(1):33-54. States. Numbers, costs, and potential effects
38. Peel NM, McClure RJ, Hendrikz JK (2006). of postmenopausal estrogen. Clinical
Health-protective behaviours and risk of Orthopaedics and Related Research,
fall-related hip fractures: a population-based (252):163-166.
case-control study. doi: 10.1093/ageing/afl056.
Age Ageing, 35(5):491-497.
39. American Geriatrics Society, British
Geriatrics Society, and American Academy
of Orthopaedic Surgeons Panel on Falls
Prevention (2001). Guideline for the prevention
of falls in older persons. Journal of the
American Geriatrics Society, 49(5):664-672.
PAGE 9Chapter II. Active Ageing: a framework for the global
strategy for the prevention of falls in older age
The WHO's Active Ageing policy offers a gender and culture, which are cross-cut-
coherent framework on which to develop a ting, and six additional groups of comple-
strategy for the prevention of falls in older mentary and interrelated determinants:
age worldwide.
1. access to health and social services,
a) What is 'Active Ageing'?
2. behavioural,
Active Ageing is the process of optimizing
opportunities for health, participation and 3. physical environment,
security in order to enhance quality of life 4. personal,
as people age.
5. social, and
Active Ageing depends on a variety of
influences or determinants that surround 6. economic.
individuals, families and communities as
expressed in Figure 1 below. They include
Figure 4. The determinants of Active Ageing
Gender
Health and
Economic social services
determinants
Behavioural
Active determinants
Social Ageing
determinants
Personal
determinants
Physical
environment
Culture
Source: Active Ageing: A Policy Framework, WHO, 2002 (http://www.who.int/ageing/publications/active/en/index.html)
PAGE 10Who global report on falls prevention in older age
Figure 2. Maintaining functional capacity over the life course
Early life Adult life Older age
Growth and Maintaining highest Maintaining independence
development possible level of function andpreventing disability
Functional capacity
Rang
e
in ind of functio
ividu n
als
Disability threshold*
Rehabilitation and ensuring
the quality of life
Age
Source: Active Ageing: A Policy Framework, WHO, 2002
Source: Active Ageing: A Policy Framework, WHO, 2002
In addition, there are the underlying 'bio- of decline is largely determined by factors
logical' factors which can play a significant related to lifestyle behaviours, as well as ex-
role as preventing individuals from falls ternal social, environmental and economic
and consequent injuries or, conversely, can factors. From an individual and societal
act as risk factors. All of these determi- perspective, it is important to remember
nants, and the interplay between them, play that the speed of decline can be influenced
an important role in affecting how high or and may be reversible at any age through
low is the risk of falling and/or if a fall oc- individual and public policy measures, such
curs, the risk of sustaining serious injuries. as promoting an age-friendly living envi-
ronment. An example of particular impor-
These determinants have to be understood
tance within the context of falls, relates to
from a life course perspective which rec-
bone mass. Good nutrition and optimum
ognizes that older persons are not a homo-
levels of physical activity throughout child-
geneous group and that individual diver-
hood and adolescence are critical for the
sity increases with age. This is expressed
development of healthy bones. As individu-
in Figure 2 (next page), which illustrates
als age they experience a gradual decline in
that functional capacity (such as muscu-
bone mass. Once again, healthy life styles
lar strength and cardiovascular output)
can slow down the process. For post meno-
increases in childhood to peak in early
pausal women in particular, such life styles
adulthood and eventually decline. The rate
PAGE 11are crucially important to counterbalance • Drop off and pick up bays close to build-
the hormonal factors that can precipitate ings and transport stops are provided for
the onset of osteoporosis. For some sec- handicapped and older people.
ondary prevention through drug-therapy
becomes an indispensable form of interven-
tion for avoiding bone fractures as a conse- 2. References
quence of even relatively minor traumas.
1. World Health Organization. Active Ageing –
A Policy Framework. Geneva: World Health
Active ageing is a lifelong process. Thus,
Organization, 2002.
age-friendly environments with barrier-
free buildings and streets, adequate public
transportation and accessible sources of
information and communication enhance
the mobility and independence of younger
as well as older persons who present the
risk of developing disabilities. Secure
neighbourhoods allow children, younger
women and older persons to venture out-
side in confidence to participate in physi-
cally active leisure and in social activities –
contributing to preventing falls at all ages,
particularly at old age. The operative word
in a society committed to active ageing is
enablement – for instance through initia-
tives such as:
• Affordable parking is available.
• Priority parking bays are provided for
older people close to buildings and
transport stops.
• Priority parking bays are provided for
people with disabilities close to buildings
and transport stops, the use of which are
monitored.
PAGE 12Who global report on falls prevention in older age
Chapter III. Determinants of Active Ageing as they
relate to falls in older age
Approaching falls in older age within the Cultural preferences are also reflected in
framework of the determinants of Active the design of public and private spaces
Ageing help us to develop effective inter- – such as shining floors and steps or
ventions and policies. The following section staircases without appropriate railings.
summarizes what is known about how the
Culture also contributes to the stigma of
determinants of Active Ageing affect falls
requesting help where that is needed or
in older age.
even unavoidable – for instance, where
1. Cross-cutting determinants: negotiating architectonic barriers that
culture and gender should not be there in the first place
but, if they are, asking for help should
a) Culture
come naturally rather than a reason for
Cultural values and traditions determine embarrassment.
to a large extent how a given society views b) Gender
older people and falls in older age.
While falls are more common among older
Culturally driven expectations affect how women than men fall-related mortality
people view older persons and falls in older is higher among older men. Policies and
age. In some cultures, social participation programmes on falls prevention need to
in older age is not seen as a virtue: the reflect a gender perspective.
perception is that old people are meant “to
rest”. In practice, this results in some older As is outlined in Chapter 1, women are
people adopting sedentary life often in more likely than men to fall and sustain
isolation due to the resignation from social, fracture (1), resulting in twice more hos-
economic and cultural participation, with pitalizations and emergency department
a resulting increase in the risk of falling. visits than men (2). However, fall-related
Furthermore, in many societies, falls in mortality disproportionately affects men.
older age are perceived as "an inevitable
The difference in falls in older age may stem
natural part of ageing" or "unavoidable
from the gender-related factors, such as
accidents". All these contribute to falls
women being inclined to make greater use
prevention not to be considered as a matter
of multiple medications and living alone
of priority on governmental agendas -
(3). In addition, biological difference also
leading to a loss of financial provisions
contributes to greater risk, for instance,
required to develop surveillance systems,
appropriate interventions and clinical
diagnostic techniques, as well as treatment
regimens for falls and fall-related injuries.
PAGE 13women's muscle mass declines faster than 2. Determinants related to health
that of men, especially in the immediate and social services
few years after menopause. To some extent
Health and social services providers are by and
this is gender-related as women are less
large unprepared to prevent and manage falls
likely to engage into the practice of muscu-
in older age.
lar building physical activity though the life
course e.g. sports. Falls in older age has been a neglected
public health problem in many societies,
Health seeking behaviour differs according
particularly in the developing world. Many
to gender. Culturally-oriented expectations
health and social services providers are
to gender roles affect behaviour when seek-
unprepared to prevent and manage falls in
ing medical care. Male higher fatality rates
older age as they lack sufficient knowledge
may be due in part to the tendency of men
to treat the conditions that predispose their
not seeking medical care until a condition
consequences and complications.
becomes severe, resulting in substantial
delay to the access to prevention and man- Falls in older age are often iatrogenic
agement of diseases. Further, men are more conditions – that is, induced by incorrect
likely to be engaged in intense and danger- diagnoses and treatments. Examples in-
ous physical activity and risky behaviours clude over-prescription of medications that
– such as climbing high ladders, cleaning cause side effects and interactions among
roofs or ignoring the limits of their physical the drugs, inadequate dosage and lack of
capacity. warning to make older people aware about
their effects.
Various policy options and falls prevention
strategies for men and women based on Appropriate training programmes cover-
gender differences in locations, circum- ing knowledge and skills in falls prevention
stances and events preceding falls and fall- and management should be a priority in
related injuries are needed. primary heath care (PHC) settings, where
increasing number of patients are older
people. PHC practitioners should be well
versed in the diagnosis and management of
falls and fall-related injuries. In addition,
social services that ensure the accessibility
of older people to falls prevention pro-
grammes are critical.
PAGE 14Who global report on falls prevention in older age
3. Behavioural determinants b) Healthy eating
a) Physical activity Eating a balanced diet rich in calcium may
decrease the risk injuries resulting from falls in
Regular participation in moderate physical older people.
activity is integral to good health and maintain-
ing independence, contributing to lowering risk Eating a healthy balanced diet is central to
of falls and fall-related injuries. healthy ageing. Adequate intake of protein,
calcium, essential vitamins and water are
Regular participation in moderate physi- essential for optimum health. If deficien-
cal activity is integral to good health and cies do exist, it is reasonable to expect that
maintaining independence. It prevents weakness, poor fall recovery and increase
onset of multiple pathologies and func- risk of injuries will ensure. Growing evi-
tional capacity decline. Moderate physi- dence supports dietary calcium and vita-
cal activities and exercise also lowers risk min D intake improves bone mass among
of falls and fall-related injuries in older persons with low bone density and that it
age through controlling weight as well as reduces the risk of osteoporosis and falling
contributing to healthy bones, muscles, and (6). No dairy and fish consumption were as-
joints (4). Exercise can improve balance, sociated with a higher risk of falling. Older
mobility and reaction time. It can increases persons with low dietary intake of calcium
bone mineral density of postmenopausal and vitamin D may be at risk for falls and
women and individuals aged 70 years and therefore fractures resulting from them (7).
over (5).
Use of excessive alcohol has been shown to
Moreover, it should be noticed that partici- be a risk factor of falls. Consumption of 14
pation in vigorous physical activities – for or more drinks per week is associated with
instance intensive running in older age an increased risk of falls in older adults (7).
may increase the risk of falls. Promoting
appropriate physical activities or exercises
to improve strength, balance, and flexibility
is one of the most feasible and cost-effec-
tive strategies to prevent falls among older
adults in the community. Activities such as
outdoor walking or mall walking indoors
is the most feasible and accessible way of
exercising that improves strength, balance
and flexibility leading to a reduction on the
risk of falling. Other kind of effective physi-
cal activities and exercises are mentioned
in Chapter 5.
PAGE 15c) Use of medicines Wearing poor fitting shoes is also a risk
taking behaviour. Walking in socks without
Older people tend to take more drugs than shoes or in slippers without a sole increases
younger people. Also as people age, they the risk of slipping indoor. Appropriate
develop altered mechanisms for absorbing shoes are particularly important – avoiding
and metabolizing drugs. If older persons high heels, thin and hard soles, or slippers
don't take medications as directed by health of unsuitable size and that do not stick
professionals, their risk of falling can be closely to the feet.
affected in several ways. Effects of uncon-
trolled medical conditions and of medica-
tion because of non-adherence can provoke
4. Determinants related to personal
or generate altering alertness, judgement,
factors
and coordination; dizziness; altering the
balance mechanism and the ability to a) Attitudes
recognize and adapt to obstacles; and in-
People's attitudes influence their behaviours.
creased stiffness or weakness (7).
Attitudes affect how people interpret and cope
When prescribing new drugs to these older with falls in older age.
patients health professionals should fully
Older people's attitudes greatly influence
ascertain other drugs being taken, includ-
whether they will avoid fall-related risk-
ing self-prescribed medicines.
taking behaviours when they participate
d) Risk-taking behaviours in activities of daily living. If older people
perceive falls as a normal consequence of
The ordinary choices people make and the ageing expressed as "seniors will always
actions they take may increase their chance of fall" their attitudes may halt preventive
falling. measures.
Some risk-taking behaviours increase the Attitudes of policy-makers determine to
risk of falling in older age. Those behav- a large extent the amount of resources
iours include climbing ladders, standing on allocated to falls prevention and develop-
unsteady chairs or bending while perform- ment and enforcement of related policies.
ing activities of daily living, rushing with Awareness and attitudes of health profes-
little attention to the environment or not sionals to falls are essential to increased in-
using mobility devices prescribed to them centive in providing appropriate services for
such as a cane or walker (8). preventing and managing falls in older age.
PAGE 16Who global report on falls prevention in older age
Professionals who design public transporta- c) Coping with falls
tions, such as buses and subway systems,
The ability of coping with falls of both older
often do not make them age-friendly,
people and health professionals can lower
neglecting the risk of falls for older people.
the risk and consequences of falling.
For example, in some developing coun-
tries, buses are designed with not enough Falls are particularly difficult to manage in
seats and rails and the steps to climb into PHC settings because health professionals
them are too high. As a consequence, older lack enough knowledge and skills. Building
people incur the risk of falling because they coping skills of health professionals to pre-
have to stand or do not have the strength vent and manage falls needs to be empha-
to climb into the buses in the first place sized. For example, health professionals are
and cannot properly hold on for support. recommended to teach patients at risk of
Moreover, the steps on the public buses falling how to get up from the floor; unfor-
are often too high to older people and they tunately clinical experience suggests that
might fall when getting into the bus. this is rarely done (9).
b) Fear of falling
Physical and mental management of falls
Fear of falling is frequently reported by by older people and their family members
older persons. Older people are usually un- is also important. Therefore, training older
der the fear of falling again, being hurt or people at high risk to avoid falling needs to
hospitalized, not being able to get up after be encouraged.
a fall, social embarrassment, loss of inde- d) Ethnicity and race
pendence, and having to move from their
homes. Fear can positively motivate some Although the relationship between falls and
seniors to take precautions against falls and ethnicity and race remains widely open for
can lead to gait adaptations that increase research, Caucasians living in the USA have
stability. For others, fear can lead to a de- higher risk of falling. In addition, for both
cline in overall quality of life and increase men and women, the rate of hospitaliza-
the risk of falls through a reduction in the tion for fall-related injuries is some two to
activities needed to maintain self-esteem, four times higher among the Whites than
confidence, strength and balance. In addi- Hispanics and Asians/Pacific Islanders, and
tion, fear can lead to maladaptive changes about 20% higher than African-Americans
in balance control that may increase the (10). It is also clear differences observed
risk of falling. People who are fearful of between Singaporeans of Chinese, Malay
falling also tend to lack confidence in their and Indian ethnic origins, and between
ability to prevent or manage falls, which native Japanese older community dwellers
increases the risk of falling again (7). and Japanese-Americans and Caucasians.
Native Japanese people have much lower
rates of falls than Japanese-Americans and
Caucasians.
PAGE 175. Determinants related to the Factors related to the public environment
physical environment are also frequent causes of fall in older age.
Even walking on a familiar route can lead
Factors related to the physical environment are to falls as a consequence of poor building
the most common cause of falls in older age. design and inadequate consideration. Most
Physical environment plays a significant problematic factors are cracked or uneven
role in many falls in older age. Factors sidewalks, unmarked obstacles, slippery
related to the physical environment are the surfaces, poor lighting and lengthy distanc-
most common cause of falls in older people, es to sitting areas and public restrooms.
responsible for between 30 to 50% of them
(11). A number of hazards in the home and
public environment that interact with other 6. Determinants related to the social
risk factors, such as poor vision or balance, environment
contribute to falls and fall-related injuries.
Social connection and inclusion are vital to
For example, stairs can be problematic –
health in older age. Social interaction is in-
studies show that unsafe features of stairs
versely related to the risk of falls.
can be frequently identified including
uneven or excessively high or narrow steps, Isolation and loneliness are commonly
slippery surfaces, unmarked edges, dis- experiences by older people particularly
continuous or poorly-fitted handrails, and among those who lose their spouse or live
inadequate or excessive lighting. alone. They are much more likely than
other groups to experience disability and
Since approximately half of falls occurs
the physical, cognitive, and sensory limita-
indoor, the home environment is critical
tions that increase the risk of falls.
for avoiding them. A high particular risk
to falls was found in homes with irregular Isolation and depression triggered by lack
sidewalks to the residence, loose carpets on of social participation increase fear of fall-
the kitchen and bathroom floors, loose elec- ing, and vice versa. Fear of falling can in-
trical wires, and inconvenient doorsteps. crease the risk of falls through a reduction
Poor surroundings around home such as in social participation and loss of personal
garden paths and walks that are cracked or contact - which in turn increase isolation
slippery from rain, snow or moss are also and depression. Providing social support
dangerous. Entrance stairs and poor night and opportunities for older people to par-
lighting can also pose risks. ticipate in social activities to help maintain
active interaction with others may decrease
their risk of falls.
PAGE 18Who global report on falls prevention in older age
7. Economic determinants 8. References
Older people with lower economic status,
1. Stevens JA et al. (2006). The costs of fatal
especially those who are female, live alone or in and non-fatal falls among older adults. Injury
rural areas face an increased risk of falls. Prevention, 12(5):290-295.
2. Hendrie D et al. (2003). Injury in Western
Studies have shown that there is a rela- Australia: The Health System Cost of Falls
tionship between socioeconomic status in Older Adults in Western Australia. Perth,
Western Australia. Western Australian
and falls. Lower income is associated with Government.
increased risk of falling (12). Older people, 3. Ebrahim S, Kalache A (1996). Epidemiology in
especially those who are female, live alone Old Age. London, Blackwell BMJ Books.
or in rural areas with unreliable and insuffi- 4. Gardner MM, Robertson MG, Campbell AJ
(2000). Exercise in preventing falls and fall
cient incomes face an increased risk of falls. related injuries in older people: A review of
Poor environment in which they live, their randomised controlled trials. British Journal of
poor diet and the fact of not being able to Sports Medicine, 34:7-17.
access health care services even when they 5. Day M et al. (2002). Randomised factorial
trial of falls prevention among older people
have acute or chronic illness exacerbates living in their own homes. BMJ, doi:10.1136/
the risk of falling. bmj.325.7356.128.
6. Tuck SP, Francis RM (2002). Osteoporosis.
The negative cycle of poverty and falls in Postgraduate Medical Journal, 78:526-532.
older age is particularly evident in rural 7. Division of Aging and Seniors (2005). Report
areas and in developing countries. The fall- on senior's fall in Canada. Ontario. Public
Health Agency of Canada.
related burden to health system will keep
8. Gallagher EH, Brunt H (1996). Head over
increasing unless resources and money are heels: A clinical trial to reduce falls among the
allocated in order to provide proper PHC elderly. Canadian Journal on Aging, 15:84-96.
and opportunities to older people for social 9. Simpson JM, Salkin S (1993). Are elderly
people at risk of falling taught how to get up
participation. It is never too late to break again? Age Ageing, 22: 294-296.
this vicious cycle. 10. Ellis AA, Trent RB (2001). Hospitalized
fall injuries and race in California. Injury
Prevention, 7:316-320.
11. Rubenstein LZ (2006). Falls in older people:
epidemiology, risk factors and strategies for
prevention. Age and Ageing, 35-S2:ii37-ii41.
12. Reyes CA et al. (2004). Risk factors for falling
in older Mexican Americans. Ethnicity &
Disease, 14:417-422.
PAGE 19Chapter IV. Challenges for prevention of falls in
older age
1. Changing behaviour to prevent • it is within their ability to do so;
falls
• they have the resources to implement
The background papers that underlie this change (including physical, psychologi-
report refer to a considerable body of cal and social capital resources);
evidence indicating the effectiveness of a
number of interventions for falls preven- • the changes are perceived as being of
tion. These include strength and balance benefit to them; and
training, environmental modification and
• the benefit outweighs the cost or effort
medical care aimed at removing or reduc-
in overcoming barriers.
ing specific risk factors by for example
review of medications and reduction of For example, the older person may care for
polypharmacy. The systematic reviews, grandchildren, and thus using time to do
evidence syntheses and meta-analyses are exercises to maintain or improve physical
well referenced in the briefing papers to be function may appear in the immediate term
found at the following WHO URL: a poor use of time or impossible if it con-
flicts with childcare responsibilities. Thus,
http://www.who.int/ageing/projects/falls_
the programme will need to be tailored to
prevention_older_age/en/index.html
fit with these responsibilities, or the person
Crucial to the success of such interventions must be persuaded that a long-term gain
is changing the beliefs, attitudes and behav- (maintaining independence and seeing
iour of older people themselves, the health the grandchildren grow up) outweighs the
and social care professionals who provide short-term 'pain'. Most importantly, the
services, and the wider communities in society in which older people live must
which older people live. For example, a value them and be willing to allocate re-
fifteen-week balance and exercise class will sources to the maintenance of their health
only have an effect if the older person goes and well-being. Expression of valuing older
to the sessions, undertakes the exercises as people must include allocation of adequate
prescribed, and continues to practice after resources towards helping people to age
completion of the course. People will only well and take part in activities that have the
change their lifestyles if: potential to prevent falls.
PAGE 20Who global report on falls prevention in older age
This chapter is based heavily on a se- At present, advice from family members
ries of recommendations made by the and health professionals tends to empha-
Psychological Aspects of Falling Group size avoiding risk rather than engaging in
(1, 2), Work Package 4 of the Prevention of activities to improve strength and bal-
Falls Network Europe (ProFaNE) and fuller ance (3-5). Informing the general popula-
evidence for the recommendations has tion about the benefits of easy-to-provide
been published (1, 2). These recommenda- interventions such as strength and balance
tions should be sufficiently general to be training activities should influence older
applicable to populations other than the people’s views and counteract fatalistic
European population for which they were views that falling is a consequence of ageing
originally developed. (6). Exercise may be generally recognized
as important for maintaining fitness and
a) Raise awareness in the general popula-
strength, but its importance in maintaining
tion of a number of interventions that could
good balance and function needs to be bet-
improve balance and prevent falls.
ter publicized. It is likely that the approach
To make choices people need to have at will prove effective for both high and
least basic information about benefits of lower-risk populations (7). Although the
taking part in activities aimed at preven- effectiveness of less intensive interventions
tion. But information alone is not enough, at a population level is currently unknown
it needs to be framed so that it promotes it would seem likely that they will provide
realistic positive beliefs about the possibili- benefit. Exercises that improve strength
ties for preventive action if any change is and balance should be recommended for all
likely to follow. Many older people seem older people (7-9).
to assume that falls prevention consists of
Emphasis must be on the positive advan-
activity restriction or the use of aids and
tages of undertaking interventions such as
home modifications. Research suggests
balance and exercise training, rather than
that many older people are ignorant that
on reduction of risk of falls since the latter
fall risks can be reduced because there is
is generally viewed negatively and of little
a fatalistic acceptance of falling that may
relevance by many older people. Uptake
contribute to low uptake of falls prevention
may be encouraged by promoting greater
interventions.
awareness among older people, their
Campaigns need to raise general aware- families and health professionals of how
ness and should not be aimed only at older undertaking specific physical activities may
people. The opinions of others, including contribute to improving balance and reduc-
health professionals and family, influence ing falls risk.
older people’s decisions.
PAGE 21b) When offering or publicizing interventions, Uptake of falls prevention interventions
promote benefits that fit with a positive self- may be enhanced by emphasizing the
identity. positive benefits that are likely to accord
with desirable self images for older people,
It seems that many older people do not
in addition to those that reduce fall risks.
acknowledge falls, for example because of
Examples of such benefits include increased
fear of:
independence, greater confidence, ability to
• negative stereotyping; take an active part in society and support
younger generations.
• beliefs that falls are an inevitable and
unavoidable consequence of ageing; and c) Utilize a variety of forms of social encour-
agement to engage older people
• embarrassment about loss of control.
Uptake may be encouraged by the use of
Falls prevention advice is often perceived as personal invitations to participate (from
being for other ‘disabled or elderly people’. a health professional or other authority
Programmes that are perceived to impact figures) and positive media images and
negatively on self-image are likely to be peer role models to illustrate the social ac-
unattractive while those, which are viewed ceptability, safety and multiple benefits of
as improving skills or characteristics val- taking part. Uptake and adherence may be
ued by older people, are likely to be more encouraged by ongoing support from fam-
popular. In interviews older people say that ily, peers, professionals and social organiza-
they would participate in falls-prevention tions. A wide range of social influences are
initiatives to be proactive in managing their known to impact on health-related behav-
own health needs, maintain independence iour, including encouragement, approval
and improve confidence (4, 5). Older people and social support from health profession-
value strength and balance training activi- als and other sources (10). Role models
ties for their potential to: should provide examples of successful ac-
complishment of health-related goals (11).
• maintain functional capabilities and
Concern about social disapproval poses a
thus avoid disability and dependence;
barrier to undertaking physical activity,
• enhance general health, mobility and while social support, positive media images
appearance; and and real-life examples of ordinary older
people doing exercise can promote greater
• be interesting, enjoyable and sociable (4, 5).
physical activity (12-14).
These characteristics are all compatible
with a positive identity and should be en-
couraged.
PAGE 22You can also read