Whole Systems Meeting: Acute Care Pathway for Older People - The Principal Met Hotel, King Street, Leeds, LS1 2HQ
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Whole Systems Meeting: Acute Care Pathway for Older People The Principal Met Hotel, King Street, Leeds, LS1 2HQ 13th June 2018 www.england.nhs.uk

Welcome back
1.15 Welcome back & table discussions Dr Sara Humphrey
Suzanne Thornber, Service
Manager & James Harper, AHP
Rapid Intervention and Treatment Team in
2.00 Lead (Mental Health)
Lancashire Care
Lancashire Care NHS
Foundation Trust
The Early detection for delirium project (ED4D):
Implementing a quality improvement approach Dr Emma Vardy, Consultant
2.30
to the identification and management of Geriatrician, Salford Hospital
delirium at Salford Royal Hospital
3.00 Table discussions (coffee available)
3.45 Summary of the day Dr Sara Humphrey
4.00 CLOSE
• Please do stay until the end if you can
• For those who must leave early, please complete a **lilac**
evaluation form and leave on your table before you go
www.england.nhs.uk
Table Discussion
‘What can we do better’
• How can we best support people with Behavioural and
Psychological Symptoms of Dementia (BPSD) in an acute
setting, care home or in the community?
• How can we best support people with dementia when they
visit Hospital/A+E (appropriate adjustments, screening, 3
D’s, appropriate and timely discharge)
• What can we do to support family carers and enable their
involvement when they come into the acute hospital
setting?
• How can we prevent re-admission through improved
discharge & advance care planning?
• How can we prevent unnecessary hospital admissions?
www.england.nhs.uk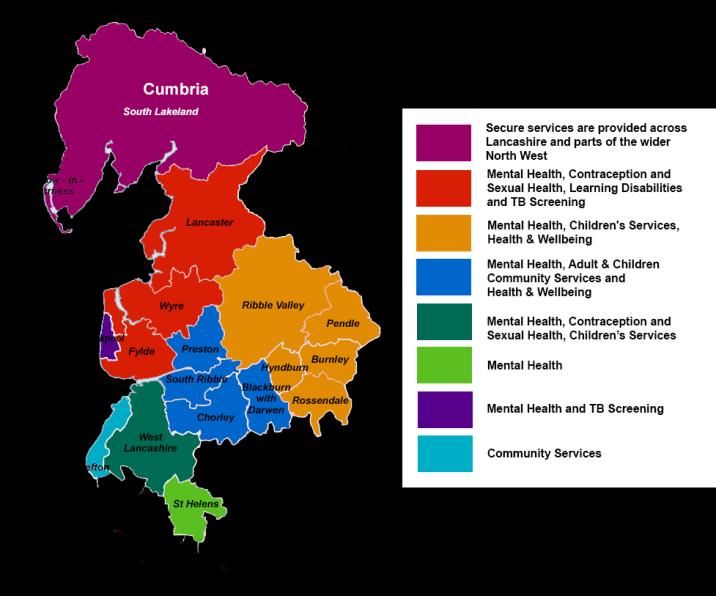
Rapid Intervention & Treatment Teams LCFT

Where we were-case for change • Large Geographical Area • 8 CCGS • 3 Local Authorities • 4 Acute Trusts • OA Bed closures in line with national strategy

• Variation across Community Mental Health Teams (CMHT) in a number of performance and productivity parameters, rates of referral, cost of contacts per team, and number of contacts per whole time equivalent. Variation in productivity within the teams Complicated patient pathways with numerous hand off and risks • Inequity of service • Inconsistent triage and initial assessment through locality based Single Point of Access

What we aimed to do • Promote faster recovery • Improved service –Providing a standardised approach across all areas with local variations • Support timely discharge from hospital • Prevent avoidable deterioration • Offer of a real alternative to hospital admission • Increase unscheduled care response, recognising the rise in referrals of people in crisis in care homes • Avoid inappropriate admissions to care homes • 8am -8pm, 7 days a week, 365 days a year

Benefits • To provide care across a whole pathway in a seamless, integrated manner • To deliver the best possible standard of care for service users and their families and carers • To ensure services are safe and effective in delivering defined outcomes • To enable the delivery of productivity and efficiency gains • To deliver within a smaller cost envelope • To deliver equitable care across Lancashire • To provide a career structure for the workforce

Staffing • Financed from existing envelope • Tasked with making cost efficiencies • Consolidation of smaller teams that had become unsustainable • 4 larger locality teams- flexibility to respond to patient need, whilst enabling 7 day service

Who is in the team-MDT Approach • Nurses • Occupational Therapists • Psychologists • Consultant Psychiatrists • Assistant Practitioners • Health Care Support Workers
A Patients Story
• Key Points:
- Patient choice in treatment
- Least restrictive options explored and implemented
- Carer’s assessment and support included in care plan
- Consideration of patient goals and role of team from
outset- and acknowledgement of changing goals throughout
involvement
- Team based approach, with timely and considered access
to wider MDT- OT and psychology, as well as nursing and
medication
- Patient and carer involvement in discharge care planningSalford Royal NHS Foundation Trust
Delirium and Dementia Project
Dr Emma Vardy
Clinical dementia lead Salford Care Organisation and
Greater Manchester &Eastern Cheshire Strategic
Clinical NetworkGDE : Delirium and Dementia • Increase detection of delirium • Enhance detection of undiagnosed dementia cases • Provide tailored care and improve outcomes. Clinically led IM&T led Exec Committee Risk assurance
Why is it important? Delirium is poorly detected Detection improves care & outcomes • Delirium is about 30% preventable • Early detection benefits patients and carers • Type of acute brain failure • Similar biomarkers to traumatic brain injury
How common? Delirium affects 1 in 8 acute hospital inpatients Up to 30% Emergency Department patients • 15% of adult acute general patients • 30% of acute geriatrics patients • 10-50% of surgical patients • 50% of Intensive Care patients • 50% of patients post hip fracture surgery
TAKES 1-2 MINUTES Specificity=84% Sensitivity=90%
Making the case for change
Delirium is distressing for patients, family and staff and has
potentially life-threatening outcomes including:
• Higher risk of falls & other harms
• 3 fold higher mortality (1 in 5 dead in one month, currently 14.1%,
MI and sepsis)
• More likely to get dementia
• Speeds up decline in dementia (doubles rate)
• More likely to go into care
• 2-3 fold increased length of hospital stay
• High readmission rate (approx 25%)
If delirium is missed in ED,
outcomes are much poorer
for patientsMeasurable outcomes identified by
the Delirium and Dementia project
Improved quality of care by increased % of over 65s
receiving an ED clinical assessment also receiving a Reduction in in-patient falls (for those patients with
4AT assessment delirium)
Improved quality of care by an increased % of over Reduction in average length of stay for patients with
65s receiving a 4AT assessment on admission to delirium recorded as i) a health issue ii) a diagnosis
hospital
Reduction in readmissions within a month of
Consistent adherence to comprehensive dementia
discharge for patients with delirium recorded as i) a
FAIR assessment process
health issue ii) a diagnosis (approx 25%)
Increased dementia diagnostic rates for over 65s,
Reduced prescription rate of anti-psychotic
leading to earlier treatment enabling prolonged
medication (in delirium)
independence and delay in institutionalisation
Improved mortality for patients diagnosed with
delirium (currently 14.3%)Early Detection for Delirium
(ED4D)Primary Driver Diagram
Liaising w ith clinicians to test
user friendliness of the
4AT Screening Tool document
Technology
Evidence based -choice of
delirium assessment and
Digital pathw ay for care bundle management tool
Incorporate patient stories
collection in carers training
Screening 65% Collect patient stories
of 65+
admissions from Training sessions planned for
the A&E various healthcare professional
department for groups
delirium by Raised aw areness and
Improve training and education mandatory training
March 2018.
Data collection on number of
falls, specials, and use of anti
psychotic medication for patients
Carer education w ho have received a delirium
screen and those w ho have not
Develop cohort of delirium Identify and train ED champions,
Leadership
champions include carersPDSA summary
Improve Training
Technology and Education Leadership
- Medical student project to
- sent email to ED staff find out understanding of - Delirium champions
and introduced 4AT into 4AT and delirium group
safety huddle 14/6 - one minute wonder - Leaders forum
posters in staff room and
- GDE EPR changes by blood gas machine - ED consultants updated
implemented 19/9 - lessons in the loo posters on progress
on the inside of bathroom
- Raise doors - ‘Well done’ poster and
awareness/introduce - Introduce delirium into ED feedback to ED staff
GDE program on the safety huddle
intranet for staff to see - Delirium resource box in
ED
- Add info about Delirium - Arrange teaching
in the Siren e-newsletter sessions for staff
- GDE educational video – EAU Consultants
development with – Junior doctors
– Nursing staff
delirium focus
- Daily walk around ED
- New doctors induction
- Presented at the team
briefUpdate • 17/22 confident in diagnosing delirium • 12/22 would use 4AT • 17/22 knew to use tools from EPR • 2 people knew to screen >65, 15 only if confused • 11/22 said delirium had been promoted • Major improvement in knowledge of tool, still some preconceptions to work on!
12/10/17
Training session for Junior
14/06/17
Doctors
Delirium
discussion added
07/12/17
to Safety Huddle
in ED New doctors induction
07/09/17
Siren newsletter
containing delirium
info was emailed out
and uploaded on the
intranet
01/04/18
Doctors changeover
19/09/17: EPR changes as part of GDE Programme went live300 No. of Patients Diagnosed With Delirium
EPR Changes
250
200
150
100
50
0
February
March
July
June
September
May
January
April
October
December
November
August
2017 2017 2017 2017 2017 2017 2017 2017 2017 2018 2018 2018Measure Baseline Dec 17 March 18
(1/10/16-3/3/17)
% 4AT in ED 8.1 33 41
% delirium who 18.3 23 14
had a fall
Mortality rate (%) 14.3 17.4 14.3
Readmission 19.5 15.1 14.3
within a month
(%)
LOS (days) 21.6 17.2 21.2National Recognition • “icanpreventdelirium” Quality Improvement Award • Shortlisted for Quality Improvement Initiative of the Year HSJ Patient Safety Awards • Contacted by other organisations across the country and are interested in using something similar in their departments.
Film Production Follow these links to watch the videos Delirium awareness = https://youtu.be/mDogR9A92cw Enid's Story = https://youtu.be/y2aXI9KVh-k
What next? • Delirium screening in ED - ongoing education • TIME management bundle • Spread screening to Emergency Assessment Unit • Improve assessment across the whole hospital • Development of a blue-printing template with GDE partners • Spread into community including NWAS • GM delirium collaboration • Ongoing QI project dementia FAIR assessment
Summary • Used QI methodology • Developed bespoke electronic documents with EPR team • Engagement at all levels • Culture change around delirium at Salford Royal NHS Foundation Trust and beyond
Acknowledgements
GDE project team ED4D team
• Umang Grover
• Shelley Heywood • Niamh Collins
• Matieusz Labiak • Beverley Thompson
• Karen Hill • Louise Nutt
• Lesley Wintle • Sarah Monks
• Yvonne Reay • Rebecca Thompson
• Sarah Hulme • Tony Holmes
• Lisa Hodgson • Chen Ng
• Lisa Orme • Alex Bagnall
• Robert Dodd • Fraser Brooks
• Nathy Connolly • Suzanne Masterman
• Jenny Wilson • Georgia Clarke
• Mike Turner • Elaine Inglesby-Burke (Executive Sponsor)
• Gareth Thomas (Group Chief Clinical
Information Officer)
Collaborators
• Scottish Delirium Association
• Karen Goudie (Health Improvement Scotland)
• Yvonne Moulds, Julie Mardon (Crosshouse
hospital)
• Haelo and Maxine PowerThank you emma.vardy@srft.nhs.uk
You can also read