WORKING PAPER DIRK ENGELS AND CHRISTIAN FRANZ - INTEGRATING NTDS: OVERLAPPING THEMES AND PROJECTS IN THE GERMAN DEVELOPMENT COOPERATION PORTFOLIO ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

WORKING PAPER DIRK ENGELS AND CHRISTIAN FRANZ INTEGRATING NTDS: OVERLAPPING THEMES AND PROJECTS IN THE GERMAN DEVELOPMENT COOPERATION PORTFOLIO on behalf of the German Network against Neglected Tropical Diseases (DNTDs)

The German Network against Neglected Tropical Diseases (DNTDs) e. V. is a national platform that cooperates with international partners to fight more strongly against poverty-related and neglected infectious diseases (NTDs, Neglected Tropical Diseases). The German network is committed to the London Declaration on NTDs, and aims to support the World Health Organisation (WHO) as well as programs in the affected countries in controlling, eliminating or eradicating at least ten of the altogether 20 NTDs by the end of the decade. Imprint Oktober 2018 Publisher: German Network against Neglected Tropical Diseases (DNTDs) www.dntds.de We thank all our discussion partners who took part in the study. Layout: www.zumweissenroessl.de Cover photo: Riccardo Lennart Niels Mayer – getty
OUTLINE
1 Abstract .........................................5 4 Overlap of NTD-programs and
selected projects funded by
Germany ......................................23
2 Introduction ..................................6 4.1 Co-morbidity between HIV and schistosomiasis .... 23
2.1 Diseases of neglect and progress 4.2 WASH and NTD-projects .................................... 26
in combatting them ...........................................6
4.3 Nutrition and NTD-projects.................................. 29
2.2 NTDs in the Global Health Transition
towards 2030 ....................................................8 4.4 German support of an NTD-program in the
CEMAC-region................................................... 31
2.3 About the working paper .....................................9
5 Health systems strengthening,
3 Mapping the assets of NTD
NTDs & prioritization of the most
interventions ................................10
vulnerable ...................................34
3.1 Operational assets for cross-sectorial projects....... 10
3.2 Strategic assets that can help in policy-making..... 20
6 Way forward .................................36
7 Abbreviations................................................... 37
8 References and Endnotes ................................... 38
Integrating NTDs 31
4 Integrating NTDsABSTRACT
FOREWORD
Neglected Tropical Diseases (NTDs) development, and the bridges that can portfolio. These case studies can serve
are intimately related to poverty and be built between so-called vertical as support for future analyses helping
poor living conditions. Often the dis- and horizontal health programs, i.e. to build integrated development pro-
abling consequences of NTDs become programs that address single diseases jects that embed the cross-sectorial
apparent and are unrecognised in vs. those that address health systems and pro-poor focus of the sustainable
other health areas (co-morbidities). as a whole. For that purpose, the au- development goals (SDGs).
Yet, those consequences are largely thors identify and outline operation-
preventable by large scale treatment al and strategic ‘assets’ of programs
Berlin, October 2018
starting early in life, as well as by against neglected tropical diseases
some of the most basic development (NTDs), i.e. processes, platforms, and
infrastructure and interventions. characteristics of NTDs and the respec-
tive projects.
The occurrence of NTDs, as a tracer
of poverty and inequity, provides an By integrating NTD programs and NTD
opportunity to monitor the capacity program components into other health
of health systems to achieve Uni- programs and cross-sectoral programs
versal Health Coverage (UHC) and (e.g. WASH (water, sanitation and hy-
implement large-scale preventive ac- giene) and nutrition) these assets can
tion to eliminate disabling infectious be put to work for a more effective
diseases in populations that are left and/or efficient achievement of com-
furthest behind. This working paper mon goals between formerly separate
aims at exploring the integration of programs. The authors illustrate those
NTD interventions in primary health assets by analysing selected ongoing
care health services and multi-sectoral projects in the German development
Integrating NTDs 52 INTRODUCTION
2.1 Diseases of neglect and progress in combatting them
Since the beginning of the current diseases – after HIV/AIDS, TB, and Lived with Disability (YLD), unlike the
millennium, Neglected Tropical Dis- malaria.3 Years of Life Lost (YLL), remains three
eases (NTDs) have emerged as a times as high as for priority commu-
group of poverty-related diseases of Yet, even though a few NTDs cause nicable diseases such as malaria.4
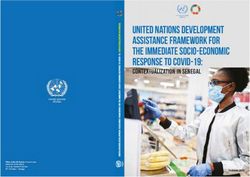
global significance in the interna- high mortality (see figure 1 page 7)
tional health and development agen- most of them cause important chron- Thus, NTDs are disabling diseases that
da. NTDs occur predominantly in trop- ic morbidity, e.g. through permanent represent medical poverty traps that
ical or sub-tropical environments. disablement. As a result, the current affect more than 1.5 billion people
They were previously looked at in residual burden in terms of Years globally in more than 100 countries,
isolation as high-burden (but rather
localized) health problems of which
the public health relevance was rap-
idly diluted when priorities needed to Table 1: Prevalence of NTDs and changes since the beginning of
be set at national, regional or glob- the 1990’s
al level. This neglects that there are
more than two billion prevalent cases
Disease Prevalent cases Change since 1990
of NTDs worldwide – with intestinal
(millions), 2013 (in %)
worm infections representing about
75 percent of all NTD-infections (see Ascariasis 804.4 -25.50
table 1 below).1 At the turn of the Trichuriasis 477.4 -11.60
21st Century, their collective burden Hookworm 471.8 -5.10
of disease, calculated as DALYs, was
Schistosomiasis 290.6 30.90
Tuberculosis (TB).2 Even though there
has been major progress in the fight Trematodes 80.2 51.10
against Neglected Tropical Diseases Dengue* 58.4 610.90
over the last 15 years, their numbers
Lymphatic filariasis 43.9 -32.10
continue to remain impressive. This
burden is represented in the concept Onchocerciasis 17 -31.20
of DALYs (Disability Adjusted Life Chagas disease 9.4 22.40
Years) which accounts for premature Other NTDs 68.74
deaths due to those diseases as well
as their debilitating and disabling
effects. According to this indicator * Represent incident cases in 2013 rather than prevalent cases.
Source: Herricks, J. R., Hotez, P. J. et al (2017). The global burden of disease study 2013: What
NTDs still account for the fourth larg- does it mean for the NTDs? PLOS Neglected Tropical Diseases, 11(8), e0005424. Original data:
est burden of disease from infectious Global Burden of Disease 2013.
6 Integrating NTDsFigure 1: Disease burden by mortality (YLL) and morbidity (YLDs)
Malaria
NTDs
CHAPTER 2
Trachoma
Onchocerciasis
Lymphatic filariasis
Hookworm disease
Trichuriasis
Leprosy
Ascariasis
Schistosomiasis
Chagas disease
Leishmaniasis
Dengue
Trypanosomiasis
Rabies
% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
YLDs YLL
Note: The numbers of leprosy were inverted in the original dataset.
Source: Fitzpatrick C et al. (2017). An Investment Case for Ending Neglected Tropical Diseases. In: Disease Control Priorities (third edition):
Volume 6, chapter 16. Underlying data: WHO, 2012.
primarily the poorest sections of pop- Deutsche Gesellschaft für Technische tion in the global public health agen-
ulations in the developing world. Zusammenarbeit (GTZ) GmbH, German da, large scale donations of medi-
NTDs can be considered as an indi- ministries, the World Health Organi- cines by the pharmaceutical sector,
cator of poverty, neglect, poor living zation (WHO) and partners.8 These enhanced R&D mostly by public-
conditions, lack of access to health workshops have led to the definition private Product Development Partner-
services, and ensuing consequenc- of a comprehensive strategy to com- ships (PDPs), financial engagement
es such as malnutrition, inability to bat a group of very diverse diseases,9 by international donors such as the
make a living, stigma and exclusion.5 in turn leading to a global program- US, UK and the Bill and Melinda Gates
As such they affect not just the Sus- matic response to what is currently Foundation, and commitment by af-
tainable Development Goal (SDG) 3 known under the umbrella term ‘Ne- fected countries and a large network
(health), but also poverty reduction glected Tropical Diseases’ (NTDs). of global health actors and develop-
(SDG 1), fight against hunger (SDG2), ment partners. More recently, Germa-
education (SDG4), gender equality This type of global programmatic re- ny has started to play an increasingly
(SDG5), clean water and sanitation sponse, often referred to as “verti- important role in the support of R&D
(SDG6), sustainable cities (SDG11), cal” like the one adopted for HIV/ for neglected and poverty-related
and climate action (SDG13).6,7 AIDS, tuberculosis, malaria, and Na- diseases, too. The focus on individual
tional Immunization Days (NIDs) as diseases has also allowed substantial
The current approach to combat- well as polio eradication, has ena- progress in controlling NTDs in are-
ting tropical diseases has originat- bled the mobilisation of unprece- as where poverty prevails, and health
ed from a series of workshops in Ber- dented resources for the fight against care infrastructure is usually weakly
lin in 2003 and 2005, with the then NTDs. These include increased atten- developed. The World Health Organ-
Integrating NTDs 7ization has played an important role volunteers for intervention delivery, eases. For example, political commit-
in mainstreaming this comprehensive providing a new impulse to the well- ment is visible not only on a national
strategic approach, as well as in mo- known primary health care concept of level (14 priority countries in sub-Sa-
bilizing increased resources and co- community-based outreach. In 2016, haran Africa have now national work
ordinating action among very diverse more than 1 billion people, equalling plans for NTDs that are annually up-
partners. 62.3 percent estimated to be a risk dated)12 and on a regional level (the
globally, benefitted from this inter- African Leaders Malaria Alliance – AL-
Progress in intervention delivery has vention.10 MA – embedded NTDs as indicators to
been most visible for large scale pre- be reviewed biannually by heads of
ventive treatment, one of the strate- Substantial progress has also been states alongside with other infectious
gies to combat NTDs whereby entire made with improving treatments disease indicators).13
populations or high-risk groups (such and control tools for complex NTDs,
as school age children or women of adapting their use to resource-poor
childbearing age) are treated with areas and as such providing access in
single-dose medicines* at a frequen- remote areas to prevention, early di-
cy determined by the endemicity lev- agnosis and prompt treatment for dis-
el. As the medicines are safe and no eases such as African sleeping sick-
individual diagnosis is required, the ness, Buruli ulcer, Chagas disease,
intervention is easy to deliver and leprosy, rabies, and visceral leishma-
guarantees in principle that all in- niasis.11 This progress is a direct con-
fected people could be reached. Suc- sequence of the renewed ambition of
cess has largely been determined by endemic countries to organize an in-
the engagement of community-based tensified management of those dis-
2.2 NTDs in the Global Health Transition towards 2030
The adoption of the Sustainable De- Moreover, the goal of “ending the ep- of most NTDs, to an extent that na-
velopment Goals (SDGs) in 2015 has idemics of AIDS, TB, malaria and ne- tional systems and services will be
introduced a paradigm shift for global glected tropical diseases” by 2030 (SDG able to deal with the residual burden
health programs. At the core of this Goal #3, target 3.3) calls for stepping as part of their routine services. While
shift lies the principle of Univer- up preventive measures. For NTDs this continuing to further expand cover-
sal Health Coverage: the provision relates to addressing their underlying age with quality care and preventive
of health services when and where socio-economic determinants – pover- treatment services, this will require a
people need them, without facing ty, inadequate sanitation, proximity to strong focus on mainstreaming NTD
financial hardship (SDG Goal #3, tar- domestic animals, livestock and infec- interventions into national health
get 3.8). It shifts the emphasis from tious vectors of disease – and acting systems and developing collaboration
global health priorities to all-inclu- jointly with other sectors and devel- with other sectors.
sive health care tailored to local situ- opment programs. Such integrated ac-
ations and communities. At the same tion across sectors will need involve-
time, the principle of “leaving no one ment of a multitude of actors, ranging
behind” calls for special attention to from education, water and sanitation,
ensuring equitable access to care for agriculture and animal husbandry, to
the specific health problems of the environment, housing, and rural and
poorest, such as NTDs. This goes hand urban development.
in hand with the need to enhance in-
tegration of NTD interventions into Meeting the specific NTD indicators to
national health systems and peripher- achieve SDG Goal #3 will logically lead * Mostly donated by the pharmaceutical in-
al health care. to elimination or near-elimination dustry
8 Integrating NTDs2.3 About this working paper
Against this background, this working the ‘not-knowing’ of the potential op- The disabling consequences of NTDs –
paper aims at understanding the po- erational benefits of integrated pro- most of which become visible in oth-
tential of integrating NTD-programs grams in achieving individual goals. er health areas (co-morbidities) – are
CHAPTER 2
with other health programs and/or Second, the structure of development preventable by large scale treatment
programs in other relevant sectors. cooperation is usually not designed starting early in life, as well as by
We identify processes, platforms, and for cross-sectorial cooperation. Units some of the most basic development
characteristics of NTDs and their pro- within governments, implementing infrastructure and interventions. We
grams that could be utilized more gen- NGOs, and advocacy have – often hope that this working paper can
erally (for which we will use the term with good reason – emphasised expert contribute to the discussion about
‘assets’). knowledge in a specific area. Moreo- potential synergies between develop-
ver, cross-sectorial projects raise con- ment programs. NTDs are just one –
Two motivations have been most cru- cerns about budget allocations within but as we outline an important angle
cial for this analysis: First, the global organizations. Structurally, the fight to look at multisectoral collaboration
health community still struggles to between ‘value for money’ and ‘long- and implementation.
find concrete pathways for synchro- term sustainability’ has made the di-
nizing efforts to achieve UHC (e.g. viding lines even more pronounced, as
through health systems strengthen- monitoring and showing evidence for
ing) and efforts to fight major debil- cross-sectorial or long-term projects’
itating or killing diseases. We believe effectiveness is deemed to be much
that part of the explanation lies in more difficult than for narrow projects.
Integrating NTDs 93 MAPPING THE ASSETS
OF NTD INTERVENTIONS
After more than a decade of steady
progress, in big part due to a strong Box 1
global programmatic focus that has
helped to enhance access to essential The Merck praziquantel donation program can supply up to 250 million
NTD medicines and to rationalize case tablets per year for the treatment of schistosomiasis in school-age chil-
management of complex NTDs, there dren in sub-Saharan Africa. This potential quantity is currently not com-
needs to be a strong focus on mak- pletely used. The praziquantel needs are currently based on the estima-
ing NTD interventions part of national tion of school-age populations in districts confirmed to be endemic by
health services. Even though interven- a regional mapping exercise. As schistosomiasis is a very focal disease,
tion delivery has always involved na- building district level capacity for decision analysis and monitoring would
tional and peripheral health services, enable to tailor the needs to the sub-district endemicity, optimize the use
health systems capacity for monitor- of praziquantel and enable to cover more children in real need in Africa.
ing, evaluation and deciding on local Merck KGaA is currently working on a new formulation of praziquantel that
intervention strategies merits to be can be administered to young children – the current tablets being only
enhanced. This is expected to lead to suitable for children older than six.
a better integration into already ongo-
ing (and funded) health programs and
optimization of resources by better
planning according to local data and tors can provide opportunities to en- projects that can be utilized by oth-
situations (illustration box 1). hance delivery of NTD interventions er sectors. Secondly, we wish to draw
in a very cost-effective manner, by attention to several ‘strategic assets’
Intervention delivery for NTDs can adding them on to already existing that describe more general aspects
provide assets to enhance delivery activities. The following sections will about the fight against NTDs and
of additional health care activities first outline ‘operational assets’, i.e. that can help policy makers to iden-
(or benefits) into remote communi- processes, platforms, and charac- tify overlaps in the goals of different
ties. Inversely, health and other sec- teristics of NTDs and the respective sector strategies.
3.1 Operational assets for cross-sectorial projects
3.1.1 NTD assets for the NTDs on some non-communicable tosomiasis) disease has since long
diseases such as anaemia (hookworm been known (see a more comprehen-
Health Systems
and schistosomiasis), cardiac disease sive list in table 2).
(Chagas disease), cancer (urinary
3.1.1.1 Co-morbidities
schistosomiasis, opisthorchiasis and
Neglected Tropical Diseases cause clonorchiasis), and chronic liver (in-
important co-morbidities in other testinal schistosomiasis and echino-
health areas. The impact of some of coccosis) and kidney (urinary schis-
10 Integrating NTDsTable 2: NTDs as causes for chronic non-communicable diseases, 2008
Chronic Condition NTDs as Etiologies Approximate Number of Major Geographic
Cases of Each Infection Distribution
CHAPTER 3
Cardiovascular disease
Cardiomyopathy Chagas disease 8–9 million Latin America
Endomyocardial fibrosis Loiasis (and other 13 million sub-Saharan Africa
helminthiases)
Cancer
Bladder cancer; squamous cell Urinary schistosomiasis 119 million Africa
carcinoma (S. haematobium
infection)
Bile duct carcinoma Opisthorchiasis and 6–44 million Southeast Asia and China
clonorchiasis
Gastrointestinal and liver disease
Inflammatory bowel disease Trichuriasis 604 million Developing countries
Megacolon and megaesophagus Chagas disease 8-9 million Latin America
Intestinal and liver fibrosis Schistosomiasis 68 million Africa, Brazil,
(S. mansoni infection and and East Asia
S.japonicum infection
Liver cyst Amebiasis N/A India, Latin America
Echinococcosis N/A Developing countries
Chronic renal disease
Hydronephrosis and renal failure Urinary schistosomiasis 119 million Africa
Blood dyscrasias
Anemia Hookworm infection 576 million Developing countries
Schistosomiasis 207 million Developing countries
Pancytopenia Leishmaniasis 12 million India, Africa, Brazil
Chronic respiratory conditions
Hemoptysis Paragonimiasis 21 million East Asia
Asthma Ascariasis 807 million Developing countries
Toxocariasis ND Worldwide
Note: Inconsistencies in the cases for per infection (column 3) and table 1 are due to different observations in time. We decided to report the
original figures reported in the source. See more information on the data in the original source: Hotez, P. J., & Daar, A. S. (2008). The CNCDs and
the NTDs: Blurring the lines dividing non-communicable and communicable chronic diseases. PLoS Neglected Tropical Diseases, 2(10), 1–3. https://
doi.org/10.1371/journal.pntd.0000312.
Integrating NTDs 11Table 3: Health threats to women resulting from neglected tropical diseases
Health Condition Neglected Tropical Disease
Sexually Transmitted Infections
HIV/AIDS Urogenital schistosomiasis
Trichomoniasis Trichomoniasis
Social Exclusion and Stigma
Limb, breast, skin, and genital deformities Lymphatic filariasis, Buruli ulcer, Onchocerca skin
disease, leprosy, leishmaniasis
Facial disfigurement Leishmaniasis, leprosy
Reproductive Health
Infertility Urogenital schistosomiasis, hookworm
Severe anaemia of pregnancy/lactation and Hookworm (major), schistosomiasis (minor)
high maternal morbidity and mortality
Anaemia associated with menstruation and Hookworm
amenorrhea
Congenital infection Chagas disease, leishmaniasis, strongyloidiasis,
hookworm
Low birthweight and/or premature birth from Hookworm and other soil-transmitted helminth
placental inflammation and maternal anaemia infections, schistosomiasis
Exacerbation of disease during pregnancy Leprosy, schistosomiasis
Source: Hotez, P. J. (2009). Empowering Women and Improving Female Reproductive Health through Control of Neglected Tropical Diseases, 3(11),
e559. Original evidence see publication. Translation by the authors.
But not only are NTDs important it because of biological reasons or for a great mutual programmatic im-
causes for non-communicable diseas- because of social and cultural norms/ pact for other areas.
es that affect hundreds of millions of role models.
people. Those parasitic, bacterial,
and viral diseases are also adverse- In the following sections we will an- HIV/AIDS and NTDs
ly affecting reproductive health of alyse in further detail some of these
women, increasing the likelihood of co-morbidities that represent not only The relationship between NTDs and
sexually transmitted diseases, and a considerable burden of disease, but HIV/AIDS – as schematically repre-
lead to social stigma and exclusion. also offer some striking overlaps in sented in figure 2 – is an interesting
Table 3 gives an overview of the intervention programs. These overlaps one as it runs in both directions: On
co-morbidities of NTDs and condi- represent a vast and increasing range the one hand side, people who have
tions in these three areas. In most of opportunities where NTD interven- HIV/AIDS are known to develop more
of these co-morbidities women and tions can relieve morbidity in other often the parasitic NTDs Chagas dis-
girls are clearly disadvantaged – be health areas and have the potential ease and Visceral leishmaniasis (VL).
12 Integrating NTDsFigure 2: Pathogenesis: The bi-directional relationship between NTDs and HIV/AIDS
Increases viral loads
NTDs
Intestinal helminths Decreases CD4 counts
CHAPTER 3
Schistosomiasis Causes anemia
Lymphatic filarisis Increases horizontal transfer
Increases mother-child transmission
HIV/AIDS
NTDs (opportunistic Increases pathogen
infections) reproduction
Chagas disease Increases
Visceral leishmaniasis immunosuppression
Source: Adapted from Noblick, J., Skolnik, R., & Hotez, P. J. (2011). Linking global hiv/aids treatments with national programs for the control and
elimination of the neglected tropical diseases. PLoS Neglected Tropical Diseases, 5(7), 1–4. Translated by the authors.
HIV/AIDS is not only leading to an FGS below). Helminth co-infection illustrates schematically how differ-
increased reproduction of living path- is associated with increased risk for ent programs directed at population
ogens in the body, but also increases mother-to-child-transmission (MCTC) groups could work together. For ex-
the immunosuppression. Especially of HIV, possibly by a mechanism in ample, clinics that provide treatment
VL has emerged as an important op- which parasite antigens activates against HIV/AIDS as well as TB and
portunistic infection associated with lymphocytes in utero.15 A recent pro- other co-infection could be stacked
HIV. In areas endemic for VL, many spective study in Tanzania has even with NTD-medications based on re-
people have asymptomatic infections. documented a significantly increased gional NTD-prevalence. Vice versa,
A concomitant HIV infection increas- risk of acquiring HIV for lymphatic fil- NTD-programs that reach into the
es the risk of developing active VL by ariasis-infected individuals.16 most rural and remote areas could
between 100 and 2320 times.14 The provide expanded HIV testing and
two diseases are mutually reinforcing: Similar relationships between other care. Thus the programs could help
HIV-infected people are particularly NTDs, HIV and other viral co-infec- decreasing HIV unawareness in these
vulnerable to VL, while VL accelerates tions such as hepatitis may exist. areas. Another example builds on the
HIV replication and progression to As an example, recent evidence has community health worker programs
AIDS. been brought up that HIV or hepa- within HIV/AIDS programs (e.g. of
titis (B and C) co-infections may be PEPFAR) to reach vulnerable and or-
On the other hand, some NTDs are associated with many unfavourable phan children. Given the ease of
likely to increase the likelihood of outcomes in leprosy patients, from a treatment of many NTDs with medi-
either transmission and/or devel- higher number of inflammatory com- cines, these community health work-
opment of HIV/AIDS. For example, plications and nerve damage to an in- ers can be trained to spot and treat
an intestinal helminths infection creased relapse rate.17 possible NTD-coinfections with HIV/
can reduce the CD4-count and/or AIDS or refer them to a nearby health
increase the viral load and can also These links between HIV/AIDS and centre. This integration would help
cause anaemia. Suffering from schis- different NTDs call for a closer look alleviate a major weakness of school-
tosomiasis infection increases the at the respective intervention pro- based programs that often unable
likelihood of horizontal transmission grams and whether there are/should to reach those children who stay (or
between individuals (see section on be an integrated approach. Figure 3 have to stay) at home.18
Integrating NTDs 13Figure 3: Operative links for integrated control of NTDs and HIV/AIDS
NTD HIV/AIDS
Control Control
School and community-
based drug distribution Treatment Clinics, Community
Children Health Workers outreach to
Orphan and Vulnerable Children
Scale up of
Mass Drug Antenatal Clinic and
community-based drug Anti-
Administra-
distribution Antenatal Clinics retroviral
tion through Pregnant
Women Therapy
Rapid Impact
Packages
Treatment Clinics
Comminuty based drug
distribution Community Health Workers
Non-pregnant outreach in the home-based
adults care setting
Source: Noblick, J., Skolnik, R., & Hotez, P. J. (2011). Linking global hiv/aids treatments with national programs for the control and elimination of
the neglected tropical diseases. PLoS Neglected Tropical Diseases, 5(7), 1–4. Translated by the authors.
HIV/AIDS and Female entifically document a causal asso- as the researcher Peter Hotez put it
Genital Schistosomiasis ciation,28,29,30,31 to the extent that 2013 – “possibly […] one of the most
WHO produced a visual pocket atlas common gynaecologic condition in
(FGS) for clinical health care professionals sub-Saharan Africa”.35
Even though gynaecological schisto- to recognize FGS,32 and for WHO and
somiasis has long been known by cli- UNAIDS to issue a joint technical
nicians, and described in the medical document presenting state-of-the art
literature as early as the 1940s,19,20 it evidence for its association with HIV/
was in the early 1970s that the syn- AIDS and advocating for large scale
drome was described close to what to- prevention.33
day is known as FGS.21,22 The term Fe-
male Genital Schistosomiasis was first The need to consider FGS as a seri-
used in the mid-1990s,23 and suspect- ous threat to the health of women in
ed as a risk-factor for the transmission Africa stems from the terrible conse-
of HIV on the basis of epidemiologic, quences of the illness (see box 2) and
immunologic, and pathophysiologic the dramatic estimates that indicate
data.24,25 Even at that time the need up to 150 million women and girls in
for a specific gender perspective was sub-Saharan Africa could be affected
already highlighted,26 but one had to by FGS.34 The estimate is based on the
wait until 2006 before an association evidence that between one third and
between FGS and HIV was first alleged 75 percent of women and girls who
on the basis of field data.27 From there are infected by schistosomiasis also
it took over a decade to further sci- have FGS. This number makes it –
14 Integrating NTDsThe connection between FGS and an
HIV infection is based on three ob-
servations: First, cross-sectional stud- Box 2
ies in several African countries have
found that adult women with uro- “FGS causes lesions and scarring in the female genital and repro-
ductive tract. These lesions provide easy entry points for the HIV
CHAPTER 3
genital schistosomiasis had 3-4-fold
higher odds of having HIV. Second, virus and can triple women’s risk of contracting HIV/AIDS. Women
among adolescent girls with FGS a who have FGS also frequently have reproductive organ damage which
higher proportion of HIV receptors on can lead to sexual and reproductive health problems such as pain-
their genital tissue cells were found ful intercourse, infertility, ectopic pregnancy, spontaneous abortion,
compared with girls that did not have premature birth and low birth weight. Women and even young (and
FGS. Third, there is a striking geo- still sexually inactive) girls with FGS are often misdiagnosed with
graphical overlap between HIV inci- having a sexually transmitted infection (STI) which leads to stigma
dence and FGS prevalence.36 and discrimination; they often suffer from psychological problems
and depression.”
Those findings lend themselves to
the conclusion that preventing young In the ‘normal’ scenario of schistosomiasis, the parasites are
girls from getting infected with Schis- present in the small blood vessels in intestines and bladder. The
tosomiasis will help reducing HIV in- eggs that are produced continuously by the adult parasite try to
fections later in life. Women who have penetrate the inside of those organs. From there they exit the body
been treated against schistosomiasis through urine or stool. As the sanitary situation in many countries
with praziquantel at least once in their of sub-Sahara Africa is insufficient, open defecation – often next
life, have developed 50 percent less to a freshwater reservoir – remains quite common and the water
FGS later on in life.37 And treatment of is used as a means of cleaning. These freshwater resources then
schistosomiasis has been suggested to become the living environment for the intermediate snail host that
decrease the number of HIV infections gets infected with the larvae hatching from the schistosome eggs,
by up to 16-20 percent.38 and multiplies and transforms them into a new form of larvae that
can penetrate the human skin. Whenever humans then come in
These findings indicate that inte- touch with the water there is a risk that these larvae penetrate the
grating the treatment of populations skin and become new adult parasites.
at risk of FGS into the traditional
HIV-programs might prove to be not It is this aspect of the transmission cycle that makes women
only cost-efficient but might also much more vulnerable to schistosomiasis. They get water from the
help to target poor communities first. reservoirs, wash their children, and do their laundry. Moreover, for
Importantly, they address an impor- women it is not only intestines and bladder that are affected, but
tant gender bias in HIV infections by also genitals. Due to the specificities of the blood vessels in the
focussing on girls and young women. female pelvis eggs can penetrate into the uterus and the vagina.
Prevention of FGS, and therefore a de-
crease in risk of transmission of HIV/
AIDS, is indeed possible by regular
treatment with praziquantel,39 as long
as it is given early in life in order to
prevent chronic damage of the genital for NTDs could indeed be added to
tract that occurs already in adoles- the package of combined preventive
cent girls in areas where schistosomi- action in girls, adolescent girls and
asis prevails.40 Hence the suggestion, young women and constitute an in-
already in 2009, that large scale pre- novative way to contribute to the tar-
ventive treatment with praziquantel get of “accelerating HIV prevention to
in children could constitute “Africa’s reduce new infections by 75 percent”,
32 Cents Solution for HIV/AIDS”.41,42 as stated in the HIV Prevention 2020
Inexpensive, large scale treatment Road Map.43
Integrating NTDs 15Anaemia and NTDs
Box 3
Anaemia in low- and middle-income
countries is usually a result of mul-
tiple etiological factors – nutrition- UNAIDS’ HIV Prevention 2020 Road Map – ‘Accelerating HIV prevention
al, infectious and genetic. Regarding to reduce new infections by 75 percent’
infectious (and thus preventable)
causes of anaemia, hookworm infec- Despite a significant reduction in new infections over the last 15 years,
tion and schistosomiasis are among around 1,8 million new HIV infections still occur annually. Globally, ado-
the most widely encountered, to- lescent girls and young women (15-24 years), account for approximate-
gether with malaria and HIV/AIDS. ly 6,900 new HIV infections every week, and out of these 5,500 were
Childhood anaemia is therefore very among young women (15-24) in sub-Saharan Africa.
common in poor communities, further
amplified by poor nutritional status, As part of global efforts to end AIDS as a public health threat, UNAIDS,
and disproportionately affects wom- UNFPA and partners launched a roadmap to reduce new HIV infections by
en of child-bearing age later in life.46 75 percent. This road map intends to enhance country-led movements
Hence the recent reminder by WHO to scale up HIV prevention programs – combining primary prevention
that every girl and every woman has with the preventive effects of treatment – to meet global and national
the right to be regularly dewormed 47 targets to end AIDS as a public health threat by 2030. The Road Map
and that the fight against NTDs should is relevant for all low and middle-income countries but focuses on 25
be linked with gender programs. countries with the highest numbers of new infections in 2016, 18 of
which are in sub-Saharan Africa.*
Mental health and NTDs As part of the implementation of combined primary prevention packag-
es, UNAIDS has recently promoted the integration of reproductive health
The burden of mental health condi- interventions in order to leverage synergies and improve women’s lives.
tions are predicted to become one of As such, HPV vaccination to prevent cervical cancer and early schistoso-
the leading contributors to the global miasis treatment to prevent Female Genital Schistosomiasis,44,45,33 were
burden of diseases by 2030.48 Co-mor- recommended to be part of primary HIV prevention programs among
bidities between mental health and school age children and girls. Adolescent girls and young women should
NTDs are as old as these ancient dis- further have access to regular screening and early clinical care for both
eases themselves. One just needs to conditions as part of Sexual and Reproductive Health and Rights (SRHR)
think about the historical treatment of programs, such as HIV screening, family planning, and mother-and-child
leprosy (social exclusion) to see what health programs. In this way, combined innovative prevention programs
disfigurement can mean for people. are likely to have an enhanced and comprehensive impact, while sat-
isfying the specific public health needs of adolescent girls and young
There are different ways how NTDs women in the poorest settings.
can affect mental health: Some NTDs
directly affect the central nervous sys-
tem. Neurocysticercosis (caused by the
pork tapeworm) manifests itself most-
ly in the form of (late onset) epilepsy. However, the more common link be-
The same is true for onchocerciasis as- tween NTDs and mental health is
sociated epilepsy (OAE) or more com- through the cycle of depression,
monly called “Nodding Syndrome”. The stigma and discrimination, exclusion
clinical picture of second stage African from participating fully in society,
* Angola, Brazil, Cameroon, China, Côte d’Ivo-
trypanosomisis (sleeping sickness) lack of educational opportunities and ire, Democratic Republic of the Congo, Ethi-
includes psychiatric manifestations exclusion from income-generation opia, Ghana, India, Indonesia, Kenya, Leso-
and coma. And ectopic localisations and employment opportunities. This tho, Malawi, Mexico, Mozambique, Namibia,
Nigeria, Pakistan, South Africa, Swaziland,
of schistosomiasis eggs in the brain particularly affects NTDs that result
Uganda, Ukraine, United Republic of Tanza-
or spinal cord can cause epilepsy, and in infertility, such as schistosomiasis nia, Zambia and Zimbabwe. Bold = BMZ partner
hemi- or para-paresis or -paralysis. and hookworm, and in disability if countries with health priority.
16 Integrating NTDsTable 4: Estimated numbers of existing cases of selected NTDs
which cause stigma and disablement
Specific NTD Disabilities resulting Number of cases/yr or with
CHAPTER 2
from disease permanent chronic symptoms
Buruli ulcer Disfigurement 5000/yr
Cutaneous/mucocutaneous Disfigurement 1.5 million/yr
leishmaniasis
Onchocerciasis Blindness, severe itching 265 000 existing cases
Lymphatic filariasis Lymphoedema 15 million existing cases
Trachoma Trichiasis 8.2 million
Yaws Disfigurement 2.5 million (global prevalence
estimate 1995)
Leprosy Disfigurement 213 000/yr
African trypanosomiasis Neuropsychiatric disorders Circa 10 000 new cases/yr
Source: Litt, E., Baker, M. C., & Molyneux, D. (2012). Neglected tropical diseases and mental health: a perspective on comorbidity. Trends in Parasi-
tology, 28(5), 195–201.
untreated, such as buruli ulcer, cu- mass treatment with azithromycin for health system. As delivery is large-
taneous leishmaniasis, leprosy, lym- trachoma has shown a wide-ranging ly carried out by resident communi-
phatic filariasis, and onchocerciasis.49 impact on other illnesses. Recent ty-based volunteers, this platform can
Women and girls invariably suffer studies have established this positive be capitalized on to bring additional,
more from mental consequences and effect particularly when it comes to simple interventions to these commu-
disorders related to NTDs. child mortality. In 2009, a study of nities, to carry out screening for spe-
effects of anti-trachoma interventions cific health problems and to help with
Table 4 gives an overview of some in Ethiopia has shown that child mor- surveillance of emerging diseases. Em-
of the most important links between tality decreased in areas where mass powering communities to assist with
NTDs and their disabling effects. Giv- treatment for trachoma had been the delivery of a simple package of in-
en the fact that mental conditions are practised.50 This impact was further terventions will contribute to building
often kept hidden or are not made investigated in a cluster-randomized community resilience and achieving
a subject of discussion, an accurate trial in Niger, Malawi and Tanzania. UHC.
estimation of the global prevalence The result was that particularly chil-
is challenging. The case numbers in- dren in the age group of one to five
dicated in column three of table 4 months had the greatest effect from 3.1.1.3 NTD supply chains
nevertheless give an indication of the the treatment (in the order of 25 per- and health systems
extent of NTD-mental health co-mor- cent reduction in child mortality).51
bidities. Intervention delivery of NTDs is asso-
ciated with a massive, but well-func-
Child mortality and NTDs 3.1.1.2 Regular annual tioning logistics and supply chain sys-
community health contact tem on which the health system 52 can
NTD interventions delivered to remote build to improve this often-under-val-
communities that have limited access The periodic, community-based deliv- ued aspect of health systems strength-
to health services can also provide ery of NTD interventions provides at ening. The network of pharmaceutical
unexpected collateral health benefits. least one annual contact of remote firms, WHO, partner countries, and NG-
For example, the effects of preventive communities with the local/national DOs has scaled the supply chain from
Integrating NTDs 17more than 700 million tablets in the er example of improvement is the re- to those, supply chains requiring fre-
year 2009 to more than 1.5 billion duction in unreported or mis-reported quent re-supply of commodities – e.g
tablets in 2016 and 2017. This supply stockpiles of medicines in receiving essential medicines supply chains –
chain involves all steps from the first countries. A joint mission of WHO vis- follow usually different processes.55
mile (application for drug donations,* ited 6 priority countries in 2016 and Better collaboration among the cam-
production, shipment, and transport found around 180 million tablets sup- paigns could theoretically range from
to Central Medical Stores in the coun- plied to the country between 2012 and complete ‘managerial integration’ to
tries)53 to the last mile (distributing 2015, that had been unreported for. The ‘sharing infrastructure’. One of the
the necessary drugs to the communi- mission was able to find information central overlaps seems to be the dis-
ties and the respective places where on 73 percent of the unreported tab- tribution network and assets. For ex-
preventive medical treatment in at-risk lets. These missions show clearly that ample, one of the NTD control program
areas is delivered). the substantial amounts of unreported managers of the NTD control program
medicines are neither lost nor expired in Malawi has an agreement with the
Managing those supply chains has but reveal the information gaps in the Director of the Expanded Program on
proven to be a challenging task. Yet, Supply Chain Management of medicine Immunization (EPI) to borrow EPI
progress has been encouraging. For that exist in endemic countries** vehicles when they are not otherwise
example, in 2015 only 20 percent of being used – and in turn covers the
medicines for preventive chemotherapy In an analysis of NTD-supply chains, operating costs of the vehicles.56
were delivered on time, i.e. two months the largest potential was seen in syn-
before date for the preventive mass chronizing NTDs with bednet cam- While the previous example highlights
treatment in the country. By 2017, this paigns, nutrition campaigns, and options for collaboration for the last
share had reached 60 percent.54 Anoth- immunization campaigns. In contrast mile, there have been initiatives to
Figure 4: Presence of neglected tropical diseases
No NTDs
1-2
3-4
5-6
7-8
Sources: The Carter Center for Guinea
Worm Disease, STH, Trachoma,
Schistosomiasis, Onchocerciasis,
Lymphatic Filariasis. WHO for Chagas
disease, dengue fever and leishmaniasis.
Note: Years of last observations vary
between 2013 and 2016. Analysis and
illustration CPC Analaytics.
18 Integrating NTDsstreamline the first mile supply chain, ly visible only at a late stage and often And even, while the impact on growth,
too: A public-private consortium es- in other medical/health areas (see sec- nutrition, educational performance and
tablished the NTD Supply Chain Forum tion on co-morbidities above). Before worker productivity has been well de-
(NTDSCF) that created a dedicated that, they cause substantial hidden or scribed for soil-transmitted helminths
‘control tower’ that works to centralize ‘subtle’ morbidity, that seriously affect and schistosomiasis, the cumulative
CHAPTER 3
management and visibility in tracking children’s educational performance and burden of infection with multiple NTDs
orders and shipments. The NTDSCF col- adult productivity. Therefore, beyond has so far been poorly documented,60
laborates with the international logis- the health sector, NTD interventions and therefore the effect of controlling
tics company DHL, that also contrib- have the potential to enhance the im- multiple NTDs on human health, well-
utes to the effort in kind.57 pact of various initiatives such as food being and life course opportunities is
security and nutritional programs, an- likely to be much more significant.
ti-hunger campaigns, and social safety
initiatives to enhance educational im-
3.1.2 The underestimated 3.1.3 Poverty
pact and employment opportunities.
‘subtle’ burden of NTDs To underpin the latter, one could cite identification
and its broad, socio- the documentation of long term eco-
economic impact on life nomic consequences of the successful The geographical occurrence of NTDs,
eradication of hookworm disease from as a proxy for poverty and neglect, can
NTDs tend to cluster in the same poor the American South, which started direct local authorities to areas where
populations, who are affected by multi- circa 1910,58 as well as the long-run water supply, sanitation infrastructure
ple diseases as a rule rather than as an impacts of investments in school-based and environmental improvements are
exception. Many NTDs, become clinical- deworming in Kenya.59 most needed and will also have most
impact. This is true both in rural and
peri-urban areas. Because of ever in-
creasing urbanization and internation-
al travel, cities are indeed becoming
important hubs for the transmission
of infectious diseases,61 as shown by
recent vector-borne disease outbreaks.
* A country’s application for drugs involves
more than just ordering tablets, but also “in-
formation on disease burden, number of people
targeted for treatment, date of scheduled MDAs,
and mechanisms for distributing donated med-
icines. The applications also include strategies
for monitoring and evaluation, providing appro-
priate training and supervision to teachers and
health workers responsible for distributing med-
icine, and preventing reinfection (i.e., provision
of health education, water, and sanitation).”
** The mission identified three major reasons
for these discrepancies: a) information on the
amount of stocks of PC medicines available at
subnational and/or national level was obtain-
able at country level but was not accurately
reported to WHO; b) some of the treatments
delivered to individuals during MDA campaigns
were not reported to WHO; and c) information
communication gap between the programs han-
dling the PC-medicine supplies and NTD pro-
gram manager on the amount supplied, utilized
and available balance.
Integrating NTDs 193.1.4 Assets of Health laboratories),62 as well as strengthen- management of all the NTDs. In 2015,
ing health information systems, would WHO has launched a global strategy
Systems and other sectors
greatly help enhancing national di- to strengthen efforts on water, sani-
to support NTD programs agnostic and care capacities, as well tation and hygiene to accelerate pro-
as capacity for monitoring and evalu- gress against NTDs.63 This strategy
Preventive or promotional programs in ation, including of potential drug re- calls for closer coordination of WASH
the health or other sectors can be used sistance (e.g. AMR). and NTD programs, through joint plan-
to deliver NTD interventions. Examples ning, delivery and evaluation of pro-
of such programs – well-known, but Similarly, mainstreaming NTDs in grams, strengthening of evidence, and
still largely under-used – are school training and capacity strengthening making better use of endemicity data
health programs, immunization and initiatives of (public and private) to target WASH services to the most
mother-and-child health programs, as health workforce will greatly contrib- vulnerable, underserved populations.
well as promotional programs for ado- ute to building national implementa- Inversely, adding a (modest) NTD im-
lescents, such as in sexual and repro- tion capacities for NTDs. plementation component – including
ductive health. The logic can further be vector containment and control - to
extended to other sectors where there National initiatives in health finance much more substantial investments in
are opportunities to reach specific risk and governance can greatly contrib- water and sanitation infrastructure is
groups during their life course, such ute to achieving UHC without finan- a cost-effective way to expand NTD
as through professional groups and cial hardship, increasing the imple- interventions. Many WASH and NTD
cooperatives, agricultural support in- mentation capacity for NTDs and actors have started to work together
itiatives, nutritional programs, etc…) lessening the dependence on external on planning and implementation and
donor funding in the long term. have started to document their expe-
Making sure that NTD requirements are riences and lessons learnt.64
met in building, renovating and equip- Water, sanitation and hygiene (WASH)
ping health infrastructure (including are critical in the prevention and
3.2 Strategic assets that can help in policy-making
3.2.1 Poverty focus pact of river blindness control in Af- ance of suffering and disability,68 but
rica.67 Not only do people not become also in terms of return on investment
NTDs are intimately related to pov- blind or suffer from severe skin dis- in the long term, both for individ-
erty and keep on anchoring affected ease anymore, but they have been ual diseases 69,70,71 as for NTDs as a
people in poverty because of their able to return to cultivate the best whole.72,73 The level of cost-effective-
impact on education, performance, fertile land near rivers they had left ness of NTD interventions is driven,
productivity and earning a livelihood, because of fear of infection with the among other factors, by the commit-
as well as de facto out-of-the pock- parasitic disease. River blindness in- ment of pharmaceutical companies to
et expenses that are related to their vestments have thus made 25 million provide free medicines, the number of
treatment and care in most health hectares of arable land safe to culti- people affected and scale of potential
systems in the developing world.65,66, vate, with the potential to feed 17 health and socio-economic benefits,
Wide access to NTD interventions – million people. the opportunities for economies of
free of charge to the end user – have scale by integrating and synergizing
a clear potential to break this vicious delivery modes, and the substantial
cycle and contribute to poverty re- 3.2.2 Investment case volunteer contributions by commu-
duction. In the long term NTD inter- and efficient spending nities and teachers.74 These econom-
ventions could therefore contribute ic effects are most likely an under-
to a livelihood approach to poverty NTD interventions are known to be estimation of the actual gain from
and migration. A good example of some of the most cost-effective pub- NTD-interventions, because they do
such improvements in both health lic health interventions, not only in not include wider social effects of in-
and wealth are provided by the im- the short term with regard to avoid- fections (e.g. productivity effect).
20 Integrating NTDs3.2.3 A vast and diversi-
fied international part- Box 4
ner network, including
Key Messages from: An Investment Case for
the private sector, that is
Ending Neglected Tropical Diseases:75
highly committed
CHAPTER 3
Neglected tropical diseases (NTDs) together account for a
Drawing inspiration from the World significant and inequitably distributed global disease burden,
Health Organization (WHO) “NTD similar in order of magnitude to those of tuberculosis or malaria
Roadmap for Implementation” 76, at approximately 22 million disability-adjusted life-years (DALYs)
which outlines bold targets for the in 2012
control, elimination or eradication Cost-effective interventions to end NTDs are available for as little
of NTDs by 2020, leaders of several as US$3 per DALY averted; these interventions reach the poorest
prominent global health and devel- and most marginalized populations and provide an integrated
opment organizations, together with approach to treat multiple diseases
industry partners, met in London in
2012 and pledged to unite in their Ambitious eradication, elimination, and control targets for
efforts to support the achievement individual diseases emerged with the launch of the World
of the WHO 2020 goals in respect to Health Organization’s NTD roadmap in 2012; the Sustainable
10 neglected tropical diseases. These Development Goals target “the end of NTDs” by 2030
collective promises of support were Interventions to end NTDs are affordable globally; estimated
formalized into the London Declara- treatment costs are US$750 million per year for 2015 to 2020
tion on NTDs,77 and it is around this and US$300 million per year for 2020 to 2030
declaration that a broad coalition Interventions to end NTDs are affordable for the governments of
of partners has emerged. This coali- most endemic countries
tion of NTD partners, called Uniting
Treatment and vector control combined require less than 0.1
to Combat NTDs,78 is composed of bi-
percent of domestic health spending. Domestic value for money is
lateral and multilateral donors, the
enhanced by the unprecedented scale of the London Declaration
private sector, philanthropic foun-
donation of medicines for nine of the most prevalent NTDs
dations, endemic countries, NGDOs,
and academia. These partners have Reaching those targets could avert an estimated 519 million
been working alongside WHO and na- DALYs from 2015 to 2030, compared to 1990 and the beginning
tional programs to address the ne- of concerted efforts to control NTDs
glected disease burden in some of The benefit to affected individuals in terms of averted out-of-
the world’s hardest to reach areas, pocket health expenditures and lost productivity exceeds US$342
tracking their progress towards the billion over the same period
2020 goals annually. The NTD index by The net benefit to affected individuals is about US$25 for every
Uniting to Combat provides an over- dollar to be invested by public and philanthropic funders between
view of a country’s progress in reach- 1990 and 2030—a 30 percent annualized rate of return
ing people in need of NTD treatment.79
The end of NTDs represents a fair and efficient transfer toward
universal health coverage and social protection for those who are
This alliance can also provide collabo-
least well-off
rative links with a vast network of very
diverse international partners, and op-
portunities to leverage investments by
individual donors or donor agencies,
not only in taking field implementa- The strict accountability approach in ion summit in January 2018. By doing
tion to scale, but also to support mul- terms of monitoring progress has led so, African leaders are making a pub-
tilateral research, translating research the African Leaders Malaria Alliance lic commitment to hold themselves
findings into practice, and swiftly in- (ALMA) to add neglected tropical dis- accountable for progress on NTDs,
troducing novel products into imple- eases to its annual scorecard on dis- as the ALMA scorecard is personally
mentation. ease progress at the 30th African Un- reviewed by African heads of state
Integrating NTDs 21Table 5: Drug donation overview by disease in 2017
Disease Drug Form Company Shipped
treatments
Lymphatic Filariasis DEC Tablet Esai 143.587.200
Albendazole Tablet GSK 770.419.000
Ivermectin Tablet MSD 113.441.437
Trachoma Azithromycin Tablet Pfizer 81.381.274
Soil-transmitted helminths Albendazole Tablet GSK 123.690.000
Mebendazole Tablet J&J 29.200.800
Onchocerciasis Ivermectin Tablet MSD 97.324.187
Ivermectin Tablet MSD 89.210.080
Schistosomiasis Praziquantel Tablet Merck 60.343.200
Leprosy PB/MB Tablets and Novartis 2.242.428
Blister packs
Visceral Leishmaniasis AmBisome Vials Gilead 62.600
Chagas Nifurtimox Tablets and Bayer 1.500.000
Blister packs
Human African trypanosomiasis Nifurtimox Tablets Bayer 300.000
Eflornithine Tablets Sanofi 3.200
Pentamidine Tablets Sanofi 1.130
* Represent number of tablets/vials shipped.
Note: Total tablet donations amount to almost 1,7 billion tablets (representing c. 1.5 billion treatments).
Source: 2017 drug donation data overwiew, Uniting to combat NTDs.
every year, putting NTDs alongside they merely require a stand-alone, in poor communities. High occurrence
malaria and maternal and child health vertical approach. There are many of NTD co-morbidities in such com-
as top health priorities for the conti- links (co-morbidities) with other munities should trigger the search
nent. Moreover, there are discussions priority public health areas such as and preventive action for NTDs, both
to also institute a nutritional score- non-communicable diseases (NCDs), in terms of preventive treatment and
card for Africa which should also en- female reproductive health, mental care as well as fundamentally preven-
tail an NTD-component. health and others. Moreover, most of tive interventions in other sectors.
the NTD consequences that become Only in this way will countries be
visible in other health areas – such as able to strengthen their health ser-
3.2.4 NTDs as an female infertility, chronic anemia and vices according to local priorities, tai-
increased HIV transmission, high inci- lor their UHC package to the needs of
opportunity to make
dence of late-onset epilepsy, liver and their poorest communities, and direct
poor people fully kidney disease due to schistosomiasis development to where it is most ur-
benefit from Universal or chronic heart disease due to Cha- gently needed and will yield the high-
Health Coverage and gas disease - are preventable by large est impact.
integrated development scale action against NTDs starting
early in life. Therefore, NTDs should
NTDs are not an isolated group of dis- become an integral part of the UHC
eases and it is wrong to think that essential benefit package especially
22 Integrating NTDsYou can also read