Male Circumcision TECHNICAL REPORT
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
TECHNICAL REPORT
Male Circumcision
TASK FORCE ON CIRCUMCISION
abstract KEY WORD
circumcision
Male circumcision consists of the surgical removal of some, or all, of the ABBREVIATIONS
foreskin (or prepuce) from the penis. It is one of the most common pro- AAFP—American Academy of Family Physicians
cedures in the world. In the United States, the procedure is commonly per- AAP—American Academy of Pediatrics
formed during the newborn period. In 2007, the American Academy of ACOG—American College of Obstetricians and Gynecologists
BV—bacterial vaginosis
Pediatrics (AAP) convened a multidisciplinary workgroup of AAP members CB—caudal block
and other stakeholders to evaluate the evidence regarding male circumci- CDC—Centers for Disease Control and Prevention
sion and update the AAP’s 1999 recommendations in this area. The Task CDM—Charge Data Master
CI—confidence interval
Force included AAP representatives from specialty areas as well as mem-
DPNB—dorsal penile nerve block
bers of the AAP Board of Directors and liaisons representing the American HPV—human papillomavirus
Academy of Family Physicians, the American College of Obstetricians and HSV—herpes simplex virus
Gynecologists, and the Centers for Disease Control and Prevention. The IELT—Intravaginal Ejaculatory Latency Times
MSM—men who have sex with men
Task Force members identified selected topics relevant to male circumci- NHDS—National Hospital Discharge Survey
sion and conducted a critical review of peer-reviewed literature by using NIS—National Inpatient Sample
the American Heart Association’s template for evidence evaluation. OR—odds ratio
RCT—randomized controlled trial
Evaluation of current evidence indicates that the health benefits of new- STI—sexually transmitted infection
born male circumcision outweigh the risks; furthermore, the benefits of UTI—urinary tract infection
newborn male circumcision justify access to this procedure for families This document is copyrighted and is property of the American
who choose it. Specific benefits from male circumcision were identified for Academy of Pediatrics and its Board of Directors. All authors
the prevention of urinary tract infections, acquisition of HIV, transmission have filed conflict of interest statements with the American
Academy of Pediatrics. Any conflicts have been resolved through
of some sexually transmitted infections, and penile cancer. Male cir- a process approved by the Board of Directors. The American
cumcision does not appear to adversely affect penile sexual function/ Academy of Pediatrics has neither solicited nor accepted any
sensitivity or sexual satisfaction. It is imperative that those providing cir- commercial involvement in the development of the content of
this publication.
cumcision are adequately trained and that both sterile techniques and
effective pain management are used. Significant acute complications The guidance in this report does not indicate an exclusive
course of treatment or serve as a standard of medical care.
are rare. In general, untrained providers who perform circumcisions have Variations, taking into account individual circumstances, may be
more complications than well-trained providers who perform the proce- appropriate.
dure, regardless of whether the former are physicians, nurses, or tradi- All technical reports from the American Academy of Pediatrics
tional religious providers. automatically expire 5 years after publication unless reaffirmed,
revised, or retired at or before that time.
Parents are entitled to factually correct, nonbiased information about cir-
cumcision and should receive this information from clinicians before con-
ception or early in pregnancy, which is when parents typically make
circumcision decisions. Parents should determine what is in the best in-
terest of their child. Physicians who counsel families about this decision
should provide assistance by explaining the potential benefits and risks
and ensuring that parents understand that circumcision is an elective
procedure. The Task Force strongly recommends the creation, revision,
and enhancement of educational materials to assist parents of male
infants with the care of circumcised and uncircumcised penises. The Task
Force also strongly recommends the development of educational materi- www.pediatrics.org/cgi/doi/10.1542/peds.2012-1990
als for providers to enhance practitioners’ competency in discussing doi:10.1542/peds.2012-1990
circumcision’s benefits and risks with parents. PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
The Task Force made the following recommendations: Copyright © 2012 by the American Academy of Pediatrics
e756 FROM THE AMERICAN ACADEMY OF PEDIATRICS
Downloaded from pediatrics.aappublications.org by guest on August 18, 2015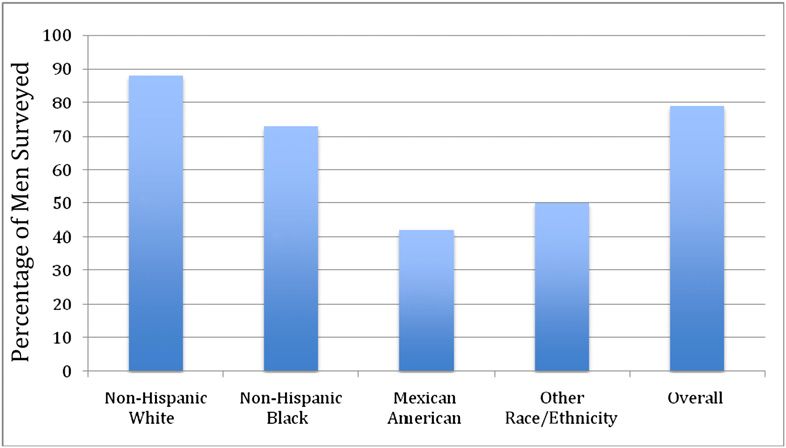
FROM THE AMERICAN ACADEMY OF PEDIATRICS
Evaluation of current evidence indi- prevent procedural and post- INTRODUCTION AND BACKGROUND
cates that the health benefits of procedural pain and are not Statement of the Issue
newborn male circumcision out- recommended as the sole meth-
The American Academy of Pediatrics’
weigh the risks, and the benefits od of analgesia. They should be
(AAP) statement on circumcision of
of newborn male circumcision jus- used only as analgesic adjuncts
the newborn penis was last issued in
tify access to this procedure for to improve infant comfort dur-
May 1999.1 The Circumcision Policy
those families who choose it. ing circumcision. Statement recognized the health ben-
Parents are entitled to factually 8 If used, topical creams may cause efits of circumcision but did not deem
correct, nonbiased information about a higher incidence of skin irrita- the procedure to be a medical neces-
circumcision that should be provided tion in low birth weight infants, sity for the well-being of the child. Since
before conception and early in preg- compared with infants of normal that time, substantial contributions
nancy, when parents are most likely weight; penile nerve block tech- have been made to the peer-reviewed
to be weighing the option of circum- niques should therefore be cho- literature concerning circumcision of
cision of a male child. sen for this group of newborns. males and its possible benefits. For this
Physicians counseling families Key professional organizations reason, in 2007, the AAP formed a Task
about elective male circumcision (AAP, the American Academy of Force charged with reviewing current
should assist parents by explaining, Family Physicians, the American evidence on male circumcision and
in a nonbiased manner, the poten- College of Obstetricians and Gyne- updating the policy on this procedure
tial benefits and risks and by ensur- cologists, the American Society of to provide guidance to AAP member-
ing that they understand the Anesthesiologists, the American ship regarding the circumcision of
elective nature of the procedure. College of Nurse Midwives, and newborn males.
Parents should weigh the health other midlevel clinicians such as The American College of Obstetricians
benefits and risks in light of their nurse practitioners) should work and Gynecologists has endorsed this
own religious, cultural, and per- collaboratively to: technical report.
sonal preferences, as the medical
benefits alone may not outweigh 8 Develop standards of trainee Background
proficiency in the performance
these other considerations for in- Male circumcision consists of the
of anesthetic and procedure
dividual families. surgical removal of some, or all, of the
techniques, including suturing;
Parents of newborn boys should be foreskin (or prepuce) from the penis. It
instructed in the care of the penis, 8 Teach the procedure and anal-
is one of the most common procedures
gesic techniques during post-
regardless of whether the new- in the world. In the United States, the
graduate training programs;
born has been circumcised or not. procedure is most frequently per-
8 Develop educational materials
formed during the newborn period.
Elective circumcision should be for clinicians to enhance their
Elective circumcision performed soon
performed only if the infant’s con- own competency in discussing
after the newborn period is generally
dition is stable and healthy. the benefits and risks of cir-
a result of deferral because of low
Male circumcision should be per- cumcision with parents;
birth weight or illness in the newborn.
formed by trained and competent 8 Offer educational materials to
Circumcision after the newborn period
practitioners, by using sterile tech- assist parents of male infants
is most commonly performed because
niques and effective pain manage- with the care of both circumcised
of the infant’s low birth weight or ill-
ment. and uncircumcised penises.
ness precluded newborn circumci-
Analgesia is safe and effective in The preventive and public health ben- sion. Other infants are circumcised
reducing the procedural pain asso- later in life because of the occurrence
efits associated with newborn male
ciated with newborn circumcision; of tight phimosis and/or urinary tract
circumcision warrant third-party
thus, adequate analgesia should infection (UTI).
reimbursement of the procedure.
be provided whenever newborn The 3 most common operative meth-
circumcision is performed. The American College of Obstetricians ods of circumcision for the newborn
8 Nonpharmacologic techniques and Gynecologists has endorsed this male include: the Gomco clamp, the
(eg, positioning, sucrose paci- technical report. Pediatrics 2012;130: Plastibell device, and the Mogen clamp
fiers) alone are insufficient to e756–e785 (or variations derived from the same
PEDIATRICS Volume 130, Number 3, September 2012 e757
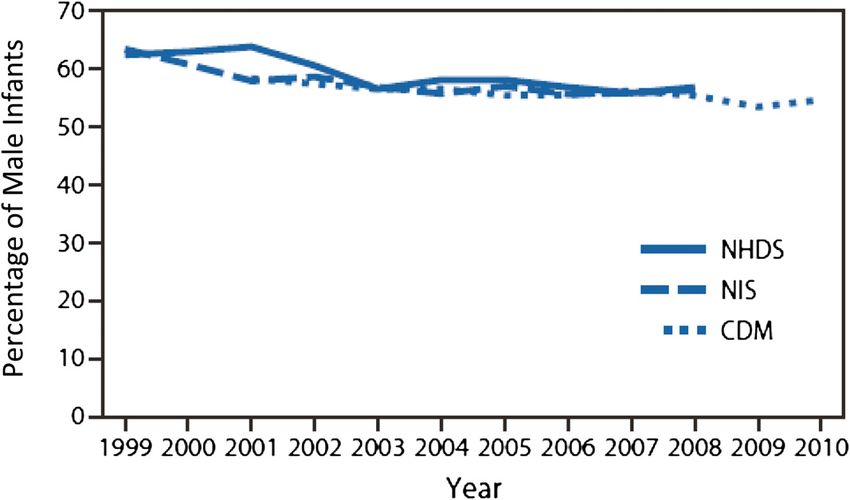
Downloaded from pediatrics.aappublications.org by guest on August 18, 2015principle on which each of these in the first month of life. Overall from rates were found in the Western
devices is based). The elements that 1999 to 2010, the CDC’s weighted states (30%) (Table 1).3
are common to the use of each of these analysis found that the approximate
devices to accomplish circumcision percentage of newborn US males NHANES
include the following: estimation of the who were circumcised was approxi- The NHANES provides a snapshot of the
amount of external skin to be removed; mately 59.1% according to the NHDS, health and nutritional status of the US
dilation of the preputial orifice so that 57.8% according to the NIS, and 55.8% population aged 14 to 59 years at the
the glans can be visualized to ensure according to the CDM. The incidence of time of the survey, by using a proba-
that the glans itself is normal; bluntly newborn male circumcision decreased bility sample of persons aged 0 to
freeing the inner preputial epithelium over time in all 3 data sources: from over 60 years. Prevalence of male cir-
from the epithelium of the glans; 62.5% in 1999 to 56.9% in 2008 cumcision is derived from participant
placing the device (at times a dorsal according to the NHDS; from 63.5% in self-report and is thus subject to
slit is necessary to do so); leaving 1999 to 56.3% in 2008 according to misclassification. From 1999 to 2004,
the device in situ long enough to pro- the NIS; and from 58.4% in 2001 to NHANES found that, of the 6174 men
duce hemostasis; and removal of the 54.7% in 2010 according to the CDM surveyed, 79% of men reported be-
foreskin. (Fig 1). A key limitation is that these ing circumcised, including 88% of
incidence rates were derived from non-Hispanic white men, 73% of non-
The extent of this practice in the United
hospital-based surveys and do not in- Hispanic black men, 42% of Mexican-
States has been estimated by various
clude out-of-hospital circumcisions; American men, and 50% of men of
federally sponsored national surveys,
thus, these data sources underes- other races/ethnicities6 (Fig 2).
each of which has its strengths and
timate the actual rate of newborn However, prevalence rates are limited
limitations; thus, multiple measures of
male circumcision in the first month by the accuracy of the examiner and/or
circumcision prevalence and incidence
of life. the self-report.7,8 These findings un-
are presented. There are large pop-
ulation measures of male circumcision NIS derscore the necessity of using a
in the United States, measuring either The NIS is a database of 5 to 8 million standardized clinical examination for
the occurrence (ie, incidence) of male hospital inpatient stays drawn from establishing circumcision status for
circumcision among newborns or the states that participate in the Health- the purpose of research on circumci-
existence of the circumcised state care Cost and Utilization Project sion. It also highlights the potential
among representative samples of (HCUP). In 2008, these states com- difficulty of advising on care of the
males in the United States at a par- prised 95% of the US population. The circumcised and uncircumcised penis
ticular period in time (ie, prevalence). NIS is used to track and analyze na- when an individual and/or clinician
The findings of these studies are tional trends in health care utilization, may not know which condition is
qualitatively similar and consistently delivery, and outcomes via a 20% present.
estimate the rate of male circumcision stratified sample of 1000 community
to range from 42% to 80% among hospitals. Weights are provided to Ethical Issues
various populations.2–6 calculate national estimates.4 The practice of medicine has long
A recent Centers for Disease Control The NIS indicates that circumcision respected an adult’s right to self-
and Prevention (CDC) study assessed was performed in 57% of male new- determination in health care decision-
trends in the incidence of in-hospital born hospitalizations between 1998 making. This principle has been
newborn male circumcision from 1999 and 2005. NIS data from 1988 to 2008 operationalized through the doctrine
to 2010 using 3 independent sources of indicate that the rate of circumcision of informed consent. The process of
discharge data on in-patient hospital- performed during newborn male de- informed consent obligates the clini-
izations: the National Center for Health livery hospitalizations increased sig- cian to explain any procedure or
Statistics’ National Hospital Discharge nificantly from 48% in 1988–1991, to treatment and to enumerate the risks,
Survey (NHDS), the Agency for Health- 61% in 1997–2000,5 then declined from benefits, and alternatives so the pa-
care Research and Quality’s National In- 61% to 56% in 2000–20086 (Fig 1). tient can make an informed choice. As
patient Sample (NIS), and the SDI Circumcision rates were highest in the a general rule, minors in the United
Health’s Charge Data Master (CDM).2,3 Midwestern states (74%), followed by States are not considered competent
These sources were used to estimate the the Northeastern (67%) and Southern to provide legally binding consent re-
incidence of newborn male circumcision states (61%). The lowest circumcision garding their health care, and parents
e758 FROM THE AMERICAN ACADEMY OF PEDIATRICS
Downloaded from pediatrics.aappublications.org by guest on August 18, 2015FROM THE AMERICAN ACADEMY OF PEDIATRICS
FIGURE 1
Incidence of in-hospital newborn male circumcision, according to data source; United States, 1999–2010.2,3
or guardians are empowered to make well-being.11 Reasonable people may In cases such as the decision to per-
health care decisions on their behalf.9 disagree, however, as to what is in the form a circumcision in the newborn
In most situations, parents are gran- best interest of any individual patient or period (where there is reasonable
ted wide latitude in terms of the how the potential medical benefits and disagreement about the balance be-
decisions they make on behalf of their potential medical harms of circumci- tween medical benefits and harms,
children, and the law has respected sion should be weighed against each where there are nonmedical benefits
those decisions except where they are other. This situation is further compli- and harms that can result from a de-
clearly contrary to the best interests cated by the fact that there are social, cision on whether to perform the
of the child or place the child’s health, cultural, religious, and familial benefits procedure, and where the procedure
well-being, or life at significant risk of and harms to be considered as well.12 It is not essential to the child’s imme-
serious harm.10 is reasonable to take these nonmedical diate well-being), the parents should
Parents and physicians each have an benefits and harms for an individual determine what is in the best interest
ethical duty to the child to attempt to into consideration when making a de- of the child. In the pluralistic society
secure the child’s best interest and cision about circumcision.13 of the United States, where parents
are afforded wide authority for de-
TABLE 1 Multivariate Cox Proportional Hazards Regression of Selected Factors Associated With termining what constitutes appropri-
Circumcision Among Male Newborn Delivery Hospitalizations, United States, 1998–20052 ate child-rearing and child welfare, it
Characteristic Weighted % of Male Adjusted Prevalence is legitimate for the parents to take
Infant Circumcisions Rate Ratios (95% CI) into account their own cultural, re-
Hospital region ligious, and ethnic traditions, in addi-
Midwest 74 3.53 (3.23–3.87) tion to medical factors, when making
Northeast 67 2.90 (2.64–3.18)
South 61 2.80 (2.56–3.07)
this choice.11
West 30 1.00 Physicians who counsel families about
Payer
Private 67 1.76 (1.70–1.82)
this decision should assist parents by
Public 45 1.00 objectively explaining the potential
Hospital location benefits and risks of circumcising their
Urban 66 1.29 (1.24–1.34) infant.10 Because some families may opt
Rural 56 1.00
Newborn health status to circumcise as part of religious or
Term, healthy 61 1.22 (1.20–1.23) traditional practice, discussion should
Not term, healthy 54 1.00 also encompass risks and benefits of
PEDIATRICS Volume 130, Number 3, September 2012 e759
Downloaded from pediatrics.aappublications.org by guest on August 18, 2015members and other stakeholders to
evaluate the evidence on male circum-
cision and update the AAP’s recom-
mendations in this area. The Task Force
included AAP representatives from spe-
cialty areas, including anesthesiology/
pain management, bioethics, child health
care financing, epidemiology, fetus
and newborn medicine, infectious
diseases (including pediatric AIDS),
and urology. The Task Force also in-
cluded members of the AAP Board of
Directors and liaisons representing
FIGURE 2 the American Academy of Family
Prevalence of male circumcision, according to self-report; United States, 1999–2004.5 Physicians (AAFP), the American Col-
lege of Obstetricians and Gynecologists
(ACOG), and the CDC. The Task Force’s
having a medical professional per- including HIV; moreover, there is the evidence review was supplemented by
form this procedure in a clinical set- risk of acquiring an STI if the in- an independent, AAP-contracted, physi-
ting versus having it performed by dividual is sexually active during the cian and doctoral-level epidemiologist
a traditional/religious provider in healing process. (See the section en- who was also part of the entire evi-
a nonmedical environment. titled Sexually Transmitted Diseases, dence review process.
Parents may wish to consider whether Including HIV.)
the benefits of the procedure can be Finally, there is a moral obligation to Literature Search Overview
attained in equal measure if the pro- take reasonable steps to reduce the The Task Force members identified
cedure is delayed until the child is of risk of harm associated with the the following topics and questions as
sufficient age to provide his own in- performance of any surgical inter- relevant to male circumcision and to
formed consent. These interests in- vention. These include ensuring that be addressed through a critical review
clude the medical benefits; the cultural the providers who perform circumci- of the peer-reviewed literature:
and religious implications of being sion have adequate training and
circumcised; and the fact that the demonstrate competence in perform- What is the current epidemiology
procedure has the least surgical risk ing the procedure; the provision of of male circumcision in the United
and the greatest accumulated health adequate procedural analgesia and States?
benefits if performed during the new- postprocedural pain control; and that What are the most common proce-
born period. Newborn males who are the risks of infection are minimized dures and techniques for newborn
not circumcised at birth are much less through appropriate infection control male circumcision?
likely to elect circumcision in adoles- measures, such as a sterile environ- What best supports the parental
cence or early adulthood. Parents who ment and sterilized instruments.14 The decision-making process regard-
are considering deferring circumcision Task Force advises against the prac- ing circumcision?
should be explicitly informed that cir- tice of mouth-to-penis contact during What is the association between
cumcision performed later in life has circumcision, which is part of some male circumcision and both mor-
increased risks and costs. Further- religious practices, because it poses bidity and sexual function/satisfac-
more, deferral of the procedure also serious infectious risk to the child. tion?
requires longer healing time than if
performed during the newborn period
What is the impact of anesthesia
TASK FORCE ON MALE and analgesia?
and requires sexual abstinence during
healing. Those who are already sexually
CIRCUMCISION What are the common complica-
active by the time they have the pro- Committee Membership and tions and the complication rates as-
cedure lose some opportunities for Research Questions sociated with male circumcision?
the protective benefit against sexually In December 2007, the AAP formed What workforce issues affect new-
transmitted infection (STI) acquisition, a multidisciplinary workgroup of AAP born male circumcision?
e760 FROM THE AMERICAN ACADEMY OF PEDIATRICS
Downloaded from pediatrics.aappublications.org by guest on August 18, 2015FROM THE AMERICAN ACADEMY OF PEDIATRICS
What are the trends in financing the preparation of the current report assist parents by explaining, in a
and payment for elective circumci- and cited accordingly. These additional nonbiased manner, the potential
sion? articles did not affect the findings of benefits and risks, and by ensuring
The group agreed on parameters for the Task Force. Areas in which there that they understand the elective
reviewing the literature on associa- were no analytic studies available for nature of the procedure.
tions between male circumcision and the time period of interest are noted as Parents should weigh the health
other outcomes. The literature review such within this document. benefits and risks in light of their
comprised analytic studies (including own religious, cultural, and per-
Evidence Quality and Use in sonal preferences, as the medical
meta-analyses) in the topic areas in
Forming Recommendations
English-language, peer-reviewed, sci- benefits alone may not outweigh
entific literature. The Task Force eval- Articles were reviewed by using the these other considerations for in-
uated studies that addressed the American Heart Association’s template dividual families.
identified clinical questions, including for evidence evaluation.15 The articles Parents of newborn boys should
all meta-analyses; all randomized con- were also assigned a level of evidence be instructed in the care of the
trolled trials; and all case-control, (Table 3) based on the methodology
penis at the time of discharge
prospective and retrospective cohort, used. Among those with evidence lev-
from the newborn hospital stay, re-
and cross-sectional studies based on els 1 through 4, the reviewers assessed
gardless of whether the newborn
the American Heart Association’s tem- the quality of the evidence as “excel-
has been circumcised or not.
plate for evidence evaluation (see the lent,” “good,” “fair,” or “poor” depend-
ing on how well the methodology was Elective circumcision should be
following section). Case reports, case
applied. Articles with an evidence level performed only if the infant’s con-
series, ecological studies, reviews, and
of 5 or higher were not included in this dition is stable and healthy.
opinions were excluded from the re-
view. Although case reports and case review. A critical assessment was made Male circumcision should be per-
series are important for generating of each article/source in terms of the formed by trained and competent
hypotheses, the Task Force limited itself research design and methods, by using practitioners, by using sterile techni-
to reviewing analytic studies. The Task the American Heart Association’s tem- ques and effective pain management.
Force compiled and vetted Medical plate (Table 4). Analgesia is safe and effective in
Subject Headings, which are defined by reducing the procedural pain asso-
the National Library of Medicine. ciated with newborn circumcision;
RESULTS
Searches were conducted in Medline, thus, adequate analgesia should
As a result of these findings, the Task be provided whenever newborn
Cochrane Database, and Embase for
Force made the following recom- circumcision is performed.
the period 1995 through 2010. The
mendations, which are described
literature search produced 1388 ab-
further in the following text: 8 Nonpharmacologic techniques
stracts that were reviewed by both the (eg, positioning, sucrose paci-
epidemiologist and the Task Force Evaluation of current evidence indi- fiers) alone are insufficient to
chair, and those citations meeting the cates that the health benefits of prevent procedural and post-
established criteria were included; newborn male circumcision out- procedural pain and are not re-
ultimately, 1014 articles were included weigh the risks, and the benefits commended as the sole method
in the review (Table 2). A second search of newborn male circumcision jus- of analgesia. They should be
was conducted in April 2010, which tify access to this procedure for used only as analgesic adjuncts
yielded 42 additional citations, of which those families who choose it. to improve infant comfort dur-
17 were included. All 1031 accepted Parents are entitled to factually ing circumcision.
articles were reviewed by the con- correct, nonbiased information about
8 If used, topical creams may
tracted physician epidemiologist and at circumcision that should be provided cause a higher incidence of
least 1 Task Force member; any dif- before conception and early in preg- skin irritation in low birth weight
ferences were resolved by consensus. nancy, when parents are most likely infants, compared with infants
In 2011, individual Task Force members to be weighing the option of circum- of normal weight; penile nerve
also identified other key articles that cision of a male child. block techniques should there-
appeared in the peer-reviewed litera- Physicians counseling families about fore be chosen for this group
ture; these articles were consulted in elective male circumcision should of newborns.
PEDIATRICS Volume 130, Number 3, September 2012 e761
Downloaded from pediatrics.aappublications.org by guest on August 18, 2015TABLE 2 Results from Medline, Cochrane
Database, and Embase Search for 8 Develop educational materials
for clinicians to enhance prac-
reported that the circumcision de-
cision was made before a discussion
1995–2010
titioners’ competency in dis- occurred with the clinician about this
Clinical Topic Areaa No. of Articles Included
cussing the benefits and risks issue. Only 4% of parents reportedly
HIV/STI 231
Procedure and 219
of circumcision with parents; discussed circumcision with their cli-
complications
8 Offer educational materials to nician before the pregnancy.16 This
UTI 53 assist parents of male infants finding is substantiated by the 2009
Pain management 159
Penile dermatoses 107 with the care of both circum- AAP survey of 1620 members with
Penile hygiene 76 cised and uncircumcised pe- a response rate of 57%, in which most
Phimosis 64 nises. respondents reported that parents
Parental decision-
making
60
The preventive and public health of newborn male patients generally
Carcinoma (penile) 58 benefits associated with new- do not seek their pediatrician’s
Carcinoma (cervical) 3 born male circumcision warrant recommendation regarding circum-
Sexual satisfaction
a
1
third-party reimbursement of the cision; only 5% reported that “all” or
“most” parents “are uncertain about
Does not include nonclinical areas such as ethics and
financing.
procedure.
circumcision and seek their recom-
mendation” about the procedure.19
Key professional organizations (AAP, There is fair evidence that parental
Parental Decision-Making
AAFP, ACOG, the American Society of decisions about circumcision are
Anesthesiologists, the American Task Force Recommendations: shaped more by family and socio-
College of Nurse Midwives, and
8 Parents are entitled to factually cultural influences than by discussion
other midlevel clinicians such as correct, nonbiased information with medical clinicians or by parental
nurse practitioners) should work about circumcision that should education.16,20
collaboratively to: be provided before conception
In 4 cross-sectional studies with fair
8 Develop standards of trainee and early in pregnancy, when
evidence, US parents most often
proficiency in the performance parents are most likely to be
reported that they chose to have their
of anesthetic and procedure weighing the option of circum-
newborn son circumcised for health/
techniques, including suturing; cision of a male child.
medical benefits, including hygiene
8 Teach the procedure and anal- 8 Physicians counseling families and cleanliness of the penis (reported
gesic techniques during post- about elective male circumci-
sion should assist parents by by 39.6%, 46%, 53%, and 67%, re-
graduate training programs;
explaining, in a nonbiased man- spectively).16,17,21,22 Social concerns
ner, the potential benefits and (such as having a father or brother
TABLE 3 Evidence Levels risks, and by ensuring that they who was circumcised) were also an
Level Definition understand the elective nature important reason given for newborn
1 RCTs or meta-analyses of multiple clinical of the procedure. male circumcision (22.8%, 23.5%, 28%,
and 37%). Religious requirements for
2
trials with substantial treatment effects
RCTs with smaller or less significant 8 Parents should weigh the circumcision, such as those of the
treatment effects
health benefits and risks in
light of their own religious, cul- Jewish and Islamic faiths, were ranked
3 Prospective, controlled, nonrandomized,
cohort studies tural, and personal preferen- less highly in importance (11%, 12.1%,
4 Historic, nonrandomized, cohort or case-
ces, as the medical benefits 13%, and 19%). Although one of these
control studies
alone may not outweigh these studies was small and included only 55
5 Case series: patients compiled in serial
fashion, lacking a control group (excluded other considerations for indi- patients drawn from a homogeneous
from review) vidual families. population,16 the findings coincide with
6 Animal studies or mechanical model studies the 3 larger and more diverse studies.
(excluded from review) The decision of whether to circumcise
7 Extrapolations from existing data collected a male newborn is frequently made For parents to receive nonbiased in-
for other purposes, theoretical analyses early in the pregnancy and even before formation about male circumcision in
(excluded from review)
8 Rational conjecture (common sense);
conception.16–18 In a cross-sectional time to inform their decisions, clini-
common practices accepted before study of parents of 55 male infants cians need to provide this information
evidence-based guidelines (excluded presenting to a family practice clinic at least before conception and/or
from review)
for a well-child visit, 80% of parents early in the pregnancy, probably as a
e762 FROM THE AMERICAN ACADEMY OF PEDIATRICS
Downloaded from pediatrics.aappublications.org by guest on August 18, 2015FROM THE AMERICAN ACADEMY OF PEDIATRICS
TABLE 4 Assessment of Research Design and Methods
Component of Excellent Good Fair Poor Unsatisfactory
Study and
Rating
Design and Highly appropriate Highly appropriate Adequate design but Small or clearly biased Anecdotal, no controls, off
Methods sample or model, sample or model, possibly biased OR population or model target end points OR not
randomized, proper randomized, proper adequate under the OR weakly defensible defensible in its class,
controls AND controls OR circumstances in its class, limited insufficient data or
outstanding accuracy, outstanding accuracy, data or measures measures
precision, and data precision, and data
collection in its class collection in its class
curriculum item in childbirth classes. care of the penis at the time largely disappeared after circum-
Information to assist in parental de- of discharge from the newborn cision (33 children had pathogenic
cision-making should be made avail- hospital stay, regardless of bacteria before circumcision and
able as early as possible. For this whether the newborn has been 4 had pathogenic bacteria after
reason, obstetrician-gynecologists and circumcised or not. circumcision).26
family physicians who manage prenatal This review found no systematic In adults and children, there is fair
care probably have a more pivotal role studies in infants and children on the evidence that periurethral flora con-
in this decision than do pediatricians. care of the uncircumcised versus tains fewer pathogens after circum-
Bright Futures: Guidelines for Health circumcised penis. cision than before circumcision.26,27
Supervision of Infants, Children, and Parents of newborn boys should be Because these studies looked at cul-
Adolescents, Third Edition, supports instructed in the care of the penis tures 1 time (4 weeks after the cir-
prenatal pediatric visits, at which time at the time of discharge from the cumcision), the long-term significance
pediatricians can provide counsel- newborn hospital stay, regardless of of the findings is unclear.
ing about male circumcision (http:// whether they choose circumcision or Penile wetness (defined as the ob-
brightfutures.aap.org). Medical benefits not. The circumcised penis should be servation of a diffuse homogeneous
and risks need to be presented accu- washed gently without any aggressive film of moisture on the surface of the
rately and in a nonbiased fashion so pulling back of the skin.24 The non- glans and coronal sulcus) is consid-
families can make a decision in light of circumcised penis should be washed ered a marker for poor penile hygiene
their own cultural, religious, and per- with soap and water. Most adhesions and is more prevalent in uncir-
sonal preferences. present at birth spontaneously re- cumcised than in circumcised men.28
There is fair evidence that there are solve by age 2 to 4 months, and the Penile wetness has been associated
financial barriers to the circumcision foreskin should not be forcibly re- with HIV infection in 1 cross-sectional
decision in the United States; when tracted. When these adhesions dis- study, although the temporal re-
the procedure is not covered by in- appear physiologically (which occurs lationship is unclear and the evidence
surance, parents are less likely to at an individual pace), the foreskin level is fair.29 A related study with fair
choose to have their child circum- can be easily retracted, and the evidence assessed the frequency of
cised.21 This finding does not seem to whole penis washed with soap and washing the whole penis (including
be true in Canada, where the preva- water.25 retracting the foreskin for uncir-
lence of circumcision did not change Circumcision reduces the bacteria cumcised men) and found that not
after circumcision for ritual, re- that accumulate under the prepuce always washing the whole penis was
ligious, cultural, or cosmetic reasons which can cause UTIs and, in the adult approximately 10 times more com-
was delisted from insurance benefits male, can be a reservoir for bacteria mon in uncircumcised than in cir-
in 1994.17,23 that cause STIs. In an internally cumcised men.30 The relationship
controlled study with fair evidence, between penile wetness and thor-
Care of the Circumcised Versus
researchers cultured the periure- ough washing of the penis is unclear
Uncircumcised Penis
thral and glandular sulcus of 50 and, because the studies were con-
Task Force Recommendations: children aged 1 to 12 weeks before ducted in STI clinics, the findings
8 Parents of newborn boys and 4 weeks after circumcision may not be generalizable to the
should be instructed in the and found the pathogenic bacteria population at large.
PEDIATRICS Volume 130, Number 3, September 2012 e763
Downloaded from pediatrics.aappublications.org by guest on August 18, 2015Male Circumcision and Diseases, entry for pathogens. The foreskin also heterosexually acquired HIV infection
Morbidities, and Sexual Function/ contains a high density of HIV target in men.40–53 One study with fair evi-
Satisfaction cells (ie, Langerhans cells, CD4 T cells, dence found that male circumcision
STIs, Including HIV macrophages), which facilitates HIV before puberty (specifically before 12
infection of host cells. The preputial years of age) is more protective than
Task Force Recommendation: space provides an environment that is circumcision occurring at a later
8Evaluation of the current evi- thought to “trap” pathogens and bodily age.50 Three large randomized con-
dence indicates that the health secretions and favor their survival and trolled trials provide good evidence of
benefits of newborn male circum- replication.26,27,34 The circumcised male such protection.54–56 A cross-sectional
cision outweigh the risks, and has no foreskin and may likely provide study with fair evidence is neutral
the benefits of newborn male a less welcoming environment for such regarding the relationship between
circumcision justify access to substances. In addition, STI-containing circumcision and HIV infection.57 Two
this procedure for those fami- secretions have increased contact time other studies with a cross-sectional
lies who choose it. in the prospective uncircumcised male design provide fair evidence that cir-
The most notable research con- host, which may increase the likelihood cumcision increases the risk of HIV
tributions to the literature since 1995 of transmission and infection. The ex- infection, although one of these stud-
are studies of male circumcision and posed surfaces of the uncircumcised ies highlights the HIV risks associated
the acquisition of HIV and the trans- penis do not offer the same physical with circumcision performed outside
mission of other STIs. Review of the barrier to resist infection that the the hospital setting and without ster-
literature revealed a consistently re- highly keratinized surface of a circum- ile equipment and medically trained
ported protective effect of 40% to 60% cised penis does. Finally, the higher personnel.58,59
for male circumcision in reducing the rates of sexually transmitted genital
A recently published study from the
risk of HIV acquisition among hetero- ulcerative disease (eg, HSV-2) observed
CDC provides good evidence that, in
sexual males in areas with high HIV in uncircumcised men may also
the United States, male circumcision
prevalence due to heterosexual trans- increase susceptibility to HIV infec-
before the age of sexual debut would
mission (ie, Africa). tion, as the presence of genital
ulcers, irrespective of circumcision reduce HIV acquisition among hetero-
There is also good evidence from sexual males.60 Although individual
randomized controlled trials that status, increases the likelihood of HIV
acquisition.35–37 sexual practices are difficult to pre-
male circumcision is associated with dict in the newborn period, the ma-
a lower prevalence of human papillo- HIV jority of US males are heterosexual
mavirus (HPV) infection31,32 and her- and could benefit from male circum-
The CDC estimates that 1.2 million
pes simplex virus type 2 (HSV-2) cision. Mathematical modeling by the
people in the United States are living
transmission,31,33 as well as a de- CDC shows that, taking an average
with HIV, the virus that causes AIDS,
creased likelihood of bacterial vagi- which is incurable. Approximately 50 000 efficacy of 60% from the African trials,
nosis (BV) in female partners.80 The Americans are newly infected with and assuming the protective effect of
evidence for male circumcision being HIV each year; more than 619 000 circumcision applies only to hetero-
protective against syphilis is less people in the United States have died sexually acquired HIV, there would be
strong,65–68 however, and male cir- of AIDS since the epidemic began.38 a 15.7% reduction in lifetime HIV risk
cumcision was not found to be asso- In the United States, HIV/AIDS predom- for all males. This is taking into ac-
ciated with decreased risk of inantly affects men who have sex with count the proportion of HIV that is
gonorrhea84,85,91–93 or chlamydia.84–89 men (MSM), who account for almost acquired through heterosexual sex
It is biologically plausible that the two-thirds (61%) of all new infections. and reducing that by 60%. The percent
circumcised state may confer pro- Heterosexual exposure accounts for reduction in HIV cases was deter-
tection against STIs (including HIV). 27% of new HIV infections, and in- mined by assessing the proportion of
Possible mechanisms for the pro- jection drug use accounts for 9% of new cases of HIV infection that could
tective effect of circumcision include new HIV cases. In other parts of the be prevented by analyzing which
the fact that the foreskin’s thin inner world (eg, Africa), heterosexual trans- infections would be presumed to oc-
surface is susceptible to microtears mission is far more common.39 cur in uncircumcised males and what
and abrasions (especially during sex- Fourteen studies provide fair evidence the reduction would be if those who
ual activity), which provides a port of that circumcision is protective against would not already be circumcised
e764 FROM THE AMERICAN ACADEMY OF PEDIATRICS
Downloaded from pediatrics.aappublications.org by guest on August 18, 2015FROM THE AMERICAN ACADEMY OF PEDIATRICS
would be circumcised. The propor- Heterosexual Women to the CDC and 18 079 cases of late
tions of transmissions prevented are Women account for 23% of new HIV and late latent syphilis. The rate of pri-
lower than in Africa because a higher infections in the United States; HIV in- mary and secondary syphilis in 2010
proportion of US HIV transmission fection in women is primarily attributed was 4.5 cases per 100 000 individuals,
occurs between MSM. In addition, a either to heterosexual contact or in- 2.2% lower than the 2009 rate. “The
portion of the population would be jection drug use.38 Two prospective total number of cases of syphilis
circumcised without any policy change, cohort studies with fair evidence lo- (primary and secondary, early latent,
and the prevented cases would only oked at the relationship between a late, late latent, and congenital) re-
occur in the additional circumcised woman’s risk of HIV infection and ported to CDC increased 2.2% (from
males. This ranges from an estimated whether her primary male partner is 44,830 to 45,834 cases) during 2009–
8% reduction in non-Hispanic white circumcised. The first study describes 2010.”67 A large percentage of syphilis
males to an estimated 21% reduction a protective effect but had consider- cases occur in MSM; in 2010, 67% of
among non-Hispanic black males. The able loss-to-follow-up and possible the reported primary and secondary
CDC study suggests that newborn cir- misclassification of the partners’ cir- syphilis cases were among MSM.67
cumcision performed in the United cumcision status.63 The other study The balance of evidence suggests that
States to prevent HIV infection is cost- showed nonsignificant protection in the male circumcision is protective against
effective without consideration of other high-risk group (ie, women who were syphilis.68–70 One meta-analysis with
health benefits. The CDC recommen- more likely to have ever engaged in sex good evidence describes a protective
dations state that all parents of new- work; to have reported 2 or more effect (relative risk: 0.67 [95% CI:
born males should be given the choice partners in the last 3 months; and/or 0.54–0.83]), but there is considerable
of circumcision. to have had a higher median lifetime heterogeneity among the studies in-
number of sex partners) but neither cluded.68 An additional cohort study
Specific HIV Risk Populations protection nor increased risk in the with fair evidence found that circum-
study population as a whole.64 A meta- cised men were significantly less
MSM
analysis with good evidence of data likely to have active syphilis at the
The association of circumcision and from 1 randomized controlled trial point of study recruitment; when the
the decreased likelihood of HIV (RCT) and 6 longitudinal analyses found men were followed up prospectively
acquisition applies to heterosexual little evidence that male circumcision for 2 years, a protective effect was
males. Circumcision seems to be less directly reduces their female partner’s also observed but was nonsignifi-
likely to protect MSM, however, and risk of acquiring HIV (summary relative cant.69 Good evidence from a large
has not been associated with de- risk: 0.8 [95% confidence interval (CI): RCT reported no reduction or trend
creased acquisition of HIV among 0.53–1.36]); however, male circum- toward reduction for male circumci-
MSM.61 There is fair evidence from 1 cision’s protective effect did not reach sion and the incidence of syphilis71;
study that there is a protective effect a level of statistical significance.65 One however, the extent to which protec-
of circumcision from HIV infection in Ugandan RCT study with good evidence tion might be afforded, and among
MSM; however, this study used self- found that, at 24 months, the risk of HIV which specific populations, is difficult
report to establish circumcision sta- infection among women whose male to determine.
tus.62 One study with fair evidence is partners were circumcised was 21.7%
neutral regarding the relationship compared with 13.4% for female part-
between circumcision and HIV in- Genital Herpes
ners of uncircumcised men.66
fection in MSM.61 It is probable that Genital herpes is an STI commonly
the differences found in the level of Ulcerative STIs manifested by recurrent genital ulcers
protection (or lack of protection) by Genital ulcers are notable both because caused by HSV-1 or HSV-2. HSV may not
studies of MSM are confounded by of the morbidity and mortality associ- be clinically evident despite infection.
the fact that MSM commonly perform ated with the causative organism and Approximately 16.2% of US individuals
both receptive and insertive sex. It is because the presence of the ulcer itself aged 14 to 49 years have HSV-2.31,72
not known to what extent circumci- facilitates the transmission of HIV. Case reporting data for genital HSV
sion may be protective against HIV are not available, but 2005–2008
transmission for MSM who practice Syphilis NHANES data indicate that the per-
insertive sex versus for those who From 2009 to 2010, there were 13 604 centage of NHANES participants aged
engage in receptive sex. cases of early latent syphilis reported 20 to 49 years who reported having
PEDIATRICS Volume 130, Number 3, September 2012 e765
Downloaded from pediatrics.aappublications.org by guest on August 18, 2015been diagnosed with genital herpes at countries, although its identification is cohort study with good evidence also
some point was 18.9%.72 not always obvious; the number of found that male circumcision, among
One meta-analysis with good evidence cases of this infection in the United other factors, was protective against BV
found some protective effect of cir- States is unknown.77 Granuloma in- in female partners.82 A cross-sectional
cumcision against HSV-2 of borderline guinale is a genital ulcerative disease study with fair evidence found no effect
statistical significance.68 Good evidence that is rare in the United States but but may have lacked the power to de-
of the protective effect of male cir- endemic in some tropical and de- tect an effect.83
cumcision is available from two of the veloping areas. The lesions might de-
large randomized controlled trials in velop secondary bacterial infection or Chlamydia
Africa. In the South African study, the can coexist with other sexually trans- Chlamydia is the most commonly
incidence of HSV-2 was 34% lower in mitted pathogens. reported notifiable disease in the
circumcised men.73 In the Uganda The literature search produced no United States and the most common
study, the risk of HSV-2 infection (ad- studies since 1995 exploring the re- STI reported to the CDC, with 1 307 893
justed for other factors) was 28% lationship between male circumci- chlamydial infections (426.0 cases per
lower in circumcised men.71 There is sion and lymphogranuloma venereum 100 000 individuals) reported to the
fair evidence from 1 study that male or granuloma inguinale. One meta- CDC in 2010.84
circumcision protects female partners analysis provided fair evidence that The balance of evidence does not re-
against HSV-2 infection.33 Two studies genital ulcerative disease was more veal any relationship between circum-
with fair evidence found that there is common in uncircumcised men but not cision and chlamydia infection.85–87 The
no effect of circumcision on the risk of to a statistically significant degree.78 1 prospective cohort study with fair
HSV-2 acquisition.6,74 One cross-sectional study with fair evidence showed a protective effect,
evidence found that male circumci- but the study had a composite end
Chancroid sion was protective against genital point with several STIs combined and
Chancroid is a bacterial disease spread ulcers, but the findings were based on used self-report of STI as the out-
through sexual contact. It is rare in the respondents self-reporting a history come (increasing the possibility of
United States, with a total of 24 cases of genital ulcerative disease and may misclassification).88 Two studies with
reported in 2010 (a rate of 0.08 case per not be accurate.79 fair evidence explored the effect of
100 000 individuals).75 male circumcision on chlamydia in-
The literature search produced no Nonulcerative STIs fection in female partners. The first,
individual studies since 1995 exploring Nonulcerative STIs generally cause in- a prospective cohort study, found a
the relationship between male cir- flammation and scarring along the re- nonsignificant increased risk in the
cumcision and chancroid. One meta- productive tract. Untreated infection female partners of circumcised men.89
analysis with good evidence found can cause cancer, can interfere with The second, a cross-sectional study,
that 6 of 7 older studies (85%) de- reproduction, and can negatively impact found a significantly decreased risk
scribed circumcision as having a pro- newborn health. Additionally, these in- of chlamydia infection among women
tective effect against chancroid. This fections can facilitate the transmission with circumcised male sexual part-
meta-analysis did not provide a sum- of HIV. ners, but a possible selection bias may
mary value for the relationship due to have affected results because only
differences in the definition and as- BV 51.8% of subjects had specimens for
certainment of outcomes and variabil- BV is a condition “in women where the analysis.90
ity among the comparison groups.68 normal balance of bacteria in the va-
One methodologically poor meta-analysis gina is disrupted and replaced by an Gonorrhea
found no effect of male circumcision on overgrowth of certain bacteria.”80 BV Gonorrhea is the second most com-
chancroid.76 is common among pregnant women; monly reported STI in the United States,
an estimated 1 080 000 pregnant women with 309 341 cases reported to the CDC
Lymphogranuloma Venereum and have BV annually. (a rate of 100.8 cases per 100 000
Granuloma Inguinale (Donovanosis) There is good evidence from 1 large individuals) in 2010.91
The CDC reports that the frequency of randomized controlled trial that male The evidence does not demonstrate
lymphogranuloma venereum infection circumcision is protective against BV any relationship between circumcision
is thought to be rare in industrialized in female partners.81 A small prospective and gonorrheal infection.85,86,92–94 The
e766 FROM THE AMERICAN ACADEMY OF PEDIATRICS
Downloaded from pediatrics.aappublications.org by guest on August 18, 2015FROM THE AMERICAN ACADEMY OF PEDIATRICS
studies that show a protective effect prevalence of high-risk HPV infection anatomic defects such as reflux or
are either barely significant or have was 28% lower in female partners of recurrent UTIs.
poorly defined or self-reported out- circumcised HIV-uninfected men, while There is fair evidence from 5 obser-
comes, thus offering only a fair level the incidence was 23% lower.32 Good vational studies that UTI incidence
of evidence.79,88 evidence from another Uganda ran- among boys under age 2 years is re-
domized controlled trial of male cir-
duced in circumcised infant boys,
HPV cumcision in HIV-infected men indicates
compared with uncircumcised boys
HPV is among the most commonly oc- that a circumcision did not reduce the
under the age of 2.108–112 The degree of
curring STIs in the United States and risk of male-to-female transmission of
high-risk HPV from HIV-infected men.103 reduction is between threefold and
can lead to the development of can-
10-fold in all studies.
cers, including cervical cancer. The
population-based data from NHANES Male Circumcision and UTIs There is fair evidence from a prospective
2003–2006 indicate that the overall According to the CDC, “A urinary tract study that there is a decreased preva-
prevalence of high- and low-oncogenic infection (UTI) is an infection involving lence of uropathogens in the periure-
risk HPV types was 42.5% among US any part of the urinary system, in- thral area 3 weeks after circumcision,
women aged 14 to 59 years. The cluding urethra, bladder, ureters, and compared with similar cultures taken at
prevalence of infection was lower for kidney.”104 UTIs are the most common the time of circumcision.113 By using
the 2 viral types with the highest risk type of health care–associated infec- these rates and the increased risks
of causing cancer, however, at 4.7% for tion reported to the National Health- suggested from the literature, it is es-
HPV type 16 and 1.9% for HPV type 18.95 care Safety Network among US timated that 7 to 14 of 1000 un-
There is good evidence that male cir- individuals. The majority of UTIs in circumcised male infants will develop
cumcision is protective against all males occur during the first year of a UTI during the first year of life, com-
types of HPV infection (nononcogenic pared with 1 to 2 infants among 1000
life. In children, UTIs usually necessi-
and oncogenic). Two prevalence studies circumcised male infants.
tate a physician visit and may involve
with good evidence found a 30% to 40% the possibility of an invasive pro- There is a biologically plausible ex-
reduction in risk of infection among cedure and hospitalization. planation for the relationship between
circumcised men.96,97 These studies fail an intact foreskin and an increased
Most available data were published
to provide information on the risk of association of UTI during infancy. In-
before 1995 and consistently show an
acquiring HPV and may reflect persis- creased periurethral bacterial coloni-
association between the lack of cir- zation may be a risk factor for UTI.114
tence of HPV rather than acquisition of
cumcision and increased risk of UTI. During the first 6 months of life, there
infection. Four studies provide fair ev-
idence that male circumcision protects Studies published since 1995 have are more uropathogenic organisms
against HPV.98–101 The selection of an- similar findings. There is good evi- around the urethral meatus of un-
atomic sites sampled may influence dence from 2 well-conducted meta- circumcised male infants than around
the results.98 analyses105,106 and a cohort study107 those of circumcised male infants
that UTI incidence among boys under (this colonization decreases in both
Good evidence of the protective effect
of male circumcision against HPV is age 2 years is reduced in those who groups after the first 6 months).115 In
available from two of the large ran- were circumcised compared with un- addition, an experimental preparation
domized controlled trials in Africa. In circumcised boys. The data from ran- found that uropathogenic bacteria
the South African study, the preva- domized controlled trials are limited. adhered to, and readily colonized, the
lence of high-risk HPV was 32% lower However, there are large cohort and mucosal surface of the foreskin but
in circumcised men.102 In the Uganda case-controlled studies with similar did not adhere to the keratinized skin
study, the risk of oncogenic HPV in- findings. Given that the risk of UTI surface of the foreskin.116
fection (adjusted for other factors) among this population is approxi-
was 35% lower in circumcised men.71 mately 1%, the number needed to Cancer
There is also good evidence that male circumcise to prevent UTI is approxi-
circumcision reduces the risk of male- mately 100. The benefits of male cir- Penile Cancer
to-female transmission of high-risk cumcision are, therefore, likely to be Penile cancer is rare, and rates seem
HPV from HIV-uninfected men. In the greater in boys at higher risk of UTI, to be declining. In the United States,
Uganda randomized controlled trial, the such as male infants with underlying Surveillance, Epidemiology, and End
PEDIATRICS Volume 130, Number 3, September 2012 e767
Downloaded from pediatrics.aappublications.org by guest on August 18, 2015You can also read