Acute Asthma CMT teaching - 6th Feb 2018 Dr Nicola Green Respiratory Consultant Northumbria Healthcare trust
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Acute Asthma CMT teaching th 6 Feb 2018 Dr Nicola Green Respiratory Consultant Northumbria Healthcare trust
Acute asthma • Why is it important? • Where are we going wrong? • Ways we can improve • Management of acute severe asthma • Pitfalls • Case report • Questions

Why is acute asthma management important ?
Why is acute asthma management important ? • 5.5 million individuals with a diagnosis of asthma in the UK • Accounts for huge number of interactions with medical services • 2011-2012 >65,000 hospital attendances • One of the highest death rates in Europe ~1200/year

Asthma Deaths • Where? • Who? • Why?
Asthma Deaths • Where? • 45% died without seeking medical attention/ emergency care • Recent hospital attendances • 47 % previous hospital admission • 21% in the last 12 months • 10% in the last 28 days

Asthma Deaths
• Who ?
• Median age of diagnosis – 37yo
• 69% diagnosed with asthma in adulthood
• Rare for 1st presentation asthma to be acute severe/life
threatening,
• Vast majority have chronic severe disease -although - this
may not have been recognised!
• previous near-fatal asthma, eg previous ventilation or
respiratory acidosis
• previous admission for asthma especially if in the last year
• requiring three or more classes of asthma medication
• heavy use of β2 agonist
• repeated attendances at ED for asthma care especially if in
the last year
• “brittle” asthma.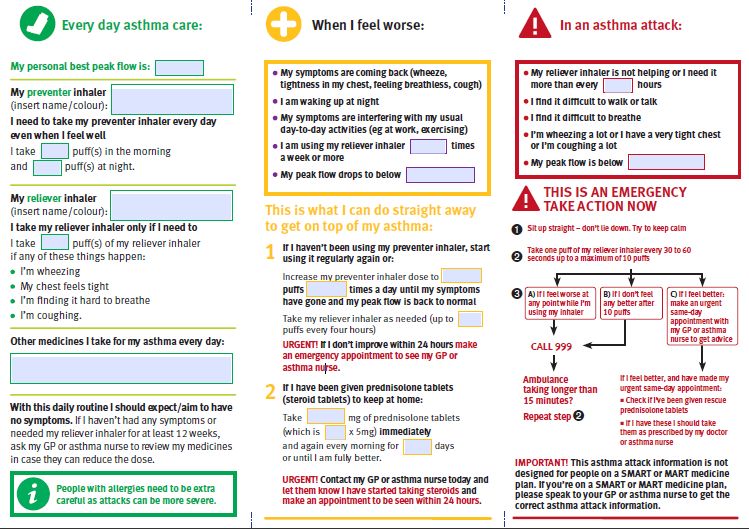
Asthma Deaths
• Why?
• Poor recognition of severity
• 58 % mis-labelled as mild/moderate
• “Complacency” in asthma management
• Poor recognition of symptom control
• Excessive bronchodilator use - 39% > 12 and 4% >
50 in last 12 months
• Poor compliance with management
• 38 % < 4 ICS or ICS/LABA in 12 months
• 80% < 12 ICS or ICS/LABA in 12 months
Asthma Deaths
• Why?
• Inadequate medical management
• Oral/ inhaled steroids
• 14% single component ICS and LABA
• 3% LABA monotherapy – no ICS
• Lack of primary and secondary care follow up
• 43% no asthma review in previous 12 months
• PAAP – Personalised Asthma Action Plans
• 77% did not have written asthma plan
• 50% no documentation in triggersAsthma Deaths • Why? • Nocturnal presentation • Poor symptom perception • Increasing age • Female • Increasing severity of disease • Duration of asthma
RCP Control Questions • In the last 2 weeks, have you woken during the night because of your asthma (including cough)? • In the last 2 weeks have you had any asthma symptoms during the day (cough, wheeze, chest tightness, SOB)? • In the last month has your asthma interfered with you usual activities (housework, work, school etc.)? • ANSWER TO ANY YES = ASTHMA NOT CONTROLLED
Asthma Deaths
Why?
• Adverse psychosocial or behavioural factors
• non-compliance with • alcohol or drug abuse
treatment or • Obesity
monitoring • learning difficulties
• failure to attend • employment problems
appointments
• income problems
• frequent home visits
• social isolation
• self discharge from
hospital • childhood abuse
• psychosis, depression, • severe domestic,
other psychiatric marital or legal stress.
illness or deliberate
self harm current or
recent major
tranquilliser useAcute Medical Management • Assess severity • Mild • Moderate • Acute severe • Life threatening • Near fatal
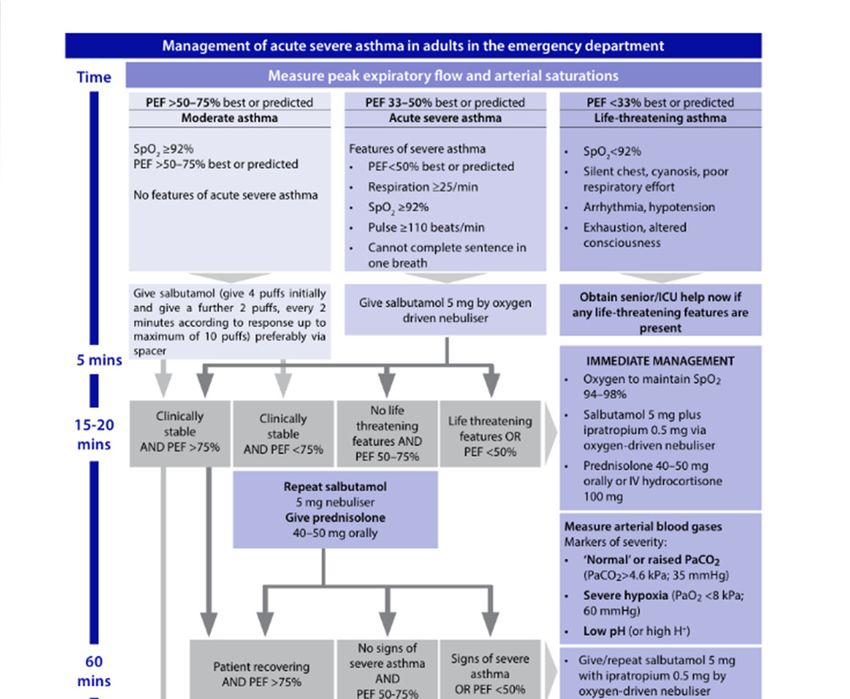
Acute Asthma Severity Assessment
Mild
PEFR >75% predicted or best
Moderate
PEFR 50 -75% predicted or best
Acute severe
PEFR 33 – 50% + any of
Sp02 ≥ 92%
RR ≥ 25/min
Pulse ≥ 110/min
Can’t complete sentence in 1 breath
Life threatening
SpO2≤ 92%
Silent chest, cyanosis, poor respiratory effort
Bradycardia, hypotension, arrhythmia
Exhaustion, confusion, coma
Near fatal
Raised pCO2
Mechanical ventilation with raised inflation pressuresAcute Asthma Management • If a patient has any severe/ life threatening features ABG is mandatory • ABG parameters of life threatening attack • Normal or high pCO2 (4.6- 6 kPa, 35 – 45 mmHg) • Severe hypoxia (< 8kPa, 60mmHg) irrespective of treatment with O2 • Low pH
https://www.brit-
thoracic.org.uk/document-
library/clinical-
information/asthma/btssign-
asthma-guideline-2009/
ASK FOR HELP
EARLYWatch Out for • Patient that has had nebulised bronchodilator prior to your assessment • The patient that tells you they feel better • A clinical scenario that can deteriorate quickly – regular reassessment is key and appropriate observation time is imperative
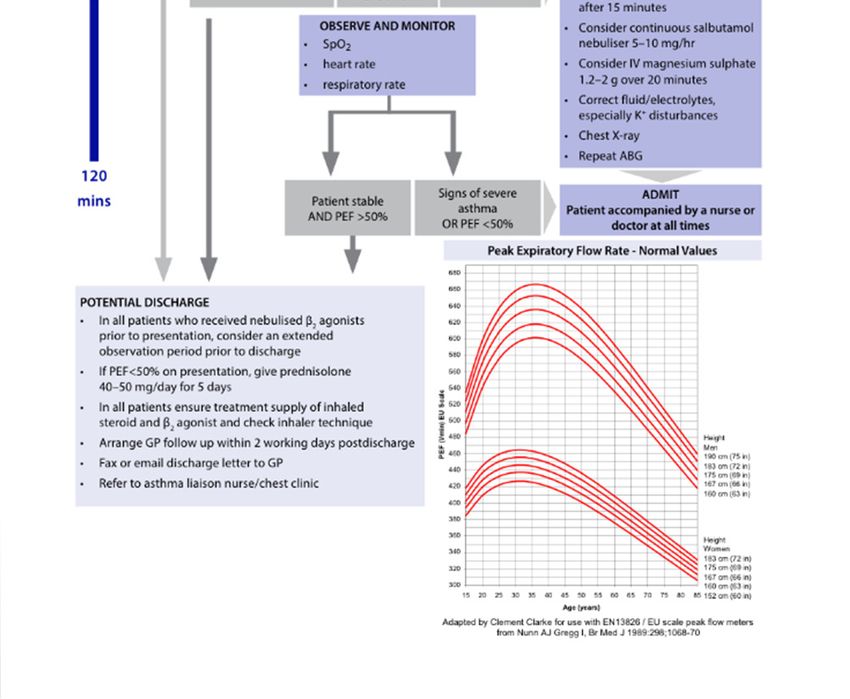
Discharge Pitfalls • Always admit a patient if they have symptoms of • Near fatal asthma • Life threatening asthma • Acute severe asthma after initial Rx • It is your responsibility to check inhaler technique if you plan to discharge a patient from A+E / out of hours • If inhaler technique is poor then no useful delivery of bronchodilator will occur post discharge • Ensure the patient has adequate doses of inhaled therapy available (including inhaled steroids)
Inhalers are confusing!
Safe Discharge
• Inhaler technique and compliance should be assessed and well
documented – if you are discharging a patient this is YOUR
responsibility
• Trigger assessment, documentation and advice
• Asthma self management plans
• Respiratory Specialist Nurse Support
• Appropriate follow-ups for every attendance and admission
• GP (48 hours)/ Specialist Nurses (2 weeks) / Specialist Asthma ClinicPAAP – Personalised Asthma Action Plan • A personalised action plan should be tailored to the person with asthma, enabling people with asthma to recognise when symptoms are worse and setting out actions to be taken when asthma control deteriorates.' • (National Institute for Clinical Excellence, 2013) • 'Written personalised asthma action plans may be based on symptoms and/or peak flows.' (BTS/SIGN, 2014) • 'An asthma action plan, together with regular reviews, is the most effective way to get the best outcomes for patients' (The British Lung Foundation (BLF), 2014) •
Peak flow 80 – 100% 60 – 80% 40 – 60%
Abbreviated Temporary Discharge PAAP
Peak flow less than 40%……………………………………. IMPORTANT
SYMPTOMS: Cough - increasing
Wheeze - increasing You MUST Seek emergency care within 1
Short of breath - increasing hour; come to accident and emergency.
Tight chest
Waking at night In the meantime use your salbutamol
Unable to do usual activities reliever inhaler via spacer to relieve
difficulty walking / talking breathlessness.Summary • Evaluating severity of acute exacerbation • Appropriate management • Identifying key factors that may have poor prognostic indicators • Safe discharge • Personalised Asthma Action Plans Every interaction with medical services is an opportunity to prevent an asthma death
Case Study - Background
• 42 year old female
• In full time employment as cleaner
• Hx of asthma since childhood
• Maintained on beclometasone 100mcg bd and
prn salbutamol
• Never hospitalised
• 1 to 2 courses oral steroids / year
• Asthma review GP March that year
• Control “ok”
• PEFR – unsure of previous valuesCase Study • Attends A+E in January • Several day Hx increasing SOB/ wheeze/ non productive cough • Deterioration overnight • In “respiratory distress” in ambulance at 3am • salbutamol neb en route with some improvement • RR – 30 HR– 110 BP 114/50 Sats 98% on 10L Temp 36.8 • PEFR 190 (= 40% of predicted 450) • Completing short sentences “Feels much better after neb” • Not cyanosed • Prolonged expiratory phase • Resonant throughout • Diffuse polyphonic wheeze
Case Study • Given further salbutamol neb • PEFR 220 (=48% predicted) • “Feels much better – more or les back to normal” • “Needs to get kids to school” • 6.30 am discharged • 5/7 course pred • 1/52 augmentin 375mg • Advised to return if not improving
Case Study • Re-attended following day 05.20am (paramedic ambulance) • Significant deterioration preceding night • Unable to complete sentences • Sats 96% RA, widespread wheeze • PEFR 90 ( 20% predicted) • Rx salbutamol neb PEFR 120 sats 92% • Further salbutamol neb PFR 180 sats 96% • D/C home with advice to complete course pred + augmentin
Case Study • Re-attended 15.20 • Further significant deterioration • RR 43 Sats 91% RA, P 125, BP 191/80 • ABG 10L - pH 7.32, pCO2 6.15, pO2 11.6, Bic 23.4, BE -1.2 • Referred to medicine • Subsequent rapid deterioration
Case Study • Unresponsive • Cyanotic • Sats 44% BP 250/110 HR 150 • ITU “fast paged” • Intubated and ventilated in A+E resus • CXR hyperinflation nil focal
Cerebral oedema secondary to
hypercapnia
Patient Normal 42 year old femaleCase Study • Asthma symptoms every day interferes with daily activities • Night-time waking ~ 1/52 • Environmental triggers – dogs/cats • Never goes anywhere without salbutamol – uses at least twice/day • ?compliance with inh steroid – only 2/3 prescribed inhalers collected poor background control with poor symptom perception
Questions?
You can also read