ALCOHOL & DRUG STRATEGY 2015 - 2018 Working together to improve the quality of life for everyone affected by alcohol and drugs living in ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
ALCOHOL & DRUG STRATEGY
2015 – 2018
Working together to improve the quality of life for
everyone affected by alcohol and drugs living in
Lanarkshire
1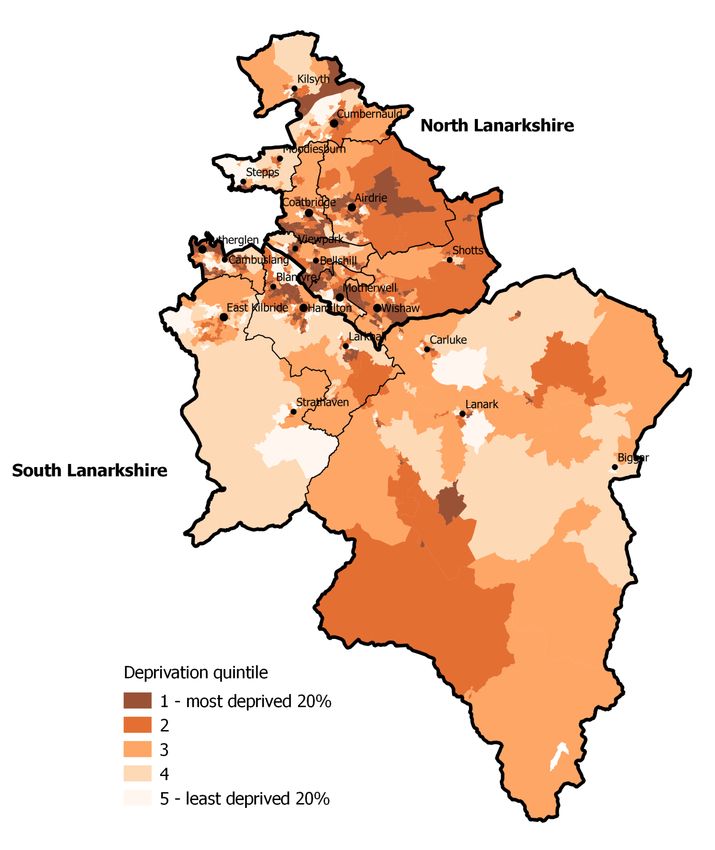
2
CONTENTS
FOREWORD 5
EXECUTIVE SUMMARY 6
CHAPTER 1: INTRODUCTION 9
1.1 INTRODUCTION 9
1.2 OUR VISION 12
Our Commitment 12
1.3 DELIVERING OUR VISION IN PARTNERSHIP 12
CHAPTER 2: OUR CHALLENGE ERROR! BOOKMARK NOT DEFINED.
2.1 LANARKSHIRE’S RELATIONSHIP WITH ALCOHOL Error! Bookmark not defined.
2.2 OUR ROAD TO RECOVERY Error! Bookmark not defined.
2.3 YOUNG PEOPLE Error! Bookmark not defined.
2.4 INEQUALITIES: THE LINK BETWEEN DEPRIVATION & HEALTH Error!
Bookmark not defined.
2.5 COMMUNITY AND ENVIRONMENT Error! Bookmark not defined.
CHAPTER 3: WHERE ARE WE NOW? 34
3.1 INTRODUCTION 34
3.2 PROMOTING THE DEVELOPMENT OF A RECOVERY ORIENTATED SYSTEM OF
CARE WITHIN OUR COMMUNITIES 36
Early Interventions 36
Responding to the Needs of Adults in Distress 37
Improving Links with Primary Care 37
Acute Services 37
Mental Health Services 38
Providing Support for the Family 38
Mutual Aid & Recovery Networks 39
Finding a Safe and Stable Place to Stay 41
Promoting Engagement in Volunteering & Other Meaningful Activities 44
Reducing the Impact of Crime within our Communities 44
Joint Work with the Fire & Rescue Service 48
3.3 SAFEGUARDING & PROMOTING THE INTERESTS OF CHILDREN & YOUNG
PEOPLE AFFECTED BY SUBSTANCE MISUSE 50
Our Early Years 50
Young People Error! Bookmark not defined.
3
3.4 PROVIDING SUPPORT TO INDIVIDUALS, IINCLUDING PARENTS AND
OLDER PEOPLE WITH ALCOHOL AND/OR DRUG RELATED PROBLEMS 58
Promoting Engagement in Treatment 58
Health & Social Care Integration 58
Improving the Quality of Services 58
Supporting Parents 62
Gender Based Violence 63
Reducing Re-offending 46
Older People 64
Supporting People with Alcohol Related Brain Injury 65
Blood Borne Viruses 44
Workforce Development Error! Bookmark not defined.
CHAPTER 4: OUR COMMISSIONING FRAMEWORK 2015 - 2018 67
4.1 THE COMMISSIONING CYCLE 67
Needs Assessment & Gap Analysis 67
Measuring success 68
Service Level Agreements & Performance Contracts 70
Monitoring & Review 70
4.2 FINANCIAL FRAMEWORK 71
CHAPTER 5: REFERENCES 72
4
FOREWORD
This strategy sets out the Lanarkshire Alcohol & Drug Partnership’s (ADP) approach
to tackling alcohol and drug related problems, both of which can be inextricably
linked to health inequalities. Tackling health inequalities is recognised as one of the
major policy challenges and requires action on the spectrum of determinants of
health (including education, employment and economic factors, physical and social
environments, and the quality and shape of services).
In writing our strategy and delivery plan for 2015-2018 we have taken a life course
perspective. We have also retained the three primary aims of our previous
strategies, as a result of consultations with a wide range of stakeholders, including
service users and their families. By reviewing a number of local and national reports
we have assessed how far we are away from providing services that have a focus on
reducing inequalities and are delivered in line with best practice.
The Scottish Government has agreed that ADP earmarked funding allocations to
support alcohol and drug outcomes will continue from April 2015, once health and
social care integration arrangements for adult services are in place. We have
therefore worked with our local shadow Integrated Partnerships during 2014-15 to
ensure our Strategy and Delivery plans are embedded within Health and Social Care
arrangements.
As the policy environment continues to evolve and the evidence base expands, our
Strategy and Delivery Plans will be subject to ongoing review and refinement to
ensure they continue to fit with national and local priorities. We will also continue to
work closely with the various public protection forums within Lanarkshire to reduce
harm and promote well-being whilst recognising the need to address the adverse
impact of substance misuse on individuals, their children, other family members and
the broader communities in which they live.
I take this opportunity to thank everyone for their generous and invaluable
contributions to the development of this strategy. I hope we have listened well and
understood what you have said. In so doing I acknowledge, like the recovery
process itself, that it reflects a challenging landscape which needs passion,
commitment, enthusiasm and hope to implement and drive forward.
Colin Sloey
ADP Chair
5
Executive Summary
Taking Forward the National Strategies in Lanarkshire
The national alcohol and drug strategies continue to provide the framework for
delivering alcohol and drug prevention, treatment and support services in
Lanarkshire. The Lanarkshire ADP is responsible for implementing these national
alcohol and drug strategies within each of our local authority areas. This strategy
therefore replaces the ADP previous strategies and delivery plans and focuses on
achieving the following three aims.
Our Aims
1 Promoting the development of a recovery orientated system of care within our
communities
2 Safeguarding and promoting the interests of children and young people
affected by substance misuse
3 Supporting adults, including parents and older people with alcohol and/or drug
related problems
As such we will continue to develop a recovery orientated system of care which has,
at its heart, the needs of individuals, their children and other family members
affected by alcohol and drug problems.
The life course perspective refers to an approach which recognises the structural,
social, and cultural contexts in which we live and work. In doing so it reflects the
importance of our early years and how this impacts on a range of other health and
social indices. Additionally therefore we will strive to promote health and well-being
within our wider communities by tackling the underlying root causes of alcohol and
drug problems, including trauma, socio-economic deprivation, family breakdown,
poverty, mental ill-health and crime.
The continued investment by the Scottish Government of £6,859,148 earmarked
funds also provides an opportunity for our ADP to make considerable progress
towards achieving the national outcomes and ministerial priorities. There are also a
suite of national recovery indicators which form part of the national Drug and Alcohol
Information System (DAISy) database which are expected to become available in
2016. We will therefore work in partnership with our local statutory and third sector
providers to ensure that these are included within our service level and partnership
agreements in order that we can measure the recovery outcomes for all clients
within our treatment and care services.
In developing this strategy we have included the views of service users, their family
members, staff working within our treatment and care services, members of our third
sector and community groups as well as other key ADP partners (housing, mental
health, criminal justice, education, social work and police). We have also reviewed a
number of local plans and national strategies to ensure that we are reflecting the key
priorities of our community planning partners.
The Community Plans and Single Outcome Agreements for both North and South
Lanarkshire Councils outline the priorities for Lanarkshire's citizens and communities
in the future. These are the overarching strategy documents which link to the
priority outcomes we hope to achieve. We have reflected these priorities within our
6
strategy and will work with our community planning partners over the next three
years to report on our progress. Further information on how this will be achieved is
included in our Delivery Plans for North and South Lanarkshire (2015 – 2018).
Our Key Priorities for 2015 - 2018
1. Promoting the development of a recovery orientated system of care
within our communities by:
Ensuring that care pathways for adults in distress are improved and that
there are appropriate systems in place within primary care, our acute
hospitals, ambulance and police services which offer compassionate support.
Aligning peer support and mutual aid opportunities to existing support
structures which promote mental well-being within each of our local towns
and villages.
Ensuring that family members who experience a problem are offered support
in their own right.
Embedding the implementation of alcohol brief interventions within our
primary care, mental health, midwifery and acute services and expanding this
provision within our most deprived communities, criminal justice and police
custody suites.
Working with our community safety partners to reduce the impact of health
inequalities and crime.
Ensuring offenders have access to a full range of supports which will increase
their recovery capital and enhance their emotional well-being.
2. Safeguarding and promoting the interests of children and young
people affected by substance misuse by:
Retaining a focus on improving the lives of children and young people
affected by substance misuse. This will include work to support
parents/prospective parents with drug or alcohol problems to understand the
importance of good attachment with their children.
Continuing to improve outcomes for pregnant women/new mothers with
substance misuse issues and their families.
Maintaining support for grass roots initiatives that use a range of
interventions to engage young people and tackle inequalities.
Fully implementing the delivery of alcohol brief interventions within youth
settings
Continuing to deliver the Strengthening Families Programme within the North
Lanarkshire Council area and expand and roll the programme into South
Lanarkshire
Increasing support for those young people who have complex issues including
substance use and mental health problems related to trauma and attachment
issues as well as increasing multi-agency training, consultation and care
planning around this same group of young people
Maintaining support for young people who, on release from custody are able
to re-integrate fully into community life.
Exploring and developing systemic and family therapeutic work.
7
3. Providing support to individuals (including parents, prisoners and older
people), with alcohol and/or drug related problems by:
Promoting engagement in treatment and care services by enhancing
motivation, building psychological resources and skills which foster
community links.
Commissioning evidence based psychological therapies which are trauma
informed.
Having a renewed emphasis on health and well-being outcomes within our
health and social care provision.
Improving the quality of service provision and the use of a validated recovery
outcome tools, including the Drug & Alcohol Outcome Star, to measure
progress over time.
Expanding the use of the Promoting Well-being Assessment, Strengthening
Families and Solihull approach within our alcohol and drug services.
Safeguarding the most vulnerable members of our communities including
those who continue to experience problems in later life.
8
CHAPTER 1: INTRODUCTION
1.1 INTRODUCTION
The Road to Recovery drugs strategy, Changing Scotland’s Relationship with Alcohol,
the National Delivery Framework and the Quality Alcohol Treatment and Support
(QATS) reports continue to provide the framework for delivering alcohol and drug
prevention, treatment and support in Lanarkshire. The Getting Our Priorities Right
(GOPR) guidance also provides an updated good practice framework for all child and
adult service practitioners working with vulnerable children and families affected by
problematic parental alcohol and/or drug use.
This guidance has been updated to reflect the Recovery agenda and the Getting It
Right for Every Child (GIRFEC) approach, both of which have a focus on ‘whole
family’ recovery, as well as aligning with the Children and Young People (Scotland)
Act 2014 which is central to the Scottish Government’s aim of making Scotland the
best place to grow up in.
About Us
Alcohol & Drug Partnerships (ADPs) were established in each Community Planning
area in 2009 in response to a Scottish Government review of Alcohol & Drug Action
Teams (ADATs). Under this national framework, ADPs are responsible for developing
local strategies for tackling alcohol and drugs misuse that are based on: a robust
assessment of needs in their area; a transparent, evidence-based process for
agreeing how funds should be deployed; and a clear focus on the outcomes that this
investment is achieving within our two local health and social care partnerships and
local communities. Our ADP includes the following organisations:
Our key responsibilities are therefore to develop, drive and secure the delivery of a
Lanarkshire wide Strategy on drug and alcohol problems, whilst incorporating the
local landscape of North and South Lanarkshire’s Community Planning structures
within our Delivery Plans for 2015 - 2018.
Our Support Team
We are supported by a small dedicated team of staff, who work across a range of
organisations within North and South Lanarkshire Community Planning Partnerships.
The ADP Support staff (see Figure 1) are responsible for the co-ordination of relevant
needs assessment, the contractual elements of commissioning and monitoring the
quality and outcomes of purchased services.
9
Figure 1: ADP Support Team
ADP Co-ordinator
Development Officer Information & Research
(North Lanarkshire) Officer (North Lanarkshire) Admin & Information
& & Officer
Development Officer Information & Research
(South Lanarkshire) Officer (South Lanarkshire)
Personal Secretary
Our support staff also update our website (www.lanarkshireadp.org) to ensure that it
continues to be a helpful resource to service users, their families, professionals
working within our services and the general public.
Our Consultation Process
For this Strategy we have consulted with a wide range of partners, including service
users and their families. Key elements of this process included:
Audits of our statutory and third sector existing service providers against the
national Quality Principles for Substance Misuse Services. This included
surveying the views of one hundred clients attending local services and fifty
clinicians who work within them, as well as case note and environmental
reviews.
Qualitative interviews with fifty-eight people who had failed to engage with
existing services, including, thirty-seven people attending mutual aid groups
(Alcoholics Anonymous, Cocaine Anonymous, Narcotics Anonymous, Al-Anon)
and twenty-one family members who participated in the Lanarkshire
Recovery Study (9)
Discussion with all ADP members and other key stakeholders within our
community planning structures
10 Focus groups with staff working in services and other key stakeholders
Consultation events to garner the views specifically from third sector and
community based groups
Following this strategic review we decided to retain one ADP across the Lanarkshire
Health Board area and have one Lanarkshire wide strategy. In order to reflect the
community planning priorities of North and South Lanarkshire Councils however we
decided to develop two Delivery Plans.
We spoke to over one hundred clients who attend our services,
thirty-seven who didn’t, twenty-one family members and fifty
clinicians and other staff groups. We have listened to what
you had to say. It is your voice that is reflected throughout
our strategy. We have used case studies to illustrate our
progress and our priorities for the next three years.
Adopting a Life Course Perspective
Causes of inequalities are complex and known to be determined by social, economic
and environmental conditions that people experience and live in. There are four
major models that describe social class inequalities in health, namely, behavioural,
material, psychosocial and life course perspectives. The life course perspective
refers to an approach which recognises the structural, social, and cultural contexts in
which we live and work. In doing so it reflects the importance of our early years and
how this impacts on a range of other health and social indices. These indices
included life expectancy, general health, unemployment and incapacity, income and
poverty levels, rates of sexually transmitted diseases, teenage pregnancy, the
prevalence of alcohol and drug related problems and feelings of mental well-being.
Thus, the way in which we live our lives are in large part influenced by our early
years.
Our strategy therefore recognises the impact of adverse childhood events and their
relationship to the development of emotional, behavioural and mental health issues,
including the development of alcohol and drug problems. Supporting children, young
people and their parents will therefore continue to be a key part of our strategy over
the next three years.
As alcohol and drug prevalence rates feature strongly within our most deprived
populations, in supporting adults, prisoners and older people who have developed a
problem we also recognise the importance of providing a range of supports which
provide access to early and psychological interventions, parenting support, mutual
aid, community prescribing, stable housing, employment, training and the
opportunity to engage in meaningful activities within our local communities.
111.2 OUR VISION
The national drug and alcohol strategies set out a vision where all alcohol and drug
treatment and care services were based on the principle of recovery. Over the past
seven years we have worked hard to deliver this vision, but we are not there yet.
We will therefore continue to work towards making sure that we have recovery-
focused outcomes in all of our services to ensure that the lives of individuals, their
children, other family members and communities affected by alcohol and drugs are
improved. Thus our vision reflects and underpins the higher level national outcomes
of our Community Planning Partners.
Working together to improve the quality of life for everyone affected by
alcohol and drugs living in Lanarkshire
Our Commitment
In pursuit of this vision, and central to our philosophy, will be the following
commitments:
We will focus on promoting health and well-being by tackling the underlying root
causes of alcohol and drug problems, including trauma, socio-economic
deprivation, family breakdown, poverty, mental ill-health and crime.
We will continue to develop a recovery orientated system of care which has, at
its heart, the needs of individuals, their children and other family members
affected by alcohol and drug problems
1.3 DELIVERING OUR VISION IN PARTNERSHIP
Community Planning provides a tool for bringing local statutory authorities and other
bodies together in partnership. As such we will work to achieve this Strategy’s aims
and objectives via our contribution to the new Community Planning arrangements,
including Health and Social Care Partnerships, Community Safety, Health &
Wellbeing, Children & Young People, Adult & Child Protection Committees and other
key structures and partnerships across both North and South Lanarkshire Council
areas.
As outlined in our Delivery Plans for North and South Lanarkshire (2015 – 2018)
(4,5) we have prioritised the areas for investment and identified the contributions
that each partner can make in realising that vision. These areas of investment link to
the priority themes of our community planning partners:
improving health and wellbeing
tackling inequalities and poverty
promoting sustainable, inclusive communities which provide opportunities for
all throughout life
reducing crime
12Links with Community Planning Structures
Health & Social Care Partnerships: Partnership arrangements in North and South
Lanarkshire have been developed in the context of the strategic direction set by the
Scottish Government via a considerable number of strategic and care group policy
documents. The Substance Misuse Planning & Performance Group in South
Lanarkshire and the Addiction Partnership Board in North Lanarkshire are responsible
for the implementation of the strategic direction set by Lanarkshire ADP and the
further development of the integrated health and social care delivery models within
their local areas as set out with the North & South Lanarkshire Delivery Plans for
2015 – 2018.
Children Young People and Families Affected by Substance Misuse Sub Group (North
Lanarkshire). The sub group is one of six thematic sub groups that feed into North
Lanarkshire’s Improving Children’s Services Group. The agenda of the sub group is
broad, covering topics that range from child protection to the importance of robust
transitional arrangements into adult services being in place. This helps to ensure a
continuum of care for children, young people and families affected by substance
misuse.
Children Affected by Substance Misuse Sub Groups (South Lanarkshire) The sub
group is one of a number of thematic sub groups that feeds into South Lanarkshire’s
Children’s Services Strategy Group. The purpose of this sub group has more of a
focus on those higher tariff young people who are affected by their own or someone
else’s substance misuse.
Life Etc. The Working Group is a partnership that comprises a range of stakeholders
from inter-related disciplines. These include NHS Lanarkshire, North and South
Lanarkshire Councils, Choose Life, Police Scotland, Scottish Fire & Rescue and the
voluntary and community sectors. The group ensures better joint planning and
delivery of overall health and wellbeing developments as opposed to working on
different themes in a “silo” fashion. The themes addressed through the work of the
group include the impact of alcohol, mental health, suicide prevention and the sexual
health and BBV agenda.
Lanarkshire Blood Borne Virus (BBV) Prevention & Care Network: The Lanarkshire
ADP works closely with the Lanarkshire BBV Prevention and Care Network which
leads and co-ordinates all work relating to blood borne viruses in Lanarkshire. The
Lanarkshire BBV PCN ensures that resources are used effectively and efficiently to
achieve the outcomes detailed in the Scottish Government’s Sexual Health and BBV
Framework1 specific to HIV, Hepatitis C and Hepatitis B across prevention, diagnosis,
treatment, care and support. The Lanarkshire BBV PCN is also responsible for the
delivery of Healthcare Improvement Scotland’s HIV Standards, Hepatitis C Quality
Indicators, and any other relevant new national BBV standards or guidelines across
the spectrum of BBV prevention, diagnosis, treatment, care and support.
ADP Working-Groups
Where there are gaps in existing community planning structures we will continue to
create working groups. There are ten themed working-groups, each focusing on
1
http://www.gov.scot/Publications/2011/08/24085708/0
13specific priorities (see Figure 2). These groups form part of the ADP governance
arrangements and help in both the development of quality improvement initiatives
and the contract monitoring processes:
Figure 2: ADP Sub-Groups
Alcohol & Drug Partnership
Board
Implementation &
Finance
Recovery New
Workforce Families & Child Protection
Commissioning Psychoactive Drug Deaths
Development Carers Forum Committee/ADP
Substances
Project Steering
Groups
Quality
Principles
Implementation and Finance Group
The ADP Board delegates the ADP Implementation and Finance Group to set out the
service priorities, and subject to approval by NHS Lanarkshire, to proceed with the
commissioning process. Membership of the ADP Implementation and Finance Group
is made up of senior representation from NHS Lanarkshire, South Lanarkshire
Council, North Lanarkshire Council and Police Scotland. The Implementation and
Finance Group are responsible for:
Co-ordinating and prioritising core business items ensuring that appropriate
actions and implementation plans are developed to deliver on the Lanarkshire
Alcohol and Drug Partnership Strategy (6) and Delivery Plans (2015 - 2018)
(7).
Commissioning and receiving reports to inform strategy development and
performance management.
Reviewing financial performance of all ADP funded services and those core
services delivered by NHS Lanarkshire, North and South Lanarkshire Councils
and Police Scotland respectively.
Reviewing and assessing the impact of new legislation and directives and
considering appropriate responses to the Scottish Government.
Ensuring effective delivery of ADP services, specifically those within NHS
Lanarkshire, North Lanarkshire Council and South Lanarkshire Council by
helping to overcome barriers in implementing policy or organisational
decisions.
Offering direction and advice to the ADP support team as required.
Commissioning Groups
These groups are created to ensure that there is a transparent and collective
decision making process in place by our partnership for commissioning any new
14services. The remit of these groups is to lead on the outcomes to be commissioned
and to participate in the short listing, interviewing and performance management of
relevant organisations. During the next three years we will ensure that we have
appropriate third sector representation on these groups and that the voices of
service users and their families are heard.
We also create steering groups for all commissioned services. The Steering groups
ensure that there is clear synergy with the ADP strategy and help to monitor
performance against agreed targets and outcomes detailed in the Service Level
Agreement whilst supporting any remedial activity where required.
Quality Principles Working Group
At a local level all ADPs have been tasked by the Scottish government to embed the
Quality Principles; Standard Expectations of Care and Support in Drug and Alcohol
Services (1) into routine clinical practice and ensure that they are incorporated into
their commissioning structures. The focus of this group is therefore to take forward
the findings of the Opiate Treatment Review (2013) (8) and the Scottish
Government’s intentions to develop an Alcohol and Drug Quality Improvement
Framework. Completed service audits and their associated improvement plans will
form part of the evidence base to support the Lanarkshire ADP’s self-assessment
framework towards achieving this aim.
The Scottish Drugs Forum’s Quality Improvement Team have offered support with
this process and have agreed to conduct client and staff surveys in South
Lanarkshire’s alcohol and drug services over the next three months. We have also
commissioned Stirling University to provide an external evaluation of the North
Lanarkshire Integrated Addiction Service.
Workforce Development
In developing our strategy we have been informed by the Scottish Government’s
Supporting the Development of Scotland’s Alcohol and Drug Workforce (9). The
Workforce Development Group focus on workforce planning issues for staff employed
within our Recovery Orientated Systems of Care. Workforce development is a
standing agenda item on our ADP board meetings. The Group also report directly
into the North Lanarkshire Addictions Partnership Board and South Lanarkshire’s
Planning and Performance Group for alcohol and drugs. Lanarkshire ADP recognises
that we have a responsibility to ensure that staff are suitably trained. A confident,
competent and well-supported workforce is of paramount importance if we are to
deliver good outcomes for our client group. We will therefore continue to fund a
range of training which supports our key aims.
15Families & Carers Working Group
This is a pan-Lanarkshire working group, with representation from Lanarkshire’s
substance misuse services, local carers’ organisations (including kinship and young
carers). The group have developed a local signposting resource for families,
particularly those “hidden” family members who are unlikely to come into contact
with services and instead try to deal with their problems within the family unit. The
pack contains information on the local supports available, information on
understanding dependency and talking to a loved one about their dependency.
Stories of family recovery are also featured in order to convey the message that
families and family members can and do recover.
Recovery Forum
We have recently established a pan-Lanarkshire recovery forum in an attempt to
bring people in recovery, current service users, local community groups and staff
who work in services together to discuss how we can improve our recovery
orientated systems of care. The forum provides a platform to share information,
providing a bridge between services and our local communities.
The ADP/Child Protection Committee Working
The ADP/Child Protection Committee Working Group includes ADP Development
officers, Child Protection Committee Coordinators and Lanarkshire Substance Misuse
Leads. This group focus on areas around workforce development, and improving
linkage between child/family services and adult substance misuse services. It should
be noted that both the North and South Lanarkshire Substance Misuse Workforce
Development Groups contain representation from child and adult services.
Developing A Strategic Approach to New Psycho-active Substances (NPS)
Emerging Trends Group
We have a well established Emerging Trends Group in Lanarkshire. The group
provides up to date information to ADP services on the different trends taking place
in Lanarkshire. A great deal of this information is harnessed through colleagues in
Police Scotland, presentations at A+E departments and service user disclosure at
Substance Misuse Services.
A consultation event on New Psychoactive Substances (NPS) has helped us to
prioritise actions for 2015 – 2018. These include greater collaboration between
Trading Standards, Police Scotland and local clinicians to create a greater
understanding on the impact of NPS on the user’s behaviour, clinical presentation
and methods of purchase. In addition we have prioritised opportunities for training
on NPS for school teachers, clinicians, staff who work with young people and
prisoners
Developing a Strategic Approach to NPS Enforcement
This group was established in January 2015 to review the current legal framework
available in tackling the sale and supply of NPS. The Group will take a practical and
operational approach to its work, drawing evidence from across a range of
professional boundaries and settings, including Trading Standards, Police Scotland,
16NHS Lanarkshire and our third sector and independent partners.
Drug Death Review Group
2013 DRD Annual report:
In 2013, 526 drug related deaths were registered in Scotland which was 9%
fewer than in 2012. Locally Lanarkshire reported a 28% increase in drug
related deaths, going from 53 in 2012 to 68 in 2013. This number includes
intentional self poisonings which have risen from 3 in 2012 to 9 in 2013.
The Drug Death Review Group is responsible for pulling local and national
information on drug related deaths (DRDs) as a means of identifying risk factors and
opportunities for reducing drug related deaths. A key local improvement target
within Lanarkshire is to provide Naloxone and overdose awareness training to staff,
clients and their families. In response to the recommendations made by the National
Forum on Drug Related Deaths, the Scottish Government commissioned the Scottish
Drugs Forum to assist ADPs in progressing the development of death prevention
strategy guidelines and to provide support with developing these strategies locally.
Following our conference last year we now have an action plan in place to take this
forward
The next chapter of our strategy provides a summary of the challenges we face in
implementing our strategy. It reviews the latest available data to show what
progress has been made in Lanarkshire in tackling the health and wider social issues
that are associated with problematic alcohol and drug use.
17CHAPTER 2: OUR CHALLENGE
2.1 LANARKSHIRE’S RELATIONSHIP WITH ALCOHOL
Levels of alcohol consumption in Lanarkshire, as in the rest of Scotland, are falling.
Fewer people are exceeding weekly drinking guidelines and the average number of
mean units consumed is falling, both for men and women (Figure 3).
Figure 3: Adherence to guidelines and mean alcohol consumption, Lanarkshire and
Scotland.
Source: Scottish Health Survey 2003-2013
Whilst this is a welcome trend it does mask a greater tendency in Lanarkshire to
exceed daily drinking guidelines, an indicator of binge drinking. 49% of men and
38% of women in Lanarkshire were found to exceed daily recommended limits (4
units for men, 3 units for women) on their heaviest drinking day. These are greater
than the Scottish averages (43% and 34% respectively) and are higher than any
other health board area in Scotland (11).
In general it appears that people struggle to understand the recommended unit
guidelines; the most recent Scottish Social Attitudes Survey (2013) (12) showed that
only around half of all adults in Scotland were able to correctly identify the number
of units in a pint of beer, measure of spirits or a glass of wine. Only around 2 of
18every 5 adults were able to correctly identify the recommended daily alcohol limits
and just one in five knew that guidelines recommend at least 2 alcohol-free days per
week.
There are some notable differences in trends in alcohol consumption amongst
different age and gender groups (Figure 4). Several years ago data suggested that
young men in Lanarkshire were drinking at worrying levels, approaching twice the
weekly consumption seen on average in Scotland. Similarly women in their 40s and
50s living in Lanarkshire were seen to be consuming more alcohol on average than
elsewhere in Scotland. Fortunately the latest data suggests that both these trends
appear to have improved and consumption levels in these groups are now much
more in line with national averages.
Figure 4: Mean alcohol consumption, Lanarkshire and Scotland, by age and gender
Source: Scottish Health Survey 2003-2013
Unfortunately the latest data also shows a significant increase in the levels of alcohol
consumed amongst older women in Lanarkshire. Whilst levels are currently within
the recommended guidelines the rate of increase in considerably greater than that
seen nationally and could suggest a worrying trend in the future.
Excessive alcohol consumption can affect both physical and mental health; it is
directly related to the incidence of the majority of chronic liver disease in Scotland
today. The burden to health and social care services is therefore considerable. In
Lanarkshire the rate of alcohol-related hospital stays currently exceeds that for
Scotland (Figure 5). The trend in the number of patients being admitted to hospital
for alcohol-related reasons has, for many years, followed a similar pattern to that
seen across Scotland. In recent years however Lanarkshire has seen a shift from the
19national trend; whilst the number of individuals being admitted to hospital has
continued to fall nationally, Lanarkshire has seen an increase in these figures. Rates
in South Lanarkshire continue to sit just under the national average but rates in
North Lanarkshire have now exceeded this.
Figure 5: Number of patients admitted to hospital with an alcohol-related diagnosis,
Lanarkshire and Scotland, as a rate per population
Number of patients admitted to hospital for alcohol-related reasons, rate per population
650
600
550
EASR per 100,000 population
500
450
400
350
300
250
200
1997/98 1998/99 1999/00 2000/01 2001/02 2002/03 2003/04 2004/05 2005/06 2006/07 2007/08 2008/09 2009/10 2010/11 2011/12 2012/13 2013/14
Scotland Lanarkshire North Lanarkshire South Lanarkshire
Deaths from alcohol-related causes have always been a particular problem in
Scotland when compared with other European countries. However, over the last
decade the number of alcohol-related deaths in Scotland has been falling; this trend
has been seen in Lanarkshire also (Figure 6).
Figure 6 Alcohol related deaths (underlying cause), Lanarkshire and Scotland, as a
rate per population
Alcohol-related deaths, as a rate per population
45
40
35
EASR per 100,000 population
30
25
20
15
10
1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013
Scotland Lanarkshire North Lanarkshire South Lanarkshire
20Despite this the rate of deaths directly attributable to alcohol-related causes such as
liver disease continues to be higher in Lanarkshire than in Scotland overall, and is of
particular concern in North Lanarkshire. There are differences in the rate of alcohol-
related death seen in men and women also; the rate of death from alcohol-related
causes is currently around twice as high in Lanarkshire males as in Lanarkshire
females (Figure 7).
Figure 7: Alcohol related deaths by gender (underlying cause), Lanarkshire and
Scotland, as a rate per population
Alcohol-related deaths, males vs females, as a rate per population
60
50
EASR per 100,000 population
40
30
20
10
0
1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013
Scotland - males Scotland - females
Lanarkshire - males Lanarkshire - females
This is not surprising given the greater consumption seen amongst men than
women. However in recent years we see that the rate of deaths is falling amongst
men in Lanarkshire at a similar rate to the rest of Scotland; unfortunately we have
not seen this same degree of improvement in the death rate amongst women.
212.2 OUR ROAD TO RECOVERY
Over the last 15 years there has been a general downward trend in problematic drug
use in Scotland; the national estimated drug prevalence rate has fallen from 2% of
the population in 2000 to 1.68% in 2012 (Figure 8).
Figure 8: Estimated prevalence rate of problematic drug use in Lanarkshire and
Scotland
Estimated prevalence rate of problem drug use
2.5
2.0
Prevalence rate (%)
1.5
1.0
0.5
0.0
2000 2003 2006 2009 2012
Scotland Lanarkshire North Lanarkshire South Lanarkshire
Source: Estimating the national and local prevalence of problem drug use in Scotland,
2000-2012
This trend has also been seen in South Lanarkshire which has seen a fall in drug
prevalence from 1.9% in 2000 to 1.52% in 2012. Unfortunately this has not been
the case in North Lanarkshire where the rate has barely changed; 1.6% in 2000 and
1.64% in 2012. The most recent period has seen increases in the drug prevalence
rate in both North and South Lanarkshire; despite this the rates in both areas remain
below the Scottish average.
Drug prevalence rates vary greatly by age and gender; men are approximately 3
times more likely to engage in problematic drug use than women (Figure 9) (13).
The number of women estimated to use drugs at problematic levels is even less in
Lanarkshire than that seen in Scotland overall. Men between the ages of 25 and 34
are those most likely to engage in problematic drug use; estimated use amongst this
group is greater in Lanarkshire than the national average and is particularly high in
North Lanarkshire at more than 5%.
22Figure 9: Estimated prevalence rate of problematic drug use by age and gender in
Lanarkshire and Scotland
Estimated drug prevalence rate by gender Estimated drug prevalence rate by age group (males only)
3.0 6.0
2.5 5.0
Prevalence rate (%)
Prevalence rate (%)
2.0 4.0
1.5 3.0
1.0 2.0
0.5 1.0
- -
Males Females 15 - 24 25 -34 35 - 64
Scotland North Lanarkshire South Lanarkshire
Source: Estimating the national and local prevalence of problem drug use in Scotland,
2012/13
As with excessive alcohol use, drug use at both recreational and problematic levels
can have a number of serious knock on effects to both physical and mental health.
Whilst the number of people being admitted to hospital for drug-related reasons is
currently well below the national rate, over the last 4 years this figure has risen
considerably (Figure 10).
Figure 10 Number of patients admitted to hospital with a drug-related diagnosis,
Lanarkshire and Scotland, as a rate per population
Number of patients admitted to hospital with a diagnosis of drug-misuse, rate per population
100
90
80
70
EASR per 100,000 population
60
50
40
30
20
10
0
1997/98 1998/99 1999/00 2000/01 2001/02 2002/03 2003/04 2004/05 2005/06 2006/07 2007/08 2008/09 2009/10 2010/11 2011/12 2012/13 2013/14
Scotland Lanarkshire North Lanarkshire South Lanarkshire
The number of drug-related deaths has continued to rise in Lanarkshire whilst the
rate of deaths from drug-related causes in Scotland appears to have plateaued and is
now falling (Figure 11).
23Figure 11: Drug related deaths, Lanarkshire and Scotland, as a rate per population
Drug-related deaths as a rate per population
14
12
EASR per 100,000 population
10
8
6
4
2
0
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013
Scotland Lanarkshire North Lanarkshire South Lanarkshire
People using drugs at problematic levels can have very specific health needs;
injecting drug users are particularly susceptible to blood borne viruses, such as
Hepatitis C, through the use of shared injecting equipment. In Lanarkshire at
present there are somewhere in the region of 2100 people living with Hepatitis C of
which at least half will have become infected through using shared equipment. The
rates are falling however and options for treatment are improving (Figure 12).
Figure 12: Number of people reported as Hepatitis C antibody positive by year of
earliest positive specimen, Lanarkshire and Scotland, as a rate per population
Number of people Hepatitis C antibody positive, as a rate per population
50
45
40
Rate per 100,000 popualtion
35
30
25
20
15
10
5
0
2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013
Scotland Lanarkshire
Source: Health Protection Scotland, Surveillance Report, May 2014
242.3 YOUNG PEOPLE
In general young people in Scotland are using drugs and alcohol at lower levels than
in the past. The most recent data shows that the proportion of 15 year olds reporting
drinking regularly has fallen by more than 20% from 46% in 2000 to 19% in 2014
(Figure 13).
Figure 13: Proportion of 13 and 15 year olds reporting having an alcoholic drink in
the previous week, Lanarkshire and Scotland
Reported having an alcoholic drink in the last week
50%
45%
40%
35%
30%
15 year olds
25%
20%
15%
10% 13 year olds
5%
0%
2002 2006 2010 2014
Scotland North Lanarkshire South Lanarkshire
Source: Scottish Schools Adolescent Lifestyle and Substance Use Survey, 2000-2014
This pattern has been seen in Lanarkshire also; however in North Lanarkshire the
figure is higher than the Scottish average at 21%. Fewer young people in Scotland
now believe that is acceptable to get drunk at the weekends (18-29 year olds: 53%
in 2004 to 40% in 2013; Scottish Social Attitudes Survey) indicating that attitudes to
excessive alcohol consumption are changing.
Similarly the proportion of young people reporting having used drugs in the past
month has also fallen both in Scotland and Lanarkshire. Across Scotland the most
recent data shows that 9% of 15 year olds reported using drugs in the last month
(Figure 14). This was slightly higher in North Lanarkshire at 10% but, more
worryingly was significantly higher in the South with 12% of 15 year olds reporting
using drugs in the previous month. The drug prevalence rate would suggest that
problematic drug use amongst young people, particularly young males, poses a
greater problem in North Lanarkshire than other areas of Scotland.
25Figure 14: Proportion of 13 and 15 year olds reporting using drugs in the last month,
Lanarkshire and Scotland
Reported using drugs in the last month
30%
25%
20%
15%
15 year olds
10%
5%
13 year olds
0%
2002 2006 2010 2014
Scotland North Lanarkshire South Lanarkshire
Source: Scottish Schools Adolescent Lifestyle and Substance Use Survey, 2000-2014
The use of new psychoactive substances, commonly known as ‘legal highs’, presents
an expanding and worrying area for those with children and communities alike. In
Scotland approximately 1.9% of 15 year olds reported using a new psychoactive
substance in the last month. In Lanarkshire the figure was lower at 1.4%; however
this masks a difference in behaviour between young people in North and South
Lanarkshire. In North Lanarkshire just 0.7% of all 15 year olds are estimated to
have used a new psychoactive substance in the last month while in South
Lanarkshire this is estimated at 2.3%, higher than in Scotland overall.
2.4 INEQUALITIES: THE LINK BETWEEN DEPRIVATION & HEALTH
An accumulation of socio economic circumstances can cause inequalities particularly
in health. Areas that have a greater incidence of socioeconomic deprivation,
indicated by, among other things, lower employment rates and lower income often
have poorer health outcomes too. These inequalities affect parts of both North and
South Lanarkshire, but are particularly prevalent in North Lanarkshire; nearly 24% of
all data zones in North Lanarkshire fall within the 15% most deprived in Scotland
compared with 13.3% in South Lanarkshire (see Figure 15). This means that an
estimated 77,000 people are living in areas of multiple deprivation in North
Lanarkshire alone; a further 40,000 are living in deprivation in South Lanarkshire.
26Figure 15: Multiple deprivation in Lanarkshire by deprivation quintile.
The darkest areas show the areas of Lanarkshire that sit in the most deprived 20%
in Scotland; the lightest areas are in the least deprived 20% in Scotland
27A result of complex combinations of circumstances taking place over time (life
course) may impact on an individual’s health. Life course approach to inequalities is
explained by the chance of someone having good or poor health having been
influenced by events that had happened to them as far back as their childhood and
the cumulative effect of disadvantages that may have followed an individual through
their whole life from childhood to adulthood.
Higher rates of unemployment are seen in Lanarkshire with greater proportions
of working age people claiming benefits than overall in Scotland; again this is
more pronounced in North Lanarkshire than in the South. A greater proportion
of children and older people are affected by poverty and deprivation in North
Lanarkshire than in South Lanarkshire or in Scotland overall. Higher
unemployment rates may be linked to lower educational achievements; a lower
proportion of young people in Lanarkshire leave school with a positive
destination such as a job, apprenticeship or training opportunity to go to (Table
1).
Table 1: Indicators of employment, education and training
Percentage of people
Percentage of leavers from publicly
with low or no
funded secondary schools in positive
qualifications - 16-64
follow-up destinations (2012/13)
(2013)
Scotland 90.0% 12.6%
North Lanarkshire 87.9% 17.5%
South Lanarkshire 89.8% 13.1%
Similarly a greater proportion of the working age population have few or no
qualifications in Lanarkshire than elsewhere in Scotland (Table 1). It is perhaps not
surprising then that health outcomes are often worse than those seen nationally. For
example life expectancy in North Lanarkshire is approximately 2 years lower than the
average for Scotland; North Lanarkshire has the 5th worst life expectancy for men
and 3rd worst for women of all the local authority areas in Scotland (Table 2).
Table 2: Indicators of health: life expectancy, death rate and number of emergency
hospital admissions
European age- Emergency hospital
Life expectancy (2010-12)
standardised death rate admissions - both
per 100,000 population - sexes - all ages - rate
Male Female persons aged under 75 per 100,000 population
(2013) (2012)
Scotland 76.6 80.8 437.5 10,194
North
Lanarkshire 74.9 79.1 520 11,450
South
Lanarkshire 76.4 80.5 451.5 10,464
There can be differences between groups within the population too; for example
women in Lanarkshire rate their own physical health and mental wellbeing lower
than the national average while men score themselves virtually the same (Table 3).
28Table 3: Self-assessed physical and mental health (Scottish Health Survey, 2008-
2011)
Self-assessed physical health - Self-assessed mental
Prevalence of limiting long-
percentage rating health as good wellbeing - WEMBWS mean
term conditions (2008-11)
or very good (2008-11) scores (2008-11)
Male Female Male Female Male Female
Scotland 77% 75% 24% 29% 50.1 49.7
Lanarkshire 76% 72% 24% 32% 49.9 48.8
The outcomes for health issues related to alcohol and drug use are also worse in
those areas were greater socioeconomic deprivation is more prevalent. Rates of
alcohol-related death are far greater in more deprived areas of Lanarkshire than in
more affluent areas (Figure 16).
Figure 16: Alcohol-related deaths by deprivation, Lanarkshire and Scotland
140
Most deprived
- Lanarkshire
120
EASR (3-year moving average)
Most deprived
100 -Scotland
Lanarkshire
80
60 Scotland
40 Least deprived
- Lanarkshire
20
Least deprived
- Scotland
0
Similarly the majority of drug-related deaths occur in those areas with the greatest
levels of multiple deprivation (Figure 17).
29Figure 17: Drug-related deaths by SIMD quintile
140
120
100
Number of deaths
80
60
40
20
0
1 2 3 4 5
most deprived SIMD quintile least deprived
Source: SIMD 2012
2.5 COMMUNITY AND ENVIRONMENT
It’s not just individuals who are affected by problematic drug and alcohol use; whole
neighbourhoods can be affected through noise, vandalism and other antisocial
behaviour and crime. Local data suggests that the number of antisocial behaviour
incidents being reported has fallen quite significantly in recent years (Figure 18).
Figure 18: Number of antisocial behaviour incidents reported to police, Lanarkshire
Reported antisocial behaviour incidents
140,000
120,000
Number of reported ASB incidents
100,000
80,000
60,000
40,000
20,000
0
2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014
Lanarkshire North Lanarkshire South Lanarkshire
30Along with evidence of improved perceptions of own neighbourhood as a good place
to live (Figure 19) and a reduction in the proportion of people perceiving problems in
their neighbourhood (Figure 19) this would suggest the level of disturbance
associated with alcohol and drug use in Lanarkshire is decreasing.
Figure 19: Proportion of people reporting their neighbourhood as a very or fairly food
place to live, Scotland and Lanarkshire.
Proportion of people rating neighbourhood as good place to live
96
% rating nieghbourhood as v ery or fairly good
94
92
90
88
86
84
82
1999-2000 2001-2002 2003-2004 2005-2006 2007-2008 2009-2010 2012 2013
Scotland North Lanarkshire South Lanarkshire
Source: Scottish Households Survey
Figure 20: Proportion of people reporting these problems as very or fairly common in
their neighbourhood, Scotland and Lanarkshire.
Proportion of people perceiving neighbourhood problems as very or fairly common
25
% reporting problem as very or failry common
Scotland North Lanarkshire South Lanarkshire
20
15
10
5
0
2005-06 2007-08 2009-10 2012 2013 2005-06 2007-08 2009-10 2012 2013 2005-06 2007-08 2009-10 2012 2013
Vandalism Harrassment/intimidation Drug misuse or dealing Rowdy behaviour including drunkeness Noise
Source: Scottish Households Survey
Despite this the number of crimes reported where the perpetrator is reported as
being under the influence of alcohol remains high (data awaited).
31Licensing in Lanarkshire: assessing for overprovision
Both the affordability and availability of alcohol are important factors when
considering the harm that alcohol can have on individuals, neighbourhoods and
communities. There is a growing body of evidence that suggests a greater presence
of alcohol outlets can lead to increased alcohol consumption and associated alcohol-
related harm (1, 2). The presence of too many licensed premises within a specified
geographical area is known as overprovision. The Licensing (Scotland) Act states
that it is the duty of each Licensing Board to assess for overprovision within any
locality in the area covered by the Board. An analysis of local data relating to
licensed premises, alcohol-related health harm and alcohol-related crime was carried
out to assess for overprovision in local areas of Lanarkshire.
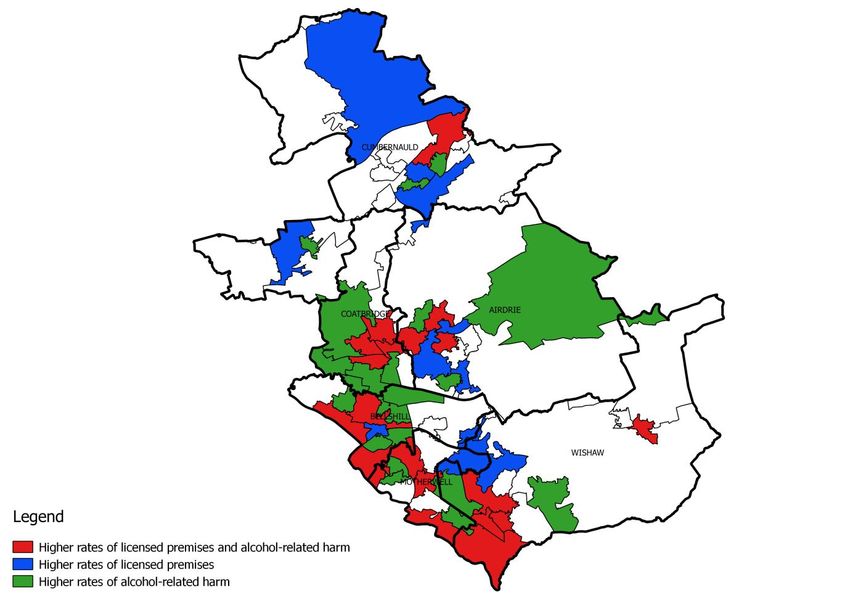
The analysis showed that a greater number of zones in North Lanarkshire had higher
rates of alcohol-related harm that were also associated with higher rates of licensed
premises (Figure 21) than in South Lanarkshire (Figure 22); 17 of these zones were
found in North Lanarkshire while 9 were found in South Lanarkshire.
Figure 21:
32However a significant proportion of zones with high rates of alcohol-related harm did
not have a higher than average number of licensed premises within the same
geographical zone. Travel and the popularity of online shopping make alcohol
consumption a more complex issue than simply the control of licensed premises
locally. Other issues such as local area socio-economic deprivation will also play a
significant part in rates of alcohol-related harm. Whilst the lack of a consistent
definition of overprovision makes assessment difficult, licensing boards should
consider local levels of alcohol-related harm and deprivation when considering new
license applications.
Figure 22:
33CHAPTER 3: WHERE ARE WE NOW?
3.1 INTRODUCTION
The Lanarkshire ADP 2012 – 2015 Strategy saw the introduction and consolidation of
a variety of initiatives to improve the lives of people who are affected by drug and
alcohol problems. This is the foundation on which we will build for 2015 - 2018.
Crucially however our new strategy will focus on a life course perspective (our early
years, our teenage years, adulthood (including parenthood and our later years)
which means that at every stage of life we have the right supports in place to help
people receive the right kind of interventions when and where they need it. In short
we want to ensure that there are individualised and comprehensive services across
the lifespan with supports, treatment and care services anchored in our local
communities. Thus we have a renewed emphasis on:
1. Promoting the development of a recovery orientated system of care
within our communities by:
Ensuring that care pathways for adults in distress are improved and that
there are appropriate systems in place within primary care, our acute
hospitals, ambulance and police services which offer compassionate support.
Aligning peer support and mutual aid opportunities to existing support
structures which promote mental well-being within each of our local towns
and villages.
Making sure that family members who experience a problem are offered
support in their own right.
Embedding the implementation of alcohol brief interventions within our
primary care, mental health, midwifery and acute services and expanding this
provision within our most deprived communities, criminal justice and police
custody suites.
Working with our community safety partners to reduce the impact of health
inequalities and crime.
Ensuring offenders have access to a full range of supports which will increase
their recovery capital and enhance their emotional well-being
2. Safeguarding and promoting the interests of children and young people
affected by substance misuse by:
Retaining a focus on improving the lives of children and young people
affected by substance misuse. This will include work to support
parents/prospective parents with drug or alcohol problems to understand the
importance of good attachment with their children.
Continuing to improve outcomes for pregnant women/new mothers with
substance misuse issues and their families.
Maintaining support for grass roots initiatives that use a range of
interventions to engage young people and tackle inequalities.
Fully implementing the delivery of alcohol brief interventions within youth
settings
Continuing to deliver the Strengthening Families Programme within the North
Lanarkshire Council area and expand and roll the programme into South
Lanarkshire
34 Increasing support for those young people who have complex issues including
substance use and mental health problems related to trauma and attachment
issues as well as increasing multi-agency training, consultation and care
planning around this same group of young people
Maintaining support for young people who, on release from custody are able
to re-integrate fully into community life.
Exploring and developing systemic and family therapeutic work.
3. Providing support to individuals (including parents, prisoners and older
people), with alcohol and/or drug related problems by:
Promoting engagement in treatment and care services by enhancing
motivation, building psychological resources and skills which foster
community links.
Commissioning evidence based psychological therapies which are trauma
informed.
Having a renewed emphasis on health and well-being outcomes within our
health and social care provision.
Improving the quality of service provision and the use of a validated recovery
outcome tools, including the Alcohol & Drug Outcome Star, to measure
progress over time.
Expanding the use of the Promoting Well-being Assessment, Strengthening
Families and Solihull approach within our alcohol and drug services.
Safeguarding the most vulnerable members of our communities including
those who continue to experience problems in later life
The rest of this chapter reflects our progress over the last three years and the
priorities which emerged during our consultation process for this strategy.
35You can also read

















































