Algorithm for laboratory diagnosis and treatment-monitoring of pulmonary tuberculosis and drug-resistant tuberculosis using state-of-the-art rapid ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Algorithm for laboratory diagnosis and treatment-monitoring of pulmonary tuberculosis and drug-resistant tuberculosis using state-of-the-art rapid molecular diagnostic technologies Expert opinion of the European Tuberculosis Laboratory Initiative core group members for the WHO European Region
Algorithm for laboratory diagnosis and treatment-monitoring of pulmonary tuberculosis and drug-resistant tuberculosis using state-of-the-art rapid molecular diagnostic technologies Expert opinion of the European Tuberculosis Laboratory Initiative core group members for the WHO European Region
Keywords
TUBERCULOSIS, PULMONARY
– DIAGNOSIS
TUBERCULOSIS, MULTIDRUG- © World Health Organization 2017
RESISTANT – DIAGNOSIS All rights reserved. The Regional Office for Europe of the World
CLINICAL LABORATORY TECHNIQUES Health Organization welcomes requests for permission to reproduce
DIAGNOSTIC TECHNIQUES AND or translate its publications, in part or in full.
PROCEDURES
EUROPE The designations employed and the presentation of the material in
this publication do not imply the expression of any opinion whatsoever
on the part of the World Health Organization concerning the legal
ISBN 978 92 890 5237 5 status of any country, territory, city or area or of its authorities, or
concerning the delimitation of its frontiers or boundaries. Dotted
lines on maps represent approximate border lines for which there
Address requests about publications of may not yet be full agreement.
the WHO Regional Office for Europe to:
The mention of specific companies or of certain manufacturers’
Publications products does not imply that they are endorsed or recommended by
WHO Regional Office for Europe the World Health Organization in preference to others of a similar
UN City, Marmorvej 51 nature that are not mentioned. Errors and omissions excepted, the
names of proprietary products are distinguished by initial capital
DK-2100 Copenhagen Ø, Denmark letters.
Alternatively, complete an online
request form for documentation, All reasonable precautions have been taken by the World Health
health information, or for permission Organization to verify the information contained in this publication.
to quote or translate, on the Regional However, the published material is being distributed without warranty
Office website (http://www.euro.who. of any kind, either express or implied. The responsibility for the
int/pubrequest). interpretation and use of the material lies with the reader. In no event
shall the World Health Organization be liable for damages arising
Cover graphic: Venomous Vectors, from its use. The views expressed by authors, editors, or expert
Shutterstock groups do not necessarily represent the decisions or the stated policy
Photo page vi: Paulista, Shutterstock of the World Health Organization.Contents
Acknowledgements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . iv
Acronyms. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . iv
Abstract. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . v
Introduction. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
Principles of laboratory diagnosis of TB. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
Prerequisites of a good laboratory network. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
Algorithms for laboratory diagnostic and follow up of TB cases. . . . . . . . . . . . . . . . . . . . . . 8
Algorithm for the initial laboratory diagnosis of individuals with symptoms
consistent with pulmonary TB. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
Algorithm for monitoring the follow-up of patients with drug-sensitive pulmonary TB. . . . . 11
Algorithm for the monitoring of follow-up of MDR-TB and RIF-resistant patients. . . . . . . . . . 13
Practical considerations for the diagnostic algorithm . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
Diagnostic methods of preference. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
Interpretation and reporting of laboratory results. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
References. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
Annex 1. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26Acknowledgements
This technical document was developed as a collaborative product by the European Tuberculosis Laboratory
Initiative (ELI) core group members. Document development was guided by Dr Masoud Dara (WHO Regional
Office for Europe) and led by Dr Soudeh Ehsani (WHO Regional Office for Europe), with ELI core group members
Professor Francis Drobniewski (Imperial College London, United Kingdom), Dr Irina Felker (Novosibirsk
Tuberculosis Research Institute, WHO National Centre of Excellence, Russian Federation), Dr Sven Hoffner (the
Public Health Agency of Sweden, Supranational Reference Laboratory Stockholm), Dr Gulmira I. Kalmambetova
(National Reference Laboratory, Kyrgyzstan), Dr Hasmik Margaryan (Tuberculosis Laboratory Expert,
Armenia), Mr Evgeni Sahalchyk (IML red GmbH, Supranational Reference Laboratory Gauting, Germany), Dr
Elina V. Sevastyanova (Central Tuberculosis Research Institute, WHO National Centre of Excellence, Russian
Federation), Dr Natalia Shubladze (Laboratory Consultant, National Centre of Tuberculosis and Lung Diseases
and the National Reference Mycobacteriology Laboratory, Georgia), Ms Nukra Sinavbarova (National Public
Health Laboratory, Tajikistan), Dr Alena Skrahina (Republican Research and Practical Centre for Pulmonology
and Tuberculosis, Belarus), Dr Rasim Tahirli (WHO Collaborating Centre on Prevention and Control of
Tuberculosis in the Penitentiary System, Azerbaijan) and former ELI core group secretariat Dr Kristin Kremer
and former ELI core group member Dr Sabine Rüsch-Gerdes (Senior WHO consultant).
Technical inputs and/or review were provided by Dr Christopher Gilpin (WHO headquarters), Mr Wayne Van
Gemert (WHO headquarters) and regional Green Light Committee members Dr Gunta Dravniece (Senior
Consultant, Access to Care Team, Technical Division, KNCV Tuberculosis Foundation) and Dr Elmira Gurbanova
(WHO Collaborating Centre on Prevention and Control of Tuberculosis in the Penitentiary System, Azerbaijan).
Development and publication of the document were enabled with financial support from the United States
Agency for International Development.
Acronyms
CM common mycobacteria MTB Mycobacterium tuberculosis
CRI colorimetric redox indicator MUT mutant
CrI credible interval M/XDR-TB multidrug and extensively drug-
DR-TB drug-resistant tuberculosis resistant tuberculosis
DST drug-susceptibility testing NRA nitrate reduction assay
ELI European Tuberculosis Laboratory NRL National Reference Laboratory
Initiative NTM non-tuberculous mycobacteria
ESTC European Union Standards for PCR polymerase chain reaction
Tuberculosis Care pDST phenotypic drug susceptibility
FL first-line testing
FLQ fluoroquinolone PPV positive predictive value
gDST genotypic DST R resistant
INH isoniazid RIF rifampicin
ISTC International Standards for RRDR Rifampicin Resistance Determining
Tuberculosis Care Region
LAMP loop-mediated isothermal S susceptible
amplification SL second-line
LED light-emitting diode SLID second-line injectable drug
LJ Löwenstein-Jensen TB tuberculosis
LPA line probe assay WT wild type
MDR-TB multidrug-resistant tuberculosis XDR-TB extensively drug-resistant
MGIT mycobacteria growth indicator tube tuberculosis
MIC minimal inhibitory concentrations
MODS microscopic-observation
drug-susceptibility
ivABSTRACT
The European Tuberculosis Laboratory Initiative (ELI), with its
secretariat at the WHO Regional Office for Europe, has developed
this technical document to address the need in the WHO European
Region for increasing timely and accurate detection of tuberculosis
(TB) and multidrug-resistant TB (MDR-TB) through scaling-up the
appropriate use of WHO-recommended rapid molecular diagnostic
techniques. The document presents comprehensive algorithms for
diagnosis and treatment-monitoring of pulmonary TB and MDR-TB
using rapid molecular techniques recommended by WHO. With
strong commitment of the Member States and continuous support
from donors and partners, most techniques have already been
introduced to the majority of countries of the Region, particularly in
the high MDR-TB burden countries. However, to yield the maximum
benefit of each technique, the appropriate and accurately timed
sequence of different laboratory tests and correct interpretation and
communication of results between laboratories and clinicians need to
be ensured. For effective operation and efficient outcomes, sustainable
financial and human resources need to be directed towards increasing
testing capacities and optimizing sample transportation and data
communication. This document aims to address these issues, taking
the challenges and opportunities of the countries of the Region into
account.
vIntroduction
Introduction
Tuberculosis (TB) accounts for over 40% of all
mortality cases from communicable diseases in
the WHO European Region and is the most common
cause of death among people living with HIV (1, 2)
Although the WHO European Region accounts for less than 5% of TB cases
worldwide, about 25% of the worldwide burden of multidrug-resistant TB
(MDR-TB) occurs in this Region (3).
Of the 30 countries classified as high MDR-TB burden countries, nine are in the
European Region (Azerbaijan, Belarus, Kazakhstan, Kyrgyzstan, the Republic of
Moldova, the Russian Federation, Tajikistan, Ukraine and Uzbekistan). The Region
includes 18 high TB priority countries, as defined in 2008 (3, 4), and 99% of the
MDR-TB cases in the Region occur in these countries (5).
Of the 30 countries classified as high MDR-TB
burden countries, nine are in the European
Region (Azerbaijan, Belarus, Kazakhstan,
Kyrgyzstan, the Republic of Moldova, the
Russian Federation, Tajikistan, Ukraine and
Uzbekistan). The Region includes 18 high TB
priority countries, as defined in 2008, and 99%
of the MDR-TB cases in the Region occur in
these countries.
1Algorithm for laboratory diagnosis and treatment-monitoring of pulmonary tuberculosis and drug-resistant tuberculosis using state-of-the-art rapid diagnostic technologies
The Region includes high-, middle- and low-income countries with diverse national
health system structures for TB control activities. Latest data from the Region
on MDR-TB prevalence amount to 16% among new TB cases and 48% among
previously treated cases (3, 6). Extensively drug-resistant TB (XDR-TB) is estimated
to occur in 23.4% of all MDR-TB cases subjected to second-line drug-susceptibility
testing (DST) (6). In 2015, treatment success rates were at 76% in new and relapse,
63% in previously treated (excluding relapses) and 51% in rifampicin-resistant/
MDR-TB cohorts (6). In 2015 with the development of an ambitious post-2015 global
End TB Strategy, to continue the progress and address the challenges in TB and
M/XDR-TB detection, prevention and care, the Regional Office developed the TB
action plan for the WHO European Region covering the period 2016–2020 (5, 6, 8).
Much work needs to be done to reach the targets set in the 2016–2020 action plan
for the laboratory diagnosis of TB in the Region, particularly in the appropriate
use of molecular diagnostics, and increasing the MDR-TB case-detection rate and
coverage of quality-assured second-line DST among MDR-TB cases. Currently
about 311 910 TB cases are registered in the 51 reporting countries of the Region
(6). Bacteriological confirmation of TB diagnosis was reported for 61.4% of all new
and relapse pulmonary cases in the Region and in four countries this was below
50% (5, 6). Only 57.9% of an estimated 74 000 MDR-TB cases were detected, against
a regional target of diagnosing at least 85% (6, 8).
Coverage of rifampicin (RIF)-resistance testing among laboratory-confirmed
pulmonary TB cases amounted to 44% of new cases and 49% of previously
treated cases in 2015. Coverage of second-line DST among laboratory confirmed
drug-resistant TB cases was 52.2% (3). Although DST coverage has improved
significantly, scale-up of testing and the use of WHO-recommended rapid
molecular tests are urgently needed to reach the target of performing DST for
close to 100% of all laboratory-confirmed cases by 2020. More directive guidance
and advocacy is also needed to address gaps in the laboratory diagnosis of TB in
the Region, especially in the nine high MDR-TB burden countries.
In response to the need to strengthen TB laboratory capacity for accurate diagnosis
and early detection of drug-resistant TB (DR-TB) in the Region and ensure
implementation of the regional action plans (8, 9), the WHO Regional Office for
Europe established the European Tuberculosis Laboratory Initiative (ELI) in 2012
(10). The mission of ELI is to strengthen TB laboratory capacity in the Region, with
a focus on the 18 high TB priority countries. ELI members consist of national and
2Introduction
international TB laboratory experts in the
Only 57.9% of an estimated
Region and international partners dedicated
to accelerating and expanding access to 74 000 MDR-TB cases were
quality-assured TB diagnostic laboratory
services. ELI has a core group of members detected, against a regional
who function as an independent, technical
advisory and support group for WHO and
target of diagnosing at
partners (10).
least 85%
ELI has been working to develop a
diagnostic algorithm, taking into consideration the substantial heterogeneity
of the Region. The algorithm combines different types of tests synergistically
by targeting patient groups appropriately and will help to make the best use of
available resources by maximizing their respective strengths and mitigating
their weaknesses (11, 12). The draft algorithm developed by the previous core
group members (2012–2014) was revised during and after the last ELI core group
meeting, held in Copenhagen, Denmark on 25 February 2016 (13). The algorithm
was finalized and agreed by members during the ELI core group meeting in Tbilisi,
Georgia on 30 November and 2 December 2016 and is presented here.
The recommendations presented here take into account and supplement
previously published recommended standards for modern TB laboratory services,
including the WHO global policy framework on implementing TB diagnostics and
the European Union Standards for Tuberculosis Care (ESTC) and International
Standards for Tuberculosis Care (ISTC) (11, 14, 15). The ESTC adapted the ISTC (14) to
reflect the European Union setting and practices (11). The ESTC builds on previous
recommendations on laboratory methods for diagnosing TB (16) to propose that:
In countries, settings or populations in which MDR-TB is suspected in a patient, rapid
testing for the identification of rifampicin- and isoniazid-resistance, using validated
tools in a quality-assured laboratory, should be performed.
To reassure rapid diagnosis of TB in the entire Region, ELI suggests further
extension of this standard by using rapid molecular diagnosis as an initial
method for all cases with clinical suspicion of TB, to be applied in all countries
of the Region. With high MDR-TB rates being present in Eastern Europe, every
presumptive TB case could also be an MDR-TB case.
3Algorithm for laboratory diagnosis and treatment-monitoring of pulmonary tuberculosis and drug-resistant tuberculosis using state-of-the-art rapid diagnostic technologies
Principles of laboratory
diagnosis of TB
Laboratory diagnosis of TB should start with
appropriate clinical screening procedures to
identify individuals with clinical suspicion of TB
Specific laboratory policies and diagnostic algorithms should be available at
country level based on the local epidemiological situation; limited resources initially
will mean that not all the required improvements can be implemented immediately,
but resource limitation should not influence the recommendation, only the rate at
which the recommendation is implemented.
WHO-endorsed rapid diagnostic tests should be key to the diagnostic work-up for
all TB presumptive cases (17). Countries shall prioritize the use of recommended
rapid molecular tests, rather than conventional microscopy, culture or DST, as
the initial diagnostic test for adults and children presumed to have pulmonary TB/
MDR-TB and/or HIV-associated TB and/or TB meningitis (17). This will ensure the
availability of early and accurate diagnosis. Conventional microscopy should be
used as an initial diagnostic test only in laboratory settings without rapid molecular
tests and in the absence of systems for timely sample transportation to a setting in
which these techniques are available.
In settings with high risk of transmission of TB and/or MDR-TB, such as prisons
in countries of the former Soviet Union, implementation of sputum polymerase
chain reaction (PCR)-based screening (GeneXpert MTB/RIF assay) as an annual
screening tool has been shown to most cost-effectively reduce TB and MDR-TB
when compared to more traditional interventions (18).
4Principles of laboratory diagnosis of TB
In the event of discrepancies between the
WHO-endorsed rapid
results of conventional and molecular
assays, it is recommended that the diagnostic tests should be
respective tests be repeated on the
same or another sample from the same key to the diagnostic work-up
patient to exclude technical errors. If
the discrepancy between microscopy
for all TB presumptive cases
and molecular tests is confirmed, the
laboratory shall report the molecular test result to the clinician instead of the
microscopy result due to the higher sensitivity and specificity of molecular tests
compared to microscopy. If the culture becomes positive after initial molecular
and microscopy tests were negative, this positive culture result should be reported
as well (as this reflects the proportion of samples for which culture remains the
most sensitive test). The proposed table in Annex 1 has been developed to help the
interpretation and explanation of all potential discordant results that may occur,
although most of these cases will be observed very rarely. The table will also assist
laboratories to explain discrepant or conflicting results to clinicians.
5Algorithm for laboratory diagnosis and treatment-monitoring of pulmonary tuberculosis and drug-resistant tuberculosis using state-of-the-art rapid diagnostic technologies
Prerequisites of a good
laboratory network
Countries should have sufficient funding
and appropriately trained human resources
available for laboratories, as well as a laboratory
maintenance and development plan (19)
Laboratories should have appropriate infrastructure, biosafety measures,
equipment, and access to regular maintenance of equipment and infrastructure.
Laboratory commodities and supplies should be managed well and laboratory data
properly recorded, preferably in an electronic format. Ideally, the laboratory would
have a clear and separate budget line within the programme/hospital budget.
Specimen transportation and referral mechanisms within a laboratory network
should be well described, with clear transportation arrangements in place. Patient
specimens kept in appropriate secure containers can be transported using most
health-care vehicles to increase transport frequency and reduce delay; the quality
of the specimens arriving should be monitored (15, 20, 21). A laboratory quality
management system in line with WHO recommendations should be in place.
The laboratory work-up of a clinical sample should be defined by the patient’s
category (new, relapse or previously treated case), the purpose of the analysis (for
diagnosis or treatment success) and the patient’s risk assessment (HIV, or risk of
MDR-TB, for instance). This information is to be recorded on the laboratory request
form together with the laboratory tests to ensure that the most appropriate,
efficient and cost-effective laboratory work-up is achieved, and to facilitate result
6Prerequisites of a good laboratory network
interpretation – in the case of discordant Similarly, line probe assays
results – and communication between
clinical doctors and laboratory staff. (LPAs) should be placed
Frequent repetitions of DST are usually
unnecessary and often not helpful. Once a at regional and central
patient has been shown to have MDR-TB, for
example, subsequent repetition of isoniazid
reference level laboratories,
(INH) and RIF testing will be unhelpful. because of the complexity
An updated manual detailing of the assay and required
recommendations for biosafety was
published in 2012 by WHO (22). The infrastructure
current recommendations are based on
assessments of the risks associated with different technical procedures performed
in different types of TB laboratories. It is recommended that culture and DST
be used only in laboratories at regional and central reference level that have
appropriate biosafety standards (22).
Similarly, line probe assays (LPAs) should be placed at regional and central
reference level laboratories (or any laboratory currently performing not automated
PCR-based amplification methodologies for infections, as the infrastructure will be
the same) because of the complexity of the assay and required infrastructure (23).
Many countries in the Region follow the principle of patient (instead of specimen)
referral to confirm the diagnosis of TB at specialized TB centres or hospitals. By
using WHO recommended rapid molecular techniques for the initial diagnosis of TB
and MDR-TB at district or subdistrict level (24, 25), a highly specific diagnosis of TB
can be achieved at a lower level in the health system, which can help countries to
reduce diagnostic delay, apply the most appropriate infection control measures and
simultaneously move towards ambulatory treatment of TB cases (9).
7Algorithm for laboratory diagnosis and treatment-monitoring of pulmonary tuberculosis and drug-resistant tuberculosis using state-of-the-art rapid diagnostic technologies
Algorithms for
laboratory diagnostic
and follow up of TB
and MDR-TB cases
Three algorithms are proposed in this document:
1. for the initial diagnostics of all presumptive TB cases
2. for follow-up of patients under first-line anti-TB treatment
3. for follow-up of MDR-TB patients (see Fig. 1–3).
Where resources and/or the availability of molecular diagnostics or other tests
are limited, different algorithms could be used for different patient groups based
on careful risk assessment and prioritization of molecular diagnostic tests and
liquid culture for those patients presumed to have pulmonary MDR-TB and/or HIV-
associated TB and/or TB meningitis.
Algorithm for the initial laboratory diagnosis
of individuals with symptoms consistent with
pulmonary TB
This starts by subjecting two clinical specimens (preferably including the morning
sample) to a WHO-endorsed molecular diagnostic test and one specimen for
culture (Fig. 1).
8Algorithms for laboratory diagnostic and follow up of TB and MDR-TB cases
Only when a positive rapid molecular test result is obtained would a subsequent
microscopy test be helpful to identify the bacterial load and infectivity. Results
of molecular tests should be communicated to the clinician without waiting for
culture results. If GeneXpert MTB/RIF is negative, no microscopy is necessary
and the sample should be sent for culture only (as culture would still be more
sensitive for TB detection).
Culture-positive samples are subjected to identification, and those cultures
identified as M. tuberculosis (MTB) complex should be subjected to DST. If the
sample that was subjected to the molecular test is culture negative (as well
as negative on the molecular test), further clinical and other non-TB specific
laboratory investigations should follow.
If the molecular diagnostic test predicts susceptibility to RIF and if first-line (FL)
LPA is available, it should be performed to identify INH mono-resistant cases. If
INH resistance is identified, INH mono-resistant regimen should be initiated. In
case FL-LPA is not available or no INH resistance is identified, the FL regimen
needs to be initiated. In both cases, culture and subsequent phenotypic drug-
susceptibility testing (pDST) should be done. Performing a WHO-recommended
rapid molecular test for drug resistance (such as Xpert or LPA) on the primary
samples reduces the delay to appropriate phenotypic resistance results.
If RIF resistance (with or without INH resistance) is confirmed, it is
recommended that the patient be referred to a DR-TB treatment initiation site
for appropriate therapy and to proceed with second-line (SL) LPA (26): this
recommendation applies to the direct testing of sputum specimens from RIF-
resistant TB or MDR-TB irrespective of the smear status, while acknowledging
that the indeterminate rate is higher when testing smear-negative sputum
specimens compared with smear-positive sputum specimens (26). SL-LPA is
suitable for use at central or national reference laboratory level; it has the
potential to be used at regional level if the appropriate infrastructure and
trained staff can be ensured (26).
Once the culture becomes positive, first- and second-line pDST should be set
up, irrespective of SL-LPA results, for patients with negative and positive SL-LPA
results. This streamlining reduces any delay for initiating an appropriate M/XDR-TB
treatment regimen. Depending on the LPA results (FL and SL), treatment should
start accordingly and be adjusted if needed once pDST results are available.
SL-LPA results that lead to the exclusion of both fluoroquinolones (FLQs) and
second-line injectable drug (SLID) resistance means that the use of a shorter
MDR-TB regimen could be considered, providing the other criteria are met (27).
9Algorithm for laboratory diagnosis and treatment-monitoring of pulmonary tuberculosis and drug-resistant tuberculosis using state-of-the-art rapid diagnostic technologies
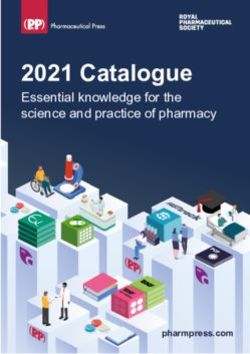
Fig. 1. Algorithm for the initial laboratory diagnosis of
individuals with symptoms consistent with pulmonary TB
Presumptive pulmonary TB cases,
sputum specimen
repeat
No result/error/
Xpert MTB/RIF 1,2,3 invalid
(WHO-endorsed molecular diagnostic test) 4 MTB detected Patient has TB
RIF indeterminate
repeat
MTB
not detected
MTB detected Microscopy
RIF susceptible/resistant (bacterial load, infectivity)
RIF susceptible RIF resistant
FL-LPA 5,6 SL-LPA (direct testing) 2,8
INH INH Refer patient Not interpretable
susceptible resistant to DR-TB Interpretable results
results
treatment
initiation
Regimen for site for
appropriate FLQ (S) FLQ (R)
FL regimen INH-mono- No result
therapy 7 SLID (S) SLID (S)
resistance
FLQ (S)
SLID (R)
FLQ (R) Culture
Culture SLID (R)
SL-LPA
(indirect
MTB not detected Individua-
MTB detected Shorter
lized
testing)8
MDR-TB MDR-TB
regimen9 regimen
Re-evaluate the patient clinically, Solid or
conduct additional testing (e.g., liquid pDST
X-ray) in accordance with
national guidelines; consider
repeating Xpert MTB/RIF testing;
use clinical judgment for Individualized
treatment decisions; alternative regimen
diagnosis
WHO-endorsed Conventional diagnostic Result of the Treatment
rapid molecular assay (microscopy or culture- diagnostics
TB diagnostic techniques based phenotypic techniques)
10Algorithms for laboratory diagnostic and follow up of TB and MDR-TB cases
Footnotes for Fig. 1
Results of molecular tests should be communicated to the clinician without waiting for culture
1 results
2 Performing a rapid molecular test for drug resistance (e.g. Xpert or LPA) on the primary samples
reduces the delay to appropriate phenotypic resistance results
In the absence of Xpert MTB/RIF, sputum smear microscopy can be used as the initial test and the
3 sample should be sent as quickly as possible to a laboratory with the capacity to perform WHO
recommended molecular tests in addition to culture
In case Xpert MTB/RIF is absent but FL LPA is available, this test should be used for smear-positive
4 sputum samples, to detect rifampicin and in addition INH resistance. If INH-R is detected this
information should guide further diagnostic work and be considered in clinical treatment decisions
5 To be performed when FL-LPA is available and has not been done already
In the absence of FL-LPA, FL regimen is suggested to be initiated and adjusted once additional DST
6 results are available
In cases SL-LPA results would not become available within one week, empirical MDR-TB treatment
7 may be initiated
8 SL-LPA are suitable for use at the central or national reference laboratory level; or at regional level
with appropriate infrastructure
9 Following eligibility criteria
Algorithm for monitoring the follow-up of patients
with drug-sensitive pulmonary TB
This algorithm is shown in Fig. 2.
Monthly microscopy and culture during the intensive phase of two sputum
samples and immediately after completion of the intensive phase (at month two
for new cases and month three for previously treated cases) is suggested, as
well as during the fifth and last month of treatment, according to the timeframe
of the treatment protocol in a particular country.
If microscopy and/or culture is/are positive from a sample taken after two months’
treatment, a WHO-endorsed molecular diagnostic test and DST are suggested to
confirm the presence/absence of MTB and the anti-TB drug-resistance pattern.
If the WHO-endorsed molecular tests (X-pert, FL-LPA) indicate resistance to RIF
with or without INH, then SL-LPA should be performed. SL-LPA results that lead
to the exclusion of both FLQs and SLID resistance means that the use of a shorter
MDR-TB regimen could be considered providing the other criteria are met (27).
Once culture results are available and RIF resistance is known (through WHO-
endorsed molecular tests), first- and second-line pDST should be performed
simultaneously.
11Algorithm for laboratory diagnosis and treatment-monitoring of pulmonary tuberculosis and drug-resistant tuberculosis using state-of-the-art rapid diagnostic technologies
Fig. 2. Algorithm for monitoring the follow-up of patients
with drug-sensitive pulmonary TB
Two sputum specimens
Microscopy
(bacterial load, infectivity) Culture
3 MTB
not detected
WHO-endorsed First-line and
molecular test 4 second-line pDST
Individualized
regimen
No resistance to Resistance to RIF
RIF or INH with/without INH
1,2
Not interpretable
Interpretable results
results
FLQ (S) FLQ (R)
No result
SLID (S) SLID (S)
FLQ (S)
SLID (R)
FLQ (R) Culture
SLID (R)
SL-LPA
(indirect
Individua-
Shorter testing)2
lized
MDR-TB MDR-TB
regimen 5 regimen
WHO-endorsed Conventional diagnostic Result of the Treatment
rapid molecular assay (microscopy or culture- diagnostics
TB diagnostic techniques based phenotypic techniques)
12Algorithms for laboratory diagnostic and follow up of TB and MDR-TB cases
Footnotes for Fig. 2
Performing a rapid molecular test for drug resistance (e.g. Xpert or LPA) on the primary samples
1 reduces the delay to appropriate phenotypic resistance results
2 SL-LPA are suitable for use at the central or national reference laboratory level; they have the
potential to be used at the regional level with appropriate infrastructure
If microscopy and/or culture is positive from a sample taken after two months treatment, a WHO-
3 endorsed molecular diagnostic test and DST are suggested to be performed to confirm the presence/
absence of MTB and to determine the resistance pattern
Before initiating the WHO-endorsed test, the results of the molecular tests conducted on previous
4 isolates of the respective patient should be checked in order to ensure that the molecular test of
choice can detect additional resistance
5 Following eligibility criteria
The purpose of diagnostic testing here is to determine the success of treatment;
repeating DST is usually not required unless the patient continues to remain smear
and culture positive or there is evidence of concurrent MDR-TB exposure (that is,
potential superinfection) or clinical deterioration. The laboratory needs to be told
that the sample has been sent only to assess treatment success.
Algorithm for the monitoring of follow-up of
MDR-TB and RIF-resistant patients
This algorithm is shown in Fig. 3.
Culture and microscopy of 1–2 sputum samples should be performed every
month (beginning from the third month) for the complete intensive phase of
treatment (28-30).
After culture conversion (that is, after two consecutive negative cultures taken
at least 30 days apart), culture can be performed every third month and smear
microscopy every month (28), or following the timeframe of the treatment
protocol in a particular country.
If microscopy becomes positive and once the culture becomes positive, SL-LPA
and pDST to additional anti-TB drugs should be performed (there is no need to
repeat the initial RIF-resistance tests, as these will remain resistant).
13Algorithm for laboratory diagnosis and treatment-monitoring of pulmonary tuberculosis and drug-resistant tuberculosis using state-of-the-art rapid diagnostic technologies
Fig. 3. Algorithm for the monitoring of follow-up of MDR-TB
and RIF-resistant patients
Two sputum specimens
Microscopy
Culture
(bacterial load, infectivity)
MTB detected MTB
AFB negative AFB positive
not detected
pDST to
SL-LPA1 additional
anti-TB drugs 2
Individualized
regimen
WHO-endorsed Conventional diagnostic Result of the Treatment
rapid molecular assay (microscopy or culture- diagnostics
TB diagnostic techniques based phenotypic techniques)
Footnotes for Fig. 3
1 To be performed only if no resistance to second line drugs (FLQ and SLID) was detected previously
2 There is no need to repeat the initial rifampicin resistance tests as these will remain resistant
14Practical considerations for the diagnostic algorithm
Practical
considerations for the
diagnostic algorithm
Various tests are performed at different levels of
laboratories and within a laboratory network. In some
countries, laboratories that perform PCR-based
diagnostics for infections other than TB will have the
skills and infrastructure necessary for LPAs, as TB
diagnosis in many countries is incorporated with other
clinical microbiology tests for other diseases
The results of all tests performed at lower levels of laboratories should be
reported and referred together with the samples and/or cultured isolates to the
National Reference Laboratory (NRL). This will prevent wasteful duplication of
tests (except in a proportion used for quality control purposes). A handbook with
the detailed methodologies needed for assay performance has been published
by the European Centre for Disease Prevention and Control European Reference
Laboratory Network (31).
WHO recommends replacing conventional microscopy with rapid molecular tests
(such as GeneXpert MTB/RIF) for the initial diagnosis of TB (3, 17, 24, 25, 32). If
resources permit, two specimens should be tested to increase the sensitivity.
Microscopy would be limited to test TB positive samples detected by rapid
molecular techniques to ascertain patient infectivity and infection control purposes
and for treatment monitoring. Continuing with microscopy also maintains quality-
assured skills in performing microscopy if molecular tests are not available.
15Algorithm for laboratory diagnosis and treatment-monitoring of pulmonary tuberculosis and drug-resistant tuberculosis using state-of-the-art rapid diagnostic technologies
Diagnostic methods of preference
Capacity for microscopy, culture and DST needs to remain, despite molecular
diagnostics. Microscopy and culture are particularly important for treatment
monitoring. The availability of molecular diagnostic tests does not eliminate the
need for conventional microscopy, culture and DST capability; microscopy and
culture remain necessary for the follow-up of treatment, and culture currently still
provides maximum diagnostic sensitivity, while conventional DST is required to
support a diagnosis of XDR-TB and provide a tailored patient-regime for M/XDR-TB
patients. Demands for conventional techniques might change in the future based on
the epidemiological situation.
Light-emitting diode (LED) fluorescence microscopy is the recommended
method for microscopy at all levels of laboratory (33). Both LED microscopy
and conventional fluorescence microscopy are at least 10% more sensitive than
Ziehl-Neelsen microscopy. Moreover, LED microscopy is less costly compared
to conventional fluorescence microscopy (33).
For culture, both solid and liquid media are recommended. Liquid culture is
more sensitive and quicker than culture on solid media (increased yield 10%) (34).
Liquid culture results may become available within days but are more prone to
contamination, more expensive and associated with a higher biosafety risk.
Positive cultures should be differentiated into MTB complex and non-
tuberculous mycobacteria. Confirmation of MTB complex is done through
biochemical reaction, molecular amplification tests or immunochromatographic
assays. The latter two are recommended for species identification on culture
isolates, as they provide a rapid and definite identification of MTB complex (34).
Drug resistance can be detected by genotypic and phenotypic methods. Automated
liquid systems are the current gold standard for FL and SL DST (34). DST should
follow WHO guidelines with stringent quality assurance methods (29, 34, 35). SL DST
should aim to include testing of the aminoglycosides, polypeptides and FLQs used
in the country. DST results on these drugs have good reliability and reproducibility
and allow a quality-assured diagnosis of XDR-TB. With the introduction of SL-LPA
for detecting resistance to FLQs and SLIDs, resistant results to these drugs can be
obtained more rapidly.
By direct testing, SL-LPA will detect 86% of patients with FLQ resistance, 87% with
SLID resistance and 69% of XDR-TB; in all cases, the test will rarely give a false
16Practical considerations for the diagnostic algorithm
positive result (26). In interpreting the results, it should be considered that SL-LPA
cannot determine resistance to individual FLQs. Resistance-conferring mutations
detected by SL-LPA are highly correlated with phenotypic resistance to ofloxacin
and levofloxacin. The correlation of these mutations with phenotypic resistance to
moxifloxacin and gatifloxacin is unclear, however, and the inclusion of moxifloxacin
or gatifloxacin in an MDR-TB regimen is best guided by pDST results (26). Mutations
in some regions of the MTB complex genome (such as the eis promoter region)
may be responsible for causing resistance
to one drug in a class (group) more than
By direct testing, SL-LPA will
other drugs within that class (group).
For example, the eis C14T mutation is detect 86% of patients with
associated with kanamycin resistance in
strains from eastern Europe (26). FLQ resistance, 87% with
Non-commercial methods for culture and
SLID resistance and 69%
DST, including microscopic-observation
of XDR-TB; in all cases, the
drug-susceptibility (MODS), colorimetric
redox indicator (CRI) methods and the test will rarely give a false
nitrate reduction assay (NRA), are also
recommended by WHO (36). These tests positive result
are currently considered as an interim
solution while scale-up of genotypic testing is developed. The systems are less
expensive than commercial systems, but may be more prone to errors due to lack
of standardization, are highly operator-dependent and only suitable for use at
reference laboratory level.
Currently, the WHO-recommended molecular diagnostic tests for TB and DR-TB
include LPAs and the Xpert MTB/RIF assay (as well as loop-mediated isothermal
amplification (LAMP) for TB diagnosis only). Data from systematic reviews and
meta-analyses show that in comparison to conventional DST, LPAs are highly
sensitive (≥97%) and specific (≥99%) for the detection of RIF resistance, alone or in
combination with INH (sensitivity ≥90%; specificity ≥99%), on isolates of MTB and on
smear-positive sputum specimens (23, 37, 38).
An extensive review (17, 32) of the Xpert MTB/RIF assay to detect pulmonary TB
disease, including studies involving almost 10 000 participants, showed the high
specificity of the Xpert MTB/RIF assay to detect TB (99% (95% CrI 98–99%)).
Sensitivity varied by smear status: 68% (95% CrI 61–74%) for smear-negative
17Algorithm for laboratory diagnosis and treatment-monitoring of pulmonary tuberculosis and drug-resistant tuberculosis using state-of-the-art rapid diagnostic technologies
culture-positive to 98% (95% CrI 97–99%) for smear-positive culture-positive
samples. Performance of the Xpert MTB/RIF assay for detection of extrapulmonary
TB varied by specimen type, with lower sensitivity for pleural and cerebrospinal
fluid (ranging from 17% to 80%, respectively) and somewhat lower specificity (93%)
for lymph node specimens, but with good sensitivity (>81%) and specificity (>98%)
for other specimen types (25).
Overall, the Xpert MTB/RIF assay had 95% (95% CrI 90–97%) sensitivity and 98%
(95% CrI 97–99%) specificity to detect RIF. When studies were analysed separately
for settings with different levels of RIF resistance, however, the sensitivity was
96% (95% CrI 91–98%) for settings with >15% RIF resistance among the tested
population, and 91% (95% CrI 79–97%) for settings with ≤ 15% RIF resistance. The
corresponding pooled specificities were 97% (95% CrI 94–99%) and 99% (95% CrI
98–99%) (17, 32).
Similar data have been published in a systematic review with a detailed health
economic analysis (39). The specificity of Xpert MTB/RIF for detecting TB is very
high (99%), and false-positive results are likely to be linked to the detection by Xpert
MTB/RIF of dead MTB bacilli that would not be detected by culture, which is the
present reference standard. Given that the specificity of Xpert MTB/RIF is not 100%,
the positive predictive value (PPV) of Xpert MTB/RIF testing for RIF resistance
testing is adversely affected in settings with a low prevalence of drug-resistant TB
disease or in populations with a low prevalence of TB. Testing for TB is not usually
implemented in a general, asymptomatic population but in individuals with clinical
suspicion of TB following some form of screening involving, for example, symptom
assessment or chest X-ray. Such screening procedures increase the prevalence of
TB in the group tested and improve the PPV of the test, reducing but not eliminating
concerns related to false-positive results (32).
Interpretation and reporting of laboratory results
Results from laboratory tests, including microscopy, molecular tests, culture
and DST, should be reported to clinicians as soon as possible after they become
available, and all means of communication, including telephone, fax, email and
SMS, should be considered to facilitate communication. Interpretation of laboratory
results by laboratory doctors or equivalent is vital, especially in situations when
results are apparently inconsistent or discrepant. Subsequently, appropriate
18Practical considerations for the diagnostic algorithm
isolation of the respective patients Results from laboratory
and adjustment of their treatment
courses according to the anti-TB drug tests, including microscopy,
susceptibility pattern of the causative
pathogens should be initiated promptly molecular tests, culture and
(29) to prevent further spread of the
disease and/or the development of
DST, should be reported to
further resistance. clinicians as soon as possible
It should be noted that mutations in the after they become available
rpoB gene are a very good marker for
MDR-TB in the Region; the percentage of RIF mono-resistant isolates has been
shown to be only 0.5% among new cases and 0.9% among previously treated
cases (5). Under these circumstances, it seems reasonable to initiate patients on
MDR treatment if the Xpert MTB/RIF or LPA results indicate RIF resistance. More
caution is necessary when interpreting the results of molecular tests for SL anti-TB
drugs.
19Algorithm for laboratory diagnosis and treatment-monitoring of pulmonary tuberculosis and drug-resistant tuberculosis using state-of-the-art rapid diagnostic technologies
References
1. The European health report 2012: charting the way to well-being. Copenhagen:
WHO Regional Office for Europe; 2012 (http://www.euro.who.int/__data/
assets/pdf_file/0004/197113/EHR2012-Eng.pdf, accessed 15 February 2017).
2. Roadmap to implement the tuberculosis action plan for the WHO European
Region 2016–2020. WHO Regional Office for Europe; 2016 (http://www.euro.
who.int/__data/assets/pdf_file/0020/318233/Roadmap-implement-TBC-
action-plan-20162020.pdf, accessed 15 February 2017).
3. Global Tuberculosis Report 2016. Geneva: World Health Organization;
2016 (WHO/HTM/TB/2016.13; http://apps.who.int/iris/bitstr
eam/10665/250441/1/9789241565394-eng.pdf, accessed 15 February 2017).
4. Plan to Stop TB in 18 priority countries of the WHO European Region, 2007–
2015. Copenhagen: WHO Regional Office for Europe; 2007 (http://www.euro.
who.int/document/E91049.pdf, accessed 15 February 2017).
5. Tuberculosis surveillance and monitoring in Europe 2016. Stockholm:
European Centre for Disease Prevention and Control/WHO Regional Office
for Europe; 2016 (http://ecdc.europa.eu/en/publications/Publications/ecdc-
tuberculosis-surveillance-monitoring-Europe-2016.pdf, accessed 15 February
2017).
6. Tuberculosis serveillance and monitoring in Europe 2017. Stockholm:
European Centre for Disease Prevention and Control/WHO Regional Office for
Europe; 2017.
20References
7. Tuberculosis surveillance and monitoring in Europe 2013. Stockholm:
European Centre for Disease Prevention and Control/WHO Regional Office
for Europe; 2013 (http://ecdc.europa.eu/en/publications/Publications/
Tuberculosis-surveillance-monitoring-2013.pdf, accessed 15 February 2017).
8. Tuberculosis action plan for the WHO European Region 2016–2020.
Copenhagen: WHO Regional Office for Europe; 2015 (http://www.
euro.who.int/__data/assets/pdf_file/0007/283804/65wd17e_Rev1_
TBActionPlan_150588_withCover.pdf, accessed 15 February 2017).
9. Roadmap to prevent and combat drug-resistant tuberculosis. The
Consolidated Action Plan to Prevent and Combat Multidrug- and Extensively
Drug-Resistant Tuberculosis in the WHO European Region, 2011–2015.
Copenhagen: WHO Regional Office for Europe; 2011 (http://www.euro.who.
int/__data/assets/pdf_file/0014/152015/e95786.pdf, accessed 15 February
2017).
10. European Tuberculosis Laboratory Initiative. In: Health topics [website].
Copenhagen: WHO Regional Office for Europe; 2017 (Report Number; http://
www.euro.who.int/en/health-topics/communicable-diseases/tuberculosis/
activities/european-tuberculosis-laboratory-initiative, accessed 15 February).
11. Migliori GB, Zellweger JP, Abubakar I, Ibraim E, Caminero JA, De Vries G, et al.
European Union standards for tuberculosis care. Eur Respir J 2012;39(4):807-
19; doi: 10.1183/09031936.00203811.
12. Ehsani S, van den Boom M, Gilpin C, Dara M, Europe WHOROf. The role of
novel molecular techniques for tuberculosis diagnostics in the WHO European
Region. J Public Health (Oxf) 2016; doi: 10.1093/pubmed/fdv200.
13. Meeting of the European Tuberculosis Laboratory Initiative (ELI) Core Group.
Copenhagen: WHO Regional Office for Europe; 2016 (http://www.euro.
who.int/__data/assets/pdf_file/0020/307433/ELI-TB-Core-Group-mtg.pdf,
accessed 15 February 2017).
14. International Standards for Tuberculosis Care, third edition. The Hague: TB
CARE I; 2014 (http://www.who.int/tb/publications/ISTC_3rdEd.pdf, accessed 15
February 2017).
21Algorithm for laboratory diagnosis and treatment-monitoring of pulmonary tuberculosis and drug-resistant tuberculosis using state-of-the-art rapid diagnostic technologies
15. Implementing tuberculosis diagnostics: policy framework. Geneva: World
Health Organization; 2015 (WHO/HTM/TB/2015.11; http://apps.who.int/iris/
bitstream/10665/162712/1/9789241508612_eng.pdf, accessed 15 February
2017).
16. Drobniewski FA, Hoffner S, Rusch-Gerdes S, Skenders G, Thomsen V,
Force WHOELST. Recommended standards for modern tuberculosis
laboratory services in Europe. Eur Respir J 2006;28(5):903-9; doi:
10.1183/09031936.06.00084906.
17. Automated real-time nucleic acid amplification technology for rapid and
simultaneous detection of tuberculosis and rifampicin resistance: Xpert MTB/
RIF assay for the diagnosis of pulmonary and extrapulmonary TB in adults
and children. Policy update. Geneva: World Health Organization; 2013 (WHO/
HTM/TB/2013.16; http://www.stoptb.org/wg/gli/assets/documents/WHO Policy
Statement on Xpert MTB-RIF 2013 pre publication 22102013.pdf, accessed 15
February 2017).
18. Winetsky DE, Negoescu DM, DeMarchis EH, Almukhamedova O, Dooronbekova
A, Pulatov D, et al. Screening and rapid molecular diagnosis of tuberculosis
in prisons in Russia and Eastern Europe: a cost-effectiveness analysis. PLoS
Med 2012;9(11):e1001348; doi: 10.1371/journal.pmed.1001348.
19. The European health report 2015: Targets and beyond – reaching new frontiers
in evidence. Copenhagen: WHO Regional Office for Europe; 2015 (http://www.
euro.who.int/__data/assets/pdf_file/0006/288645/European-health-report-
2015-full-book-en.pdf, accessed 15 February 2017).
20. Policy Framework for Implementing New Tuberculosis Diagnostics. Geneva:
World Health Organization; 2010 (http://www.who.int/tb/laboratory/
whopolicyframework_rev_june2011.pdf, accessed 15 February 2017).
21. Guidance on regulations for the Transport of Infectious Substances 2015–2016.
Geneva: World Health Organization; 2015 (WHO/HSE/GCR/2015.2; http://apps.
who.int/iris/bitstream/10665/149288/1/WHO_HSE_GCR_2015.2_eng.pdf,
accessed 15 February 2017).
22References
22. Tuberculosis laboratory biosafety manual. Geneva: World Health
Organization; 2012 (WHO/HTM/TB/2012.11; http://apps.who.int/iris/
bitstream/10665/77949/1/9789241504638_eng.pdf, accessed 15 February
2017).
23. Molecular line probe assays for rapid screening of patients at risk of
multidrug-resistant tuberculosis (MDR-TB): policy statement. Geneva: World
Health Organization; 2008 (http://www.who.int/tb/features_archive/policy_
statement.pdf, accessed 15 February 2017).
24. Automated Real-time Nucleic Acid Amplification Technology for Rapid
and Simultaneous Detection of Tuberculosis and Rifampicin Resistance:
Xpert MTB/RIF System. Policy statement. Geneva: World Health
Organization; 2011 (WHO/HTM/TB/2011.4; http://apps.who.int/iris/
bitstream/10665/44586/1/9789241501545_eng.pdf, accessed 15 February
2017).
25. Xpert MTB/RIF implementation manual. Technical and operational ‘how-to’:
practical considerations. Geneva: World Health Organization; 2014 (WHO/HTM/
TB/2014.1; http://apps.who.int/iris/bitstream/10665/112469/1/9789241506700_
eng.pdf, accessed 15 February 2017).
26. The use of molecular line probe assays for the detection of resistance to
second-line anti-tuberculosis drugs: Policy guidance. Geneva: World Health
Organization; 2016 (WHO/HTM/TB/2016.07; http://apps.who.int/iris/bitstr
eam/10665/246131/1/9789241510561-eng.pdf, accessed 15 February 2017).
27. WHO treatment guidelines for drug-resistant tuberculosis, 2016
update. Online Annexes 4,5,6. Geneva: World Health Organization;
2016 (WHO/HTM/TB/2016.04; http://apps.who.int/iris/bitstr
eam/10665/250125/5/9789241549639-webannexes-eng.pdf, accessed 15
February 2017).
28. Definitions and reporting framework for tuberculosis – 2013 revision. Geneva:
World Health Organization; Updated December 2014 (WHO/HTM/TB/2013.2;
http://apps.who.int/iris/bitstream/10665/79199/1/9789241505345_eng.pdf,
accessed 15 February 2017).
23Algorithm for laboratory diagnosis and treatment-monitoring of pulmonary tuberculosis and drug-resistant tuberculosis using state-of-the-art rapid diagnostic technologies
29. Guidelines for the programmatic management of drug-resistant tuberculosis:
update 2011. Geneva: World Health Organization; 2011 (WHO/HTM/TB/2011.6;
http://apps.who.int/iris/bitstream/10665/44597/1/9789241501583_eng.pdf,
accessed 15 February 2017).
30. Same-day diagnosis of tuberculosis by microscopy: policy statement. Geneva:
World Health Organization; 2011 (WHO/HTM/TB/2011.7; http://apps.who.int/
iris/bitstream/10665/44603/1/9789241501606_eng.pdf, accessed 15 February
2017).
31. Handbook on TB laboratory diagnostic methods for the European Union.
Stockholm: ECDC: European Centre for Disease Prevention and Control; 2016
(http://ecdc.europa.eu/en/publications/publications/tuberculosis-laboratory-
diagnostic-methods-eu.pdf, accessed 15 February 2017).
32. Using the Xpert MTB/RIF assay to detect pulmonary and extrapulmonary
tuberculosis and rifampicin resistance in adults and children. Expert Group
Meeting Report. Geneva: World Health Organization; 2013 (WHO/HTM/
TB/2013.14; http://apps.who.int/iris/bitstream/10665/112659/1/WHO_HTM_
TB_2013.14_eng.pdf, accessed 15 February 2017).
33. Fluorescent light-emitting diode (LED) microscopy for diagnosis
of tuberculosis: policy statement. Geneva: World Health
Organization; 2011 (WHO/HTM/TB/2011.8; http://apps.who.int/iris/
bitstream/10665/44602/1/9789241501613_eng.pdf, accessed 15 February
2017).
34. Use of liquid TB culture and drug susceptibility testing in low- and medium-
income settings. Summary report of the Expert Group Meeting on the use
of liquid culture media. Geneva: World Health Organization; 2007 (http://
www.who.int/tb/laboratory/use_of_liquid_tb_culture_summary_report.pdf,
accessed 15 February 2017).
35. Policy guidance on drug-susceptibility testing (DST) of second-line
antituberculosis drugs. Geneva: World Health Organization: The STOP
TB department; 2008 (WHO/HTM/TB/2008.392; http://www.who.int/tb/
publications/2008/who_htm_tb_2008_392.pdf, accessed 15 February 2017).
24References
36. Noncommercial culture and drug-susceptibility testing methods for screening
patients at risk for multidrugresistant tuberculosis: policy statement. Geneva:
World Health Organization; 2011 (WHO/HTM/TB/2011.9; http://apps.who.int/
iris/bitstream/10665/44601/1/9789241501620_eng.pdf, accessed 15 February
2017).
37. Bwanga F, Hoffner S, Haile M, Joloba ML. Direct susceptibility testing for multi
drug resistant tuberculosis: a meta-analysis. BMC Infect Dis 2009;9:67; doi:
10.1186/1471-2334-9-67.
38. Arentz M, Sorensen B, Horne DJ, Walson JL. Systematic review of the
performance of rapid rifampicin resistance testing for drug-resistant
tuberculosis. PLoS One 2013;8(10):e76533; doi: 10.1371/journal.pone.0076533.
39. Drobniewski F, Cooke M, Jordan J, Casali N, Mugwagwa T, Broda A, et al.
Systematic review, meta-analysis and economic modelling of molecular
diagnostic tests for antibiotic resistance in tuberculosis. Health Technol
Assess 2015;19(34):1-188, vii-viii; doi: 10.3310/hta19340.
25Algorithm for laboratory diagnosis and treatment-monitoring of pulmonary tuberculosis and drug-resistant tuberculosis using state-of-the-art rapid diagnostic technologies
Annex 1
Results obtained by genotypic (Xpert MTB/RIF and
first-line LPA) and phenotypic methods (MGIT and
LJ) to support primarily NRLs or regional reference
laboratories for better understanding and interpreting
discrepant results
Both methods, Xpert MTB/RIF and first-line line probe assays (LPA), have a high
sensitivity and specificity to detect tuberculosis (TB) and rifampicin resistance.
The Xpert MTB/RIF assay has 95% sensitivity and 98% specificity for rifampicin
detection and LPA 97% and 99% respectively (25, 26). That means there are few
false susceptible and false resistant strain results reported to clinicians.
Genotypic results are recommended to be reported first to clinicians, due to the
rapidity of the techniques and their high sensitivity and specificity. With this, the
clinician can start treatment with first-line drugs or a multidrug-resistance (MDR)
regimen based on the initial rapid molecular test results.
After repeating results with the other molecular-based technique (often LPA, as
Xpert MTB/RIF is proposed to be used as the initial test) and phenotypic drug-
susceptibility testing (pDST), the results can in rare cases differ. If both genotypic
DST (gDST) methods show resistance but pDST results are susceptible, there is
likely to be an error in performing conventional DST. Before clarification of the
reasons behind the discordance, the clinician shall proceed with the initiation of
treatment based on the gDST results.
26You can also read