An Update on Eosinophilic Esophagitis: Etiological Factors, Coexisting Diseases, and Complications - Karger Publishers
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Review
Digestion 2021;102:342–356 Received: November 21, 2019
Accepted: April 26, 2020
DOI: 10.1159/000508191 Published online: June 22, 2020
An Update on Eosinophilic Esophagitis:
Etiological Factors, Coexisting Diseases,
and Complications
Samiullah Khan a Xiaopei Guo b Tianyu Liu a Muhammad Iqbal c Kui Jiang a
Lanping Zhu a Xin Chen a Bang-mao Wang a
aDepartment of Gastroenterology and Hepatology, Tianjin Medical University General Hospital, Tianjin, China;
bDepartment
of Gastroenterology and Hepatology, Erasmus University Medical Centre, Rotterdam, The Netherlands;
cDepartment of Otorhinolaryngology, The First Affiliated Hospital, Sun Yat-Sen University, Guangzhou, China
Keywords be manifested as isolated or with coexisting conditions and
Esophagus · Eosinophilic esophagitis · Etiological factors · should be taken into consideration in the differential diag-
Comorbid conditions · Complications nosis. This study aimed to provide gastroenterologists with
novel insights into the evaluation of esophageal involve-
ment with eosinophils and to pay special attention to the
Abstract etiological factors, coexisting clinical diseases, and compli-
Background: Eosinophilic esophagitis (EoE) is an immune- cations. © 2020 S. Karger AG, Basel
mediated clinicopathological condition characterized by
esophageal infiltration with eosinophils resulting in chronic
inflammation and stricture. Summary: The recent increase
in the incidence of EoE and the characteristic presentation of Introduction
symptoms with difficulty swallowing and food bolus impac-
tion has raised key concerns of clinicians as well as research- Eosinophilic esophagitis (EoE) is a chronic, relapsing,
ers. EoE often presents with dysphagia, food impaction, nau- immune-mediated esophageal disease [1–4] character-
sea, regurgitation or vomiting, and decreased appetite. It is ized by hyperplasia of basal cells, microabscesses, degran-
more common in males, affecting both adults and children. ulation, dilated intercellular spaces [5], and predominant
The causative manner of this condition is complex and mul- eosinophilic infiltration in the esophagus [6]. The esoph-
tifactorial. Throughout recent years, researchers have made agus is unique from the rest of the gastrointestinal tract;
a significant contribution to understanding the pathogene- normally, there is no eosinophil in the esophagus. The
sis of EoE, genetic background, natural history, work on al- prevalence is higher in both children and adults [1]. In
lergy, and standardization in the evaluation of disease activ- EoE, high counts of eosinophil are build up in the epithe-
ity. There is relatively high prevalence of EoE among the pop- lial lining of the esophagus [7]. This eosinophilic buildup,
ulation, emphasizing the importance of this disease. Key which is a reaction to multiple factors including foods,
messages: Esophageal involvement with eosinophils may allergens, atopic conditions, diseases, or acid reflux, may
karger@karger.com © 2020 S. Karger AG, Basel Prof. Bang-mao Wang
www.karger.com/dig Department of Gastroenterology and Hepatology
Tianjin Medical University General Hospital
154 Anshan Road, Tianjin 300052 (China)
mwang02 @ tmu.edu.cnColor version available online
• Infants and toddlers: Nausea, emesis, abdominal pain, failure to thrive
• School-age children: Recurrent abdominal pain or vomi�ng
Symptoms • Adolescents and adults: Dysphagia, heartburn and regurgita�on
• Children: Normal appearance of esophageal �ssue or plaques or edema
• Adults: mucosal fragility, esophageal rings , white exudates or plaques,
Endoscopic longitudinal furrows, diffuse esophageal narrowing, and strictures
features
• Biopsy: At least 3 or more biopsies from proximal and distal esophagus
• Histology: Eosinophilic-infiltra�on of >15 eosinophils per high power field is
Biopsy & the diagnos�c criterion
Histology
Fig. 1. Clinical characteristics of patients
with eosinophilic esophagitis.
deteriorate or damage the tissue of the esophagus which It is estimated to be around 30–52 cases per 100,000
contributes to fibrosis and strictures [2, 8]. inhabitants in the general population [21]. A research
The symptoms of patients with EoE vary with age [9]; study between 2005 and 2011 in central Spain [22] found
infants and toddlers most commonly have nausea, eme- an average yearly incidence of 6.37/100,000 residents and
sis, abdominal pain, refusing eating, or not growing prop- a prevalence of 44.6/100,000 residents, the latter being
erly (failure to thrive) [3, 10, 11]. School-age children of- greater in urban regions [23].
ten experience recurrent abdominal pain or vomiting EoE has been described in all races and continents and
[12], and adolescents and adults have difficulty swallow- can occur at any age, and it most commonly occurs in
ing, heartburn, and regurgitation most often [9, 13, 14] Caucasian males [24] and has a strong hereditary compo-
(Fig. 1). nent with large sibling risk ratio [11]. It is more frequent
Endoscopic characteristics of children with EoE in- in males than in females (3:1). The mean age at the time
clude having either a normal appearance of esophageal of diagnosis ranges between 30 and 50 years in adults and
tissue or plaques or edema findings, whereas adults dis- 5.4 and 9.6 years in children [25].
play mucosal fragility, esophageal rings (trachealization), The pathogenesis of EoE is relatively poorly under-
white exudates or plaques, longitudinal furrows, diffuse stood. Increasing evidence suggests a strong involvement
esophageal narrowing, and strictures (Fig. 2). EoE is a of genetic and environmental factors [26], premature de-
transmural disorder affecting all layers of the esophagus livery, cesarean birth, early antibiotic exposure, food al-
[15]. Histological identification of predominant eosino- lergy, lack of breast feeding, and lack of early microbial
philic infiltration of >15 eosinophils per high-power field exposure are associated with EoE [7, 11] (Table 1).
(HPF) is the diagnostic criterion [3, 8, 16, 17]. A mini-
mum of 3 or more biopsies from the proximal and distal
esophagus should be collected for an adequate diagnostic Mechanistic Aspects of Esophageal Damage in EoE
yield [9, 18, 19].
The mechanism of dysphagia in EoE is multifactorial,
including mucosal stickiness, esophageal fibrosis, stric-
Epidemiological Aspects tures, and ring formation [27]. Eosinophils produce and
release numerous proteins and mediators, namely, major
Over recent years, there has been a rise in the incidence basic protein, eosinophilic cationic protein, eosinophil-
and prevalence of EoE [20]. In both children and adult pop- derived neurotoxin, and eosinophilic peroxidase, which
ulations, the prevalence has also increased. It is the leading play a key role in tissue damage and remolding [28, 29].
cause of dysphagia in children and young adults [20]. Serum analyses of absolute eosinophil count, eosinophil-
Etiological Factors, Coexisting Diseases, Digestion 2021;102:342–356 343
and Complications of EoE DOI: 10.1159/000508191a
Color version available online
b c
d e f
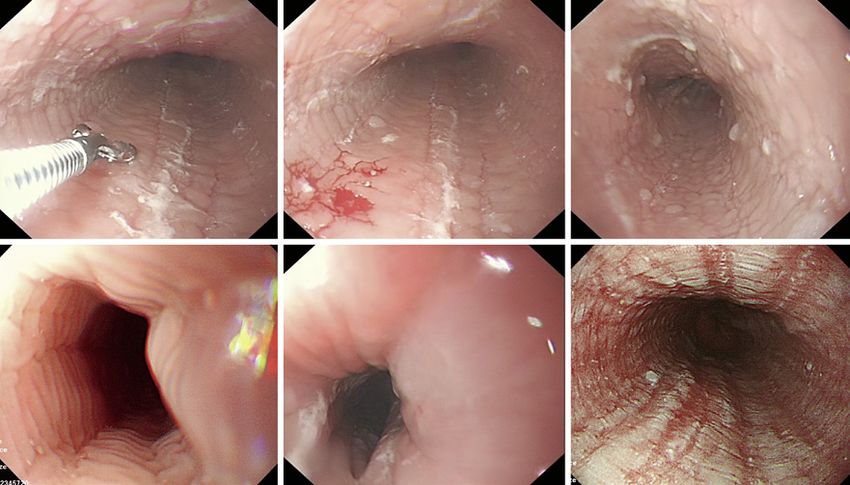
Fig. 2. Images of 3 patients (patient 1 (a–c); patient 2 (d, e); patient 3 (f)) with eosinophilic esophagitis in our
endoscopic department show linear furrowing (a), mucosal friability and tearing (b), multiple nodules 0.2–0.3
cm (c), trachealization (d), esophageal narrowing with exudates (e), and severe eosinophilic microabscess with
linear furrowing (f).
Table 1. Epidemiology of eosinophilic esophagitis Table 2. Mechanistic aspects of EoE
Prevalence in both children and adults ↑ Proteins and mediators by eosinophils
Dysphagia in children and young adults ↑
All races and continents Yes Major basic protein
Any age Yes Eosinophilic cationic protein
Commonly in Caucasian males Yes Eosinophil-derived neurotoxin
Hereditary/sibling risk ratio ↑ Eosinophilic peroxidase
Gender M>F Bone morphogenetic protein
Mean age of diagnosis in adults 30–50 years Phospholamban
Mean age of diagnosis in children 5.4–9.6 years Transforming growth factor-β1
Histamine-producing mast cells and basophils
Activated CD3+CD8+ T cells
Tumor necrosis factor-α
Interferon gamma
ic cationic protein, and eosinophil-derived neurotoxin EoE, eosinophilic esophagitis.
were higher in EoE patients in one prospective study, be-
sides absolute eosinophil count predicted posttreatment
eosinophilia [30]. Bone morphogenetic proteins [31]
promote squamous differentiation of basal progenitor
cells upon their activation in the adult’s esophagus, and is an important player in transforming growth factor-β1-
basal cell hyperplasia in biopsy samples is associated with mediated esophageal squamous mucosa cell and myofi-
high levels of follistatin [32]. Activated eosinophil- and broblast contraction in the pediatric population [35].
mast cell-derived transforming growth factor-β1 secre- Eosinophils and mast cells [36, 37] as well as histamine-
tion is crucial in EoE-associated tissue remodeling [33, producing mast cells and basophils [38–40] play a very
34]; also, phospholamban, an integral membrane protein, important role in bringing eosinophils into the esophageal
344 Digestion 2021;102:342–356 Khan/Guo/Liu/Iqbal/Jiang/Zhu/Chen/
DOI: 10.1159/000508191 WangTable 3. Etiological factors associated with EoE
N Etiologies Associated factors Ref.
1 Inflammatory mediators TH2-mediated IL-4, IL-5, IL-13, IL-33 and TSLP [1, 3, 11, 15, 16, 44, 45]
2 Genetic susceptibility TSLP and CAPN14 [53]
3 Environmental factors Pollen seasons, cold or dry climate [57, 58]
4 Atopic conditions Asthma, allergic rhinitis, and atopic dermatitis [9, 63]
5 Dietary products Cow’s milk, soy, egg, wheat, peanut/tree nuts, seafood, and legumes [64–67]
6 Esophageal microbiome Haemophilus, Corynebacterium, Neisseria, Firmicutes and Bacteroides [20, 72]
7 Oral immunotherapy IgE-mediated food allergy (cow milk, egg, and shellfish) [74–76]
8 Inversely associated Helicobacter pylori and the development of EoE, and EoE versus Barrett’s [11, 78]
conditions esophagus
9 Acid suppressor PPI → preventing peptic digestion of food allergens → alter microbial dysbiosis [43]
EoE, eosinophilic esophagitis; TH2, T helper type 2; IL, interleukin; TSLP, thymic stromal lymphopoietin; CAPN14, calpain 14; IgE,
immunoglobulin E; PPI, proton pump inhibitors.
epithelium [39]. In the EoE-active group, a high number Inflammatory Mediators
of activated CD3+CD8+ T cells were found to secrete tu- EoE is still a relatively poorly understood entity. In-
mor necrosis factor-α and interferon gamma in compari- creasing evidence indicates a vigorous presence of the in-
son with the EoE-remission and control groups [18]. volvement of genetic and environmental factors [26]. The
Moreover, the role of calcium-activated chloride channel T helper type 2 (TH2)-mediated inflammatory cytokines,
Anoctamin 1 in esophageal cell proliferation and basal interleukin (IL)-4, IL-5, IL-13 [1, 3, 11, 15, 16, 44, 45], and
zone hyperplasia in EoE has also been reported (Table 2). IL-33 in pediatric [46], and invariant natural killer T cells
[26] are involved in trafficking eosinophils into esopha-
geal tissue.
Etiological Factors Activation of signal transducer and activator of tran-
scription-6 (STAT6) by IL-4 and IL-13 mediates the
Certain conditions such as inflammatory mediators, ge- pathogenesis of allergic disorders [47, 48]. In experimen-
netic susceptibility, environmental factors, atopic condi- tal models, IL-13 has been demonstrated to induce esoph-
tions, dietary products, esophageal microbiome, and oral ageal eosinophilia and regulate numerous identified
immunotherapy have been associated with a higher risk of genes associated with EoE [11]. Moreover, epithelial cells
EoE formation. However, various other conditions with and the thymic stromal lymphopoietin (TSLP) gene and
distinct clinical and histological characteristics have also its receptor appear to be risk factors for EoE as they un-
been identified to be associated with esophageal eosino- dergo polymorphisms in the eotaxin-3 [49–51] and other
philia such as eosinophilic gastrointestinal diseases, proton chemoattractants [15].
pump inhibitor (PPI)-responsive esophageal eosinophilia,
drug hypersensitivity, pemphigus, connective tissue disor- Genetic Susceptibility
ders, graft-versus-host disease [41], and hypereosinophilic Genetic associations are prone to various types of al-
syndrome, a rare group of conditions that are associated lergic conditions, including EoE. The TSLP and cal-
with persistent high eosinophilia with eosinophil counts pain-14 (CAPN14) are 2 widely studied genetic compo-
>1,500/μL, which most commonly affects the heart, central nents involved in EoE and atopy. Variants in the 5q22
nervous system, skin, and respiratory tract [42]. locus encoding the gene for TSLP have been associated
Moreover, there is a hypothesis that medications such with EoE and the most common atopic diseases, includ-
as acid suppressor (PPIs) might contribute to the patho- ing atopic dermatitis, asthma, and allergic rhinitis [20,
genesis of EoE by preventing peptic digestion of food al- 52]. TSLP is an epithelial cell-derived cytokine that is se-
lergens and altering microbial dysbiosis. EoE such as eo- creted in response to allergen exposure on membrane
sinophilic gastroenteritis might have mucosal and muscle surfaces and is involved in the initiation of type 2 inflam-
predominant types that may cause esophageal motility mation.
disorders including achalasia [43] (Table 3).
Etiological Factors, Coexisting Diseases, Digestion 2021;102:342–356 345
and Complications of EoE DOI: 10.1159/000508191In the esophagus, TSLP in biopsy samples from sub- Atopic Conditions
jects with EoE was found to be overexpressed as com- The majority of patients with EoE are atopic [2, 26, 44].
pared with healthy individuals [52]. Similarly, variants in Most studies reported associations between EoE and
the 2p33 locus encoding the CAPN14 gene are strongly atopic disorders. Patients with EoE are at increased risk
associated with EoE and atopy, with CAPN14 upregula- of asthma, allergic rhinitis, atopic dermatitis, and food al-
tion in the esophagus among those with active esophagi- lergies, suggesting potential common pathogenesis [25,
tis or after exposure to type 2 cytokines [53]. Previous 63].
reports have also found the association of CAPN14 dys- In general, eosinophils have been hypothesized to
regulation with epithelial barrier dysfunction [54]. Like- move to the esophagus in response to various ingested
wise, these studies show a common set of genetic changes and/or inhaled allergens, thereby associating EoE with
that may predispose an individual to various allergic allergy-induced diseases. As a result of that, a high preva-
manifestations, including EoE. lence of atopic diseases (e.g., asthma, allergic rhinitis, and
atopic dermatitis) and sensitization to food and environ-
Environmental Factors ment allergens is seen in pediatric and adult EoE popula-
The rapid change in incidence and prevalence of EoE tions [9, 64].
demonstrates the potential importance of environmental
factors [11, 55]. Environmental allergen exposure may The Role of Dietary Products in EoE
also play critical roles in the pathogenesis and ongoing In the pathophysiology of EoE, food allergy is believed
manifestations of EoE, such as pollen seasons spring/fall to play a crucial role [65–68]. However, the relationship
or living in a cold or dry climate [11]. About the temper- between food allergy and EoE is complex. Allergy tests
ate climate zone, studies reported an increased risk of EoE (skin tests, patch tests, or blood tests) are important.
in patients residing in a cold climate zone [56]. While Many studies have shown that most EoE patients have
some of these studies suggest an association between sea- evidence of IgE-mediated food sensitization based on
son and EoE [57, 58], some studies have indicated no as- IgE-specific in vitro or skin prick testing [64]. Once a food
sociation [59, 60]. is eliminated from the diet of a patient, symptoms usu-
Recently, a study related to seasonality and pollen ally improve in a couple of weeks.
counts was carried out in 36 EoE patients in the New York Foods such as dairy products, egg, soy, and wheat can
City area. The counts of 11 different pollen taxa were cause an allergic disorder that is non-IgE mediated [44]
studied, including Acer (maple), Betula (birch), Populus and are the main causes of EoE. Wheat and cow’s milk are
(poplar), Ulmus (elm), Quercus (oak), Carya (hickory), a commonly implicated trigger in EoE. Exclusive cow’s
Fraxinus (ash), Platanus (sycamore, London planetree), milk evading has recently been documented, and cow’s
Fagus (beech), Poaceae (grass pollen family), and Ambro- milk elimination induced clinicopathological remission
sia (ragweed). Increased patient symptoms were recorded in most EoE patients, endorsing its use as a first-line in-
in summer, and increased diagnoses were noted in the fall tervention. However, a 6-food elimination diet targeting
months. Moreover, symptoms of EoE correlated with the common intact proteins is associated with food aller-
peak levels of grass pollen [61]. Similarly, another study gies (cow’s milk, soy, egg, wheat, peanut/tree nuts, and
showed differences in the association between seasonality seafood).
and EoE by climate zone, with the strongest evidence of The recurrence of esophageal eosinophilia after the re-
seasonal variation in EoE diagnoses in temperate and introduction of food provides definite evidence of the role
cold climates. Higher EoE diagnosis was associated with of food allergens in EoE [69]. A more tolerable 4- food
summer months, but peak diagnoses varied by month de- elimination diet (dairy products, wheat, egg, and le-
pending on the climate zone [55]. gumes) was followed by adult EoE patients; after sequen-
Besides, peripheral eosinophilia and elevated serum tial reintroduction of food(s), only 1 or 2 foods were re-
immunoglobulin E (IgE) levels are usually found in 50 ported as responsible for EoE in 65–85% of all EoE pa-
and 75% of patients [13], and there is no phenotypical tients, regardless of age [68]. This approach has the
variation in adult EoE with IgE-mediated food sensitivity benefit of shortening the time it takes to identify the
and non-food-sensitive patients [62]. Together, these re- food(s) responsible for EoE, meaning fewer endoscopic
sults point toward climate and geographic changes, sug- procedures.
gesting that aeroallergens may contribute to the develop-
ment of disease or flare.
346 Digestion 2021;102:342–356 Khan/Guo/Liu/Iqbal/Jiang/Zhu/Chen/
DOI: 10.1159/000508191 WangThe Role of Esophageal Microbiome in EoE were diagnosed with EoE and asymptomatic esophageal
The human microbiome is both immense and com- eosinophilia after a cow milk-free diet. Moreover, the au-
plex, with 100 trillion microbes representing multiple thor also stated that all patients allergic to cow milk who
genera colonizing the gastrointestinal tract alone [70]. underwent OIT developed EoE, showed unfavorable
Recently, the microbiome has been concerned with vari- progress, and required a dose reduction of cow milk.
ous allergic and inflammatory diseases. The esophagus is In one follow-up study, a hazardous ratio of 9.1 for
colonized by hundreds of bacterial species, with members children with IgE-mediated food allergy in developing
of the Firmicutes and Bacteroides phyla being among the EoE was observed, the strongest association was detected
highest in both children and adults [20]. among the various allergic march relationships [77]. Such
The esophageal microbiome may play a vital role in findings together indicate that both IgE-mediated food
EoE, especially Haemophilus[71, 72], Corynebacterium, allergy and EoE may result from a common allergen-spe-
and Neisseria[20, 73]. According to the study by Harris et cific TH2 response. Furthermore, the concern for iatro-
al. [71], the average bacterial load detected in all subjects genic EoE in patients undergoing OIT is warranted, and
with EoE was significantly greater than that determined patients undergoing OIT should be strictly monitored for
from normal subjects. By comparison, there was also a EoE symptoms.
significant increase in the average bacterial load observed
in gastroesophageal reflux disease (GERD) subjects com- Inverse Relationship between EoE and Helicobacter
pared with normal esophagus control subjects. pylori
Besides, alterations in the salivary microbiome have An interesting inverse association between EoE and H.
also been reported in EoE [72]. The associations between pylori[11] and an inverse relationship between H. pylori
early-life environmental pressures and the development and the development of EoE were established in recent
of EoE existed. For example, antibiotic exposure and diet studies taking into account that environmental factors
known to influence and alter normal esophageal flora are might influence the development of EoE [56, 78]. Fur-
associated with EoE in the majority of studies. Similarly, thermore, H. pylori infection has been found to be in-
cesarean delivery also increases the risk of EoE. Such find- versely related with atopic diseases (asthma, atopic der-
ings together support the role of environmental pressures matitis, and allergic rhinoconjunctivitis) and may play a
that modify the microbiome, leading to the development protective role in these conditions [63]. Similarly, an in-
of EoE and other allergic manifestations. To expand upon verse relationship between EoE and Barrett’s esophagus
this work and identify the most relevant microbes and has also been reported in a Japanese study [79]. A study
involvement of immunological mechanisms, however, by Dellon et al. [80] reported an inverse relationship of
future research is necessary. esophageal eosinophilia and H. pylori infection (OR 0.77)
in esophageal biopsy samples accumulated from a US pa-
Oral Immunotherapy and EoE thology database. Also, the analysis showed that odds of
Recently, the increasing number of EoE detection in H. pylori infection decreased as esophageal eosinophilia
patients undergoing oral immunotherapy (OIT) for IgE- increased (OR 0.52 for >90 eosinophils/HPF).
mediated food allergy has raised serious concerns that Moreover, von Arnim et al. [63] reported serological
OIT may elicit EoE in susceptible individuals. This asso- analyses for H. pylori infection in 58 patients with clini-
ciation was further investigated in a meta-analysis show- cally and histologically proven EoE. Among them, 3 pa-
ing a positive correlation between OIT and EoE, with the tients reported with current H. pylori infection and 5 pa-
occurrence of new onset in 2.7% of OIT patients [20, 74]. tients reported with previous eradication therapy for H.
However, it is uncertain at present whether OIT triggers pylori infection as serologically negative posteradication
EoE or whether OIT aggravates moderate EoE in other- therapy status. EoE patients with current H. pylori infec-
wise subclinical individuals. tions displayed a significantly lower prevalence than the
The prevalence of EoE was observed higher in patients control groups. EoE (current and former) was strongly
with IgE-mediated food allergy than in the general popu- inversely associated with seroprevalence of H. pylori (OR
lation [75], and the history of IgE-mediated food allergy 0.24, 95%).
to the 3 common food allergens (milk, egg, and shellfish) Recently, a large multicenter case-control study
was closely linked to the subsequent diagnosis of EoE straightly examined the relationship between H. pylori
[75]. Gómez Torrijos et al. [76] reported 57 children who and EoE in a prospective manner. A total of 808 individ-
underwent OIT for cow milk allergy in which 3 of them uals, including 170 children, were studied. The study
Etiological Factors, Coexisting Diseases, Digestion 2021;102:342–356 347
and Complications of EoE DOI: 10.1159/000508191found no difference in H. pylori prevalence between cases Table 4. Coexisting conditions with EoE
and control groups in either children or adults [81]. A
possible correlation between EoE and H. pylori infection GERD
IBD (Crohn’s disease and ulcerative colitis)
has not been sufficiently investigated in the literature and CD
therefore requires further study and discussion. Lymphocytic esophagitis
Eosinophilic cholangitis
Type 2B von Willebrand disease
Comorbid Conditions Esophageal intramural pseudo diverticulosis
Vascular changes in eosinophilic esophagitis
Immunoglobulin G4-related disease
EoE is a chronic, allergic, immune system-mediated Herpetic esophagitis
disease associated with an increased risk of comorbid Esophagitis dissecans
conditions (Table 4). Siderius-Hamel syndrome
EoE and eosinophilic subserosal gastroenteritis with ascites
Possible Relationships between GERD and EoE EoE, eosinophilic esophagitis; GERD, gastroesophageal reflux
Over the past 2 decades, esophageal eosinophilia has disease; CD, celiac disease; IBD, inflammatory bowel disease.
progressed from a clinical criterion of GERD to an ulti-
mate histological marker of EoE and now back to an actu-
ally complex association between the 2 entities. The in-
creasing GERD reports in the general population are high EoE [84]. Moreover, von Arnim et al. [85] reported 10
enough to make the coexistence of GERD with EoE in- characteristic marker set (atopy, food impaction, dyspha-
evitable. EoE and GERD have overlapping clinical, endo- gia, PPI-refractory symptoms, peripheral eosinophilia,
scopic, manometric, and histopathologic features. EoE IgE, weight loss, painful swallowing/odynophagia, age,
may contribute to the development of GERD via many and sex) which effectively distinguish GERD from EoE.
eosinophil products that can relax the muscle of the low- Besides, the 10 markers were further reduced to 4 param-
er esophageal sphincter as a result altering motility or eters (history of atopy, history of food impaction, PPI-
causing structural changes. In contrast, GERD causes refractory symptoms, and either IgE or peripheral eosin-
EoE, leading to acid injury of the epithelium, increased ophilia), which were also able to excellently predict EoE
epithelial permeability, and increased immune cells re- and differentiate EoE from GERD.
cruitment [26, 67, 82]. In refractory GERD patients, EoE is not uncommon.
EoE is commonly seen in dysphagic patients and, to a It may exist with symptoms of dysphagia, heartburn, and
lesser extent, PPI-resistant GERD [64]. According to the the impaction of food. Esophageal screening with biopsy
study by Zukerberg et al. [83], patients with EoE (mean is necessary for older patients with longstanding GERD,
peak eosinophil count of 53/HPF) showed increasingly positive for atopy, or not responding to gastric acid in-
higher intraepithelial eosinophilic numbers than those hibitors.
with reflux esophagitis (mean peak eosinophil count of
27/HPF). EoE and Inflammatory Bowel Disease
In general, patients with EoE demonstrate diffuse Inflammatory bowel disease (IBD) and EoE are chron-
esophageal involvement (as measured by the number of ic inflammatory disorders associated with an impaired
eosinophils), while reflux esophagitis is usually confined mucosal immune response; however, the immune re-
to the distal part of the esophagus. Moreover, the study sponses are different. EoE is believed to be an antigen-
stated that patients with EoE showed significant submu- driven allergic disorder in genetically predisposed indi-
cosal fibrosis and abscesses which composed of eosino- viduals mediated by TH2 cells, which contributes to eo-
phils. sinophil migration into the esophageal mucosa. In
The literature by García-Rojo et al. [40] reported that contrast, IBD is regarded as multifactorial. More recently,
CD3-, CD4-, and CD8- marker analysis may be used to the coexistence of EoE and IBD has been increasingly rec-
distinguish between GERD and EoE patients. In rare situ- ognized [66, 86, 87]. Talathi et al. [86] reported a case se-
ations, for example, children with strong clinical suspi- ries of 6 pediatric patients with coexisting EoE and IBD
cion where fragments do not reach 15 intraepithelial eo- (4 Crohn’s disease and 2 ulcerative colitis), which re-
sinophils/HPF, immunostaining for arachidonate-15 li- vealed characteristic endoscopic and histological findings
pooxygenase has been found to be a sensitive marker for suggestive of EoE.
348 Digestion 2021;102:342–356 Khan/Guo/Liu/Iqbal/Jiang/Zhu/Chen/
DOI: 10.1159/000508191 WangRegarding the gastrointestinal tract, eosinophilia is EoE and Lymphocytic Esophagitis
common in IBD and the number of eosinophils is reliant Lymphocytic esophagitis most commonly present
on the severity of the disease. Recent studies reported a with symptoms of dysphagia, abdominal pain, heartburn,
progressively complex course in patients with concurrent and nausea. Endoscopic features of lymphocytic esopha-
IBD and EoE, which includes IBD-related complications, gitis can be similar to EoE including esophageal rings,
poor response to infliximab, and poorer nutritional out- furrows, exudates, narrow lumen, or stenosis, but in one-
comes [87]. third of patients, the esophageal mucosa appears macro-
This study underlines the need for physicians to con- scopically normal [93].
sider the possibility of concurrent EoE and IBD, particu- Lymphocytic esophagitis is diagnosed when more
larly when the eosinophilic condition is isolated to the than 40 intraepithelial lymphocytes/HPF are present and
esophagus in patients with IBD and the existence of other no intraepithelial granulocytes or occasional presence of
histological features related EoE. Such understanding will CD15 + intraepithelial granulocytes. The compound eo-
help in the early diagnosis and management of these pa- sinophilic and lymphocytic esophagitis can be considered
tients and also help to better understand the relationship in patients who fulfilled both EoE and lymphocytic
between these 2 conditions. esophagitis diagnostic criteria (>15 eosinophils/HPF and
>40 intraepithelial lymphocytes/HPF) [93, 94].
EoE and Celiac Disease EoE and lymphocytic esophagitis can sometimes be
Celiac disease (CD) and EoE have recently been the considered as an overlapping phenotype of endoscopic
main focus of various pediatric studies with variable out- features similar to that in EoE when there are over 40 in-
comes. Both diseases are mediated by the immune sys- traepithelial lymphocytes/HPF present [93, 94]. Accord-
tem, and dietary factors play a significant role in their ing to the study by Truskaite et al. [93], compound EoE/
pathogenesis. When untreated, both diseases lead to the lymphocytic esophagitis show the leading cause of food
destruction of the epithelium [88]. Both celiac disease and bolus impaction in patients ˂50 years of age.
EoE need biopsy results for diagnosis, and both condi-
tions may occur despite an utterly normal appearance of Relationship between EoE and Eosinophilic
the mucosa [89]. Cholangitis
One study reported the initial endoscopic evaluation Eosinophilic cholangitis is a rare condition defined as
of 10 children with coexisting CD and EoE on histopath- an eosinophilic infiltration of the biliary tree that can lead
ological findings; their symptoms improved after a glu- to fibrosis, stricture, and biliary obstruction. Recently,
ten-free diet, topical glucocorticosteroid, and elimination Tanaka et al. [95] reported a 70-year-old female with eo-
diet [88]. Patton et al. [90] reported a cohort of 22 patients sinophilic cholangitis with a past history of EoE, who was
diagnosed with CD and EoE, in whom soy was well toler- treated with prednisolone (2.5–7.5 mg/day) for 1 year.
ated, and suggested that reintroduction of this food first, She was negative for the hepatitis virus and IgG4 staining.
or trialing a soy-inclusive dietary elimination is a viable However, marked eosinophilic infiltrates were seen on
strategy. Moreover, Vaz et al. [91] reported a patient with her biliary biopsy in the common bile duct (60 cells/HPF).
characteristic features of EoE and underwent topical and She was started with prednisolone 30 mg/day and tapered
systemic corticosteroids, in whom repeated endoscopy of the dose to 2.5 mg/day, and she was asymptomatic with-
the duodenal mucosa showed multiple papules and the out common bile duct wall thickening.
biopsies’ results were consistent with CD. Furthermore,
Ari et al. [92] evaluated both isolated CD and EoE and EoE and Type 2B von Willebrand Disease
combined CD + EoE and stated that these are 2 coexisting von Willebrand disease is the most common heredi-
entities in patients who present with combined CD + EoE tary blood-clotting disorder in humans. There are 4 he-
and they share certain characteristics with their counter- reditary types: type 1, type 2, type 3, and pseudo or plate-
parts with isolated CD and EoE. let-type. Type 2 is subdivided into 4 types: 2A, 2B, 2M,
According to Wallach et al. [89], there is greater adher- and 2N.
ence to guidelines for biopsy in which celiac disease and A case study by Corder et al. [96] reported a 20-year-
EoE are ultimately diagnosed. The diagnoses of both CD old female with type 2B von Willebrand disease with an
and EoE are associated with adequate adherence to the 8-year history of solid food dysphagia. Type 2B von Wil-
guidelines, and detection rates of the disease increase with lebrand condition is characterized by qualitative defects
increased mucosal sampling. in the “von Willebrand factor” structure or function. She
Etiological Factors, Coexisting Diseases, Digestion 2021;102:342–356 349
and Complications of EoE DOI: 10.1159/000508191had a history of bleeding ranging from recurrent epistax- Immunoglobulin G4-Related Disease
is, easy bruising, gum bleeding, prolonged menses, and 2 The role of immunoglobulin G4 (IgG4) in the develop-
severe episodes of hemoperitoneum secondary to a rup- ment of EoE is unclear. There are predominant IgG4-as-
tured ovarian cyst requiring hospitalization. Her initial sociated plasma cells up to 180–300/HPF in the deep lam-
endoscopy revealed longitudinal furrows, white plaques, ina propria in adult EoE, not an IgE-induced allergy
and edema throughout the esophagus with a severe focal [101–103].
stricture at the gastroesophageal junction. Esophageal bi- According to the study by Clayton et al. [101], esopha-
opsies revealed increased eosinophils in both the proxi- geal deposits of IgG4 in EoE arise from dense plasmacyt-
mal (60 eosinophils/HPF) and distal esophagus (80 eo- ic infiltrates in the lamina propria, which shows abundant
sinophils/HPF). She underwent multiple balloon dilation IgG4-containing plasmacytes, and IgG4 serum levels re-
13.5–18 mm with preprocedure and postprocedure pro- active to particular foods, indicating that EoE in adults is
phylaxis of human plasma-derived von Willebrand factor IgG4-associated. Moreover, Zukerberg reported 58 and
(HP-vWF-FVIII) concentrate prophylaxis. 40% of cases with EoE and GERD that were positive for
mucosal IgG4 plasmacytes, indicating that the presence
Esophageal Intramural Pseudodiverticulosis of intrasquamous IgG4 deposits is a useful adjunctive
It is a rare idiopathic benign condition characterized marker in differentiation between GERD and EoE pa-
by a flask-like outpouching of the esophageal wall that is tients [83, 104, 105].
distinguished by dilatation and inflammation of excre- These findings indicate the possible associations be-
tory ducts within submucosal glands of the esophagus. tween EoE and IgG4-related diseases. However, fibrosis
Patients with EoE and pseudodiverticulosis had signifi- is a characteristic feature of both IgG4-related disease and
cantly more food bolus obstructions. EoE, although the quality and the pattern of fibrosis are
Few cases have been reported on concomitant EoE generally different: IgG4-related disease is characterized
with pseudodiverticulosis. Scaffidi et al. [97] documented by fibrosis of the storiform type, whereas EoE has a pat-
5 patients with pseudodiverticulosis who had endoscopic tern-less fibrosis pattern [2, 104].
findings suggestive of EoE and met the histological crite-
ria of ≥15 eosinophils/HPF. Herpetic Esophagitis with EoE
Patients with EoE tend to have pseudodiverticulosis Herpes simplex esophagitis is an acute and severe viral
within the mid-to-distal esophagus, whereas patients infection of the esophagus, rarely seen in individuals with
without EoE had pseudodiverticula primarily in the prox- immunocompetence. Various studies indicated a possi-
imal esophagus. Moreover, Kathi et al. [98] reported an ble link between herpes simplex virus infection/esopha-
endoscopic and biopsy findings of a patient with dyspha- gitis and EoE [11].
gia and gastroesophageal reflux disease who was found to Both entities can be diagnosed simultaneously or one
have an esophageal pseudodiverticula along with EoE. prior to the other, raising a possible causal relationship
[106, 107]. A study by Fritz et al. [106] retrospectively
Vascular Changes in EoE evaluated 5 immunosuppressed and 11 immunocompe-
The changes in the vascular structure and function and tent herpetic esophagitis patients’ data. After herpes sim-
their association in hypertension can sometimes severely plex infection, the 5 immunosuppressed patients had re-
damage blood vessels, which can lead to a significant nar- peated biopsies, which revealed eosinophilic infiltration
rowing of blood vessels and ischemia in various tissues. in accordance with current EoE diagnostic criteria. How-
Mahjoub et al. [99] reported an esophageal biopsy of a ever, EoE was a comorbid in almost half of the 11 immu-
pediatric patient with EoE overlying small arteries within nocompetent patients. Similarly, a series of 5 adult pa-
the lamina propria showed markedly thickened media tients with herpes simplex esophagitis had histological
with medial hypertrophy to the point of obstruction. and clinical symptoms consistent with the diagnosis of
Moreover, Frech et al. [100] reported EoE patients EoE [108]. Kim et al. [109] reported an 11-year-old Ko-
with diffuse cutaneous systemic sclerosis, Raynaud’s, and rean boy suffering from fever, odynophagia, dysphagia,
skin thickening, one had facial telangiectasia and another and chest pain. His upper endoscopic examination of the
had early interstitial lung disease. The gastrointestinal distal esophagus revealed longitudinal ulcers with volca-
tract, especially the esophagus, is most commonly affect- nic appearance. The test results for a polymerase chain
ed by systemic sclerosis. reaction and biopsy samples were found positive for her-
pes simplex virus type 1. He received acyclovir and PPIs,
350 Digestion 2021;102:342–356 Khan/Guo/Liu/Iqbal/Jiang/Zhu/Chen/
DOI: 10.1159/000508191 WangTable 5. Complications associated with EoE
Conditions Characteristics
Inflammatory conditions Furrows, white exudates, edema, esophageal rings, and stenosis
Esophageal perforation Boerhaave syndrome, fibrostenotic condition, and esophageal dilatation
Hepatic portal venous gas Intraluminal gas enters the portal venous circulation due to endoscopic dilation for benign esophageal
strictures with EoE
Intramucosal dissection of Inflammatory conditions → separation of mucosa and/or submucosa → false lumen
the esophagus
Esophageal dysmotility Esophageal mucosa infiltration by eosinophils and their interactions with the microenvironment and
inflammatory cytokines
Achalasia-like changes Esophageal muscularis propria → abnormally buildup of eosinophils → myoactive and neuroactive
eosinophilic secretory products → cytotoxic eosinophil secretory products
Adrenal insufficiency Low morning serum cortisol levels
EoE, eosinophilic esophagitis.
but the follow-up esophagoscopy demonstrated typical disease, celiac disease, and EoE) was reported in a child
EoE patterns and the biopsies were consistent with the with Siderius-Hamel syndrome [111]. Thus, physicians
EoE diagnostic criteria. For immunocompetent patients should be aware of this rare occurrence while evaluating
with herpetic esophagitis, especially those with atopic patients with Siderius-Hamel syndrome.
conditions, clinical follow-up is therefore required.
Eosinophilic Subserosal Gastroenteritis with Ascites
Esophagitis Dissecans with EoE A recent study of a 30-year-old woman with increased
Esophagitis dissecans superficialis and EoE are dis- peripheral eosinophilia, IgE, and tumor marker Ca-125
tinctive esophageal conditions with characteristic clinical revealed increased thickening of the esophageal and small
and histological findings. Esophagitis dissecans superfi- bowel wall with ascites as well as marginally narrowed
cialis is an unusual endoscopic finding consisting of peel- esophageal lumen with eosinophils >15/HPF [112].
ing large esophageal mucosa fragments. Esophagitis dis-
secans patients may vomit casts of sloughed-off esopha-
geal mucosa, while others may present with dysphagia, Complications
epigastric pain, or heartburn.
Guerra et al. [110] reported a patient with both esoph- EoE is a prolonged esophageal inflammatory condi-
agitis dissecans and EoE with significant mid-esophageal tion with persistent or spontaneous course of instability.
findings of gross abnormality of ulcerations, furrowing, So far, life expectancy does not seem to be affected, but it
streaks of white layering of mucosa with sloughing, and often affects the quality of life. To date, no association be-
friability. Severe esophagitis was observed on histology tween esophageal cancer and EoE was found [113]; how-
with marked squamous epithelium infiltration of neutro- ever, there are major concerns that the prolonged, uncon-
phils and eosinophils and mucosal separation with bul- trolled inflammation may cause irreversible structural
lous spaces and ulceration. These findings together sig- changes in the esophagus, resulting in tissue fibrosis,
nify that esophagitis dissecans might be another unspe- stricture formation, and impairment of the esophageal
cific finding of EoE and the differential should be function (Table 5).
considered while encountering such conditions.
Inflammatory Conditions
Siderius-Hamel Syndrome EoE may present with an inflammatory phenotype,
It is characterized by intellectual disability and distinct such as furrows, white exudates, and edema, or strictur-
facial features. Recently, a triple association of (Crohn’s ing phenotype (rings and stenosis) [14], or a combination
Etiological Factors, Coexisting Diseases, Digestion 2021;102:342–356 351
and Complications of EoE DOI: 10.1159/000508191of them. In this regard, partial or complete esophageal flammatory cytokines might be the leading causes of
obstruction due to esophageal scarring and narrowing or esophageal dysmotility [117].
food impaction and eating difficulties are 2 important According to Martin Martin et al. [118], pan-esopha-
complications of EoE and is a medical emergency [93]. geal pressurization is associated with bolus impaction in
patients with EoE. Moreover, pan-esophageal pressuriza-
Esophageal Perforation tion has been found to be the most common esophageal
Perforation of the esophagus is a potentially serious motor abnormality assessed by high-resolution manom-
complication of EoE. To date, a few cases of spontaneous etry.
esophageal perforation have been reported in patients
with EoE, also known as Boerhaave syndrome. The pres- Achalasia-Like Changes
ence of eosinophilic infiltrates is the possible mechanism Achalasia is an impaired peristaltic condition of the
that causes epithelial inflammation to progress toward fi- esophagus due to neuronal damage in myenteric plexus
brostenotic condition that leads to esophageal remodel- resulting in incomplete relaxation of the lower esopha-
ing. This remodeling potentially deteriorates esophageal geal sphincter. However, achalasia is rarely associated
motility and often leads to dysphagia and food impaction, with EoE, the majority of patients with achalasia have ev-
and spontaneous perforation may occur as damage prog- idence of an abnormal buildup of eosinophils and/or
ress [114–116]. Moreover, Gisasola et al. [4] reported a their degranulation products in the esophageal muscula-
patient with mediastinal abscess secondary to EoE with- ris propria.
out trauma, perforation, or previous surgery. Esophageal eosinophilia may cause achalasia-like mo-
It is important to note that vomiting-induced esopha- tility defects, likely by releasing myoactive and neuroac-
geal perforation is a potentially serious complication of tive eosinophilic secretory products, which disrupt peri-
EoE. Therefore, EoE should be evaluated in patients with stalsis and interfere with lower esophageal sphincter re-
nontraumatic Boerhaave syndrome, especially young laxation, and by releasing profibrotic products causing
men with a prior history of dysphagia and allergies. tissue remodeling. Moreover, achalasia can also be caused
Endoscopic interventions for alleviating food impac- by esophageal eosinophils by releasing cytotoxic eosino-
tion may result in complications such as esophageal per- phil secretory products that destroy intramural neurons
foration due to the friability of the esophageal mucosa of the esophagus, which mediate peristalsis and lower
[116]. Because of chronic inflammation of the esophagus, esophageal sphincter relaxation. Hypothetically, it is un-
endoscopy can cause instrumental perforation, vertical clear whether the destruction of enteric neurons in acha-
mucosal lacerations, and emesis-induced rupture or tears lasia is the cause of eosinophils infiltrating the esophageal
in the esophageal lining tissue upon esophageal dilata- muscular propria, nor clear that an antigen-driven EoE
tion. Sometimes, tearing happens spontaneously. In rare mainly involves the esophagus muscle, contributing to
cases, spontaneous transmural esophageal perforation the development of abnormal esophageal motility [17,
has also been noted [14, 114]. 119]. A study by Surdea-Blaga et al. [17] reported a pa-
tient with EoE who underwent a high-resolution esopha-
Esophageal Dysmotility geal manometry and upper gastrointestinal endoscopy
In older children and adults, intermittent dysphagia for dysphagia and food impaction which revealed achala-
and food impactions are the 2 most common symptoms sia-like pattern, multiple white spots, along the entire
of EoE. However, in most cases, there is no underlying esophagus with 39 eosinophils/HPF, eosinophilic micro-
anatomical condition, which could lead to major esopha- abscesses, and basal zone hyperplasia. He was started on
geal motility disorders [117, 118]. prednisone 25 mg/day, tapered to 5 mg/week. His symp-
The etiopathogenesis is not well known for esophageal toms relieved during the treatment; however, after stop-
dysmotility. It may be associated with esophageal mucosa ping the steroids, the dysphagia reappeared. Similarly,
infiltration by eosinophils and its interactions with the Landres et al. [120] reported EoE in a patient with vigor-
microenvironment. It is unclear how eosinophilic infil- ous achalasia presented with epigastric pain, eosinophilic
tration might produce esophageal dysmotility; however, infiltration of the esophagus, and esophageal hypertro-
many speculations exist that the interaction of fibroblasts phy with predominant muscle layer involvement [120].
with eosinophils, eosinophil degranulation, binding of Further research is needed to investigate the role of eo-
the eosinophil-derived major basic protein with musca- sinophils in the pathogenesis of achalasia and other
rinic acetylcholine receptors, gastric eosinophilia, and in- esophageal motility disorders.
352 Digestion 2021;102:342–356 Khan/Guo/Liu/Iqbal/Jiang/Zhu/Chen/
DOI: 10.1159/000508191 WangIntramucosal Dissection of the Esophagus EoE and its relationship with coexisting and correlated
Acute intramucosal esophageal dissection is an un- diseases.
common complication of EoE [121, 122]. Acute intramu-
cosal dissection consists of the separation of mucosa and/
or submucosa from deeper muscular layers, resulting in Disclosure Statement
the development of a false lumen [121, 122]. The risk of
The authors have no conflicts of interest to declare.
intramucosal dissection of the esophagus is increased in
iatrogenic cases due to fragility of the esophageal mucosa,
including routine endoscopy or endoscopic manipula-
Funding Sources
tion with air insufflation, mucosal trauma during foreign
body ingestion, and inflammatory conditions, such as This study was supported by Science and Technology Plan
EoE [121, 123]. Project of Tianjin (17ZXMFSY00210).
Hepatic Portal Venous Gas
Hepatic portal venous gas is an uncommon condition Author Contributions
in which intraluminal gas or gas produced by bacteria in
the gastrointestinal tract enters the portal venous circula- S.K. contributed to the paper in writing, data collection, and
manuscript preparation. G.X. was involved in clinical studies. T.L.
tion. It is often related to significant underlying patholo- and M.Q. were involved in endoscopic imaging and literature
gies such as intestinal ischemia, sepsis, inflammatory search. K.J. contributed to the definition of intellectual content,
bowel diseases, bowel obstruction, diverticulitis, appen- data acquisition, and structural format. L.P.Z. performed review.
dicitis, and trauma. Rarely, hepatic portal venous gas after B.M.W. and X.C. contributed to the study concept, design, manu-
an upper gastrointestinal endoscopy and dilation for be- script editing, and manuscript review. All authors read and ap-
proved the final manuscript.
nign esophageal strictures with EoE has also been report-
ed in few studies [124, 125].
Geolocation Information
Adrenal Insufficiency
It is a condition of inadequate production of steroid This study was carried out in Tianjin City, People’s Republic of
hormones by adrenal glands, mainly cortisol; however, China.
the aldosterone production can also be impaired. Recent-
ly, a children-based study reported 5% of cases of EoE,
who were treated with topical corticosteroids, presented
with adrenal insufficiency [126]. However, more data and References 1 Mudde ACA, Lexmond WS, Blumberg RS,
research work are required to assess the efficacy of screen- Nurko S, Fiebiger E. Eosinophilic esophagitis:
published evidences for disease subtypes, in-
ing adrenal insufficiency in patients with EoE. dications for patient subpopulations, and how
to translate patient observations to murine
experimental models. World Allergy Organ J.
2016;9:23.
Conclusions 2 Guarino MP, Cicala M, Behar J. Eosinophilic
esophagitis: new insights in pathogenesis and
EoE is recently a more frequently occurring condition therapy. World J Gastrointest Pharmacol
Therapeut. 2016;7(1):66–77.
characterized by chronic inflammation and strictures. 3 Choudhury S, Baker S. Eosinophilic esopha-
The etiology of EoE is multifactorial and most frequently gitis: the potential role of biologics in its treat-
occurs in patients with certain risk factors such as inflam- ment. Clin Rev Allergy Immunol. 2019.
4 Gisasola P, Iriarte A, Larez MR, Casanova L,
matory mediators, genetic susceptibility, environmental Bujanda L. Mediastinal abscess, an unusual
factors, atopic conditions, and dietary products. Esopha- way of presentation of eosinophilic esophagi-
geal involvement with eosinophils may be manifested as tis. Allergy Asthma Clin Immunol. 2019;
15:12.
isolated or with coexisting conditions and should be tak- 5 Andreae DA, Hanna MG, Magid MS, Maler-
en into consideration in the differential diagnosis. There ba S, Andreae MH, Bagiella E, et al. Swallowed
could be a number of other contributing factors that can fluticasone propionate is an effective long-
term maintenance therapy for children with
lead to EoE. Therefore, significant research studies are eosinophilic esophagitis. Am J Gastroenterol.
necessary to better understand the etiopathogenesis of 2016;111(8):1187–97.
Etiological Factors, Coexisting Diseases, Digestion 2021;102:342–356 353
and Complications of EoE DOI: 10.1159/0005081916 González-Cervera J, Lucendo AJ. Eosinophil- 20 Capucilli P, Hill DA. Allergic comorbidity in 34 Rawson R, Yang T, Newbury RO, Aquino M,
ic esophagitis: an evidence-based approach to eosinophilic esophagitis: mechanistic rele- Doshi A, Bell B, et al. TGF-β1-induced PAI-1
therapy. J Investig Allergol Clin Immunol. vance and clinical implications. Clin Rev Al- contributes to a profibrotic network in pa-
2016;26(1):8–18. lergy Immunol. 2019;57(1):111–27. tients with eosinophilic esophagitis. J Allergy
7 Furuta GT, Katzka DA. Eosinophilic esopha- 21 Hruz P, Straumann A, Bussmann C, Heer P, Clin Immunol. 2016;138(3):791–800.e4.
gitis. N Engl J Med. 2015;373(17):1640–8. Simon HU, Zwahlen M, et al. Escalating inci- 35 Tkachenko E, Rawson R, La E, Doherty TA,
8 Richter JE. Current management of eosino- dence of eosinophilic esophagitis: a 20-year Baum R, Cavagnero K, et al. Rigid substrate
philic esophagitis 2015. J Clin Gastroenterol. prospective, population-based study in Olten induces esophageal smooth muscle hypertro-
2016;50(2):99–110. County, Switzerland. J Allergy Clin Immunol. phy and eosinophilic esophagitis fibrotic gene
9 Soylu A, Altintas A, Cakmak S, Poturoglu S, 2011;128(6):1349–50.e5. expression. J Allergy Clin Immunol. 2016;
Kaya H, Sevindir I, et al. The coexistence of 22 Arias Á, Lucendo AJ. Prevalence of eosino- 137(4):1270–2.e1.
eosinophilic esophagitis with allergic rhinitis. philic oesophagitis in adult patients in a cen- 36 Niranjan R, Rajavelu P, Ventateshaiah SU,
Eur Rev Med Pharmacol Sci. 2016; 20(11): tral region of Spain. Eur J Gastroenterol Hep- Shukla JS, Zaidi A, Mariswamy SJ, et al. In-
2315–23. atol. 2013;25(2):208–12. volvement of interleukin-18 in the pathogen-
10 Teoh T, Chan ES, Avinashi V, Ko HH, Gold- 23 Spergel JM, Book WM, Mays E, Song L, Shah esis of human eosinophilic esophagitis. Clin
man RD. Diagnosis and management of eo- SS, Talley NJ, et al. Variation in prevalence, Immunol. 2015;157(2):103–13.
sinophilic esophagitis in children. Can Fam diagnostic criteria, and initial management 37 Arias Á, Lucendo AJ, Martínez-Fernández P,
Physician. 2015;61(8):687–90. options for eosinophilic gastrointestinal dis- González-Castro AM, Fortea M, González-
11 Lyles J, Rothenberg M. Role of genetics, envi- eases in the United States. J Pediatr Gastroen- Cervera J, et al. Dietary treatment modulates
ronment, and their interactions in the patho- terol Nutr. 2011;52(3):300–6. mast cell phenotype, density, and activity in
genesis of eosinophilic esophagitis. Curr Opin 24 Ahmed M. Eosinophilic esophagitis in adults: adult eosinophilic oesophagitis. Clin Exp Al-
Immunol. 2019;60:46–53. an update. World J Gastrointest Pharmacol lergy. 2016;46(1):78–91.
12 Leung J, Beukema KR, Shen AH. Allergic Therapeut. 2016;7(2):207–13. 38 Iwakura N, Fujiwara Y, Tanaka F, Tanigawa
mechanisms of eosinophilic oesophagitis. 25 Gomez Torrijos E, Gonzalez-Mendiola R, Al- T, Yamagami H, Shiba M, et al. Basophil infil-
Best Pract Res Clin Gastroenterol. 2015; varado M, Avila R, Prieto-Garcia A, Valbuena tration in eosinophilic oesophagitis and pro-
29(5):709–20. T, et al. Eosinophilic esophagitis: review and ton pump inhibitor-responsive oesophageal
13 Jung DH, Yun GW, Lee YJ, Jo Y, Park H. Clin- update. Front Med. 2018;5:247. eosinophilia. Aliment Pharmacol Ther. 2015;
icopathologic analysis of proton pump inhib- 26 Ridolo E, Martignago I, Pellicelli I, Incorvaia 41(8):776–84.
itor-responsive esophageal eosinophilia in C. Assessing the risk factors for refractory eo- 39 Merves J, Chandramouleeswaran PM, Benitez
Korean patients. Gut Liver. 2016;10(1):37–41. sinophilic esophagitis in children and adults. AJ, Muir AB, Lee AJ, Lim DM, et al. Altered
14 Nguyen N, Furuta GT, Menard-Katcher C. Gastroenterol Res Pract. 2019;2019:1–9. esophageal histamine receptor expression in
Recognition and assessment of eosinophilic 27 Gentile N, Katzka D, Ravi K, Trenkner S, eosinophilic esophagitis (EoE): implications
esophagitis: the development of new clinical Enders F, Killian J, et al. Oesophageal narrow- on disease pathogenesis. PloS One. 2015;
outcome metrics. Gastroenterol Hepatol. ing is common and frequently under-appre- 10(2):e0114831.
2015;11(10):670–4. ciated at endoscopy in patients with oesopha- 40 García-Rojo M, Sánchez J, de la Santa E,
15 Cheng E, Zhang X, Wilson KS, Wang DH, geal eosinophilia. Aliment Pharmacol Ther. Durán E, Ruiz JL, Silva A, et al. Automated
Park JY, Huo X, et al. JAK-STAT6 pathway 2014;40(11–12):1333–40. image analysis in the study of lymphocyte
inhibitors block eotaxin-3 secretion by epi- 28 D’Alessandro A, Esposito D, Pesce M, Cuomo subpopulation in eosinophilic oesophagitis.
thelial cells and fibroblasts from esophageal R, De Palma GD, Sarnelli G. Eosinophilic Diagn Pathol. 2014;9(Suppl 1):S7.
eosinophilia patients: promising agents to im- esophagitis: from pathophysiology to treat- 41 Dellon ES, Gonsalves N, Hirano I, Furuta GT,
prove inflammation and prevent fibrosis in ment. World J Gastrointest Pathophysiol. Liacouras CA, Katzka DA. ACG clinical
EoE. PloS One. 2016;11(6):e0157376. 2015;6(4):150–8. guideline: evidenced based approach to the
16 Shoda T, Morita H, Nomura I, Ishimura N, 29 Rothenberg ME. Molecular, genetic, and cel- diagnosis and management of esophageal eo-
Ishihara S, Matsuda A, et al. Comparison of lular bases for treating eosinophilic esophagi- sinophilia and eosinophilic esophagitis (EoE).
gene expression profiles in eosinophilic tis. Gastroenterology. 2015;148(6):1143–57. Am J Gastroenterol. 2013;108(5):679–93.
esophagitis (EoE) between Japan and West- 30 Min SB, Nylund CM, Baker TP, Ally M, Rein- 42 Gambichler T, Kröger ES, Tannapfel A, Dör-
ern countries. Allergol Int. 2015;64(3):260–5. hardt B, Chen YJ, et al. Longitudinal evalua- ler M, Susok L. Hypereosinophilic syndrome
17 Surdea-Blaga T, David L, Botan EC, Dumi- tion of noninvasive biomarkers for eosino- complicated by severe vascular damage and
trascu DL. Achalasia-like changes in eosino- philic esophagitis. J Clin Gastroenterol. 2016; gangrene. J Vasc Surg Cases Innov Tech.
philic esophagitis. J Gastrointest Liver Dis. 51(2):127–35. 2019;5(3):384–7.
2019;28:146. 31 Dellon ES, Speck O, Woodward K, Covey S, 43 Spechler SJ. Eosinophilic esophagitis: novel
18 Sayej WN, Ménoret A, Maharjan AS, Fernan- Rusin S, Gebhart JH, et al. Markers of eosino- concepts regarding pathogenesis and clinical
dez M, Wang Z, Balarezo F, et al. Character- philic inflammation for diagnosis of eosino- manifestations. J Gastroenterol. 2019; 54(10):
izing the inflammatory response in esopha- philic esophagitis and proton pump inhib 837–44.
geal mucosal biopsies in children with eosino- itor-responsive esophageal eosinophilia: a 44 Cianferoni A. Wheat allergy: diagnosis and
philic esophagitis. Clin Transl Immunology. prospective study. Clin Gastroenterol Hepa- management. J Asthma Allergy. 2016; 9:13–
2016;5(7):e88. tol. 2014;12(12):2015–22. 25.
19 Savarino EV, Tolone S, Bartolo O, de Cassan 32 Jiang M, Ku WY, Zhou Z, Dellon ES, Falk 45 Arasi S, Costa S, Magazzù G, Ieni A, Crisaful-
C, Caccaro R, Galeazzi F, et al. The GerdQ GW, Nakagawa H, et al. BMP-driven NRF2 li G, Caminiti L, et al. Omalizumab therapy in
questionnaire and high resolution manome- activation in esophageal basal cell differentia- a 13-year-old boy with severe persistent asth-
try support the hypothesis that proton pump tion and eosinophilic esophagitis. J Clin In- ma and concomitant eosinophilic esophagi-
inhibitor-responsive oesophageal eosinophil- vest. 2015;125(4):1557–68. tis. Ital J Pediatr. 2016;42:32.
ia is a GERD-related phenomenon. Aliment 33 Lucendo AJ. Cellular and molecular immu-
Pharmacol Ther. 2016;44(5):522–30. nological mechanisms in eosinophilic esoph-
agitis: an updated overview of their clinical
implications. Expert Rev Gastroenterol Hepa-
tol. 2014;8(6):669–85.
354 Digestion 2021;102:342–356 Khan/Guo/Liu/Iqbal/Jiang/Zhu/Chen/
DOI: 10.1159/000508191 WangYou can also read