Arthroscopy Reconstruction Surgery for Chronic Scapholunate Injury with ILA - Internal Ligament Augmentation - GMReis
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Arthroscopy Reconstruction Surgery for Chronic
Scapholunate Injury with ILA - Internal Ligament
Augmentation
Márcio Aita , MD
Literature Review
The scapholunate ligament (SLL) is the most commonly When all above coexist in a wrist with SL gap reducible,
injured intercarpal ligament of the wrist. Ligaments are not DISI, abnormal coronal/sagittal misalignment, radio
merely static cables binding bones together, but complex lunate relationship, and peri scaphoid cartilages normal,
arrangements of dense collagen fibers that contain sensorial SLL reconstruction (360°) associated with dorsal/palmar
elements (mechanoreceptors) able to detect changes in capsulodesis using the palmaris longus (PL), brachiorradialis
carpal bone postion, and transmit this information to the (BR), flexor carpi radialis(FCR) tendon graft, ILA - Internal
sensorimotor system for centralized control of neuromuscular Ligament Augmentation with Fastlock GMReis, assisted by
joint stabilization. Although SLL ( volar and dorsal portions) arthroscopy offered clinically significant procedural and
is the primary stabilizer of the scapholunate (SL) joint, the functional advantages (4).
scaphotrapeziotrapezoid (STT), radioscaphocapitate (RSC),
and radiolunate (RL) ligaments may also contribute to SL
stability.
Diagnosis is often delayed owing to the lack of radiographic
findings [dorsal intercalated segmental instability (DISI),
Terry-Thomas signal, and ring signals] and is made following
chronic failure (instability) of the joint and wrist pain.
Treatment of acute instability usually involves stabilization
and ligament suturing using cast immobilization. Though
the ligament healing process generally requires eight weeks
until one year (Sharpey fibers formation), particularly when
the condition is under diagnosed.
Fig.: GMReis Ø3.5 x 8.5 mm Fastlock SA Knotless Tape Loaded Anchor with open eyelet.
Treatment of chronic lesions depends on the Clinical
symptoms: pain, weakness, click, functional disability and
presence of viable ligament fibers based on radiographic
findings (if reducible, DISI deformity, Terry-Thomas signal, Surgical Technique
and ulnar translation of the lunate); signs of post-traumatic
osteoarthritis (SLAC lesion) may require scapholunate Diagnostic arthroscopy is an important tool to identify the cause
ligament portion repair, dorsal or palmar capsulodesis, of wrist pain in cases where SL dissociation may be associated
SL reconstruction only or associated with capsulodesis, with other pathologies.
other ligaments reconstructions (STT, RSC, RL) or salvage The surgery was performed under general anesthesia. The
procedures, as partial arthrodesis. patient was placed in a dorsal recumbent position, with the
arm suspended in a specific wrist traction tower, under 10–13
Indications lb of traction. A tourniquet was inflated or passed. Continuous
To determine whether these procedures can be performed via irrigation with saline solution was achieved with a pump and
arthroscopy and the advantages there of, we performed the specific equipment under the action of gravity.
following arthroscopically:
An inventory of the radio carpal joint was made initially through
• SL diagnosis: dissociation is complete and repairable
portals 3–4, 4–5, and 6 R for the saline solution exit; the mid
• Debridement: if carpal misalignment is easily reducible or to
perform SL interval debridement for to reduction that interval carpal joint was assessed through the radial (MCR) and ulnar
• Cartilage: periscaphoid cartilage is normal
(MCU) portals. Small transverse incisions were made along the
skin folds for a better scar appearance.
• Lunate: sagital or coronal misalignment, indicating a radoiocarpal
derangement
1-4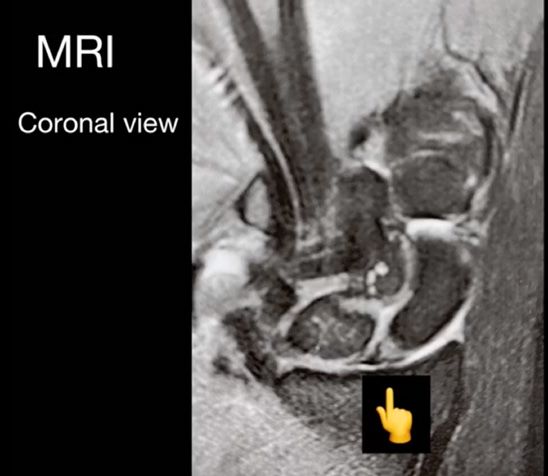
Arthroscopy Reconstruction Surgery for Chronic Scapholunate Injury
with ILA - Internal Ligament Augmentation
Márcio Aita, MD
Arthroscope measuring 2.7 mm was used. The joint was The tendon graft was prepared with with GMReis Stitch
systematically inspected and the results were documented. Surgical Tape to perform ILA - Internal Ligament Augmentation,
When necessary, radial debridement was performed at the continuous Krackow suture and passed through bone tunnels
same time, with 2-mm and 2.9-mm shaver blades. Intra- with specific (grooved) needles or wires from the palmar to the
articular fibrosis was removed to improve wrist mobility and to dorsal side of the scaphoid and from the dorsal to the palmar
promote gap reduction and SL alignment, as well as to correct aspect of the lunate. The tendon graft was passed outside the
DISI deformity. dorsal capsule, so that it was reinserted linearly under the SL
gap (linear capsulodesis).
The rebuilding step was initiated with a 3cm lateral incision
along the proximal transverse fold of the wrist to identify the The fixation of the graft in the palmar radius bone tunnel
insertion of the brachiorradialis tendon (BR). BR graft was with GMReis Ø3.5 x 8.5 mm Fastlock Knotless Tape Loaded
extracted with or without the use of a tendon stripper. A 2 mm Anchor was perdormed. The final part of the graft was sutured
proximal incision was made in the fascia of the anterior-lateral at the same site of the graft entry point into the scaphoid
forearm to identify the myotendinous transition of the BR, in (reconstruction of the palmar portion of the SL ligament). The
order to excise it. Both dorsal and volar joint capsules were mid. carpal joint was once again inspected through the MCR
preserved, unaltered. At that moment, the wrist was ready for or MCU portal. The SL gap was once again inspected with
the preparation of the bone tunnels. probe tweezers, as described by Geissler. This interval should
be closed. Any tissue interposition in the SL gap pre-venting a
Fluoroscopy was used to assess the wrist. If a DISI deformity was complete reduction, was arthroscopically removed. SL stability
observed, the extended lunate position would be corrected by was confirmed by arthroscopy and fluoroscopy.
flexion of the wrist to restore the normal radio lunate angle
and the radio ulnar joint, with fixation or not with a 1.6 mm The layers were cleaned and sutured, and a plaster cast was
Kirschner wire inserted percutaneously. placed. Two weeks postoperatively, the plaster cast was
removed; all patients started rehabilitation in occupational
The wrist was then passively extended to correct the flexion therapy.
deformity of the scaphoid and restore a normal SL angle. If these
corrections were not achieved, additional arthroscopic release
of the fibrosis around the scaphoid and lunate was performed.
If it was still impossible to reduce the DISI deformity, then Surgical Technique
ligament reconstruction would be abandoned; fortunately, this
The reconstruction performed for our patient is appropriate
did not occur in this study. Through the dorsal portals 4–5 or 6
for complete, irreparable SLL injury with reducible
R, MCR, or MCU, a 1.1 mm guide wire was placed inside a soft
misalignment that has been diagnosed early; however, this
tissue protector (drill guide) on the lunate and scaphoid under
procedure is not appropriate for patients with irreducible
fluoroscopic guidance. When the radius and lunate were well
carpal misalignment and post traumatic arthritis.
aligned with the guide wire, the direction of the radius should
be perpendicular to the long axis of the lunate; i.e., parallel to
the line joining the tip of volar and dorsal lips of the lunate
(lateral view). The guide wire was advanced 2–3 mm from the Tips and Tricks
bone margin and then toward the volar cortex. With the flexor The choice of a tendon graft used in this patient is novel and
tendons and median nerve, including the palmar cutaneous offers several advantages.
branch, carefully moved to the ulnar side, the exit of this wire
was identified. Another guide wire was then inserted into the The small diameter and the direction of the bone tunnels averts
scaphoid through the 3–4 dorsal portal. It was placed parallel complications such as iatrogenic fractures of the scaphoid and
or oblique to the lunate guide wire, provided that the SL angle lunate.
had been corrected. Otherwise, its entrance should be slightly
The insertion is preserved and helps during the surgical
more distal than that of the lunate guide wire; it should be
procedure to stress the graft and auxiliary materials into
moved toward the palmar and proximal direction to provide
floating lunate reduction. The tendon graft is adjacent to
a better correction of the scaphoid rotation and flexion. With
the radiocarpal joint to avoid an additional surgical site. The
the flexor carpi radialis tendon radially moved, the scaphoid
function of the donor forearm is not affected by the withdrawal
wire was advanced through the volar face. Both tunnels were
of the tendon graft.
sequentially enlarged with 2.0, 2.7, or 3 mm cannulated drills,
depending on the thickness of the tendon graft. The drill of When we seek that procedure, we don’t burn any bridges and
smallest possible diameter should be used to ensure a smooth so other techniques can be done in case it fails.
passage of the graft and avoid iatrogenic fracture or avascular
necrosis of these bones. In our point of view, successful surgery performed on our
2-4
Arthroscopy Reconstruction Surgery for Chronic Scapholunate Injury
with ILA - Internal Ligament Augmentation
Márcio Aita, MD
patients for SLL reconstruction via arthroscopy is attributable
to our efforts to preserve the dorsal capsule, to promove dorsal
and palmar capsulodesis (reconnection capsules with bones)
and the technique provided the best view of the radio carpal
and mid carpal joints and was less invasive.
The choice of the GMReis Ø3.5 x 8.5 mm Fastlock promoting the
maintenance stable of scapho lunate interval with advantageous:
• To create safety bone tunnel about 3.5mm into palmar face of the
distal radius (avoid iatrogenic fracture in carpal bones);
Figs.: Diagnosis aspects: MRI (magnetic resonance image) x Wrist Arthroscopy
• Without implants or knot around the first carpal row (avoid pain
(midcarpal view) showing SLIL with SL gap, Geissler test positive (probe pass into
and impact in radio carpal or mid carpal joint);
interval SL) and classification by IWAS 3b (palmar portion lesion).
• The good solution to reducing lunate translation (avoid secondary
dislocation or re-gap scapho-lunate because re-connect radio
carpal joint),
• Use Stitch tape versus wire (high resistance system to maintain
360º SLIL reconstruction technique).
Complications
Bone tunnel iatrogenic fractures, stiffness, sensorial
branches symptoms, and recurrence of scapho lunate
interval may occur after ligament reconstruction or
repair.
Conclusion Figs.: To perform SL 360º reconstruction technique, assisted by wrist arthroscopy.
To pass: guide wire (1.6 mm), drill (2.7 mm) and tendon graft / ILA - Internal
SL lesion of the carpus is commonly encountered. Ligament Augmentation into scaphoid / lunate in wrist neutral position. After,
This lesion is characterized by an unusual pass drill (3.5 mm), unicortical, palmar to dorsal direction, in distal radius and
appearance on radiographs, with subtle fix tendon graft with GMReis Ø3.5 mm Fastlock Knotless Tape Loaded Anchor.
abnormalities. Radiographic findings of the wrist
may be evident, though not always, such as the
Te r r y -T h o m a s a n d r i n g s i g n a l s f r o m a p o s t e r i o r –
a n t e r i o r ( PA ) v i e w a n d D I S I d e f o r m i t y f r o m a
l a t e r a l v i e w. T h e S L l e s i o n m a y a l s o b e e v i d e n t
as an increased scapho lunate space, which has
b e e n a s s o c i a t e d w i t h t h e u l n a r c a r p a l “r o c k i n g
c h a i r s i g n” f o r f l o a t i n g l u n a t e . Va r i a t i o n s i n
normal scapho lunate space raise the need for a
comparison with radiographs of the unaffected
wrist.
Thus, ligament reconstruction (360º) with dorsal/
palmar capsulodesis, with ILA - Internal Ligament
Fig.: Post op Radiographic aspects: Arthroscopy Reconstruction Surgery for Chronic
A u g m e n t a t i o n u s i n g Ø 3 . 5 m m Fa s t l o c k K n o t l e s s Scapholunate ligament lesion with ILA - Internal Ligament Augmentation. Check
Ta p e L o a d e d A n c h o r, p r o m o t i n g t h e m a i n t e n a n c e maintenance stable of scapho lunate interval and good relationship radio carpal
stable of scapho lunate inter val, assisted by joint.
a r t h r o s c o p y, i m p r o v e s m e c h a n o c e p c i o n a n d j o i n t
s t a b i l i t y.
Fu r t h e r, w e b e l i e v e t h a t t h i s i n j u r y s h o u l d n o t
be considered as a simple ligament rupture but a
c o m p l e x c a r p a l i n s t a b i l i t y. Fi n a l l y, p a t i e n t s w e r e
satisfied with the procedure and no complications
were noted, a longer follow-up period is needed
o w i n g t o t h e p a t i e n t ’s a c t i v i t i e s .
3-4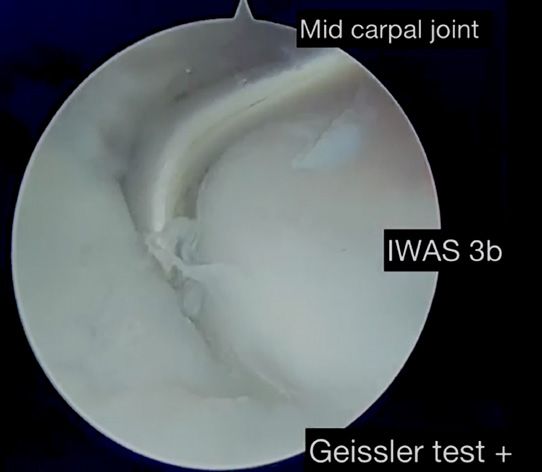
Arthroscopy Reconstruction Surgery for Chronic Scapholunate Injury
with ILA - Internal Ligament Augmentation
Márcio Aita, MD
FASTLOCK IMPLANT
CODE DESCRIPTION
320-35085-SA Fastlock Knotless Tape Loaded PEEK Anchor Ø3.5 x 8.5 mm Open eyelet
References:
1. Linscheid RL, Dobyns JH, Beabout JW, Bryan RS. Traumatic instability of the wrist. Diagnosis, classification, and pathomechanics. J Bone Joint Surg Am 1972;54:1612–32.Diagnosis,
classification, and pathomechanics. J Bone Joint Surg Am 1972;54:1612–32;
2. Garcia-Elias M, Lluch AL, Stanley JK. Three-ligament tenodesis for the treatment of scapholunate dissociation: indications and surgical technique. J Hand Surg Am. 2006;31(1):125e134;
3. Short WH, Werner FW, Green JK, Masaoka S. Biomechanical evaluation of the ligamentous stabilizers of the scaphoid and lunate: Part II. J Hand Surg Am. 2005;30(1): 24e34;
4. Short WH, Werner FW, Green JK, Masaoka S. Biomechanical evaluation of ligamentous stabilizers of the scaphoid and lunate. J Hand Surg Am. 2002;27(6):991e1002;
5. Mitsuyasu H, Patterson RM, Shah MA, Buford WL, Iwamoto Y, Viegas SF. The role of the dorsal intercarpal ligament in dynamic and static scapholunate instability. J Hand Surg Am.
2004;29(2): 279e288;
6. Rosati M, Parchi P, Cacianti M, Poggetti A, Lisanti M. Treatment of acute scapholunate ligament injuries with bone anchor. Muscu- loskelet Surg. 2010;94(1):25e32;
7. Rohman EM, Agel J, Putnam MD, Adams JE. Scapholunate inter- osseous ligament injuries: a retrospective review of treatment and outcomes in 82 wrists. J Hand Surg Am.
2014;39(10):2020e2026;
8. Zarkadas PC, Gropper PT, White NJ, Perey BH. A survey of the surgical management of acute and chronic scapholunate instability. J Hand Surg Am. 2004;29(5): 848e857;
9. Chennagiri RJ, Lindau TR. Assessment of scapholunate instability and review of evidence for management in the absence of arthritis. J Hand Surg Eur Vol 2013;38:727–38;
10. Delétang F, Segret J, Dap F, Dautel G. Chronic scapholunate instability treated by scaphocapitate fusion: a midterm outcome perspective. Orthop Traumatol Surg Res 2011;97:164–
71;
11. Berger RA, Imeada T, Berglund L, An KN. Constraint and material properties of the subregions of the scapholunate interosseous ligament. J Hand Surg Am 1999;24:953–62;
12. Chabas JF, Gay A, Valenti D, Guinard D, Legré R. Results of the modified Brunelli tenodesis for treatment of scapholunate instability: a retrospec- tive study of 19 patients. J Hand
Surg Am 2008;33:1469–77;
13. Surdziel P, Romanowski L, Czarnecki P, Kaczmarek L, Splawski R. Dynamic correction of scapholunate instability using ECRB tendon transfer. Ortop Traumatol Rehabil 2006;8:134–8;
14. De Carli P, Donndorff AG, Gallucci GL, Boretto JG, Alfie VA. Chronic scapholunate dissociation: ligament reconstruction combining a new extensor carpi radialis longus tenodesis
and a dorsal intercarpal ligament capsulodesis. Tech Hand Up Extrem Surg 2011;15:6–11;
15. Moran SL, Ford KS, Wulf CA, Cooney WP. Outcomes of dorsal capsulodesis and tenodesis for treatment of scapholunate instability. J Hand Surg Am. 2006;31(9):1438–46;
16. Taleisnik J. Wrist anatomy function and injury. In: Instructional Course Lectures, The American Academy of Orthopaedic Surgeons. St Louis: Mosby; 1978;27:61–87;
17. Mayfield JK. Patterns of injury to carpal ligaments. A spectrum. Clin Orthop Relat Res 1984;(187):36–42;
18. Short WH, Werner FW, Sutton LG. Dynamic biomechanical evaluation of the dorsal intercarpal ligament repair for scapholunate instability. J Hand Surg Am. 2009;34(4): 652–9;
19. Yi IS, Firoozbakhsh K, Racca J, Umeda Y, Moneim M. Treatment of scapholunate dissociation with palmaris longus tendon graft: a biomechanical study. Univ Pennsylvania Orthop
J 2000;13:53–9;
20. Zdero R, Olsen M, Elfatori S, Skrinskas T, Nourhosseini H, Whyne C, Schemitsch EH, von Schroeder H. Linear and torsional mechanical characteristics of intact and reconstructed
scapholunate ligaments. J Biomech Eng. 2009;131(4):041009;
21. Ho PC, Wong CW, Tse WL. Arthroscopic-Assisted Combined Dorsal and Volar Scapholunate Ligament Reconstruction with Tendon Graft for Chronic SL Instability. J Wrist Surg.
2015;4(4): 252-63;
22. Hagert E, Ljung BO, Forsgren S. General innervation pattern and sensory corpuscles in the scapholunate interosseous ligament. Cells Tissues Organs. 2004;177(1):47-54;
23. Hagert E, Forsgren S, Ljung BO. Differences in the presence of mechanoreceptors and nerve structures between wrist ligaments may imply differential roles in wrist stabilization.”
J.Orthop Res. 2005;23(4):757-63;
24. Hagert E, Garcia-Elias M, Forsgren S, Ljung BO. “Immunohistochemical analysis of wrist ligament innervation in relation to their structural composition.” J Hand Surg Am.
2007;32(1):30-6;
25. Overstraeten LV, Camus EJ, Wahegaonkar A, Messina J, Tandara AA, Binder AC, et al. Anatomical Description of the Dorsal Capsulo-Scapholunate Septum (DCSS)-Arthroscopic
Staging of Scapholunate Instability after DCSS Sectioning. J Wrist Surg. 2013;2(2):149-54;
26. Marcuzzi A, Leti Acciaro A, Caserta G, Landi A. Ligamentous reconstruction of scapholunate dislocation through a double dorsal and palmar approach. J Hand Surg Br.
2006;31(4):445–9;
27. Corella F, Del Cerro M, Larrainzar-Garijo R, et al. Arthroscopic ligamentoplasty (bone–tendon- tenodesis). A new surgical technique for scapholunate instability: preliminary
cadaver study. J Hand Surg Eur Vol. 2011;36:682–9;
28. Carvalho VB, Ferreira CHV, Hoshino AR, Bernardo VA, Ruggiero GM, Aita MA. Dorsal capsulodesis associated SL ligament reconstruction assisted by arthroscopy using the tendon
graft by palmaris longus. RBO 2016 - accept;
29. Brunelli GA, Brunelli GR. A new technique to correct carpal instability with scaphoid rotary subluxation: a preliminary report. J Hand Surg Am. 1995;20(3 Pt 2):S82–S5.
GMReis Educational Resources - Technical Report TR0009 - Rev. 00 4-4
You can also read