BNP Workshop Greater Manchester & Cheshire Cardiac and Stroke Network - Regent House Heaton Lane
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

BNP Workshop
Greater Manchester & Cheshire Cardiac and Stroke Network
Thanks to Alison Bali, Joanne Langton & Amanda Schofield
Regent House
Heaton Lane
Stockport 24th April 2012
SK4 1BS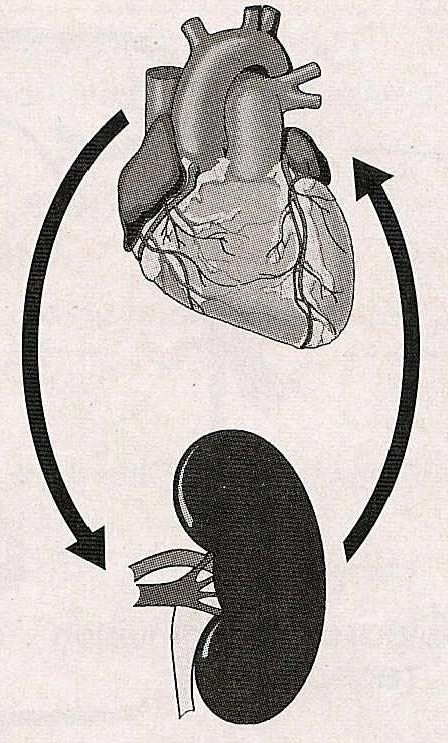
Programme 10:00 – 10:05 Welcome & Introduction – Dr Sanjay Arya, Consultant Cardiologist, Wrightington, Wigan & Leigh NHS FT (RAEI) 10:35 – 11:05 The Bolton Experience – Gilbert Wieringa, Consultant Biochemist, Bolton NHS FT 10:05 – 10:35 Work of the BNP Steering Group & Brief Overview of Wigan Service – Dr Sanjay Arya, Consultant Cardiologist, Wrightington, Wigan & Leigh NHS FT (RAEI) 11:05 – 11:35 Commissioning a BNP Service – Dr Shikha Pitalia, Director of SSP Health & Chair of United League Commissioning (a practice based commissioning organisation in the North West) 11:35 – 12:30 Question & Answer Session, Evaluation & Close
Heart Failure Common final pathway for all cardiac diseases Malignant manifestation of Coronary Heart Disease Survival rates as bad as cancer of colon Worse than Ca of breast, uterus, cx, bladder & prostate 40% of patients with HF die within a year 5% of all deaths in the UK are due to heart failure Worse QOL compared to Arthritis, Chronic lung disease or Angina
NSF (March 2000); NICE (July 2003) Accounts for 5% of all medical admissions 16% (1 in 6) of patients with HF get admitted 38% (4 in 10) of patients get re-admitted within 6 months Average length of stay is 13.3 days In England 1 million inpatient bed days are due to HF Annual cost of HF to the NHS £716 million (2001)
The prevalence of heart failure
The Echocardiographic Heart of England Study
25
20
Percentage with definite heart failure
15
10
5
0
45-54 55-64 65-74 75-84 85+
Age group (years)
EPIDEMIOLOGY AND HEALTH
Men Women SERVICE IMPACT
Davies et al, Lancet, 2001
EPIDEMIOLOGY AND HEALTH
SERVICE IMPACT
The incidence of heart failure
The Hillingdon Heart Failure Study
Median age at first presentation
18 is 76 years
16
14
(new cases/1000 population/year)
12
10
Incidence
8
6
4
2
0
25-34 35-44 45-54 55-64 65-74 75-84 85+
Age group (years)
Men Women
Cowie et al, Eur. Heart J., 1999
HEART FAILURE IS DIFFICULT TO DIAGNOSE
DIAGNOSTIC ACCURACY
FINLAND STUDY 32%
UK STUDY 29%
ECHOES 22%
NO ONE SYMPTOM, SIGN OR COMBINATION OF SYMPTOMS AND / OR
SIGNS IS ABSOLUTELY SENSITIVE OR SPECIFIC FOR THE DIAGNOSIS
OF HEART FAILURE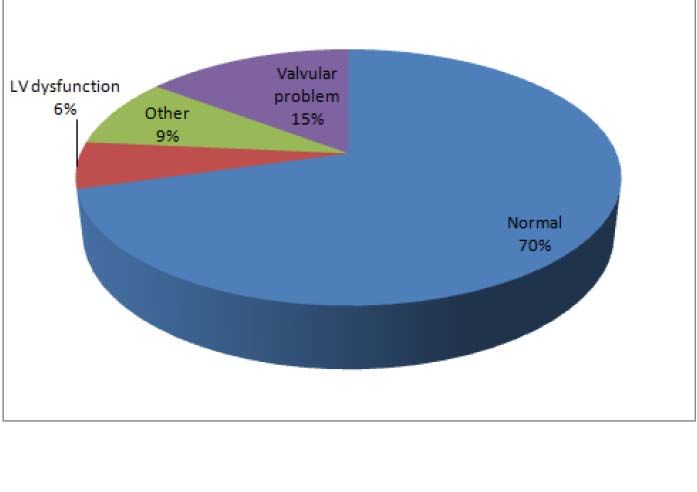
Symptoms
SENSITIVITY SPECIFICITY
SOBOE 66 52
ORTHPNOEA 21 81
ANKLE OEDEMA 23 80
PND 33 76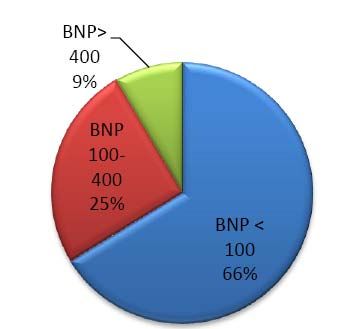
SIGNS
SENS SPECP
ELEVATED JVP 10 97
SWOLLEN ANKLES 23 80
PULMONARY CRACKLES 13 91
TACHYCARDIA 7 99
DISPLACED APEX 40 96
GALLOP RHYTHM 31 95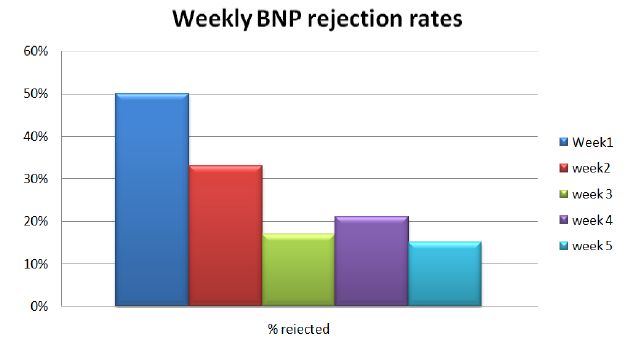
NICE Aug 2010
NTBNP>2000
NTBNP 400-2000
NTBNPSanjay Arya
MBBS (Hons), FRCP (London), FRCP (Glasgow)
Consultant Cardiologist, Royal Albert Edward Infirmary, Wigan
Honorary Senior Lecturer, University of Central Lancashire
Lecturer, British Heart Foundation
Brain Natriuretic Peptides in the diagnosis of
Heart Failure – Wigan ExperienceBrain Natriuretic Peptide (BNP)
BNP
(Distress hormone)
Pathophysiology of HF
Amino-acid peptide
Myocardial Injury
secreted by the ventricles in
(MI, IHD, HT etc)
response to ventricular volume
expansion & pressure overload
Inhibits the action of RAAS Activation of the RAAS
and SNS BNP and SNS
Peripheral vasodilatation
Peripheral vasoconstrictio
Sodium excretion
Sodium retention
Water excretion
Water retention
Inhibit myocardial fibrosis
Myocardial fibrosisBNP level for the prediction of clinical
outcome
45
Death or CHF Hospitalization (%)
40
35
30
BNP >480 pg/mL
25
20
15
BNP 230-480 pg/mL
10
5 BNPAudit: Echo requests by GPs for HF ( Nov-Dec 2004)
Total 42
Good LV 23 (55%)
Mild LVD 15 (36%)
Moderate LVD 3 (7%)
Severe LVD 1 (2%)
Positive yield 45%
42 Echo @ £100/echo = £4200
(76x12x=912 = £27142/year)
42 BNP @ £25 = £1050
19 Echo @ £100 = £1900
Total = £ 2950
Saving = £ 1250Wigan Heart Failure Service
1. GP suspects Heart Failure
2. Fills the NT-Pro BNP referral form and
sends patient’s blood to the hospital lab
3. If NT-Pro BNP high, the referral form is faxed to cardiology dept
4. Echo performed – one copy to GP and one copy on my desk
5. Echo and clinical details on form reviewed by me:
a. Letter of advice to GP
b. OPD arranged, only if necessary
c. Refer to Acute trust/Community HF nursesNT-Pro BNP Wigan Experience
WIGAN WIGAN
BNP audit Oct 05-July 06 June 08-Sept 08
(10 months) (3 months)
Total number of BNP tested 200 (10/month) 228 (76/month)
Total number of positive BNP 76 (38%) 110 (48%)
Number of patients who did not
require Echo (Unlikely to be HF) 114 (62%) 118 (52%)
Cost of Direct Echo (£ 100/echo) £20,000 £ 22,800
Cost of BNP (£ 25 / test) £5000 £ 5700
Cost of Echo for BNP +ve patients £7600 £11,000
Net saving £7400 £ 6,100 (£24k)
Extra BNP 296 244 (960)
Extra Echo 74 61 (240)Echo findings in BNP Positive patients
WIGAN WIGAN ST HELENS
Oct 05 – July 06 June 08 – Aug 08 Oct08 – Sept09
BNP Positive patients 76 110 40 (7 no echo)
Echocardiogram:
Systolic Heart Failure 24/76 (32%) 35/110 (32%) 15/40 (38%)
No systolic heart failure 52/76 (68%) 75/110 (68%) 25/40 (62%)
-AF, Valve disease, Pul HT 47/52 (90%) 60/75 (80%) 16/25 (64%)
-Completely Normal Echo 5/52 (10%) 15 /75 (20%) 9/25 (36%)
Patients have reasons for
Breathlessness 71/76 (93%) 95/110 (86%) 31/40 (78%)Early diagnosis leads to early treatment and reduced morbidity and mortality
WWL NHS Trust Platt Bridge area Atherleigh/Patient Focus
BNP blood test 30 days 21 days 11 days
to
Echocardiogram
----------------------------------------------------------------------------------------------------------
Echocardiogram 73 days 22 days 19 days
to
Cardiologist
Consultation
----------------------------------------------------------------------------------------------------------
BNP blood test 103 days 43 days 30 days
to (3.5 months) (1.5 months) (1 month)
Cardiologist
ConsultationTotal number of BNP echo 90
No action needed 46 (51%) had no significant abnormality
noted on echo: mild valve disease, mild LA
dilatation, mild PHT etc, Non HF causes
i.e. no OPD visit required
Advice given by me to GP 27 (30%) had significant abnormality
but advice given by me should be
sufficient for patient management (very
elderly, dementia, multiple comorbidities)
i.e. no OPD visit required
OPD arranged by me for 17 (19%) had significant abnormality
cardiologist opinion ie. OPD visit requiredConclusions: BNP is cost effective in the diagnosis / exclusion of Heart Failure Early diagnosis of heart failure Early treatment of heart failure Reduced hospital admissions Prevents un-necessary echo and reduces echo waiting list Reduced referrals to Cardiology clinics by 81%
Is the NICE guideline cut-off value of NTProBNP >400pg/ml satisfactory for the diagnosis of heart failure? NT-pro BNP sample = 60 (Oct – Nov 2010) NT ProBNP < 400 (n=34) NT ProBNP > 400 (n=26) Mod/Severe LVD 3 (9%) Mod/Severe LVD 6 (23%) Mild LVD 3 (9%) Mild LVD 5 (19%) Pul HT 7 (20%) Pul HT 6 (23%) AF 0 AF 4 (15%) Valve disease 2 (6%) Valve disease 1 (4%) Normal Echo 19 (56%) Normal Echo 4 (15%)
Is the NICE guideline on time frame for echo achievable? NTProBNP >2000 2 weeks n = 4/26 (15%) = 0% NTProBNP 400-2000 6 weeks n = 22/26 (85%) = 77% We are now fully compliant on time frame for echo, both at WWL and in the community
Brain Natriuretic Peptide (BNP)
1. As a diagnostic aid:
A normal level makes the diagnosis of HF unlikely (Rule out test for HF)
A high level supports the diagnosis only if high clinical suspicion of HF (Does not
confirm the diagnosis)
Breathing not properly (BNP) multinational study: NEJM 2003; 347: 161-7
Sensitivity: 90% Negative predictive value: 89%
Specificity: 76% Positive predictive value: 79%
Primary care study (where less cardiac decompensation) (Lancet 1997; 350: 1347-51
Sensitivity: 97% Negative predictive value: 98%
Specificity: 84% Positive predictive value: 70%Brain Natriuretic Peptide (BNP)
2. Assessment of severity
Patients with more severe heart failure have higher levels
3. As a prognostic aid
• Useful in risk stratification
• High BNP is associated with poor prognosis (Increased morbidity and mortality
• BNP 5 fold higher in non-survivors than in survivors (Circulation1997;96: 509
4. As a monitoring tool
• BNP levels fall after treatment with diuretics, ACEI and BB
• Targeting therapy to BNP levels improves morbidity and mortality
• Fewer death, hospital admission or heart failure in group receiving therapy
titrated to plasma NT-proBNP (Lancet 2000; 355: 1126-30)
• Failure of BNP levels to fall after optimum therapy is associated with a poorer
outlookwww.camlt.org/DL_web/946_BNP.html
Non-Heart Failure causes of High BNP
Cardiac: LVH
Ischaemia
Tachycardia (AF)
RV overload (Pulmonary Hypertension)
Renal dysfunction (eGFRGreater Manchester & Cheshire
Cardiac and Stroke Network
BNP workshop
The Bolton experience
Gilbert Wieringa
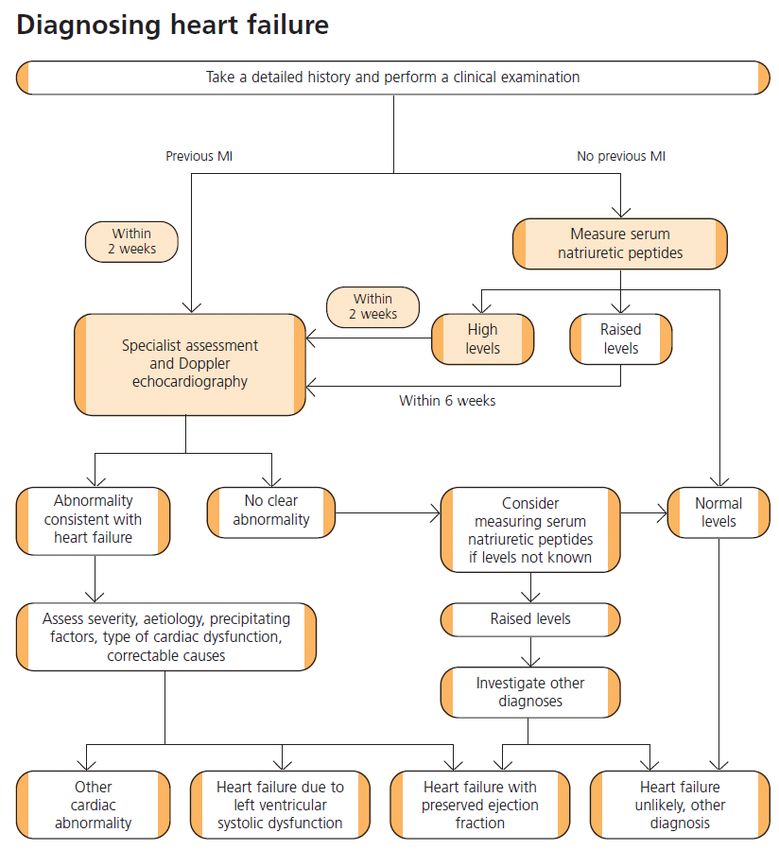
24th April 2012Nice guidelance, Aug 2010: The investigation of heart failure
Oct 2009: Audit of 35 echocardiogram
requests for ?heart failureIssues in starting a BNP service • No money • Silo budgeting • Uncontrolled demand • Limited understanding of value of BNP • New ways of working • Peer support
Commissioner expectations • No new money • Improved productivity • Patient-led, safe service • Protocol-driven care • Waiting list for echos < 6 weeks • Sustained services only if pilot is successful
Approach to service start-up
Timeline Milestone
Autumn/Winter 2010/11 GP awareness raising
2011 Pilot
April 2012 onwards Sustained commissioning?GP awareness • BNP for heart failure investigation only • Accessing the service • Sample collection/patient preparation • Onward referral pathways to echo • Commissioner expectations
Map of Medicine
Brain Natriuretic Peptide (BNP)
• 1988
• Identified from porcine
brain
• Later on isolated from
heart muscleBNP – how is it produced?
Fluid Ventricular
Overload stretch
Pro BNP
NT- proBNP BNPWhat does BNP do ?
Diuresis
Decreased
plasma
Vasodilatation volume and
BNP
BP
Natriuresis
Fluid overloadBNP – a screening test
If BNP levels is less than
100pg/ml i.e NEGATIVE
then it is high unlikely the
symptoms ( breath-
lessness) are due to
heart failureHow to request test and pathway • It is a blood test and sent to the RBH laboratory • Use a normal form or, preferably, Anglia ICE system • Because of instability of BNP, the sample should be processed by lab within 4 hours of taking the blood sample. • So if bloods are taken in house, make sure it is the last blood test of the morning or do blood test close to time of collection
Sample transport
• Take 2 red bottles and one brown
bottle. This will enable the BNP test to X2
be done as well as FBC, electrolytes, X1
LFTs and TFTs at the same time.
These are useful tests in the
preliminary assessment of someone
who is breathless or with heart failure
• Then put in the brown envelope with
yellow circle marked BNP test (so lab
can identify sample quickly )
• Results will come through the normal
path lab linkBNP< 100pg/ml NORMAL
Review patient and consider other diagnosis for
breathlessness with the help of history, examination and
the following tests if not already done:
1. CXR
2. Spirometry
3. Blood tests/ D- Dimer
4. ECG
Refer to Respiratory Medicine if neededBNP 100–400 pg/ml Raised
Refer to direct access cardiology
echocardiogram clinic
ROUTINE ( usually within 6 weeks )BNP> 400pg/ml HIGH
Refer to direct access cardiology
echocardiogram clinic
URGENT – should be seen within 2 weeks2011 pilot outcomes
January 2011 reject rates
BNP request patterns 2011
140
120
100
80
60
40
20
0
Jan Feb Mar Apr May June July AugDistribution of results
Jan- Oct 2011 referrals for echo
Number of No. referred for
abnormal BNP echocardiogram
results
BNP (100 – 400) 763 733
BNP (>400) 98 90BNP 100 – 400 pg/ml
400
350
BNP (pg/ml)
300
250
200
150
100
Negative Positive
Echo Echo
n= 131 n= 12BNP > 400 pg/ml
3000
2500
BNP (pg/ml)
2000
1500
1000
500
0
Negative Positive
Echo Echo
N=45 N = 13Productivity • Access to heart failure investigation:- – In 2010: 430 people by echocardiogram – In 2011: 1537 people by BNP/ echo • Cost effectiveness: – In 2010: Cost per patient £91 – In 2011: Cost per patient £52.33
Learning lessons • Learn from what others have done • Encourage ownership in the service – raise awareness, report audits/outcomes • Engage silos – commissioners, GPs, Lab, Cardiology, Transport drivers, Practice nurses, Phlebotomists • Engage peer support – GM&Cheshire cardiac network, pathology network
BNP - St Helens
A commissioning journey
2006 - 2010
Dr Shikha Pitalia, GP Chair United League Commissioning
GP of the year RCGP Mersey Faculty 2008The PBC Consortium
The ‘League’ formed in
2006
• 9 practices
• 20 GPs
• 42,000 patients
2010 – ULC
• Across 2 PCTs
• 25 practices
• 45 GPS
• 106,000 patientsUnscheduled Care - the size of the problem
• Halton and St Helens PCT had the
Halton and St Helens PCT – second highest
non elective admission rate second highest non-elective admission
rate within the SHA
• Service utilization review in North
Cheshire Hospital identified 43% of
patients admitted could have had their
admission avoided had appropriate
community based alternatives been
available.
• “Our Health, Our Care, Our Say”
suggests 50 per cent of patients taken to
A&E by ambulance could be cared for in
the community.The Journey begins… • 2006 ULC includes BNP testing in its business plan • Local Acute Trust had BNP kits but … • …PCT would not approve commissioning of test
ULC Record of Achievements Winner NHS – Health & Social Care Awards 2009 Winner GP Enterprise Award RCGP 2009 Winner NHS Alliance Acorn Award for PBC 2007 Highly Commended – NAPC Awards 2009 Highly Commended - HSJ Awards 2007
National Evidence and Guidance
NICE – 2003 Chronic Heart Failure
“Seek to exclude heart failure through:
• 12-lead ECG
• and/or natriuretic peptides (BNP or NTproBNP)”
NSF for Coronary Heart Disease – 2000
“…many people have heart failure that has not been recognised or
appropriately treated.”
“There is also evidence that some people who are treated do not have
heart failure.”Heart Failure – Facts
Primary Care
On average:
•A GP will look after 30 patients with heart failure per year
•Suspect a new diagnosis of heart failure in perhaps ten patients annually
•Heart failure often poorly diagnosed in COPD patients
•St Helens practice prevalence varies 0.38-2.19%
• Prevalence of heart failure increases significantly with age
Secondary Care
•Heart failure accounts for a total of 1 million inpatient bed days per year
•2% of all NHS inpatient bed-days
•5% of all emergency medical admissions to hospital
•Hospital admissions because of heart failure are projected to rise by 50%
over the next 25 yearsNational Facts : Heart failure • Around 900,000 people in the UK have heart failure • Almost as many have damaged hearts but, as yet, no symptoms of heart failure • Prevalence of heart failure is rising with an ageing population and improved survival of people with ischaemic heart disease • Heart failure has a poor prognosis: 30–40% of patients diagnosed with heart failure die within a year • Heart failure is a major cause for emergency admissions
Local Facts NW Highest mortality in England (St Helens 29% higher than national average) Ageing population High prevalence of smoking, alcohol and obesity Referrals for ECHO increasing Emergency admissions increasing Earlier diagnosis of heart failure a priority?
Negotiating with Local GPs
2007
4 consortia in Halton & St Helens PCT
ULC GPs supported use of BNP
1 group totally opposed
2 groups undecided
ULC agreed to explore a pilotNegotiating with Primary Care Trust
July 2008
Pilot approved for 12 months
ULC to commission directly from Acute TrustNegotiating with Acute Trusts
Cost - £23 per test
Path links
Direct access to ECHO
September 2008
ULC pilot goes live!Education, Education, Education September 2008 – March 2009 Clinical education sessions for each practice Monthly monitoring of uptake with reminders Quick reference guide Risks Non-referral 12 month window to demonstrate VfM
Borough-wide business case October 2009 Audit of ULC pilot presented as evidence: Evaluation clearly showed: Reduced need to refer to Cardiology outpatient More appropriate referrals for ECHO Earlier diagnosis and treatment of heart failure with reduced risk of emergency admission Better quality of life for patients Projected savings – Planned and unplanned care budgets Cost of rollout - £10,000 per year for 300,000 population (Reduced cost of £10 per BNP test) 4 complex elderly admissions avoided per year covers cost 2010 Boroughwide rollout – 4 years after initial ULC proposal!
NT-Pro BNP Wigan & St Helens Experience:
WIGAN WIGAN ST HELENS
BNP audit Wigan pop. 300k Oct 05-July 06 June 08 -Sept 08 Oct 08 – Sept 09
St Helens pilot 50k (10 months) (3 months) (12 months)
Total number of BNP tested 200 (10/month) 228 (76/month) 212 (18/month)
Total number of positive BNP 76 (38%) 110 (48%) 47 (22%)
Number of patients who did not 114 (62%) 118 (52%) 165 (78%)
require Echo
Cost of Direct Echo (£ 100/echo) £20,000 £ 28,800 £21,200
Cost of BNP (£ 15 / test) £3000 £ 3420 £4876 (@£23)
Cost of Echo for BNP + patients £7600 £11,000 £4700
Net saving £9400 £ 14,380 £11,624St Helens – Journey’s End BNP testing • Allows earlier diagnosis of heart failure • Allows earlier treatment of heart failure • Reduces hospital admissions • Reduces referrals to Cardiology clinics • Reduces unnecessary echo and has reduced echo waiting list
BNP vs PBR Tariff 2012/13
ECG Costs as Procedure and as Daycase 2012/13 Pbr Tariff Guidelines
Combined
day case /
Outpatient
ordinary
HRG code HRG name procedure
elective
tariff (£)
spell tariff
(£)
EA45Z Complex Echocardiogram (include Congenital, Transoesophageal and Fetal Echocardiography) 330 330
EA47Z Electrocardiogram Monitoring and stress testing 145 326
Outpatient Attendance costs 2012/13 Pbr Tariff Guidelines
WF01B WF02B
WF01A WF02A
First First
Follow Up Follow Up
Treatment Attendance Attendance
Treatment function name Attendance - Attendance -
function - Single - Multi
Single Multi
Profession Profession
Professional Professional
al al
172 Cardiac Surgery 293 293 171 171
300 General Medicine 210 251 105 121
430 Geriatric Medicine 303 303 139 139
812 Diagnostic Imaging 0 0 0 0
Direct access services
2012-13
tariff
Cost of
(including
HRG code HRG name reporting
the cost of
2012-13 (£)
reporting)
(£)
Simple Echocardiogram
RA60Z Simple Echocardiogram 57St Helens – Epilogue!
BNP is cost effective in the diagnosis and exclusion of
Heart Failure
BNP testing improves management of Heart Failure
and generates QIPP savings
Earlier diagnosis with BNP
improves quality of lifeYou can also read

















































