Burden, access, and disparities in kidney disease - World Kidney Day
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
editorial www.kidney-international.org
Burden, access, and disparities in
kidney disease
Kidney International (2019) 95, 242–248; https://doi.org/10.1016/j.kint.2018.11.007
KEYWORDS: acute kidney injury; end stage renal disease; global health; health equity; social determinants of health
ª World Kidney Day 2019 Steering Committee
idney disease is a global public health quite variable across settings. This situation is of
Deidra C. Crews , 1,2,3
K problem that affects more than 750
million persons worldwide.1 The burden
of kidney disease varies substantially across the
particular concern in low-income countries. For
example, a meta-analysis of 90 studies on CKD
burden conducted across Africa showed very few
Aminu K. Bello4 and world, as does its detection and treatment. studies (only 3%) with robust data.5 The provi-
Gamal Saadi5; for the Although the magnitude and impact of kidney sion of adequate resources and a workforce to
World Kidney Day Steering disease is better defined in developed countries, establish and maintain surveillance systems (e.g.,
Committee6 emerging evidence suggests that developing screening programs and registries) is essential
and requires substantial investment.6 Incorpo-
1
Division of Nephrology, countries have a similar or even greater kidney
Department of Medicine, Johns disease burden.2 rating kidney disease surveillance parameters in
Hopkins University School of
Medicine, Baltimore, Maryland,
In many settings, rates of kidney disease and existing chronic disease prevention programs
USA; 2Welch Center for the provision of its care are defined by socio- might enhance global efforts toward obtaining
Prevention, Epidemiology and economic, cultural, and political factors, lead- high-quality information on kidney disease
Clinical Research, Johns ing to significant disparities in disease burden, burden and attendant consequences.
Hopkins Medical Institutions, even in developed countries.3 These disparities
Baltimore, Maryland, USA;
In addition to a need for functional sur-
3
Johns Hopkins Center for
exist across the spectrum of kidney disease— veillance systems, the global importance of
Health Equity, Johns Hopkins from preventive efforts to curb development of kidney disease (including AKI and CKD) is yet
Medical Institutions, Baltimore, acute kidney injury (AKI) or chronic kidney to be widely acknowledged, making it a
Maryland, USA; 4Division of disease (CKD), to screening for kidney disease neglected disease on the global policy agenda.
Nephrology & Transplant among persons at high risk, to access to sub-
Immunology, Department of
For instance, the World Health Organization
Medicine, University of Alberta,
specialty care and treatment of kidney failure (WHO) Global Action Plan for the Prevention
Edmonton, Canada; and with renal replacement therapy (RRT). World and Control of Non-Communicable Diseases
5
Nephrology Unit, Department Kidney Day 2019 offers an opportunity to raise (NCDs) (2013) focuses on cardiovascular dis-
of Internal Medicine, Faculty of awareness of kidney disease and highlight dis- eases, cancer, chronic respiratory diseases, and
Medicine, Cairo University, Giza, parities in its burden and current state of global
Egypt
diabetes but not kidney disease, despite advo-
capacity for prevention and management. In cacy efforts by relevant stakeholders such as the
Correspondence: Deidra C.
this editorial, we highlight these disparities and International Society of Nephrology and the
Crews, Johns Hopkins University
School of Medicine, 301 Mason emphasize the role of public policies and International Federation of Kidney Founda-
F. Lord Drive, Suite 2500, organizational structures in addressing them. tions through activities such as World Kidney
Baltimore, Maryland 21224, We outline opportunities to improve our un- Day. This situation is quite concerning because
USA. E-mail: dcrews1@jhmi.edu derstanding of disparities in kidney disease, the estimates from the Global Burden of Disease
This article is being published best ways for them to be addressed, and how to study in 2015 showed that around 1.2 million
in Kidney International and streamline efforts toward achieving kidney people were known to have died of CKD,7 and
reprinted concurrently in
health equity across the globe. more than 2 million people died in 2010
several journals. The articles
cover identical concepts and because they had no access to dialysis. It is
Burden of kidney disease
wording, but vary in minor estimated that another 1.7 million die from
Availability of data reflecting the full burden of
stylistic and spelling changes, AKI on an annual basis.8,9 It is possible,
detail, and length of manu- kidney disease varies substantially because of
therefore, that kidney disease may contribute to
script in keeping with each limited or inconsistent data collection and sur-
more deaths than the 4 main NCDs targeted by
journal’s style. Any of these veillance practices worldwide (Table 1).4
versions may be used in citing the current NCD Action Plan.
Whereas several countries have national data
this article.
collection systems, particularly for end-stage Risk factors for kidney disease. Data in
Note that all authors contrib- recent decades have linked a host of genetic,
renal disease (ESRD) (e.g., United States Renal
uted equally to the concep-
tion, preparation, and editing Data System, Latin American Dialysis and Renal environmental, sociodemographic, and clinical
of the manuscript. Transplant Registry, and Australia and New factors to risk of kidney disease. The popula-
6
See Appendix for list of
Zealand Dialysis and Transplant Registry), high- tion burden of kidney disease is known to
members of the World Kidney quality data regarding nondialysis CKD is correlate with socially defined factors in most
Day Steering Committee. limited, and often the quality of ESRD data is societies across the world. This phenomenon is
242 Kidney International (2019) 95, 242–248
editorial
Table 1 | World Bank country group chronic kidney disease gaps
Low-income Lower-middle-income Upper middle-income High-income
CKD care countries (%) countries (%) countries (%) countries (%)
Governmental recognition of 59 50 17 29
CKD as a health priority
Government funds all aspects of 13 21 40 53
CKD care
Availability of CKD management 46 73 83 97
and referral guidelines
(international, national, or
regional)
Existence of current CKD 6 24 24 32
detection programs
Availability of dialysis registries 24 48 72 89
Availability of academic centers 12 34 62 63
for renal clinical trial
management
CKD, chronic kidney disease.
Data from Bello et al.4
better documented in high-income countries, are limited. Hypertension is also estimated to
where racial/ethnic minority groups and people affect 1 billion persons worldwide20 and is the
of low socioeconomic status carry a high burden second leading attributed cause of CKD.18
of disease. Extensive data have demonstrated that Hypertension control is important for slowing
racial and ethnic minorities (e.g., African CKD progression and decreasing mortality risk
Americans in the United States, Aboriginal among persons with or without CKD. Hyper-
groups in Canada and Australia, Indo-Asians in tension is present in more than 90% of persons
the United Kingdom, and others) are affected with advanced kidney disease,18 yet racial/
disproportionately by advanced and progressive ethnic minorities and low-income persons with
kidney disease.10–12 The associations of socio- CKD who live in high-income countries have
economic status and risk of progressive CKD and poorer blood pressure control than their more
eventual kidney failure also have been well socially advantaged counterparts.21
described, with persons of lower socioeconomic Lifestyle behaviors, including dietary pat-
status bearing the greatest burden.13,14 terns, are strongly influenced by socioeconomic
Recent works have associated apolipopro- status. In recent years, several healthful dietary
tein L1 risk variants15,16 with increased kidney patterns have been associated with favorable
disease burden among persons with African CKD outcomes.22 Low-income persons often
ancestry. In Central America and South- face barriers to healthful eating that may in-
eastern Mexico, Mesoamerican nephropathy crease their risk of kidney disease.23–25 People
(also referred to as CKD of unknown causes) of low socioeconomic status often experience
has emerged as an important cause of kidney food insecurity (i.e., limited access to affordable
disease. While multiple exposures have been nutritious foods), which is a risk factor for
studied for their potential role in CKD of CKD26 and progression to kidney failure.27 In
unknown causes, recurrent dehydration and low-income countries, food insecurity may lead
heat stress are common denominators in most to undernutrition and starvation, which has
cases.17 Other perhaps more readily modifi- implications for the individual and, in the case
able risk factors for kidney disease and CKD of women of child-bearing age, could lead to
progression that disproportionately affect so- their children having low birth weight and
cially disadvantaged groups also have been related sequelae, including CKD.28 Rates of
identified, including disparate rates and poor undernourishment are as high as 35% or more
control of clinical risk factors such as diabetes in countries such as Haiti, Namibia, and
and hypertension, as well as lifestyle Zambia.29 However, in high-income countries,
behaviors. food insecurity is associated with overnutrition,
Diabetes is the leading cause of advanced and persons with food insecurity have
kidney disease worldwide.18 In 2016, 1 in 11 increased risk of overweight and obesity.30,31
adults worldwide had diabetes and more than Further, food insecurity has been associated
80% were living in low- and middle-income with several diet-related conditions, including
countries19 where resources for optimal care diabetes and hypertension.
Kidney International (2019) 95, 242–248 243editorial
Acute kidney injury. AKI is an underdetected that patients and families were burdened with
condition that is estimated to occur in 8% to 16% having to navigate multiple health and social
of hospital admissions32 and is now well estab- care structures, negotiate treatments and costs,
lished as a risk factor for CKD.33 Disparities in finance their health care, and manage health
AKI risk are also common, following a pattern information.40 Challenges may be even greater
similar to that observed in persons with CKD.34 for families of children with ESRD, because
AKI related to nephrotoxins, alternative (tradi- many regions lack qualified pediatric care
tional) medicines, infectious agents, and hospi- centers.
talizations and related procedures are more
pronounced in low-income and lower-middle- Organization and structures for kidney disease
income countries and contribute to increased care
risk of mortality and CKD in those settings.35 The lack of recognition and therefore the
Importantly, the majority of annual AKI cases absence of a global action plan for kidney dis-
worldwide (85% of more than 13 million cases) ease partly explains the substantial variation in
are experienced in low-income and lower-middle- structures and capacity for kidney care around
income countries, leading to 1.4 million deaths.36 the globe. This situation has resulted in varia-
tions in government priorities, health care
Health policies and financing of kidney disease budgets, care structures, and human resource
care availability.41 Effective and sustainable advo-
Because of the complex and costly nature of cacy efforts are needed at global, regional, and
kidney disease care, its provision is tightly linked national levels to get kidney disease recognized
with the public policies and financial status of and placed on the global policy agenda.
individual countries. For example, gross domes- In 2017, the International Society of
tic product is correlated with lower dialysis-to- Nephrology collected data on country-level ca-
transplantation ratios, suggesting greater rates pacity for kidney care delivery using a survey, the
of kidney transplantation in more financially Global Kidney Health Atlas,4 which aligned with
solvent nations. In several high-income coun- the WHO’s building blocks of a health system.
tries, universal health care is provided by the The Global Kidney Health Atlas highlights limited
government and includes CKD and ESRD care. awareness of kidney disease and its consequences
In other countries, such as the United States, and persistent inequities in resources required to
ESRD care is publicly financed for citizens; tackle the burden of kidney disease across the
however, optimal treatment of CKD and its risk globe. For example, CKD was recognized as a
factors may not be accessible for persons lacking health care priority by government in only 36% of
health insurance, and regular care of undocu- countries that participated in this survey. The
mented immigrants with kidney disease is not priority was inversely related to income level:
covered.37 In low-income and lower-middle- CKD was a health care priority in more than half
income countries, neither CKD nor ESRD care of low-income and lower-middle-income coun-
may be publicly financed, and CKD prevention tries but in less than 30% of upper-middle-
efforts are often limited. In several such coun- income and high-income countries.
tries, collaborations between public and private Regarding capacity and resources for kidney
sectors have emerged to provide funding for RRT. care, many countries still lack access to basic di-
For example, in Karachi, Pakistan, a program of agnostics, a trained nephrology workforce, uni-
dialysis and kidney transplantation through joint versal access to primary health care, and RRT
community and government funding has existed technologies. Low-income and lower-middle-
for more than 25 years.38 income countries, especially in Africa, had
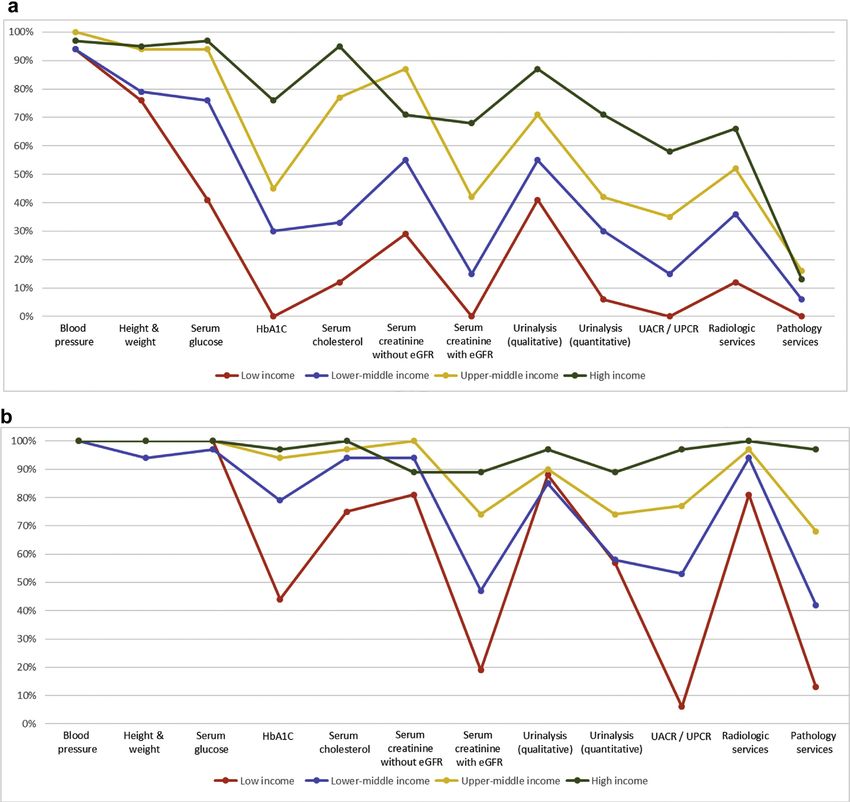
In many settings, persons with advanced limited services for the diagnosis, management,
CKD who have no or limited public or private and monitoring of CKD at the primary care level,
sector funding for care shoulder a substantial with only 12% having serum creatinine mea-
financial burden. A systematic review of 260 surement, including estimated glomerular filtra-
studies including patients from 30 countries tion rate. Twenty-nine percent of low-income
identified significant challenges, including countries had access to qualitative urinalysis using
fragmented care of indeterminate duration, urine test strips; however, no low-income country
reliance on emergency care, and fear of cata- had access to urine albumin-to-creatinine ratio or
strophic life events because of diminished urine protein-to-creatinine ratio measurements at
financial capacity to withstand them.39 Authors the primary care level. Across all world countries,
of another study conducted in Mexico found availability of services at the secondary/tertiary
244 Kidney International (2019) 95, 242–248editorial
care level was considerably higher than at the low-income regions. For instance, more than
primary care level (Figure 1a and b).4,42 90% of upper-middle-income and high-
Renal replacement therapies. The distribu- income countries reported having chronic
tion of RRT technologies varied widely. On the peritoneal dialysis services, whereas these ser-
surface, all countries reported having long-term vices were available in 64% and 35% of low-
hemodialysis services, and more than 90% of income and lower-middle-income countries,
countries reported having short-term hemodi- respectively. In comparison, acute peritoneal
alysis services. However, access to and distri- dialysis had the lowest availability across all
bution of RRT across countries and regions was countries. More than 90% of upper-middle-
highly inequitable, often requiring prohibitive income and high-income countries reported
out-of-pocket expenditure, particularly in having kidney transplant services, with more
Figure 1 | Health care services for identification and management of chronic kidney disease by country income level. (a) Primary care (i.e.,
basic health facilities at community levels [e.g., clinics, dispensaries, and small local hospitals]). (b) Secondary/specialty care (i.e., health facilities
at a level higher than primary care [e.g., clinics, hospitals, and academic centers]). eGFR, estimated glomerular filtration rate; HbA1C, glycated
hemoglobin; UACR, urine albumin-to-creatinine ratio; UPCR, urine protein-to-creatinine ratio. Data from Bello et al.4 and Htay et al.42
Kidney International (2019) 95, 242–248 245editorial
than 85% of these countries reporting both The appropriate number of nephrologists in
living and deceased donors as the organ source. a country depends on many factors, including
As expected, low-income countries had the need, priority, and resources, and as such there
lowest availability of kidney transplant services, is no global standard with respect to nephrol-
with only 12% reporting availability, and live ogist density. Regardless, the demonstrated low
donors as the only source. density in low-income countries calls for
Workforce for kidney care. Considerable concern as nephrologists are essential to pro-
international variation was also noted in the vide leadership in kidney disease care, and a
distribution of the kidney care workforce, lack of nephrologists may result in adverse
particularly nephrologists. The lowest density consequences for policy and practice. However,
(15 nephrologists low-income and lower-middle-income coun-
per million population) was reported mainly in tries, in part thanks to fellowship programs
high-income countries (Figure 2).4,43,44 Most supported by international nephrology organi-
countries reported nephrologists as primarily zations.45 It is important to note that the role of
responsible for both CKD and AKI care. Pri- a nephrologist may differ depending on how
mary care physicians had more responsibility the health care system is structured. The den-
for CKD care than for AKI care, as 64% of sity statistic merely represents the number of
countries reported that primary care physicians nephrologists per million population and pro-
are primarily responsible for CKD care and vides no indication of the adequacy to meet the
35% reported that they are responsible for AKI needs of the population or quality of care,
care. Intensive care specialists were primarily which depends on volume of patients with
responsible for AKI in 75% of countries, likely kidney disease and other workforce support
because AKI is typically treated in hospitals. (e.g., availability of multidisciplinary teams).
However, only 45% of low-income countries For other care providers essential for kidney
reported that intensive care specialists were care, international variations exist in distribution
primarily responsible for AKI, compared with (availability and adequacy). Overall, provider
90% of high-income countries; this discrepancy shortages were highest for renal pathologists,
may be due to a general shortage of intensive vascular access coordinators, and dietitians (with
care specialists in low-income countries. 86%, 81%, and 78% of countries reporting a
Figure 2 | Nephrologist availability (density per million population) compared with physician, nursing, and
pharmaceutical personnel availability by country income level. Pharmaceutical personnel include pharmacists,
pharmaceutical assistants, and pharmaceutical technicians. Nursing and midwifery personnel include
professional nurses, professional midwives, auxiliary nurses, auxiliary midwives, enrolled nurses, enrolled
midwives, and related occupations such as dental nurses. A logarithmic scale was used for the x-axis [log(xþ1)]
because of the large range in provider density. Data from Bello et al.,4 Osman et al.,43 and the World Health
Organization (for pharmaceutical personnel: http://apps.who.int/gho/data/view.main.PHARMS and http://apps.
who.int/gho/data/node.main-amro.HWF?lang¼en, for nursing and midwifery personnel: http://apps.who.int/
gho/data/view.main.NURSES, for physicians: http://apps.who.int/gho/data/view.main.92000).44
246 Kidney International (2019) 95, 242–248editorial
shortage, respectively), and the shortages were worldwide. The provision and delivery of kid-
more common in low-income countries. Few ney care varies widely across the world.
countries (35%) reported a shortage in laboratory Achieving universal health coverage worldwide
technicians. This information highlights signifi- by 2030 is one of the WHO Sustainable
cant inter- and intra-regional variability in the Development Goals. Although universal health
current capacity for kidney care across the world. coverage may not include all elements of kidney
Important gaps in awareness, services, workforce, care in all countries (because this is usually a
and capacity for optimal care delivery were iden- function of political, economic, and cultural
tified in many countries and regions.4 The find- factors), understanding what is feasible and
ings have implications for policy development important for a country or region with a focus
with regard to establishment of robust kidney care on reducing the burden and consequences of
programs, particularly for low-income and lower- kidney disease would be an important step
middle-income countries.46 The Global Kidney toward achieving kidney health equity.
Health Atlas has therefore provided a baseline
understanding of where countries and regions
APPENDIX
stand with respect to several domains of the health Members of the World Kidney Day Steering Committee are Philip
system, thus allowing the monitoring of progress Kam Tao Li, Guillermo Garcia-Garcia, Sharon Andreoli, Deidra
through the implementation of various strategies Crews, Kamyar Kalantar-Zadeh, Charles Kernahan, Latha Kumar-
aswami, Gamal Saadi, and Luisa Strani.
aimed at achieving equitable and quality care for
the many patients with kidney disease across the DISCLOSURE
globe. All the authors declared no competing interests.
How could this information be used to miti-
ACKNOWLEDGMENTS
gate existing barriers to kidney care? First, basic The authors thank the Global Kidney Health Atlas
infrastructure for services must be strengthened Team, M. Lunney, and M.A. Osman.
at the primary care level for early detection and
management of AKI and CKD across all coun- REFERENCES
tries.46 Second, although optimal kidney care 1. GBD 2015 DALYs and HALE Collaborators. Global,
regional, and national disability-adjusted life-years
obviously should emphasize prevention to reduce (DALYs) for 315 diseases and injuries and healthy life
adverse consequences of kidney disease at the expectancy (HALE), 1990-2015: a systematic analysis
population level, countries (particularly low- for the Global Burden of Disease Study 2015. Lancet.
2016;388:1603–1658.
income and lower-middle-income countries) 2. Hill NR, Fatoba ST, Oke JL, et al. Global prevalence of
should be supported at the same time to adopt chronic kidney disease–a systematic review and meta-
more pragmatic approaches in providing RRT. analysis. PLoS One. 2016;11:e0158765.
3. Crews DC, Liu Y, Boulware LE. Disparities in the
For example, acute peritoneal dialysis could be an burden, outcomes, and care of chronic kidney disease.
attractive modality for AKI, because this type of Curr Opin Nephrol Hypertens. 2014;23:298–305.
dialysis is as effective as hemodialysis, requires far 4. Bello AK, Levin A, Tonelli M, et al. Global Kidney Health
Atlas: a report by the International Society of
less infrastructure, and can be performed with Nephrology on the current state of organization and
solutions and catheters adapted to local re- structures for kidney care across the globe. https://
sources.47 Third, kidney transplantation should www.theisn.org/images/ISN_advocacy/GKHAtlas_
Linked_Compressed1.pdf. Published 2017. Accessed
be encouraged through increased awareness August 22, 2018.
among the public and political leaders across 5. Stanifer JW, Jing B, Tolan S, et al. The epidemiology of
countries, because this is the clinically optimal chronic kidney disease in sub-Saharan Africa: a
systematic review and meta-analysis. Lancet Glob
modality of RRT and it is also cost-effective, Health. 2014;2:e174–e181.
provided that costs of the surgery and long- 6. Davids MR, Eastwood JB, Selwood NH, et al. A renal
term medication and follow-up are made registry for Africa: first steps. Clin Kidney J. 2016;9:
162–167.
sustainable through public (and/or private) 7. GBD 2015 Mortality and Causes of Death
funding.48 Currently, most kidney transplants are Collaborators. Global, regional, and national life
conducted in high-income countries in part expectancy, all-cause mortality, and cause-specific
mortality for 249 causes of death, 1980-2015: a
because of lack of resources and knowledge in systematic analysis for the Global Burden of Disease
low-income and lower-middle-income countries, Study 2015. Lancet. 2016;388:1459–1544.
as well as cultural practices and absence of legal 8. Liyanage T, Ninomiya T, Jha V, et al.
Worldwide access to treatment for end-stage kidney
frameworks governing organ donation.48 disease: a systematic review. Lancet. 2015;385:
1975–1982.
CONCLUSION 9. Mehta RL, Cerda J, Burdmann EA, et al. International
Society of Nephrology’s 0by25 initiative for acute kidney
Socially disadvantaged persons experience a injury (zero preventable deaths by 2025): a human rights
disproportionate burden of kidney disease case for nephrology. Lancet. 2015;385:2616–2643.
Kidney International (2019) 95, 242–248 247editorial
10. Samuel SM, Palacios-Derflingher L, Tonelli M, et al. 29. Food and Agriculture Organization of the
Association between First Nations ethnicity and United Nations. The FAO hunger map 2015. http://
progression to kidney failure by presence and severity www.fao.org/3/a-i4674e.pdf. Published 2015. Accessed
of albuminuria. CMAJ. 2014;186:E86–E94. August 22, 2018.
11. Nicholas SB, Kalantar-Zadeh K, Norris KC. Racial 30. Shariff ZM, Khor GL. Obesity and household food
disparities in kidney disease outcomes. Semin Nephrol. insecurity: evidence from a sample of rural households
2013;33:409–415. in Malaysia. Eur J Clin Nutr. 2005;59:1049–1058.
12. Van den Beukel TO, de Goeij MC, Dekker FW, et al. 31. Popkin BM. Contemporary nutritional transition:
Differences in progression to ESRD between black and determinants of diet and its impact on body
white patients receiving predialysis care in a universal composition. Proc Nutr Soc. 2011;70:82–91.
health care system. Clin J Am Soc Nephrol. 2013;8: 32. Sawhney S, Marks A, Fluck N, et al. Intermediate and
1540–1547. long-term outcomes of survivors of acute kidney
13. Crews DC, Gutierrez OM, Fedewa SA, et al. Low injury episodes: a large population-based cohort
income, community poverty and risk of end stage study. Am J Kidney Dis. 2017;69:18–28.
renal disease. BMC Nephrol. 2014;15:192. 33. Heung M, Steffick DE, Zivin K, et al. Acute kidney injury
14. Garrity BH, Kramer H, Vellanki K, et al. Time trends in recovery pattern and subsequent risk of CKD: an
the association of ESRD incidence with area-level analysis of Veterans Health Administration data. Am J
poverty in the US population. Hemodial Int. 2016;20: Kidney Dis. 2016;67:742–752.
78–83. 34. Grams ME, Matsushita K, Sang Y, et al. Explaining the
15. Parsa A, Kao WH, Xie D, et al. APOL1 risk variants, race, racial difference in AKI incidence. J Am Soc Nephrol.
and progression of chronic kidney disease. N Engl J 2014;25:1834–1841.
Med. 2013;369:2183–2196. 35. Luyckx VA, Tuttle KR, Garcia-Garcia G, et al. Reducing
16. Peralta CA, Bibbins-Domingo K, Vittinghoff E, et al. major risk factors for chronic kidney disease. Kidney Int
APOL1 genotype and race differences in incident Suppl. 2017;7:71–87.
albuminuria and renal function decline. J Am Soc 36. Lewington AJ, Cerda J, Mehta RL. Raising awareness of
Nephrol. 2016;27:887–893. acute kidney injury: a global perspective of a silent
17. Correa-Rotter R. Mesoamerican nephropathy or killer. Kidney Int. 2013;84:457–467.
chronic kidney disease of unknown origin. In: García- 37. Cervantes L, Tuot D, Raghavan R, et al. Association of
García G, Agodoa LY, Norris KC, eds. Chronic Kidney emergency-only vs standard hemodialysis with
Disease in Disadvantaged Populations. Cambridge, MA: mortality and health care use among undocumented
Academic Press; 2017:221–228. immigrants with end-stage renal disease. JAMA Intern
18. Levin A, Stevens PE, Bilous RW, et al. Kidney Med. 2018;178:188–195.
Disease: Improving Global Outcomes (KDIGO) CKD 38. Rizvi SA, Naqvi SA, Zafar MN, Akhtar SF. A kidney
Work Group. KDIGO 2012 clinical practice transplantation model in a low-resource country: an
guideline for the evaluation and management experience from Pakistan. Kidney Int Suppl. 2013;3:236–240.
of chronic kidney disease. Kidney Int Suppl. 39. Roberti J, Cummings A, Myall M, et al. Work of being
2013;3:1–150. an adult patient with chronic kidney disease: a
19. Chan JC, Gregg EW, Sargent J, Horton R. Reducing systematic review of qualitative studies. BMJ Open.
global diabetes burden by implementing solutions 2018;8:e023507.
and identifying gaps: a Lancet Commission. Lancet. 40. Kierans C, Padilla-Altamira C, Garcia-Garcia G, et al.
2016;387:1494–1495. When health systems are barriers to health care:
20. Kearney PM, Whelton M, Reynolds K, et al. Global challenges faced by uninsured Mexican kidney
burden of hypertension: analysis of worldwide data. patients. PLoS One. 2013;8:e54380.
Lancet. 2005;365:217–223. 41. Murray CJ, Frenk J. A framework for assessing the
21. Plantinga LC, Miller ER 3rd, Stevens LA, et al. Blood performance of health systems. Bull World Health
pressure control among persons without and with Organ. 2000;78:717–731.
chronic kidney disease: US trends and risk factors 42. Htay H, Alrukhaimi M, Ashuntantang GE, et al. Global
1999-2006. Hypertension. 2009;54:47–56. access of patients with kidney disease to health
22. Banerjee T, Liu Y, Crews DC. Dietary patterns and CKD technologies and medications: findings from the
progression. Blood Purif. 2016;41:117–122. Global Kidney Health Atlas project. Kidney Int Suppl.
23. Johnson AE, Boulware LE, Anderson CA, et al. 2018;8:64–73.
Perceived barriers and facilitators of using dietary 43. Osman MA, Alrukhaimi M, Ashuntantang GE, et al.
modification for CKD prevention among African Global nephrology workforce: gaps and opportunities
Americans of low socioeconomic status: a qualitative toward a sustainable kidney care system. Kidney Int
study. BMC Nephrol. 2014;15:194. Suppl. 2018;8:52–63.
24. Crews DC, Kuczmarski MF, Miller ER 3rd, et al. 44. World Health Organization. Global Health Observatory
Dietary habits, poverty, and chronic kidney indicator views. http://apps.who.int/gho/data/node.
disease in an urban population. J Ren Nutr. imr#ndx-P. Accessed August 22, 2018.
2015;25:103–110. 45. Harris DC, Dupuis S, Couser WG, Feehally J. Training
25. Suarez JJ, Isakova T, Anderson CA, et al. Food access, nephrologists from developing countries: does it have
chronic kidney disease, and hypertension in the U.S. a positive impact? Kidney Int Suppl. 2012;2:275–278.
Am J Prev Med. 2015;49:912–920. 46. Couser WG, Remuzzi G, Mendis S, Tonelli M. The
26. Crews DC, Kuczmarski MF, Grubbs V, et al. Effect contribution of chronic kidney disease to the global
of food insecurity on chronic kidney disease in burden of major noncommunicable diseases. Kidney
lower-income Americans. Am J Nephrol. 2014;39: Int. 2011;80:1258–1270.
27–35. 47. Chionh CY, Soni SS, Finkelstein FO, et al. Use of
27. Banerjee T, Crews DC, Wesson DE, et al. Food peritoneal dialysis in AKI: a systematic review. Clin J
insecurity, CKD, and subsequent ESRD in US adults. Am Soc Nephrol. 2013;8:1649–1660.
Am J Kidney Dis. 2017;70:38–47. 48. Muralidharan A, White S. The need for kidney
28. Piccoli GB, Alrukhaimi M, Liu ZH, et al. Women and transplantation in low- and middle-income countries
kidney disease: reflections on World Kidney Day 2018. in 2012: an epidemiological perspective.
Kidney Int. 2018;93:278–283. Transplantation. 2015;99:476–478.
248 Kidney International (2019) 95, 242–248You can also read

















































