Cancer du sein du Sujet Agé Traitements Systémiques - Dr Etienne Brain Institut Curie Saint-Cloud, France
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Cancer du sein du Sujet Agé
Traitements Systémiques
Dr Etienne Brain
Institut Curie
Saint-Cloud, France
www.siog.org
etienne.brain@curie.fr
1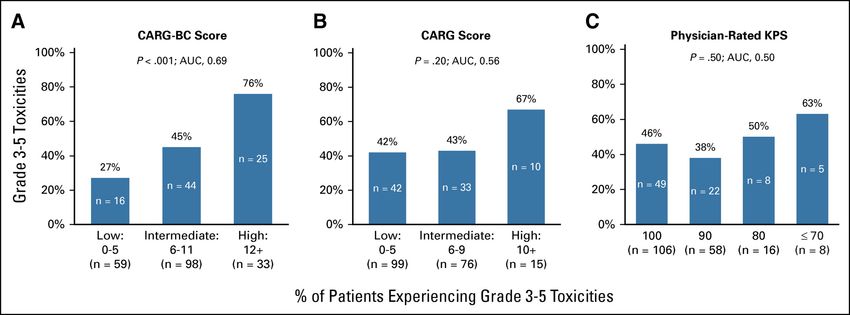
• Most common shortcut in statistics
“1 in 8 women will develop BC in their lifetime”
instead of
“If everyone lived beyond the age of 70, 1 in 8 of those women
would get or have had BC”
• Since BC risk increases w/ age, lifetime risk changes depending on age
– Age 20-29 1 in 2,000
– Age 30-39 1 in 229
– Age 40-49 1 in 68
– Age 50-59 1 in 37
– Age 60-69 1 in 26
– Ever 1 in 8
2
Worldwidebreastcancer.com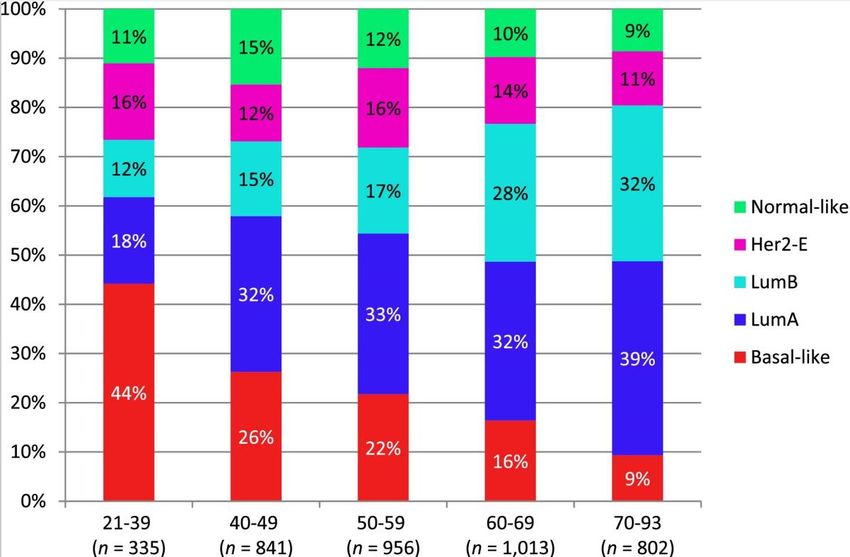
Few older adults included in registration studies!
Breast cancer as an example
Agent Name Approval N Age ≥ 65 N Age ≥ 75
37 44% 8 10%
Palbociclib 2/2015
86 25% --
Everolimus 7/2012 290 40% 109 15%
Pertuzumab 6/2012 60 15% 5 1%
Eribulin mesylate 11/2010 121 15% 17 2%
34 17% 2 1%
Lapatinib 1/2010
282 44% 77 12%
45 10% 3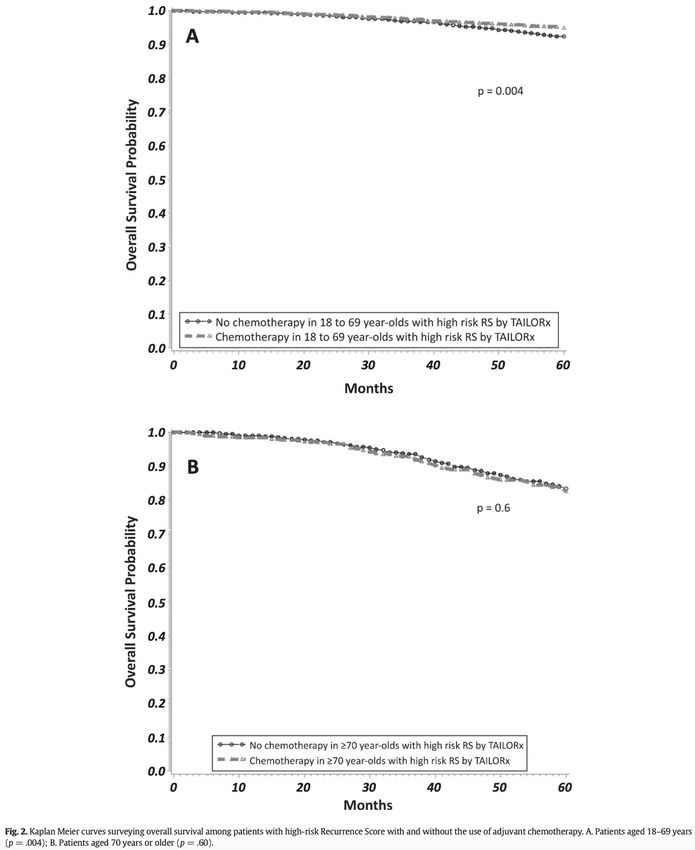
Competing Causes for Mortality
4
Kendal Cancer 2008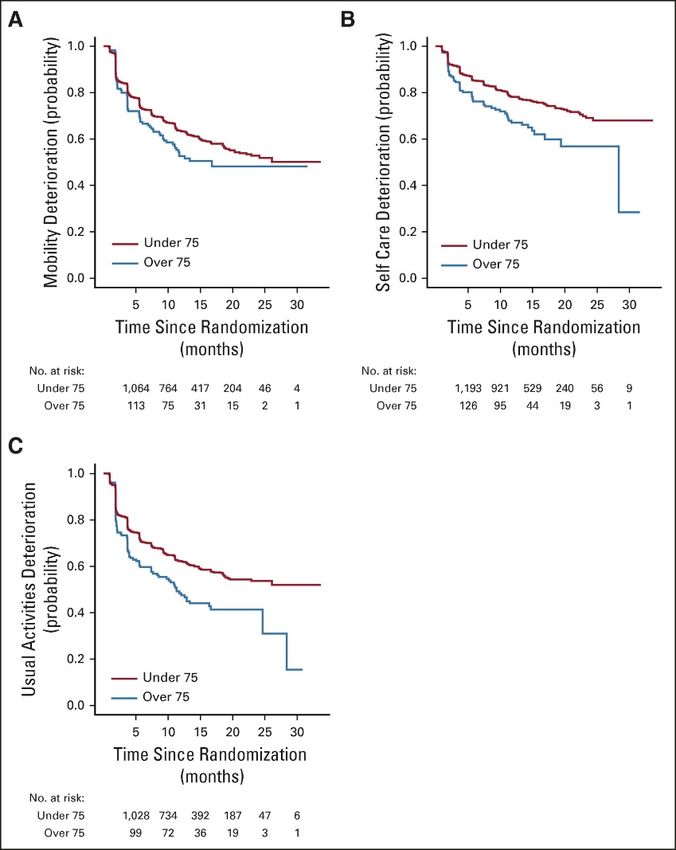
Competing risks for mortality
Dutch & Belgian postmenopausal pts w/ EBC ER+ in the TEAM trial (2001-2006)
exemestane vs sequential tamoxifen à exemestane 5 yr
3,159 pts (70%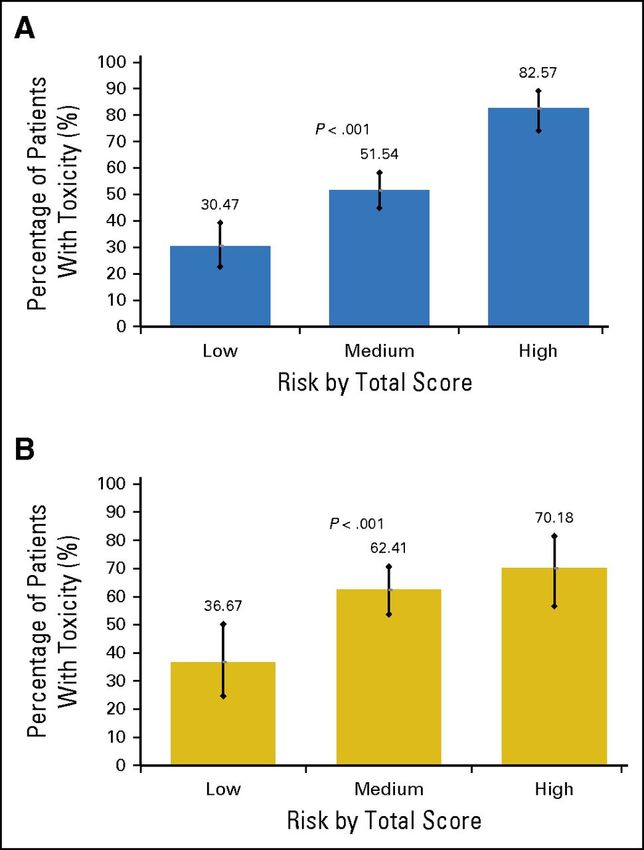
Competing risks for mortality
≥70 yr & no comorbidity (33%)
à higher BC mortality
22.2%, 95% CI, 17.5–26.9 vs 15.6%, 95% CI, 13.6–17.7
sHR 1.49, 95% CI, 1.12–1.97, p = .005
6
Derks The Oncologist 2019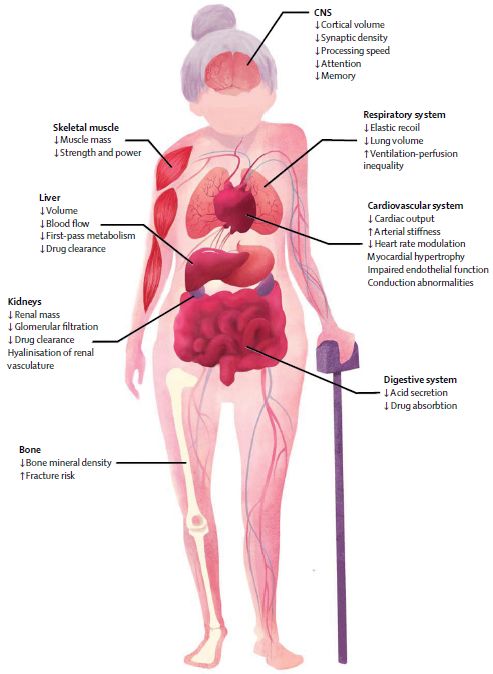
Phénotype
Plus de formes hormonosensibles (RH+)
Moins de formes agressives (triple négatif, HER2+++)
BC biology according to age
de Kruijf Mol Oncol 2014, Jenskins Oncologist 2014
Le cancer du sein de la femme âgée se
prête volontiers à l’hormonothérapie
car il est plus souvent RH+
Mais entre anti-aromatase (letrozole/FEMARA, anastrozole/ARIMIDEX,
exemestane/AROMASINE et anti-oestrogène (tamoxifène),
la question de l’observance est majeure (et donc l’ajustement à la tolérance)
En contexte adjuvant/précoce, l’hormonothérapie se donne 5 ans en général
(discussion sur les extensions au delà)
• TAM / 0
Réduction du Bénéfice absolu à 10
60 %
risque de rechute ans
50 %
RO+ 41 % 13,6 % 45,0 contrôle
38,3
rechute
40 %
33,2 TAM 5A
30 % 26,5
• IA / TAM 24,7 AI 5A
20 %
Réduction du Bénéfice absolu à 10 15,1
risque de rechute ans
10 %
RO+
20 % 5%
Post- MP 5 10 15Question centrale
Cancer du sein controlatéral Cancer du sein controlatéral
Ostéoporose
Myalgies
Troubles lipidiques
?
Cognition
Thromboses veineuses
Cancer de l’endomètre
Bouffées de chaleur
Sexualité
Troubles lipidiques
Tamoxifène Cœur et vaisseaux Anti-aromatases
Bouffées de chaleur
Arthralgies & myalgies
Thromboses veineuses
Ostéoporose
Cancer de l’endomètre
Troubles génito-urinairesEndocrine therapy combinations
• With everolimus (BOLERO)
• With CDK4-6 inhibitors (PALOMA)
• Potential similar efficacy
• But safety profiles are different since trials
populations are highly selected
12Phase III 2:1 > NSAI
PFS +4.1-6.5 mths (x 2)
But! AEs
Fatigue, stomatitis, rash, anorexia, diarrhea
Hyperglycemia, non-infectious pneumonitis
à 20% dose adjustment
13
Baselga N Engl J Med 2012724 patients à 265 (40%) 65+ à 164 (23%) 70+
70+ vs• European phase IIIb • Expanded-access multicenter trial • 2133 patients, 26% 70+ • Key AEs: stomatitis, fatigue, anemia, NIP
16
1. CDK4/6 inhibitor + AI as 1st line treatment of HR+
MBC in older women à similar efficacy benefit as
seen in younger women
2. Incidence and severity of Grade 1-4 AEs similar
between age groups, but greater SAEs and
discontinuations occurred in patients ≥75 (89%
vs 73%)
3. EQ-D5 à decline in HRQoL regardless of treatment
4. Need for inclusion of greater numbers of patients ≥70
in clinical trials
17
Howie JCO 2019La chimiothérapie, c’est plus
compliqué…
Car index thérapeutique plus étroit que l’hormonothérapie
Des doses généralement ajustées (inférieures)Physiological variations x PK & PD
Mechanism Consequences
Absorption of proteins,
Absorption Gastric dumping and secretions î
vitamins and drugs î
Hepatocytes, blood flow, CYP Protein synthesis, (de-)
Metabolism P450 activity î activation of drugs and
Interactions (CYP P450) carcinogens î
Vd hydrosolubles drugs î
Distribution H2O, albumin, Hb î
Vd liposolubles drugs ì
Renal elimination of drugs
GFR, tubular filtration î
Excretion excreted by kidney î
Biliary excretion è 19
Biliary
Balducci Oncologist 2000; elimination
Wildiers è
Clin Pharmacokinet 2003; http://www.ema.europa.euLes grands médicaments
• Anthracyclines (adriamycine, épirubicine, schémas FEC 100 ou AC)
– Myélotoxicité
– Cardiotoxicité
• Alkylants (cyclophosphamide/Endoxan®, schéma FEC 100 ou AC)
– Myélotoxicité
– Attention à la fonction rénale
• Taxanes (docetaxel/Taxotère®, paclitaxel/Taxol®)
– Myélotoxicité
– Neuropathie
– Onycholyse
– Rétention hydrique
• Antimétabolites (5-flurorouracile, forme orale = capecitabine/Xeloda®)
– Syndrome mains pieds
– Diarrhée
20Benefit/risk balance of chemotherapy is narrower
than other treatments, especially in older patients
• Myelosuppression: greater in older patients
– Lower threshold (But also other issues difficult to capture!
1. Past medical history
Survivors! With long-term toxicity of previous cancer treatments
• Cognitive impairment, cardiotoxicity, depression and anxiety, neurotoxicity, ototoxicity, imbalance & lack of
coordination, osteoporosis, metabolic syndrome, second malignancy, sexual and vaginal dysfunction
2. Problems and complications due to comedication/polypharmacy
29% take > 7 drugs, NSAID/MTX, pain medications & cachexia (falls, fractures)
3. Social and psychological aspects
Fear for pain and dependance, frailty and end of life aspects
22Chemotherapy à Specific Doses!!!
• CPA & renal function
CMF
• Capecitabine
– 750-1000 mg/m² x 2/d 2 wk/3
23
Gelman J Clin Oncol 1984; Crivellari J Clin Oncol 2000; Bajetta J Clin Oncol 2005Doxorubicine, CHF and Age
• 630 patients (3 phase III) with 32 CHF • HRage
26% >550 mg/m² 2.25 (1.04–4.86) vs 3.28 (1.4–7.65)
if >400 mg/m²
>50%: reduction of LVEF 65:£65) = 2.25
0.8 95% CI of (>65: £65) = (1.04–4.86)
Log rank p-value = 0.029 >65
0.6 Wilcoxon p-value = 0.78
0.4 £65
*Patients at risk
0.2
0
£65* 468 431 345 296 103 59 20 6 4
>65* 172 151 110 92 28 12 3 1 1
0 100 200 300 400 500 600 700 800 900 1000
Cumulative dose of doxorubicin (mg/m2) 24
Swain Cancer 2003Taxanes
• 2 cornerstones
– Paclitaxel 50% grade ³ 3 à RD: 26 mg/m²
– q2w 50 mg/m² GERICO-04
– Grade 3-4 neurosensory/motor toxicity 28%/14% (vs• CALGB (1975-1999)
Adjuvant chemo • 4 randomized trials
DFS All ≤50 • 6487 pts
> 65 yo 542 (8%)
> 70 yo 159 (2%)
OS All ≤50
51-64 ≥65
26
51-64 ≥65
• Results
– Benefit identical
– Toxicity careful!!
• Toxic deaths 1.5% Muss JAMA 2005Adjuvant chemo & mortality in 65+ stage I-III BC
Giordano* Elkin
No. total 41,390 No. total 5,081
No. w/ chemo 4,500 No. w/ chemo 1,711
Nodal status ER HR (95% IC) HR (95% IC)
pN0 any 1.05 (0.85-1.31) NA
pN+ + 1.05 (0.85-1.31) NA
pN0 & pN+ - NA 0.85 (0.77-0.95)
pN+ - 0.72 (0.54-0.96) 0.76 (0.65-0.88)
pN+ > 70 yo - 0.74 (0.56-0.97) NA
*: BC specific mortality
Adjuvant chemo is useful FIRST
in ER-, pN0 or pN+, even > 70 yo
27
Giordano & Elkin J Clin Oncol 2006ER+ ER-
CALGB 49907
(AC or CMF vs X)
RFS 56% vs 50%
(HR 0.80; P = .03)
BCSS 88% vs 82%
(HR 0.62; P = .03)
OS 62% vs 56%
(HR 0.84; P = .16)
ER+ (HR 0.89; P = .43)
ER- (HR 0.66; P = .02)
43.9% deaths
(13.1% BC vs 16.4% others vs 14.1% ?)
Second non BC 14.1%
28
Muss JCO 2019Crozier Lancet Oncol 2020
A true predictive model for
chemo-related grade 3-5 toxicity
1. 58% grade ≥ 3 toxicity
2. Risk increased w/
increasing risk score
3. AUC/ROC 0.65 (95%CI
0.58-0.71) ~ development
cohort 0.72 (95%CI 0.68-
0.77) (P = .09)
4. No association between
PS and chemo toxicity (P
= .25)
30
Hurria J Clin Oncol 2016CARG-BC 473 pts evaluable/501 (283 development/190 validation), median age 70 (65-85)
Stage I/II/III 39%/41%/20%, TNBC/ER+/HER2+ER+/HER2+ER- 24%/48%/10%/17%
Grade 3-5 AEs 46% (haematological 25%/non-haematological 36%)
31
Magnuson J Clin Oncol 202132 Magnuson J Clin Oncol 2021
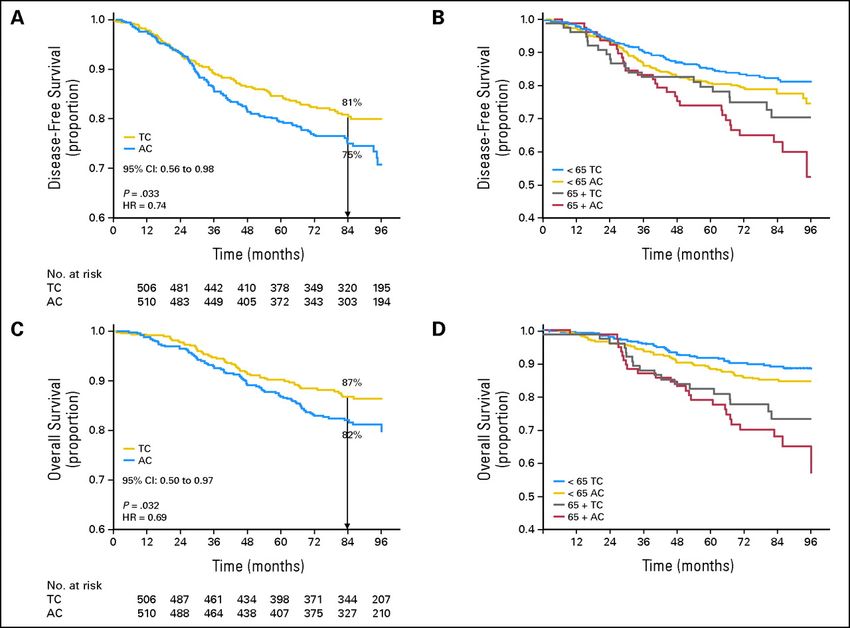
Fig 1. Disease-free survival (DFS) and overall survival (OS) (A) DFS by treatment; (B) DFS by treatment
and age; (C) OS by treatment: 1 day; (D) OS by treatment and age
Jones, S. et al. J Clin Oncol; 27:1177-1183 2009
Copyright © American Society of Clinical Oncology• 6,600 pts < 70
– 02/2007-08/2011
– 112 institutions in 9 European countries
– 11,291 registered patients
– 6,673 enrolled (59.1%)
Mammaprint
Risk of distant recurrence
@ 5 years
w/ no treatment
Primary goal
In patients w/ high-risk clinical & low-risk GEP and no chemotherapy, lower boundary of the 95% CI
34
for the rate of 5-yr survival w/o distant M+ ≥ 92% (i.e. the noninferiority boundary) at a 1-sided significance level of 0.025High recurrence score > 70 yo
• Higher likelihood of death
(HR 1.47, 95% CI 1.15-1.90)
• Chemo à lower risk of death in younger
but not in older group
35
Kizy JGO 2019ASTER 70s (EUDRACT N° 2011-004744-22, PHRC national 2011, NCT01564056)
Adjuvant chemotherapy for ER+ HER2- BC in 70+ patients
Microarray
CGA
qRT-PCR
screened
randomized
Chemo = 4 TC or 4 AC or4 MC
4-yr OS
36ASTER 70s 10 key points
• Specifically for 70+ EBC women
• Common question
• Non-exclusive inclusion criteria (40% G8 ≤14 & 20% previous
cancer w/ 50% local or controlateral relapse)
• Question of treatment escalation & de-escalation
• Observational arm for ineligible patients à selection bias
• Education of both patients & physicians
• Taking/spending time to explain the relevance of a trial
• Collaboration w/ geriatrician
• QoL and acceptability
• Translational research (biobank)
37EORTC–ETF-BCG
Study 1745 (APPALACHES):
A Phase II study of Adjuvant PALbociclib as an
Alternative to CHemotherapy in Elderly patientS
with high-risk ER+/HER2- early breast cancer
Hans Wildiers, Etienne Brain, Kevin Punie
38Non-comparative randomized (2:1) phase II study
366 patients required (244:122)
Accrual 2y
Adjuvant chemo -> AI 80 centres required
70+, surgery for stage II-III
EBC ER pos, HER2 neg Pros:
adjuvant chemotherapy 1 - Easy endpoint, clinically relevant
- Feasible numbers
required according to - Similar endpoint in 1 arm was
treating physician and used in Mindact and Tolaney
study (both NEJM)
patient
2 AI + Palbo 2y - If study is + (88% not included in
CI), the conclusion and
Stratification for clinical frailty consequences can be similar as
(G8 >14 vs ≤ 14) and stage for Mindact and Tolaney study:
new standard
- QoL and OS/BCSS can be
Adjuvant chemo choice: compared to chemo as secondary
- 4 TC + G-CSF Primary endpoint endpoints
Cons:
3y DRFI (distant metastases or death - No formal comparison w/ chemo
- 4 EC or AC + G-CSF
from breast cancer) for AI+Palbo arm group for primary endpoint
- 12 taxol weekly - Less data on QoL/OS/BCSS
- 3-year DRFI ofGeneral recommendations for adjuvant
chemo & trastuzumab in older BC patients
• Focus on ER- and HER2+ (if > 5 mm)
• Regimen
• Validated 4 AC, 6 CMF
• Options 4 TC; paclitaxel qw x 12?; liposomal doxorubicin?
• No! capecitabine, docetaxel qw
• No data! Sequential regimen
• Primary prophylaxis of febrile neutropenia w/ G-CSF
• No restriction on trastuzumab if chemo indicated
• 4 TC + trastuzumab
• Paclitaxel qw x 12 + trastuzumab (Tolaney)
• TCH x 6?? (but very unlikely in older patients since carboplatin AUC 6!)
• Trastuzumab alone: can be considered, especially for unfit patients (+ ET if ER+)
• Shorter duration for trastuzumab (6 months?)
Cheung, Livi, Brain in Geriatric Oncology/Elsevier, Editors Extermann, Fulop, Dale, Klepin & Brain 2019
Brain J Ger Oncol 2019Thérapies ciblées
Cleopatra double-blinded phase III trial
Pertuzumab + trastuzumab + docetaxel
(n = 402)
MBC L1
HER2+
R
(central review)
1:1
N = 808 Placebo + trastuzumab + docetaxel
(n = 406)
• Pertuzumab: 840 mg loading dose à 420 mg
• Trastuzumab: 8 mg/kg loading dose à 6 mg/kg
• Docetaxel: 75 mg/m2 à 100 mg/m2 depending on tolerance
• Primary objective: PFS
• Secondary objectives: OS, ORR, tolerance
• Stratification: geography, (neo)adjuvant treatment
Baselga N Engl J Med 2012Cleopatra
Swain ESMO 2014; Swain NEJM 2015Pertuzumab
CLEOPATRA
808 patients
à 127 (16%) 65+
à 19 (2%) 75+
More frequent in elderly patients
• Any grade: diarrhea, asthenia,
fatigue, anorexia, vomiting and
dysgueusia
• Grade 3: diarrhea, peripheral
neuropathy
• Dose intensity: 12% dose
escalation , 31% dose
reduction, 20-30% G-CSF
44
Miles Breast Cancer Res Treat 2013EORTC 75111-10114
(Co-PI Hans Wildiers & Etienne Brain)
Pertuzumab
+
80 pts HER2+ MBC
Trastuzumab
≥ 70 Years ® 1:1 PD T-DM1
(≥65/≥60y with co-
morbidity) Pertuzumab +
Trastuzumab +
Primary endpoint
PFS at 6 months of PH or PHM metronomic CT
Secondary endpoints
OS, BCSS, toxicity, RR (RECIST v1.1), Stratification: ER/PgR, previous HER2 treatment, G8
HRQoL, evolution of GA during treatment
Pertuzumab 840 mg loading dose, further 420 mg q3w iv
Trastuzumab 8 mg/kg loading dose, further 6 mg/kg q3w iv
Chemotherapy Metronomic chemotherapy: cyclophosphamide 50 mg/d po continuously
On progression Option to have T-DM1 (3.6 mg/kg iv q3w) till progression
46
Wildiers Lancet Oncol 2018Elderly/frail HER2+ MBC population
Metronomic chemo + TP
• à 7-mth longer median PFS vs TP
• Acceptable safety profile
• T-DM1 at progression active
• Alternative to standard taxane + TP?
47
Wildiers Lancet Oncol 2018• SEER database
• 2,028 patients ≥ 66, stage I-III, 2005-2009, trastuzumab
– 71.2% < 76
– 66.8% w/o comorbidities (Charlson)
– 85.2% w/ chemotherapy
– 81.7% w/ complete trastuzumab treatment (> 9 months)
– Factors correlated w/ incomplete treatment
• Age 80+ vs 66-70 OR 0.40 (0.30-0.55)
• Comorbidities 2 vs 0 OR 0.65 (0.49-0.88)
Vaz-Luiz. J Clin Oncol 2014- 2 gr 3 LVSD (0.5%) (95% CI, 0.1%-1.8%)
- 13 significant asymptomatic LVEF decline
(3.2%) (95% CI, 1.9%-5.4%)
Tolaney NEJM 2015! ! ! ab
T um 275 patients
uz 2009-2014
C
st
tra !
Non-infériorité
E
HR 1.22-1.69 β 20%
au e Suivi 4.1 ans (0.3-8)
e iq u
P
i é
c éat
o
S
ss st
a y
io re s
R E q
e l
u tn
re peu
a
h
e
im êt
c as
p
t
u tê
Pe
50
Sawaki JCO 2020IBCSG 55-17 TOUCH
Phase II open-label, multicenter, randomized trial of neoadjuvant palbociclib in combination
with hormonal therapy and HER2 blockade versus paclitaxel in combination with HER2
blockade for elderly patients with hormone receptor positive/HER2 positive early breast
cancer
A: paclitaxel
Early BC, trastuzumab
ER+, surgery
HER2+, pertuzumab +
≥65 years,
Neo-adj.
R
B: palbociclib
treatment
planned letrozole
trastuzumab surgery
pertuzumab +
Week 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16
staging Pertuzumab:
loading dose
FFPE sample FFPE sample
IBCSG 55-17 TOUCH | Investigator meeting 27 September 2019Targeted Therapy for MBC in Elderly
• Generally feasible to administer
• Benefit is variable
• Toxicity often (slightly) increased; but often lower than
chemotherapy toxicity
• Beware of a high-selection bias
à Most data only in “fit” elderly!
• Balance efficacy vs toxicity (+ cost) in every individual
• Challenging choice of right partner (endocrine therapy)
and multi-blockade (e.g. EORTC 75111 trial) 53Tumour General
extent health
TNM status
Geriatric assessment
Life expectancy
Treatment toxicity
Tumour Patient
biology preference
Luminal A/B & acceptability
HER2 & TNBC
Gene expression profile
54Attitudes et attentes
2 questions
1. Chirurgie vs HT seule
2. ± CT adjuvante
• Etude observationnelle prospective, observationnelle
• 3416 patientes 70+ K sein localisé, 56 centres, 2013-2018
– 2979 RO+ : 2354 chirurgie (82%) et 500 HT seule (18%).
– Bien que chirurgie > HT chez sujets « fit », plus de choix pour HT seule
si information « renforcée » (temps + documents d’aide à la décision
couvrant pronostic, effets secondaires, etc.)
55
https://agegap.shef.ac.uk.56 Biganzoli Lancet Oncol 2012; Cancer Treat rev 2016; Brain J Ger Oncol 2019
General recommendations for adjuvant
chemo & trastuzumab in older BC patients
• Focus on ER- and HER2+ (if > 5 mm)
• Regimen
• Validated 4 AC, 6 CMF
• Options 4 TC; paclitaxel qw x 12?; liposomal doxorubicin?
• No! capecitabine, docetaxel qw
• No data! Sequential regimen
• Primary prophylaxis of febrile neutropenia w/ G-CSF
• No restriction on trastuzumab if chemo indicated
• 4 TC + trastuzumab
• Paclitaxel qw x 12 + trastuzumab (Tolaney)
• TCH x 6?? (but very unlikely in older patients since carboplatin AUC 6!)
• Trastuzumab alone: can be considered, especially for unfit patients (+ ET if ER+)
• Shorter duration for trastuzumab (6 months?)
Cheung, Livi, Brain in Geriatric Oncology/Elsevier, Editors Extermann, Fulop, Dale, Klepin & Brain 2019
Brain J Ger Oncol 20192 worlds confronting one another?
• Young patient • Elderly patient
– Social and family obligations (children) – QoL+++
– Quantity of life +++ – Independence
versus – Staying at home
or
• Oncology
– Therapies and innovation
– Toxicity, response, survival
+ GA• Geriatrics
– Symptoms, diagnosis
– Quality of survival, i.e. amount of
• RECIST
? life with good QoL
• NCI CTC v4.0 • Cognition
• Survival (DFS, PFS, Genomic
DDFS, OS) GA • Functional status
defects
• Translational research defects • Nutrition, etc.
– Fast-moving world
targeted targeted– Requiring time
therapy geriatric– "Global portrait" of patient & GA
– "Molecular portrait" of tumour & GEP
intervention
58Charlson, CIRSG, CGA, MCI,
MNA, GDS, MMS, ADL, IADL,
FEC, AACR, FAC, ASCO, anti-PDL1, GFI, TUG, JAGS, EUGMS, G8,
anti-PD1, CMF, SABCS, PD-1, PD-L1, CARG, CRASH, Oncodage,
DXR, PK/PD, CEX, 5FU CDDP, Calvert, VES-13, TRFs, JGO, NIA,
ESMO, Chatelut AUC, CTC, TILs, SoFOG, Walter’s score, Lee’s
population PK, cfDNA, EORTC, score, CRASH, etc.
FOLFIRI, ctDNA, FOLFOX 7, CPA, DFS,
CALGB, DDFS, OS, TTP, NCI, CYP
P450, JCO, JNCI, HER2, PI3K, mTOR,
Phase 0, ECCO, antibody drug
conjugate ADC, ib and ab, SWOG,
etc.
59FEC, FAC, SoFOG, ADL, IADL, CMF,
SABCS, DXR, PK/PD, CEX, G8, EORTC,
5FU CDDP, MCI, Calvert and Chatelut
AUC, CARG, GDS, population PK, AD,
FOLFIRI, MMS, FOLFOX, CPA, CRASH,
SWOG, DFS, OS, TTP, NCI, GERICO, TILs,
CARG, anti-PDL1, anti-PD1, EORTC TFE,
JCO, JNCI, Charlson, JGO, CIRSG, PD-1,
PDL-1, ctDNA, EGS, EGA, MNA, GFI,
Unicancer, Lee’s score, JAGS, etc.
To be practice changing,
let us be practice sharing!
6061
Optimising treatment
in older cancer patients
is precision medicine too!
7th edition
June 2021
62You can also read

















































