CAPILLARY PUNCTURE VS. VENIPUNCTURE: ADVANTAGES AND LIMITATIONS TO USING CAPILLARY BLOOD - BRAD S. KARON MD PHD PROFESSOR OF LABORATORY MEDICINE ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Capillary Puncture vs. Venipuncture:
Advantages and Limitations to Using
Capillary Blood
Brad S. Karon MD PhD
Professor of Laboratory Medicine and Pathology
Chair, Division of Clinical Core Laboratory Services
©MFMER | 3793435-1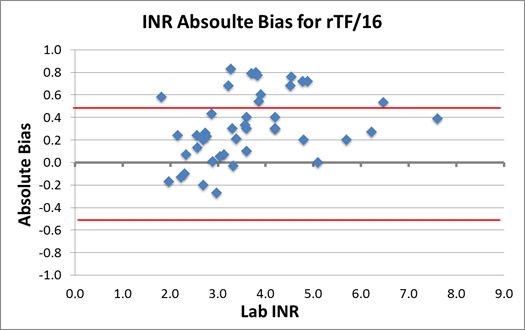
Disclosures
Relevant Financial Relationship(s):
Nothing to Disclose
Off Label Usage:
Nothing to Disclose
©MFMER | 3793435-2Outline
• Capillary vs venous blood
• Use of capillary blood and arterialized capillary blood for infants
and children
• Use cases for capillary blood in adults
• Summary
©MFMER | 3793435-3Blood circulation
• Heart lungs heart arteries capillaries (deliver
oxygen/glucose to tissue, pick up waste) veins heart
• Heart: blood sampled directly from heart in ICU, cath lab
• Lungs: No option to sample capillary bed in lungs
• Arteries: Peripheral arteries can be accessed when needed
• Veins: Easy to access, few differences from arterial blood
• Capillaries: Content reflects local tissue exchange, partially
venous and partially arterial in content, cannot be directly
accessed (too small)
©MFMER | 3793435-4Venous blood
• Reference sample for most laboratory testing
• Whole blood removed directly from vein by venipuncture or catheter
• Easy to obtain (compared to arterial)
• Reflects circulating concentration of cells, analytes, proteins in blood
• Defined by ADA as reference type for diabetes diagnosis (venous
plasma glucose, glucose concentration available to brain)
• Situations requiring arterial blood or possible differences
• Oxygenation status: requires arterial blood for pO2/sO2 with exception
of arterialized heelstick for infants
• Ammonia and lactate: Some data to suggest arterial better reflection of
disease state, differences most often minimal
©MFMER | 3793435-5Capillary blood
• Capillaries cannot be directly accessed (sample capillary bed)
• “Capillary blood” is mixture of arterial blood, venous blood,
intracellular fluid (cells break during capillary puncture), and
interstitial fluid (not blood, fluid that bathes tissue)
• Cellular content of K, AST, LDH several-fold higher than
circulating blood
• Many analytes reach equilibrium between interstitial fluid and
circulating blood, but not all things we want to measure
• No hemoglobin or cellular material (amazingly Hgb and cell counts work
OK, but more variability in capillary blood)
• Glucose lag after eating (venous, then capillary, then interstitial)
©MFMER | 3793435-6Mayo Clinic guidelines for capillary collections
• Heelstick up to 12 months or 20 lb
• Fingerstick after 12 months or 20 lb
• If heelstick depth not to exceed 2 mm
©MFMER | 3793435-7Capillary sampling limitations: biochemical testing
• Blood gas and acid base
• Heating heel of infant with “arterialize” capillary blood
• pO2 of arterial blood normally 80-100 mm Hg (assume adequate
oxygen exchange in tissues)
• pO2 of venous blood normally 40-50 mm Hg (no information
about oxygen delivery or exchange to tissues)
• Can assess acid-base status, indirectly respiratory status thru pCO2,
but not oxygenation with venous blood gas
• “Arterialized” heelstick samples in adults can provide information
on oxygen exchange thru analysis of pO2 (separate reference
intervals required)
©MFMER | 3793435-8Capillary sampling limitations: biochemical testing
• Fingerstick capillary blood gas can provide information
equivalent to venous blood gas (acid-base status, indirect
information about respiratory status thru pCO2)
• Fingerstick capillary pO2 does not correlate with arterial blood
pO2, provides no information on oxygenation
©MFMER | 3793435-9Capillary sampling limitations: biochemical testing
Hemolysis and potassium
• Measurement of potassium from capillary samples
• Patel et al, 1983 Arch Dis Child 1988;63:752-3
• 40 neonates with art line and capillary blood gas and electrolyte
measurements
• Capillary K ran 1.2 ± 1.0 higher than art line after 2 mL flush
• Capillary K higher than arterial, but why?
©MFMER | 3793435-10Studies of hemolysis in capillary puncture
• Algeciras et al., Clin Biochem 2007;40:1311-6
• Studied plasma Hgb level in 151 infant capillary punctures
• 45 samples collected by 14 trained outpt phleb (Group 1)
• 37 samples collected by 5 re-trained outpt phleb (Group 2)
• 69 samples collected from inpatient nursery (Group 3)
• Group 1 median Hgb 128 mg/dL
• Group 2 median Hgb 164 mg/dL
• Group 3 median Hgb 156 mg/dL (not stat sig)
• Overall mean Hgb 162 mg/dL
• Capillary samples contain more free hemoglobin (hemolysis) than
venipuncture, can’t train that away
©MFMER | 3793435-11Studies of hemolysis in capillary puncture
• Meites et al, Clin Chem 1981;27:875-8
• Studied mean plasma Hgb level in 417 capillary punctures, monolet lancet
and lithium heparin microtainer, 15 trained technologists
• Typical venous free Hgb < 50 mg/dL
Age n Mean Hgb
0-13 d 176 390 mg/dL
14d- 3 mo 47 220 mg/dL
3 mo – 2 yr 49 160 mg/dL
> 2 yr 145 150 mg/dL
Overall 417 260 mg/dL
©MFMER | 3793435-12Effect of hemolysis on capillary K
• Oostendorp et al, Arch Pathol Lab Med 2012;136:1262-65
• Compared avg K to H index (semi-quant) for 332,760 venous and 2620 capillary
samples (ED and ICU excluded)
Venous samples Capillary samples
H index % samples Avg K % samples Avg K
0 81.1 ~ 4.0 37.5 ~ 4.0
1 13.6 ~ 4.2 42.2 ~ 4.5
2 4.3 ~ 4.5 10.6 ~ 5.0
3 0.4 ~ 4.8 3.9 ~ 5.2
4 0.2 ~ 5.0 2.4 ~ 5.5
≥5 0.1 ~ 5-6 3.0 ~ 6.0
©MFMER | 3793435-13Capillary K, blood gas samples
• Mayo Clinic cap gas reference interval study (n=22)
• Heal warming, capillary tube collections, hand transport
12.0
10.0
Whole blook K 8.0
6.0
4.0
2.0
0.0
0 5 10 15 20 25
Subject #
• Mean K = 5.7 mmol/L
• Range 4.0 – 10.0
• Made decision not to report K with capillary blood gas
©MFMER | 3793435-14Capillary K (hemolysis) conclusions
• Capillary samples contain more free Hgb (hemolysis) than
venipuncture samples
• For a given amount of free Hgb, raise in K higher for capillary
compared to venous samples
• Release of K from cells and tissue during capillary puncture?
• Measurement of capillary K best limited to equipment with H
index measurement
• Even then lab should consider different H index cut-off for capillary
samples, or apply cut-off strictly
• Biochemical tests with analytic interference (direct bilirubin) from
free hemoglobin also rejected frequently with capillary samples
©MFMER | 3793435-15Cell counts using capillary blood
• Variability due to variable amount of interstitial fluid (no cells) in
specimens
• Capillary samples more prone to clot due to time to collect and
method of collection
• Fully clotted specimens rejected by lab
• Partially (micro) clotted specimens can have erroneous cell counts
reported
• Use of a transfer device (device that introduces EDTA into specimen
before it reaches the tube) may help
©MFMER | 3793435-16Capillary vs venous cell counts (using transfer device)
HGB capillary vs. Venous Collection
20.0%
15.0%
% Difference 10.0%
5.0%
1st Capillary
0.0%
2nd Capillary
-5.0%
-10.0%
-15.0%
-20.0%
10.0 12.0 14.0 16.0 18.0 20.0
LH 750 - Venous
PLT capillary vs. Venous Collection
80.0%
60.0%
40.0%
% Difference
20.0%
1st Capillary
0.0%
2nd Capillary
-20.0%
-40.0%
-60.0%
-80.0%
0 100 200 300 400 500
LH 750 - Venous
©MFMER | 3793435-17Mayo approach to capillary collections for kids
• If ≤ 1 cc blood needed, phlebotomists given script to ask parent
whether capillary or venipuncture collection preferred
• Some other institutions successful at getting over 1 cc blood via
capillary collection
• Mayo practice
Capillary heelstick bilirubin very common
Capillary heelstick CBC fairly common, data suggests higher than
desirable (5-6%) redraw rate for both due to clotting
Fingersticks in children not common (capillary blood gas in children)
Newborn screening
©MFMER | 3793435-18What tests should not be collected capillary for infants and
children?
• K very high in heelstick samples
• Lactate tends to run high, caution
• Other blood gas and electrolytes OK
• Liver function (disease) tests not evaluated
• Most other chemistries OK, reject many direct bilirubin due to
hemolysis analytical interference
• CBC with diff OK
• Coag probably not (see adults, very limited application infants
and children)
©MFMER | 3793435-19Capillary sampling: Adults
• Capillary sampling limited to situations requiring frequent
sampling, rapid turnaround time, or sample collection in non-
traditional settings
• Primary uses capillary glucose testing and point of care INR
monitoring
©MFMER | 3793435-20Capillary glucose measurement
• Common at home and in hospital
• At home: Self-monitoring of blood glucose (SMBG), improves diabetic
outcomes (still controversial for Type 2 diabetes)
• In hospital: Facilitates glycemic control, need rapid decisions to titer
insulin and prevent hospital-acquired hypoglycemia (2-fold increase in
chance of death in hospital)
©MFMER | 3793435-21Capillary glucose measurement
• Capillary vs. arterial/venous glucose
• Two primary limitations capillary glucose measurement
• Glucose lag: 20-50 mg/dL difference between venous and capillary
glucose in 30-60 minutes after meal (effect blunted in diabetics and
critically ill)
• Physiologic differences between capillary and venous glucose when
tissue perfusion impaired (extended lag)
• Impact of BP, edema and shock, tissue perfusion
• Blood pressure: Shock (systolic BP less than 80 mm Hg) associated with
falsely decreased or increased capillary glucose measurement
©MFMER | 3793435-22Capillary glucose measurement
• Accuracy of capillary WB at low and high glucose
• Khan et al Arch Pathol Lab Med 2006;130:1527-32
• Kanji et al Crit Care Med 2005;33:2778-85
• Only 1 of 3 FDA-approved glucose meters (healthcare use)
approved for capillary sampling in all hospitalized patients
(including critically ill patients)
• Did not meet CLSI POCT12-A3 or FDA defined requirements for
accuracy using capillary blood, but still approved as benefits of
rapid turnaround time thought to exceed dangers of inaccuracies
in capillary glucose measurement
©MFMER | 3793435-23POC INR measurement
Why monitor warfarin
• Narrow therapeutic window
• Variability in patient response
• Genetics
• Co-morbidities
• Drug and diet interactions
• Time delay (~1 day) between dosing and ability to measure
response
©2011 MFM
©MFMER | slide-24
| 3793435-24POC INR measurement
Why monitor warfarin
• Target INR 2.0 – 3.0
• INR 4.5: 2-3 fold increase in risk of bleeding
• INR 5.5: 5 fold increase
• INR >6.0: 8-10 fold increase
• Risk of repeat thromboembolism as INR decreases below 2.0
increases rapidly
• Goal is to prevent venous thromboembolism while minimizing
the risk of hemorrhage
• --Setting the right target range
• --Getting to the right target quickly
• --Staying in the therapeutic range as much as possible
©2011 MFMER| 3793435-25
©MFMER | slide-25POC INR testing
Why monitor warfarin
• Times of increased risk with sub- or supra-therapeutic levels
• Initiation of therapy
• Changes in medications and/or diet
• Illness, hospitalization
• Transitions of care
• Hospital discharge
• Provider change
©MFMER | 3793435-26POC INR testing
Why monitor warfarin
• Success and safety of therapy contingent upon
• Patient knowledge & compliance
• Education opportunities during therapy/measurement
• Provider knowledge, experience & diligence
• Need to follow up after INR result for treatment recommendation?
• Systems of care delivery
• How good is system at ensuring INR measurment at correct
time/intervals, recommendations for treatment reach patient, patient
understands recommendations
• Time in therapeutic range, incidence of both bleeding and thrombosis,
both improved by coagulation clinic or home capillary INR monitoring
©2011 MFMER| 3793435-27
©MFMER | slide-27POC INR testing
Is it accurate?
• Venous blood PT/INR testing
• Gold standard warfarin monitoring
• Venous blood in citrate anticoagulant, add back Ca and thromboplastin
(phospholipids) to activate extrinsic clotting pathway, time (in seconds)
for blood to clot is prothrombin time (PT) converted to INR
• Capillary INR monitoring
• Capillary fingerstick sample applied to strip (capillary blood will contain
some cell fragments (phospholipid), calcium not chelated with EDTA so
available to initiate clotting
• Strip contains thromboplastin (same lipid substance used in lab
PT/INR), as blood clots electrochemical current changes used to
measure clotting time in seconds (PT), convert to INR
©MFMER | 3793435-28POC INR testing
Is it accurate?
• Accuracy of POC INR relative to laboratory plasma INR
• Multiple studies show 90% or more POC INR results are within ± 0.5
INR units of lab plasma INR, 5-10% of results will differ from lab plasma
INR by ≥ 1.0 INR unit
• Need to “pair” POC and lab methods for consistent results within
healthcare system (no truth in coag)
• Warfarin dosing discrepancies common
• Favorable outcome associated with POC INR measurement means
fewer patients harmed by inaccurate POC INR compared to number
that might have harm due to insufficient monitoring without POC
• Only FDA-approved for patients stably anticoagulated with warfarin,
mostly adults
©MFMER | 3793435-29POC INR testing
Is it accurate?
• POC INR (and most other POC tests) have greater variability
over time due to lot to lot drift and change in calibration to
reference methods
©MFMER | 3793435-30Capillary sampling in adults: Other use cases
• Hemoglobin A1C (monitor glycemic control per guidelines in
diabetic patients)
• Lipid testing (perhaps, accuracy still an issue with capillary
collection and methods)
• Sexually transmitted disease (HIV screening particularly,
although oral fluid methods also available)
©MFMER | 3793435-31Summary
• Capillary heelstick samples collected frequently in infants
• Arterialized blood gas, basic chemistries other than K and direct
bilirubin, CBCs
• In children not used frequently at Mayo, fingerstick venous blood gas
done rarely
• Capillary sampling in adults
• Primarily limited to use cases requiring rapid action after testing, or
where evidence better outcomes from POC testing
• Glucose, INR, hemoglobin A1C, possibly lipids or STDs
©MFMER | 3793435-32QUESTIONS & DISCUSSION
©MFMER | 3793435-33Next Upcoming Webinar
Quality Metrics
Michele Legried
November 18, 2020
11am-12pm CT
© MFMER | slide-34You can also read