Caring Today, Planning for Tomorrow - 09 July 2021 - Northern Ireland ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Caring Today, Planning
for Tomorrow
09 July 2021
Northern Ireland Ambulance Service Airway
Management Update June 2021
The safe and effective management of a patient’s airway, is an essential skill that
NIAS clinicians deliver to the most ill or injured patients. NIAS has a responsibility to
continually ensure that all clinical practice and supporting systems are as current as
possible. This is particularly important in relation to airway management and the skill
of endotracheal intubation practised by Paramedics.
This airway update consist of three elements:
• NIAS position statement on the practice of intubation, this will become an annually
reviewed position.
• NIAS airway management clinical guideline
• NIAS end tidal monitoring clinical guideline
NIAS clinicians are asked familiarise themselves with the content of the guidelines.
Points to emphasise:
• Step wise approach to airway management is essential
• Intubation is not a performance maker for resuscitation or airway management
• The use and understanding of end tidal monitoring should be considered for all
critically ill and injured patients and essential when an I-GEL or ETT is used
Paramedics must keep a log of their airway interventions to be discussed at an annual
review of airway skills and exposure. This will be digital in the future via REACH/EPR.
Some of the airway equipment has been refined to streamline equipment carried
and intervention delivery, this is listed in the appendix of the airway guideline. Local
management teams will manage the transition of stock in a phased approach.
The aim is to refine equipment carried to stream line clinical practice. A pragmatic
approach to exact sizes used is understood until all stock rotates and specific sizes
outlined are the only sizes available.
A face to face or virtual update of these guidelines and airway practice details will
follow. Specific airway equipment bag is being developed as part of the response
bag project and an update will follow. We are scoping how to provide post intubation
checklist in a useable format and update will follow.
Any questions please contact:
Neil Sinclair, Assistant Clinical Director (Paramedicine)
Neil.Sinclair@nias.hscni.net
To consistently
show compassion,
professionalism
and respect to the
patients we care for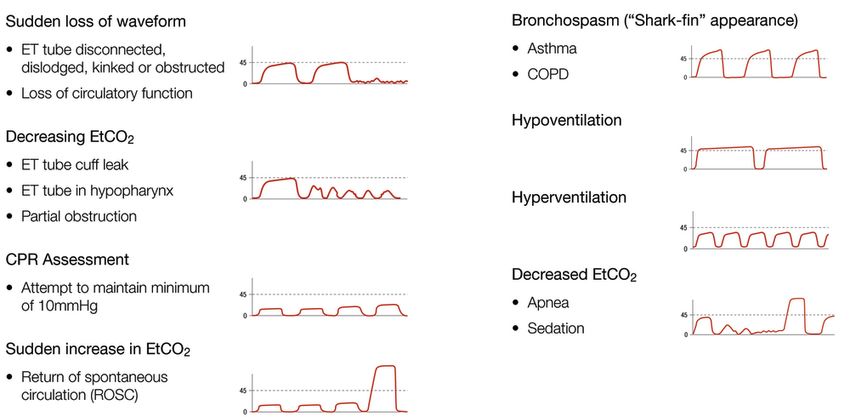
Northern Ireland Ambulance Service Intubation Position Paper v0.01
Background
Paramedics have historically practiced intubation as part of their airway management skills and is a
component of clinical practice for Paramedics in the Northern Ireland Ambulance Service (NIAS). This
scope of practice had historically covered adult and paediatric patients.
Paramedic intubation has not been without contention and discussion over the past 10 years plus.
This contention is predominantly linked to the benefit/risk trade-off for the intervention of endo-
tracheal intubation, effectively delivered this will provide effective airway management, although if
misplaced and unrecognised. This will lead to the certain death of the patient.
In 2008 Deakin et al, functioning as a JRCALC review group outlined concerns with the practice of
paramedic intubation and proposed the removal of the practice. In response to this Woolard (2008),
responded on behalf of the College of Paramedics (COP) challenging the JRCALC recommendation,
highlighting the lack of evidence base and methodology linked to the decision. With the conclusion
the skill of intubation was to remain in the scope of practice for UK Paramedics.
Further challenge regarding the practice of intubation was highlighted by an English coroner’s report
in 2013 (Connor 2013). This was in response to a tragic sequence of events, where a member of an
NHS England ambulance control centre staff suffered a cardiac arrest at work. The responding
clinicians unfortunately did not recognise an oesophageal intubation, the incident led to the death of
the patient. Since the release of these recommendations, there has been a developing change of
practice for intubation across UK ambulance trusts.
As pre-hospital clinicians and an NHS/HSC Organisation, we all have a duty to constantly review the
clinical care we provide and to improve patient safety. We should all aim to “first do no harm”, as
this has potentially devastating consequences for our patients, their families and for us as caring
health professionals.
This paper will provide a further overview of intubation within NIAS and future recommendations for
practice.
1
Discussion
Current NIAS clinical practice
The practice of adult intubation is still practised by all paramedics in NIAS. Paediatric intubation was
removed from practice in November 2020.
From an audit of NIAS 2017/18 cardiac arrest data, this demonstrates 1016 incidents where the
patient was in cardiac arrest and received CPR/active resuscitation. As Paramedic intubation is only
practised in the cardiac arrest patient presentation, this outlines the maximum number of intubation
opportunities annually in NIAS. Extrapolated across the approximate 550 operational NIAS
Paramedics and considerations to geography and higher volume presentations in more densely
populated areas. The exposure to intubation opportunities for NIAS paramedics on an annual basis is
low.
Overview of UK Clinical Practice
There have been changes linked to intubation across UK ambulance trusts since 2010. A volume of
NHS England trusts have removed the practice of intubation from standard operational Paramedics
and this is restricted to focused group of enhanced skill responders. This is outlined in an
unpublished survey with results presented in appendix A. This demonstrates that 6 of the 12 trusts
surveyed have stopped the practice of intubation for standard paramedics. No UK ambulance trusts
is practising paediatric intubation.
Key Highlights from Relevant Reports to Consider
JRCALC a critical review of airway competence (Deakin 2010)
The group believes that tracheal intubation without the use of drugs has little value in pre-
hospital practice.
There is a paucity of evidence to suggest that tracheal intubation without the use of drugs
is of patient benefit or improves outcome.
NHS England - Coroner recommendations (Connor 2013)
The level of training associated with paramedic intubation – both initial training and
subsequent refresher training, particularly given how infrequently most paramedics are
called upon to intubate.
Whether use of waveform end-tidal carbon dioxide monitors is now mandatory.
Availability of these (etc02) devices to staff, and training on how to use and interpret them.
In the absence of radical changes, in particular in relation to initial and refresher training,
ambulance services should consider whether paramedics should be permitted to intubate
patients at all.
Current Evidence Base
A high level review of current evidence (academic publications and guidelines) has been conducted.
This is not a full literature review and is aimed at high level/highlight findings and recommendations.
2
Joint Royal College Ambulance Liaison Committee (JRCALC) Guidelines 2019 – ALS guideline:
The tracheal tube is a challenging airway device to insert successfully and requires both
adequate initial training and ongoing practice. Paramedics must ensure that they have
appropriate competence to undertake it safely and that this skill has been regularly updated
and evidenced through maintaining an airway skill log.
There is no evidence that patient outcome is any better following tracheal intubation
compared with any other type of airway.
When tracheal intubation is undertaken, the availability of a bougie and use of waveform
capnography is mandatory.
Advanced Life Support Guidelines 2015 (Soar 2015)
There is no high quality evidence supporting one particular intervention over another
SAD/Tube (Soar 2015/ Fouche 2014).
Anyone attempting tracheal intubation must be well trained and equipped with waveform
capnography.
Personnel skilled in advanced airway management should attempt laryngoscopy and
intubation without stopping chest compressions; a brief pause in chest compressions may be
required as the tube is passed through the vocal cords, but this pause should be less than 5
seconds.
International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care
(Soar 2015)
Depending on the circumstances and the skills of the rescuers, use either an advanced
airway (tracheal intubation or supraglottic airway (SGA) or a bag-mask for airway
management during CPR (Soar2015).
College of Paramedics Consensus Statement on Intubation
Further research is required to understand how paramedics maintain their skill in intubation,
given the limited opportunities to use the skill in a clinical setting and lack of opportunities
with employing organisations for retraining.
The consensus of this group is that paramedics can perform tracheal intubation safely and
effectively. However, a safe, well-governed system of continual training, education and
competency must be in place to serve both patients and the paramedics delivering their
care.
Effect of a Strategy of a Supraglottic Airway Device vs Tracheal Intubation during Out-of-Hospital
Cardiac Arrest on Functional Outcome: The AIRWAYS-2 Randomized Clinical Trial (Bender 2018)
Primary outcome: There was no statistical difference in the Modified Rankin Scale score at
hospital discharge or 30 days after out-of-hospital cardiac arrest, whichever occurred sooner
3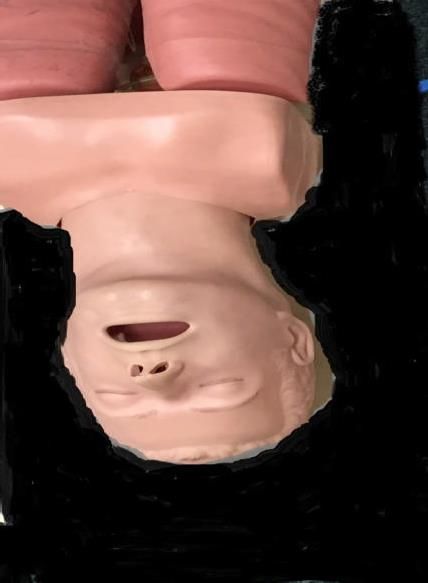
Airways 2 Results Outcome Measures I-GEL ETT
Alive with little or no disability 6.4% 6.8%
Ventilation success on first two attempts 87.4% 79%
Regurgitation 26.1% 24.5%
Aspiration 15.1% 14.9%
Conclusions and Relevance: Among patients with out-of-hospital cardiac arrest,
randomisation to a strategy of advanced airway management with a supraglottic airway
device compared with tracheal intubation did not result in a favorable functional outcome at
30 days.
Equipment
Second generation Supraglottic Airway Devices (SAD) have evolved and they are strongly
recommended for use in the pre hospital environment, NIAS carries a full range of I-Gel devices.
Waveform end tidal monitoring is defined as a key adjunct when using advanced airways (Soar
2015). NIAS provides this via a mainstream sampling device, with waveform analysis on the CORPLUS
monitor. There is an opportunity to improve service policy related to this device and practice.
Additional equipment and practices have developed in recent years which may support airway
management when using an I-GEL device. I-Gel devices have a gastric port where a Nasogastric tube
can be passed into the stomach, reducing pressure and allowing for drainage/suction. Next
generation large bore suction devices have been developed to facilitate the management of
significant stomach regurgitation and facilitate air way management (Mcclelland 2020). Investigation
of the role of both of these devices in NIAS should be fully scoped.
Access to airway equipment which is in a structured, organised and refined state is shown to reduce
error, patient harm and reduce time to intervention (Cook 2011/Swinton 2018). NIAS should
annually review all airway equipment, response bags and systems to ensure they are current, refined
and effective.
Supporting Clinical Governance
Clinical governance is classically defined as: “a system through which NHS organisations are
accountable for continuously improving the quality of their services and safeguarding high standards
of care by creating an environment in which excellence in clinical care will flourish." (Scally and
Donaldson 1998).
NIAS Airway management clinical governance:
Paramedics to record all airway interventions in a log, to allow for an objective
understanding individual exposure and education needs
4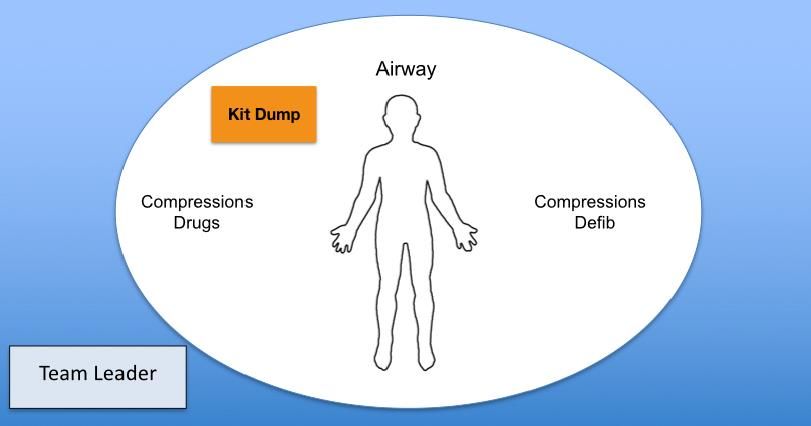
Following a review of the airway log, provide all paramedics with an annual airway
management assessment
Ensure NIAS has a clear policy re the step wise approach to airway management and support
that intubation is not a marker of success
Ensure clear policy and ongoing understanding of the use of ETC02 monitoring
Supplying tangible tools from the above guidance; NIAS specific algorithms and checklists to
support safe practice and decision making
Process and outcome markers linked to airway management and resuscitation
Equipment and response bags to be as refined as possible and provide supportive systems to
support the delivery of safe and effective care.
Never Event
Never Events are defined as Serious Incidents that are wholly preventable because guidance or
safety recommendations that provide strong systemic protective barriers are available at a national
level and should have been implemented by all healthcare providers. Strong systemic protective
barriers are defined as barriers that must be successful, reliable and comprehensive safeguards or
remedies – for example, a uniquely designed connector that stops a medicine being given by the
wrong route (Clark 2018). NIAS should develop patient harm related to intubation as a never event,
with the specific aim of never having an unrecognised oesophageal intubation in the organisation.
Conclusion
There is a changing landscape of intubation by Paramedics in the UK. The ongoing challenge of
benefit versus harm, is still the key issue and there is no clear national UK practice or evidence base.
There has been highlighted sensitive episode of patient harm/death associated with intubation with
associated coroner’s recommendation.
There are multiple reports and national guidelines which outline the need for the balanced delivery
of this intervention as part of a well governed system to optimise effectiveness and safety. There is
no clear evidence base to support or refute the impact of Paramedic intubation on patient morbidity
and mortality.
Some UK trusts have refocused the skill of intubation from all Paramedics, to a focused group of
enhanced skill Paramedics, who will have further training and a higher exposure. NIAS unfortunately
does not have a developed career framework yet to consider this option.
There is a clear theme throughout all the related narrative that there is a need to re-focus on the
patients overall clinical need when intubation may be considered, ensure the focus is on the
overarching resuscitation attempt and improving survival. There is a clear understanding that
intubation is not a marker of resuscitation attempt effectiveness. Current evidence outlines that
Intubation does not improve patient’s outcome and could be considered a source of distraction/task
fixation. There is a clear need that this practice is delivered as part of a focused and evolutional
clinical governance structure.
5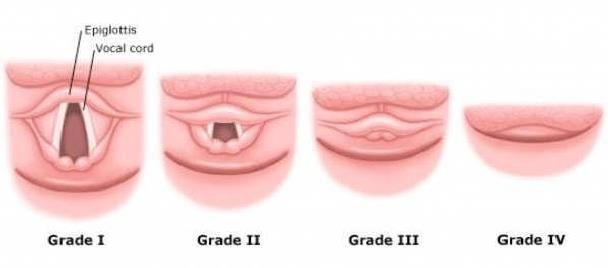
As final conclusion/recommendation; it is proposed NIAS continues to practice adult intubation with
a revised improved clinical governance system supporting and reframing the use of intubation in
NIAS. Recommendations outlined below:
Recommendations
Paediatric intubation practice withdrawn from practice November 2020 – this is to remain
Adult intubation practice to remain with an improved governance structure:
o 12 month annual review of NIAS intubation practice – (Annually April)
o NIAS never event developed – unrecognised oesophageal intubation in NIAS
o Specific guidance re stepwise airway management to be developed with embedded
decision support tools
o Specific ETC02 guidance to be developed
o Specific guidance on the use of bougies in NIAS
o Use of Nasogastric tubes and SALAD suction use to be full scoped
o Structured airway management equipment bags developed (Adult + Paeds)
o Review and refine airway equipment to be as focused and structured as possible
o Annual airway management discussion and assessment for all paramedics
o Airway intervention log in place to record individual paramedic airway interventions
o Clinical quality indicators – process measures - ETC02 compliance to be developed
o Clinical quality indicators – outcome measures - Return of Spontaneous Circulation
(ROSC) and survival at cardiac arrest to be developed
6
References
Benger JR, Kirby K, Black S, et al.(2018) Effect of a Strategy of a Supraglottic Airway Device vs
Tracheal Intubation During Out-of-Hospital Cardiac Arrest on Functional Outcome The AIRWAYS-2
Randomized Clinical Trial. JAMA. 2018;320(8):779–791. doi:10.1001/jama.2018.11597
Connor (2013) Coronor Report , Available at: https://www.judiciary.uk/wp
content/uploads/2014/07/Perrons-2014-0158.pdf (Accessed: 01/03/2021).
Cook (2011) 'NAP4: Major Complications of Airway Management in the United Kingdom', Difficult
Airway Society.
Clark (2020) Revised Never Events Policy , Available at:
https://improvement.nhs.uk/documents/2265/Revised_Never_Events_policy_and_framework_FINAL
.pdf (Accessed: 02/03/2021).
Deakin CD, Clarke T, Nolan J, Zideman DA, Gwinnutt C, Moore F, Ward M, Keeble C, Blancke W. A
critical reassessment of ambulance service airway management in prehospital care: Joint Royal
Colleges Ambulance Liaison Committee Airway Working Group, June 2008. Emerg Med J. 2010
Mar;27(3):226-33. doi: 10.1136/emj.2009.082115. PMID: 20304897.
Fouche PF, Simpson PM, Bendall J, Thomas RE, Cone DC, Doi SA. Airways in out-of-hospital cardiac
arrest: systematic review and meta-analysis. Prehosp Emerg Care 2014;18:244-56.
Gowens (2019) College of Paramedic Intubation Statement , Available at:
https://www.collegeofparamedics.co.uk/COP/Professional_development/Intubation_Consensus_Stat
ement_/COP/ProfessionalDevelopment/Intubation_Consensus_Statement_.aspx?hkey=5c999b6b-
274b-42d3-8dbc-651c367c0493 (Accessed: 02/2021).
McClelland,G. (2018) 'Soiled airway tracheal intubation and the effectiveness of decontamination by
United Kingdom paramedics (SATIATED2): A randomised controlled manikin study', Australian
jounral of paramedicine , (), pp. [Online]. Available at:
https://ajp.paramedics.org/index.php/ajp/article/view/783/1005 (Accessed: 03/2021).
Scally G and Donaldson LJ (1998) Clinical governance and the drive for quality improvement in the
new NHS in England. British Medical Journal 317(7150) 4 July pp.61-65.
Soar J, Nolan JP, Bottiger BW, et al. European Resuscitation Council Guidelines for Resuscitation
2015 Section 3 Adult Advanced Life Support. Resuscitation 2015;95:99-146.
7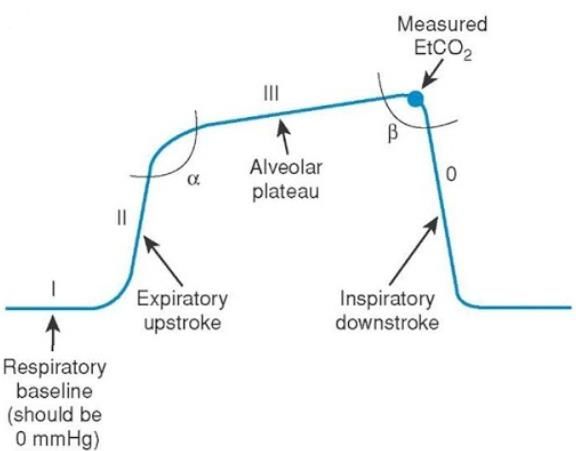
Soar J, Callaway CW, Aibiki M, et al. Part 4: Advanced life support: 2015 International Consensus on
Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment
Recommendations. Resuscitation 2015;95:e71-e122.
Swinton P, Corfield AR, Moultrie C, et al. Impact of drug and equipment preparation on pre-hospital
emergency Anaesthesia (PHEA) procedural time, error rate and cognitive load. Scand J Trauma
Resusc Emerg Med. 2018;26(1):82. Published 2018 Sep 21. doi:10.1186/s13049-018-0549-3
Woollard M, Furber R, The College of Paramedics (British Paramedic Association) position paper
regarding the Joint Royal Colleges Ambulance Liaison Committee recommendations on paramedic
intubation. Emergency Medicine Journal 2010;27:167-170.
8
Appendix – UK Ambulance Intubation Practice
Trust Intubate Intubate Adults Alternative solution
Children
SWAST No No Critical Care / HART paramedics with
Extended skills under strict governance and
annual reassessment.
LAS No* No* APP-Critical Care
Clinical Team Managers
24/7 HEMS Cover
EEAST No* No* HEMS teams, x 5 (most 24/7) plus small
number of Advanced Paramedics – Critical
Care
NEAS No Yes* Two Specialist Paramedic resource 24/7
and HEMS 4/7.
WMAS No No* Two Critical Care Paramedic RRVs
0700/1900
HEMs X4
Critical Care car 24/7
NWAS No No Senior, Advanced & Consultant paramedics
will continue to intubate adults (approx. 340
staff)
IWAS No Yes HEMS (not 24/7)
SCAS No Yes but not all, particularly NQPs. Specialist Paramedics on HEMS and Cars
WAST No Yes HEMS
YAS No No (all paramedics).Only cardiac Cardiac arrest team lead and HEMS
arrest team leaders and HEMS.
SAS No Yes HEMS/Trauma Teams/Critical Care Para
NIAS No Yes HEMS
9Northern Ireland Ambulance Service
Airway Care Clinical Guideline
Version V.01
Approved By Medical Director
Author Neil Sinclair
Date Issued 01/06/2021
Review Date 01/05/2022
Authorised staff Paramedics
EMT
Aim
Provide clear guidance and support to clinicians on airway management
techniques and equipment used within the service.
Background
Airway management by ambulance clinicians can be a challenging task given the unpredictable patient
environment. Timely, effective and decisive airway management in an emergency can mean the
difference between life and death, or between long term ability and disability. Similarly, the loss
of a patent airway and its resultant failure to adequately ventilate can be equally detrimental. This
guideline aims to support best practice and optimise patient care.
Guidance
The main priority in airway management is to confidently adopt a step wise approach. This is outlined
in the airway ladder in Appendix 1. This stepwise approach allows clinicians to ensure the patient’s
airway is open and patent at all times, either by the patient themselves, manually by clinicians or
using one or more adjuncts. This ladder also allows for clinicians to reassess the patient’s needs if
deterioration occurs. Intubation is not considered a performance marker for airway or cardiac arrest
management.
All airway equipment in use in the service is defined in appendix 10. The principles for using each
individual piece of equipment are also outlined in the attached appendices.
Date of release: March 2021 Page no: 1 Author: Assistant Clinical Director
(Paramedicine)
Version: 0.1 Review date: February 2022Patient positioning
Patients in the pre-hospital environment present in unpredictable and uncontrolled situations. This is
unlike patients in hospital who are normally on a bed in a well-lit environment, as experienced during
initial in-hospital training.
Positioning the patient well to effectively manage their airway is essential. If you cannot get sufficient
access to manage the patient’s airway, you should consider how to move the patient to achieve this,
please refer to image D in appendix 6 for information.
Suction
Suction is an essential part of all airway management. To ensure the device is working effectively,
clinicians should ensure the device is checked pre-shift according to service policy. In situations where
there is substantial airway soiling; If there is more than one resource on scene, consider using an
additional suction units from the additional vehicle, using two units + catheters will clear the debris
more quickly.
Equipment preparation
Preparation of all airway equipment prior to undertaking the task will allow for a more controlled
environment in which to manage the patients’ airway. Ideally equipment should be prepared in line
with guidance in the relevant appendices.
Equipment should ideally be prepared in a kit dump style to the right of the patients head, allowing
equipment to be passed to or picked up by the clinician’s free right hand. This pre-preparation of
equipment will allow for a structured and effective approach to airway management. Please refer to
image C+D in appendix 6.
Airway management and cardiac arrest
Intubation is a key traditional element of paramedic training which is directly linked to cardiac arrest
management. Whilst this intervention may provide a patent airway.
Thought must be given to the clinical priority of the clinical situation and patient’s needs. During a
cardiac arrest the priority of needs to be delivering effective ventilation, oxygenation and chest
compressions to the patient to optimise the patients resuscitation and survival, these basics of
resuscitation much be given priority. A stepwise approach should be adhered to at all times during the
management of cardiac arrest (Deakin 2017).
Paediatric airway management
The service supplies 2nd generation supraglottic airway devices all for paediatric patients and adults.
Guidance for these is defined in appendix 5. This equipment has replaced paediatric intubation and
should only be utilised if basic airway techniques +/- basic adjuncts do not provide adequate
airway management or ventilation. The skill and equipment to perform paediatric laryngoscopy has be
retained to allow for the removal of foreign bodies in the event of a choking patient.
ETCO2 monitoring
All monitoring devices used in the service have the facility to monitor end tidal
CO2. End tidal monitoring must be used for all patients who have a supraglottic airway device or
endotracheal tube used as an airway adjunct. All ventilated patients should have ETCO2 monitoring
(Deakin 2017). Please refer to the service clinical guideline for ETCO2 monitoring for further
information.
Date of release: March 2021 Page no: 2 Author: Assistant Clinical Director
(Paramedicine)
Version: 0.1 Review date: February 2022Appendices
1. Airway Management Algorithm
2. Basic Airway Manoeuvres
3. OPA guidance
4. NPA guidance
5. Supraglottic airway guidance (I Gel)
6. Intubation guidance
7. Intubation visual strategy
8. Post SAD/intubation placement checklist
9. Needle cricothyrotomy guide
10. NIAS Airway equipment list
Date of release: March 2021 Page no: 3 Author: Assistant Clinical Director
(Paramedicine)
Version: 0.1 Review date: February 2022Appendix 1
Northern Ireland Ambulance Service – Airway Management Algorithm
At Risk Airway Suction as required at all stages - if
*Consider direct laryngosco py as
significant volume use two suction
required to inspect for FBAO
units (if available)
Inspect airway fo r
FBAO*
Apply caution in potential
Head Tilt/Chin Lift
If airway intervention is not effective and the patient cannot be ventilated return to the initial airway intervention steps
C-spine injury
With consideration to the patient presentation is this sufficient to maintain the airway
and allow for adequate ventilation? No - Continue
Jaw Thrust
ETC02 Monitoring
Consider
With consideration to the patient presentation is this sufficient to maintain the airway
and allow for adequate ventilation? No - Continue
OPA
With consideration to the patient presentation is this sufficient to maintain the airway
and allow for adequate ventilation? No - Continue
NPA
With consideration to the patient presentation is this sufficient to maintain the airway
and allow for adequate ventilation? No - Continue
In a Cardiac Arrest it is
IGEL reasonable to streamline
to IGEL ASAP
ETC02 Monitoring
With consideration to the patient presentation is this sufficient to maintain the airway
and allow for adequate ventilation? No - Continue
Essential
Consider NIAS ETT Essential:
Algorithm ETT Post tube checklist
ETC02 monitoring
With consideration to the patient presentation is this sufficient to maintain the airway
and allow for adequate ventilation? No - Continue
Short term intervention.
Needle Cric
Rapid transport to ED or
HEMS required
Date of release: March 2021 Page no: 4 Author: Assistant Clinical Director
(Paramedicine)
Version: 0.1 Review date: February 2022Appendix 2
Northern Ireland Ambulance Service Basic Airway Manoeuvres Guidance
Approach
Gather equipment required and ensure integrity of packaging. Adopt standard precautions regarding
PPE and hand hygiene.
Indication
The approach to airway management should always be performed in a step wise manner. Patient
positioning is imperative to this process and will allow ease of head tilt-chin lift and jaw thrust
manoeuvres. Use caution with head tilt manoeuvres in trauma patients, instead a jaw thrust will
prevent any unnecessary extension of the neck.
Manual Airway Manoeuvres
Head tilt–chin lift;
Maintaining a patient’s airway and ability for ventilation is the priority, consideration should be
given to potential cervical spine injuries.
Only use the head tilt–chin lift technique to manage the airway if you are confident that there
is no risk of C-spine injury.
If positioned on the patient’s right side, the clinician’s left hand is used to apply pressure to the
patient’s forehead (Image A)
The tips of the clinician’s index and middle fingers on the right hand are used to elevate the
patient’s mandible to lift the tongue from the posterior pharynx (Image B).
If the clinician is on the patient’s left side, use the hands oppositely, but with the same
technique.
Jaw thrust;
If there is a possible risk of C-spine injury, use the jaw-thrust technique to manage the airway
manually and prevent neck movement.
The clinician should be positioned at the patient’s head, looking down at the patient’s face.
Place the fingers of each hand on the angle of the patient’s jaw (Image C).
Place the thumbs near the angle of the jaw, and apply an upwards posterior pressure to
elevate the mandible to lift the tongue from pharynx (Image D).
Date of release: March 2021 Page no: 5 Author: Assistant Clinical Director
(Paramedicine)
Version: 0.1 Review date: February 2022Head tilt/chin lift images
A B
Jaw thrust images
C D
The impact and effect of a head tilt chin lift can be seen on the video link below. This also
demonstrates the need to be careful with patients who may have a cervical injury.
https://m.youtube.com/watch?v=GzoVZ2IQaMU
Date of release: March 2021 Page no: 6 Author: Assistant Clinical Director
(Paramedicine)
Version: 0.1 Review date: February 2022Appendix 3
Northern Ireland Ambulance Service Oral pharyngeal Airway (OPA) Guidance
Approach
Gather equipment required and ensure integrity of packaging. Adopt standard precautions regarding
PPE and hand hygiene.
Indication
Indications for use include patients with an unprotected airway, despite basic airway manoeuvres.
OPA’s alone may not guarantee a patent airway and are likely to be used in conjunction with basic
manoeuvres i.e. head tilt/chin lift.
Sizing and insertion
To check the appropriate size of airway for the patient, compare the length of
the OPA airway with the distance from the middle of the incisor teeth to the
angle of the jaw (image B).
Ensure the visible airway is clear – use suction if required.
Adult patients
Open the patient’s mouth and, holding the flanged end of the OP airway, insert ‘upside down’ so the
curved surface faces upwards to the roof of the mouth (Image C).
Insert approximately half of its length and rotate the OP airway advancing it until the flanged end rests
outside the patients lips (image D).
Paediatric patients
Correctly size the OP airway as above, but insert the airway the correct way round – by depressing the
tongue with a tongue depressor – and place the airway into position.
Important
Using an OP airway is contraindicated when the patient has a gag reflex.
Once the OP is inserted, maintain close observation of the patient for signs of obstruction of the lumen
of the OP airway – clear with suction if required.
The OP airway will not protect the patient’s airway from aspiration of fluids.
A B C D
Date of release: March 2021 Page no: 7 Author: Assistant Clinical Director
(Paramedicine)
Version: 0.1 Review date: February 2022Appendix 4
Northern Ireland Ambulance Service Nasopharyngeal Airway (NPA) Guidance
Approach
Gather equipment required and ensure integrity of packaging. Adopt standard precautions regarding
PPE and hand hygiene.
Indication
Indications for use include patients with an unprotected airway, despite basic airway manoeuvres.
NPA’s alone may not guarantee a patent airway and are likely to have to be used in conjunction with
basic manoeuvres and/or an OPA. Other indications include patients who cannot accept an OPA due to
trismus.
Sizing and insertion
Check the size of the patient’s nostrils – one may be larger than the other. Select the widest
nostril.
Current evidence advises that a small-sized adult requires a size 6 airway, medium size adult
requires size 7 airway and a large-sized male requires a size 8 airway.
Lubricate with appropriate lubricant (avoid blocking the airway with excessive application,
Select the widest nostril.
Insert gently with the NP airway pointing posterior along the floor of the nose, (90degrees to
the patient’s face (Image A and B).
If resistance is felt, stop – do not force, gently rotate anticlockwise
45 degrees clockwise while continuing to insert.
If further resistance is felt, re-lubricate and try the other nostril or a smaller airway
Two NPA’s can be used in combination with an OPA as seen in image C
Cautions
Cautions include severe maxillofacial injury or suspected basal skull fracture, however with careful and
correct insertion this should not be an issue. Insertion of the NPA may cause epistaxis from localised
trauma, potentially leading to airway obstruction; consideration should be given to elderly patients
who you suspect to be on anticoagulants.
Insertion of NPA images with OPA in situ
A B C
Date of release: March 2021 Page no: 8 Author: Assistant Clinical Director
(Paramedicine)
Version: 0.1 Review date: February 2022Appendix 5
Northern Ireland Ambulance Service Supraglottic Airway (I-Gel) Guidance
Approach
Gather equipment required and ensure integrity of packaging. Adopt standard precautions regarding
PPE and hand hygiene.
Indication
Indications for use include patients who require further airway management, despite basic airway
manoeuvres and NPA/OPA use. This stepwise approach should be followed in all circumstances.
Sizing
Sizes and colour reference for I-Gel:
Sizes Weight Colour
1.5 5-12kg – Infant BLUE
2.0 10-25kg – Small paediatric GREY
2.5 25-35kg – Large paediatric BLACK
3.0 30-60kg – Small adult YELLOW
4.0 50-90kg – Medium adult GREEN
5.0 90+kg – Large adult ORANGE
Preparation and insertion
Open the I-GEL packaging and take out the pack containing the device
Place a small bolus of water based lubricant onto the smooth outer surface of the
device ready for use (Image A)
Grasp the I-GEL along the integral bit block and lubricate the back, sides and front of
the cuff.
After lubrication, avoid touching the cuff and ensure that no bolus of lubricant remains
in the bowl of the cuff or elsewhere
Introduce the leading soft tip in to the patients’ mouth in the direction of the hard
palate
Glide the device downwards and backwards along the hard palate with gentle,
continuous pushing until a definitive resistance is felt (Image B).
The incisors rest on the integral bite block.
Date of release: March 2021 Page no: 9 Author: Assistant Clinical Director
(Paramedicine)
Version: 0.1 Review date: February 2022A. B. C.
Post Insertion
Assess the patient for;
Chest rise
Equal chest sounds on auscultation
ETCO2 monitoring and results (please refer to the ETCO2 clinical guideline for further
information)
Continually assess the airway and suction as required (port of I-GEL is for NG tube placement
not suction), ventilate the patient as required.
Date of release: March 2021 Page no: 10 Author: Assistant Clinical Director
(Paramedicine)
Version: 0.1 Review date: February 2022Appendix 6
Northern Ireland Ambulance Service Intubation Guidance
Approach
Gather equipment required and ensure integrity of packaging. Adopt standard precautions regarding
PPE and hand hygiene.
Related documents;
Airway Algorithm (Appendix 1)
Intubation strategy and equipment list (Appendix 7)
Post intubation check list (Appendix 8)
Overview
This intervention should ideally be delivered when there are three clinicians at the scene. Tracheal
intubation can be a challenging procedure to perform effectively in the pre-hospital environment due
to the unpredictable environment and patient presentation. There is a significant risk/benefit balance
with this intervention and all steps must be taken to reduce associated risk.
Intubation by paramedics in the Northern Ireland Ambulance Service is not to be considered as a
performance indicator for airway or cardiac arrest management. If attempting intubation you must
expect and prepare for the intervention to be challenging to perform, this preparation will maximise
the effective delivery of the intervention and the overall resuscitation attempt.
Tube sizes
The service now carries adult tube sizes 6mm, 7mm and 8mm.
Standard female size is 7mm.
Standard male size is 8mm.
6mm tube acts as a backup size for smaller anatomy situations.
Grade of view
An accurate understanding of the grade of view seen when performing laryngoscopy is essential for
credible intubation practice. Effective preparation will help to maximise the view available. Intubation
should only be attempted when there is a grade I + II view. The grade of view should be recorded for
the any handover. The use of a bougie as described later in this document should be followed.
Date of release: March 2021 Page no: 11 Author: Assistant Clinical Director
(Paramedicine)
Version: 0.1 Review date: February 2022Image A (Cormack 1984)
Positioning
Paramedics almost always intubate on the floor in sub optimal situations. Taking the opportunity to
position your patient as effectively as possible will optimise the clinicians view and the success of the
first pass of the intubation attempt. Consideration need to be given to the patients overall position on
the floor. Assess whether the patient can and needs to be moved to facilitate effective airway
management and resuscitation, before attempting intubation. Once the patients general position has
been optimised, use what is available to you to position the patients head into the sniffing the morning
air position (Image B).
Image B
Date of release: March 2021 Page no: 12 Author: Assistant Clinical Director
(Paramedicine)
Version: 0.1 Review date: February 2022Bougies
The principle benefit of this device is that when faced with a sub optimal condition. It is easier to pass a
smaller device (bougie), than trying to pass a larger tracheal tube which will potentially obscure the
view as the tube descends.
Bougie Technique
The use of a bougie is a two person technique, the intubator operator and as assistant.
Step 1
With an appropriate kit dump assembled; the intubating clinician performs direct larangyscopy,
utilising their first view of the glottis and not removing their eyes from this view to select equipment
etc.
Step 2
From here the assistant passes the bougie into the line of sight of the intubator who under direct vision
passes the bougie through the glottis/vocal cords, firmly holding on to the bougie.
Step 3
Maintaining direct vision of the glottis/view, the assistant railroads the ET tube over the bougie into
the hands of the intubator.
Step 4
Once there is enough of the tube with the intubator and enough of the bougie with the assistant. The
assistant takes hold of the bougie and the intubator takes control of the tube. The tube is then passed
under direct vision through the cords. The bougie is then removed whilst maintaining a strong grip on
the tube position, clear communication on actions is led by the intubator. Finally the larnagyscope is
removed; post intubation checks apply as per checklist (Appendix 8).
NB The practice of passing a blind bougie and assessing for signs of “hold up” to indicate tracheal
placement should not be practiced, this practice has proven to cause trauma and damage to the
trachea.
Date of release: March 2021 Page no: 13 Author: Assistant Clinical Director
(Paramedicine)
Version: 0.1 Review date: February 2022Equipment - The preparation of equipment is an essential step which will speed the delivery and safety
of the intervention. A “kit dump” should be set up to the right of the patients head, allowing for ease
of passing or accessing equipment, as demonstrated below in (Image C).
Image C
Image D
Post checks and ETCO2
The correct placement of the tube in the trachea is essential. Post intubation checks in line with the
post intubation check list (Appendix 8) must be used. If there is any concern remove the tube.
All CORPULS m o n i t o r s in the service have the facility to monitor
ETCO2. End tidal monitoring must be used for all patients who have a
supraglottic airway device or endotracheal tube used as an airway adjunct. Further information is
available in Appendix 9.
Date of release: March 2021 Page no: 14 Author: Assistant Clinical Director
(Paramedicine)
Version: 0.1 Review date: February 2022Handover practice
Best practice when handing over a patient who has been intubated should cover the following
information:
Number of attempts to pass tube
Grade of view seen
Size of tube used
Length of tube at the patients lips
Outcome of ETCO2 monitoring, ideally with a print out
Date of release: March 2021 Page no: 15 Author: Assistant Clinical Director
(Paramedicine)
Version: 0.1 Review date: February 2022Appendix 7
Northern Ireland Ambulance Service – Intubation Strategy
Th is guidance should be used in combination with the service airway algorithm and clinical guidance. Airway
management should always be in a step wise manor.
Stage One Pre – Intubation Equipment and Patient Preparation
Prepare all equipment before attempting laryngoscopy Preparing and positing the patient well will maximise the
chance of a first time pass of the tube.
Laryngoscope and blade x2
ETT with cuff checked and lubricated x2 Do not rush into have a look this is counter
Bougie prepared productive
ETC02 present and attached to monitor Your first attempt should be your best attempt
Suction unit ready for use Positon the patient as demonstrated in appendix 6.
Thomas tube holder
Stethoscope
Stage Two – Intubation Strategy Algorithm
Step One
Intubation attempt – up to Post Intubation checklist
Success
30 seconds to perform must be used
Do not become task fixated
Failed Attempt
Considerations for change
Patients position
Three Intubation Step Two
Ventilate and Oxygenate the Operators position
Attempts Maximum Blade size
patient with basic
techniques Tube size
Intubator operator change
Manipulation of the Thyroid
cartilage
Step Three
You must change something
to continue to attempt
intubation
Are you continuing
intubation?
No
Step Four
Stop Intubation Attempt
Step Five
a
REF: RCOA 2015
Refer to the airway
algorithm and progress
management in a step wise
manner.
Date of release: March 2021 Page no: 16 Author: Assistant Clinical Director
(Paramedicine)
Version: 0.1 Review date: February 2022Appendix 8
Northern Ireland Ambulance Service Post Intubation Checklist
Northern Ireland Ambulance Service Post Intubation Checklist
The following seven steps must be confidently completed to confirm ETT placement
Tube visualised passing through cords Y/N
Bilateral chest rise on ventilation Y/N
Tube cuff inflated with no air leak Y/N
Bilateral chest sounds on auscultation Y/N
No gastric sounds on ventilation Y/N
Waveform Capnography Confirmed Y/N
Tube secured firmly in place Y/N
(Ref; RCOA 2015)
Date of release: March 2021 Page no: 17 Author: Assistant Clinical Director
(Paramedicine)
Version: 0.1 Review date: February 2022Appendix 9
Northern Ireland Ambulance Service Needle Cricothyroidotomy Guidance
Approach
Gather equipment required and ensure integrity of packaging. Adopt standard precautions requiring
PPE and hand hygiene.
Indications
For all adults, when all other airway management techniques have been unsuccessful and the patient
is at risk of deteriorating into cardiac arrest due to hypoxia.
This is a temporary emergency solution. Following this intervention, patients should be rapidly
transported to an Emergency Department or RVP with a physician led medical team EG HEMS/BASICS if
appropriate.
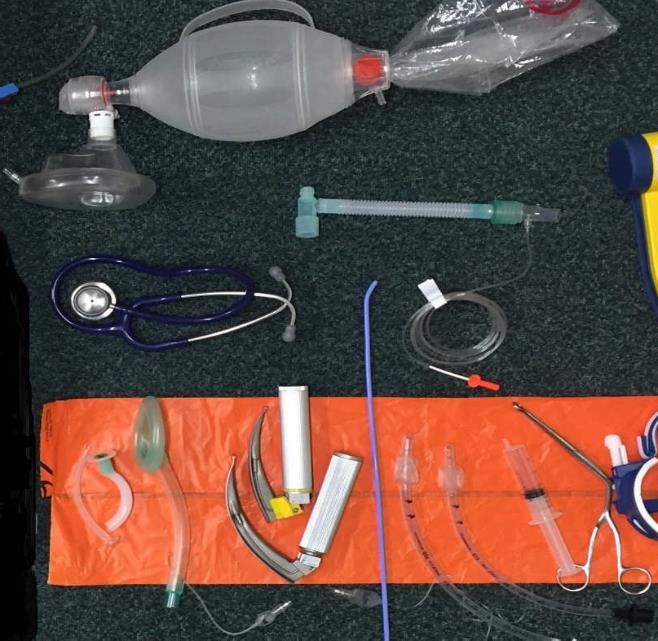
Equipment
1. 14g Cannula
2. 10ml Syringe
3. Oxygen tubing
4. Three way tap
5. Oxygen supply
Position and Anatomical Landmarks
Position the patient supine, with the head in neutral alignment. Manage the C-spine as
required.
Identify the cricothyroid membrane – a palpable recessed area, approximately 2cm below the
V notched of the thyroid cartilage (Adams apple) (Image A).
Process
Identify landmarks as described as above
Attach the 14g cannula to the syringe
Insert the cannula through the cricothyroid membrane in an angled downward motion –
towards feet (Image B)
Confirm entry into the trachea by aspirating air
Advance the cannula into the trachea, aspirating air to confirm its position. (If you are unable
to aspirate air, the cannula is not in the trachea)
Remove the syringe and needle, and secure the cannula in situ with tape.
Attach oxygen tubing and a three way tap to the cannula (Image C)
Connect tubing to the oxygen supply at rate of: 15 litres/min
Allow the oxygen to be applied for 1 second and escape for 4 seconds. Do this intermittently by
adjusting the three way tap.
Date of release: March 2021 Page no: 18 Author: Assistant Clinical Director
(Paramedicine)
Version: 0.1 Review date: February 2022A B C
Date of release: March 2021 Page no: 19 Author: Assistant Clinical Director
(Paramedicine)
Version: 0.1 Review date: February 2022Appendix 10
Northern Ireland Ambulance Service Airway Equipment List
This list is the defined list of airway management equipment that is currently in use in the Northern
Ireland Ambulance Service:
Laryngoscope handles
Adult size
Laryngoscope blades
Macintosh sizes - 2,3 4,
Nasal Pharyngeal Airway
Sizes 6mm, 7mm and 8mm
Oropharyngeal Airway
Sizes 000, 00, 0, 1, 2, 3, and 4
Oropharyngeal Airway (Second generation) I-GEL
Sizes 1, 1.5, 2 ,2.5, 3 ,4 and 5
Endotracheal tubes
Sizes 6mm, 7mm and 8mm
Airway adjuncts
Bougie 15mm
Adult Thomas tube holder – (Thomas tube select device, being introduced over 2021)
Lubricating gel 10g
Syringe 20ml
ETC02 inline measurement - CORPULS
Date of release: March 2021 Page no: 20 Author: Assistant Clinical Director
(Paramedicine)
Version: 0.1 Review date: February 2022References;
RCOA (2015) Major complications of airway management. Available at:
https://www.rcoa.ac.uk/system/files/CSQ-NAP4-Section3.pdf (Accessed: 12
September 2016).
CORMACK, R.S. and LEHANE, J. (1984) ‘Difficult tracheal intubation in obstetrics’, Anaesthesia,
39(11), pp. 1105–1111. doi: 10.1111/j.1365- 2044.1984.tb08932.x.
Deakin, C. (2017). Prehospital resuscitation. [online] Resus.org.uk. Available at:
https://www.resus.org.uk/resuscitation-guidelines/prehospital-resuscitation/ [Accessed 26 May
2017].
Date of release: March 2021 Page no: 21 Author: Assistant Clinical Director
(Paramedicine)
Version: 0.1 Review date: February 2022Northern Ireland Ambulance Service End Tidal Monitoring
Clinical Guideline V0.01
Version V.01
Approved By Medical Director
Author Neil Sinclair
Date Issued 01/06/2021
Review Date 01/05/2022
Authorised staff Paramedics
EMT
Indications for waveform capnography
Should be used for all self-ventilating patients where there is a concern re their respiratory
rate or level of consciousness
Should be used for all patients ventilated with a BVM
Must be used for all patients with an IGEL intervention
Must be used for all patient with an endotracheal tube intervention
Background
End tidal monitoring and the use of waveform capnography, is the continuous quantitative
measurement of exhaled c02 throughout the respiratory cycle. Measuring and understanding C02
provides valuable information on ventilation, haemodynamic and metabolism for a range of critically
ill and injured patients. It technically does not measure ventilation, but the content of the C02 within
the ventilation cycle. It is a powerful tool for the monitoring of any critical patient in the pre-hospital
environment.
The understanding and use should not solely focus on airway interventions, but broaden to be a key
measurement for all critical patients, providing assurance and measurement of airway, breathing
and circulation in one measurement.
The corpuls system uses mainstream ETC02 and measures the C02 concentration in the patient’s
expiratory breath (ETC02) in real time, with the peak value displayed numerically in Kpa. A normal
ETC02 is considered between 4.6-6.6 kpa, however results can be influenced by various physiological
results.
CORPULS Monitor and Equipment
NIAS provides equipment so this can be measured in self-ventilated and patients receiving positive
pressure ventilation. The corpuls system uses mainstream ETC02 measurement system, two sensors
measure the C02 as it passes between the sensors during inspiration and expiration. These sensors
as demonstrated in picture a, these are located in corpuls right side pocket marked C02
1Picture A
Procedure for nasal capnography monitring
2NB Tape is optional, be aware of any fragile skin
3Procedure for BVM/IGEL/ETT capnography monitoring
Remove the corpuls disposable oral connector from its package
Attach the in line connector to the breathing circuit, via BVM/IGEL/ETT
Connect the corpuls ETC02 sensors to the oral connector
If placing an ETT, placement confirmation needs to be part of a multi check process
Confirm ETC02 wavefrom and values are disaplayed on the monitor
4ETC02 Values and Waveforms
It is important to have an understadning of the values, wave froms and any trends to make optimal
use of ect02 monitoring.
Waveform capnography consists of four phases – diagram a/b
Phase I – Inspiratory baseline - reflects inspired gas devoid of c02
Phase II – Expiratory upstroke – reflects the transition of anatomical dead space and alveolar
gas from the alveoli/Bronchioles
Phase III – Alveolar plateau reflects last of the alveolar gas being sampled
Phase 0 – Inspiratory down stroke – reflects the beginning of inspiration
Diagram a
Diagram B
5Change in Trends
Becoming familiar with ETC02 values, waveforms and understand this in the context of the patients
presentation is key.
Diagram c
Physiological factors which may affect ETC02 levels – Diagram d
6ETC02 and Cardiac Arrest
ETC02 can be a valuable tool to assess the patient’s conditions and the effectiveness of the
resuscitation attempt, it has considerable more scope than historic focus of only tube placement
confirmation.
PQRST pneumonic for ETC02 assessment in cardiac arrest
Diagram E
P Position of the tube
Q Quality of the compressions/ventilation
R ROSC detection
S Strategy for further treatment
T Termination of resuscitation
The use of ECT02 alone should not be used to terminate resuscitation (JRCALC 2019 ALS Guideline)
If the capnography trace if flat post intubation, then it must be assumed that the tracheal tube is
sited incorrectly and must be removed – JRCALC 2019 ALS Guideline.
References
JRCALC 2019 ALS Guideline
7You can also read