CCS Heart Failure Guidelines: 2014 Update On New Therapies, Biomarkers, Anemia Management, And Complex Cases - May 2015
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
CCS Heart Failure Guidelines: 2014
Update On New Therapies,
Biomarkers, Anemia Management,
And Complex Cases
May 2015
Disclosures
• Justin Ezekowitz
– Honoraria: Bristol-Myers Squibb, Novartis, Pfizer; Clinical Trials: AMGEN,
Bayer, Bristol-Myeres Squibb, Johnson & Johnson, Novartis, Pfizer
• Eileen O’Meara
– Honoraria: Novartis, Otsuka, Pfizer, Servier; Clinical Trials: Novartis
• Shelley Zieroth
– Speaker honoraria: Pfizer, Medtronic, Servier
• Serge Lepage
– Honoraria: Abbott Vascular, Bayer, AstraZeneca, Boehringer Ingelheim,
Otsuka, Pfizer, Servier; Clinical Trials: Abbott Vascular, AMGEN,
AstraZeneca, Bayer, Boehringer Ingelheim, Bristol-Meyers Squibb,
GlaxoSmithKline, Otsuka, Pfizer, Servier, sanofi-aventis
www.ccs.ca Heart Failure Guidelines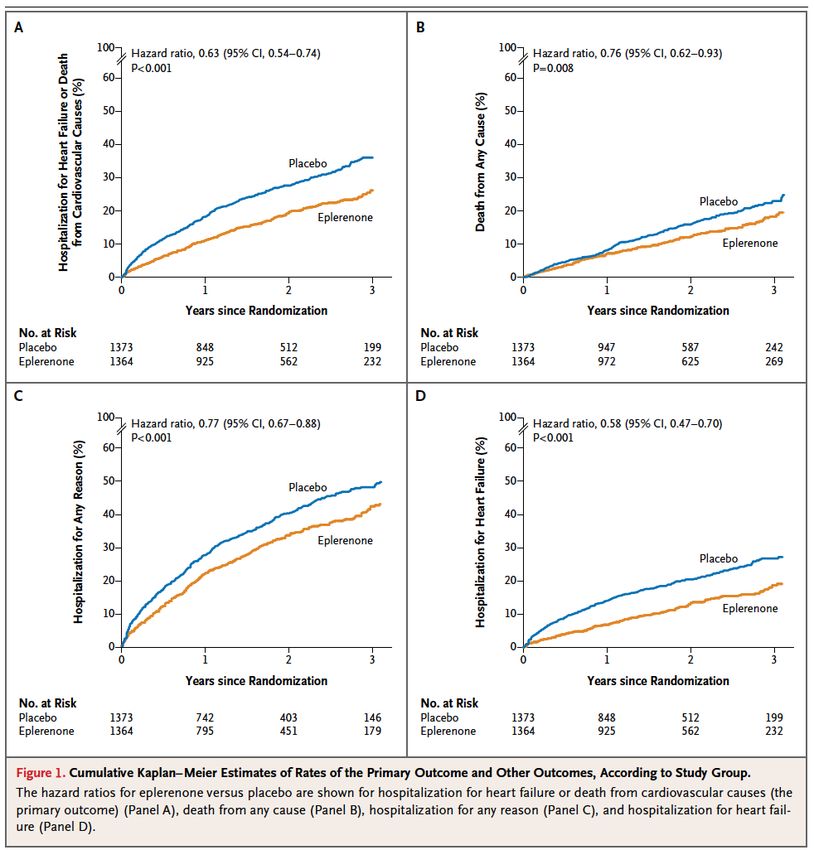
Audience Participation
• Case summaries have been distributed and will be used
with Turning Point software to collect responses throughout
the session.
• Microphones are available in the room for the question and
answer portion of this presentation.
www.ccs.ca Heart Failure Guidelines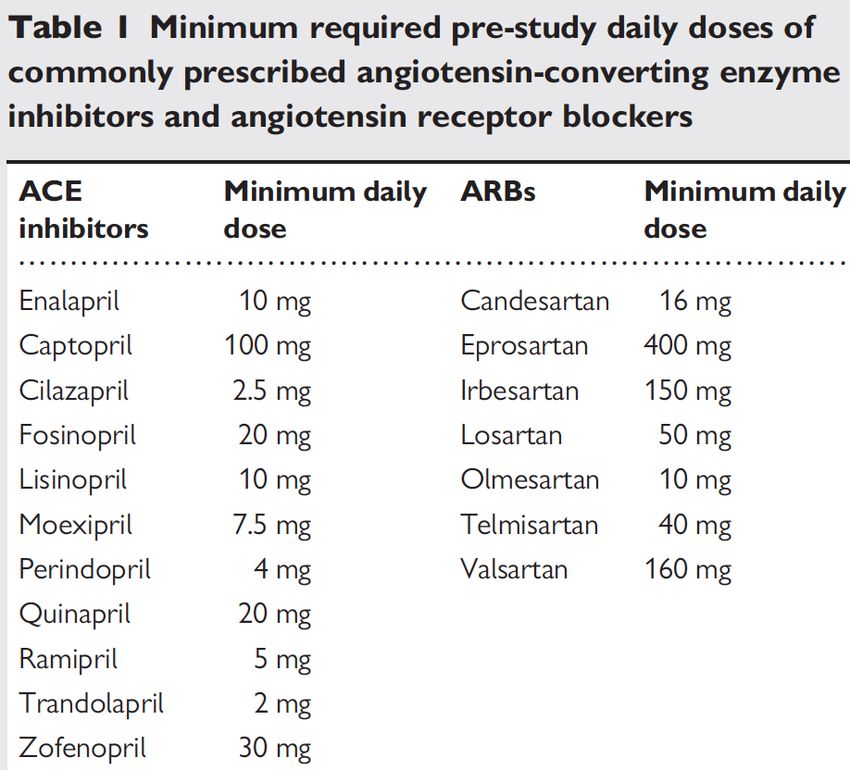
Topics
1. Spiro and HFpEF: When to use spironolactone in HFpEF
(TOPCAT and new regional variations paper could be
briefly discussed); which patients, how to monitor
2. Anemia: When should I investigate, what should I look for
and when should I treat or refer?
3. NPs: NYHA 2/3 with elevated BNP; Asymptomatic new
referral: do I test and what do I do?
4. LCZ: Up titrating ACEIs or ARBs assuming that LCZ will
become available in 2016
www.ccs.ca Heart Failure Guidelines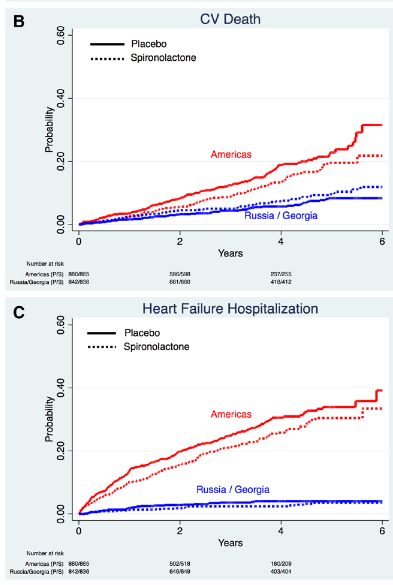
Spironolactone and HFpEF www.ccs.ca Heart Failure Guidelines
HF with Preserved Ejection Fraction
What’s the Truth?
A) HF-PEF incidence and mortality is less than HF-REF
B) HF-PEF incidence and mortality is equivalent to HF-REF
C) HF-PEF incidence and mortality is more than HF-REF
www.ccs.ca Heart Failure GuidelinesHF with Preserved Ejection Fraction
What’s the Truth?
B) HF-PEF incidence and mortality is equivalent to HF-REF
www.ccs.ca Heart Failure GuidelinesHF-PEF Guidelines 2006-2012 www.ccs.ca Heart Failure Guidelines
HF – Preserved Ejection Fraction
• No pharmacologic therapy specifically recommended for
HF-PEF with “strong” evidence
• Complicated phenotype(s) and trial design(s)
• Different patient demographics
• Many pharmacologic and non-pharmacologic
interventions have been tried:
• ACE, ARB, BB, exercise, etc
• Recently: mineralocorticoid receptor antagonists (MRA’s)
www.ccs.ca Heart Failure GuidelinesCase: Mrs. PEF
• ID: 75 yr female referred from GP for new onset HF
• HPI: 4 mos progressive SOBOE, 2+bilateral pitting edema,
2 pillow orthopnea. GP started furosemide 1 month ago;
SOBOE improved and orthopnea resolved.
• PMHx:
– HTN x 20 years
– DM x 15 years, on glyburide
– Atrial fibrillation x 3 years, on NOAC and rate controlled
– COPD on puffers
www.ccs.ca Heart Failure GuidelinesCase: Mrs. PEF
Medications
HF Furosemide 40mg daily (started 1 mo ago)
HTN HCTZ 25mg daily
Potassium chloride 20MEq daily
Amlodipine 5mg daily
ECASA 81mg daily
DM Glyburide 5 mg po BID
Rosuvastatin 10mg daily
Atrial Fibrillation Metoprolol 25mg BID
Dabigatran 110mg BID
www.ccs.ca Heart Failure GuidelinesCase: Mrs. PEF
• Investigations:
– Echo: dilated LA, LVH, EF = 45%, diastolic dysfunction, aortic
sclerosis
– MIBI: normal perfusion, EF 50%
– ECG: atrial fibrillation, HR = 68bpm
– CXR: normal cardiac silhouette, no pulmonary edema
– Labs: Scr = 125 umol/L; K = 4.8 mmol/L; Na = 134 mmol/L
• Currently NYHA 3
• BP = 125/73 mmHg sitting; no postural drop
• CVS Exam = JVP 3 cm ASA, Euvolemic, 2/6 SEM
www.ccs.ca Heart Failure GuidelinesCase: Mrs. PEF – Question
What would you do next?
A. See in follow-up 6 month
B. Uptitrate amlodipine
C. Initiate spironolactone 12.5
mg po OD with follow-up
electrolytes
D. Refer for angiogram
0% 0% 0% 0%
e
am
th
..
n
12
on
pi
gr
di
m
ne
gio
lo
6
to
am
an
p
ac
-u
or
l
e
no
w
at
rf
llo
ir o
itr
fe
fo
t
Re
sp
Up
n
te
ei
tia
Se
i
In
www.ccs.ca Heart Failure GuidelinesTOPCAT
• Double-blind, placebo-controlled RCT
• NHLBI Sponsored
• Significant Canadian involvement
• Randomization, 1:1
– Spironolactone, 15, 30, 45 mg daily vs placebo
• Primary Composite Endpoint:
– CV death, HF hospitalization, or aborted cardiac arrest
• Follow-up 6 years
• Assumed: 3-year placebo rate of 17.4%
Desai, Rationale and design, Am Heart J 2011
Pfeffer, TOPCAT NEJM 2013
www.ccs.ca Heart Failure GuidelinesTOPCAT: Eligibility Criteria
• Inclusion: • Major Exclusion:
– Symptomatic Heart Failure – eGFR2.5mg/dL (221umol/L)
– stratified according to: – uncontrolled hypertension
• HF Hospitalization within the – AF with rate > 90/min
past year, or
– recent ACS, PCI or CABG
• Elevated natriuretic peptides
– restrictive, infiltrative, or
– BNP ≥100 pg/mL
hypertrophic cardiomyopathy
– NT-proBNP ≥360 pg/mL
Desai, Rationale and design, Am Heart J 2011
Pfeffer, TOPCAT NEJM 2013
www.ccs.ca Heart Failure GuidelinesTOPCAT: Primary Outcome
(CV Death, HF Hosp, or Resuscitated Cardiac Arrest)
351/1723 (20.4%)
320/1722 (18.6%)
Placebo
Spironolactone
HR = 0.89 (0.77 – 1.04)
p=0.138
Pfeffer, TOPCAT NEJM 2013
www.ccs.ca Heart Failure GuidelinesTOPCAT: Enrollment Strata
• BNP/NT-proBNP: 28.5%
• Prior HF hosp: 71.5%
Spiro Placebo Hazard Ratio P-value
Enrolled by:
event rate event rate (95% CI)
Natriuretic 15.9% 23.6% 0.65 (0.49-0.87) 0.003
peptide
Heart Failure 19.6% 19.1% 1.01 (0.84-1.21) 0.923
Hosp
*P=0.013 for interaction
Pfeffer, TOPCAT NEJM 2013
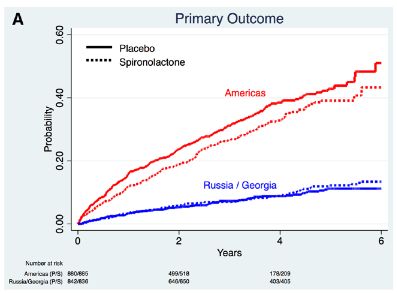
www.ccs.ca Heart Failure GuidelinesTOPCAT: Placebo Event Rates
Placebo:
280/881 (31.8%)
US, Canada,
Argentina, Brazil
12.6 per 100 pt-yr
Russia, Rep Georgia
Placebo:
71/842 (8.4%)
2.3 per 100 pt-yr
Pfeffer, TOPCAT NEJM 2013
www.ccs.ca Heart Failure GuidelinesGeographical Variation in
Baseline Characteristics
TOPCAT Americas Russia/Georg
N=3445 N= 1767 N=1678
Age, median (IQR), years 67 (61,76) 72(64,79) 66(59,71)*
Female, % 52 50 53*
Ejection Fraction, median, % 56 58 55*
Diabetes, % 33 45 20*
Atrial Fibrillation, % 35 42 28*
eGFR, median, IQR 65 (54,79) 61(49,77) 69(58,81)*
Enrollment Stratum, %
Hosp. for HF 72 55 89*
Natriuretic Peptide 29 45 11*
Medications, %
ACE-I or ARB 84 79 90*
Beta-blocker 78 79 77
Diuretic 81 89 74*
Pfeffer, TOPCAT
Circ HF 2015
www.ccs.ca Heart Failure GuidelinesTOPCAT: Regional Outcomes
Pfeffer, TOPCAT
Circ HF 2015
www.ccs.ca Heart Failure GuidelinesTOPCAT: Taking into Account
Regional Differences
• Fully adjusted model for primary endpoint including region
and other variables:
– HR 0.85, 95%CI 0.73 to 0.99, p=0.043
– “15% relative risk reduction for the primary endpoint in favor of
spironolactone”
Pfeffer, TOPCAT NEJM 2013
www.ccs.ca Heart Failure GuidelinesTOPCAT: Safety
• Doubling in the rate of hyperkalemia:
• 9.1% in the placebo group
• 18.7% in the spironolactone group
• No deaths due to hyperkalemia
• Fewer events of hypokalemia
• No renal failure leading to dialysis
• CCS HF Guidelines currently recommend monitoring Cr
and K after initiating MRA:
– 1 week
– 4 weeks
– 4 months
www.ccs.ca Heart Failure GuidelinesHF-PEF Recommendation Recommendation We suggest that in individuals with HFpEF, an elevated natriuretic peptide level, serum potassium < 5.0 mmol/L and an eGFR ≥30 ml/min, a mineralocorticoid receptor antagonist like spironolactone should be considered, with close surveillance of serum potassium and creatinine. (Weak Recommendation, Low Quality of Evidence). Values and Preferences: This recommendation is based upon a pre-specified subgroup analysis of the TOPCAT trial, which includes analysis of the pre-defined outcomes according to admission NT-BNP level, as well as the corroborating portion of the trial conducted within North and South America. www.ccs.ca Heart Failure Guidelines
Back to Mrs. PEF – Case Resolution
• What would you do next?
C) Initiate spironolactone 12.5 mg po OD with follow-up
electrolytes
www.ccs.ca Heart Failure GuidelinesAnemia www.ccs.ca Heart Failure Guidelines
Definition
• Anemia
– Definition OMS HB< 130 g/dL for men and 120 g/dL for women
– Other definitions exist (age, condition)
– Moreover, no specific definition for heart failure
www.ccs.ca Heart Failure GuidelinesPrevalence
• The prevalence of anemia varies between 10 and 49%
• A meta-analysis of 153,180 pts shows a prevalence of 34%
• Variability is related to:
– Definition
– M/W ratio
– Age
– IRC
– NYHA classification
• Pseudoanemia (dilution)
• Importance of re-testing
• Up to 20% of normal patients will become anemic within 6
months
www.ccs.ca Heart Failure GuidelinesPathophysiology of Anemia in HF
↓ Cardiac output
↓ Renal perfusion
Activation RAAS Pro inflammatory Cytokines CKD
Volume overload ACEi / ARB ↓ EPO secretion
Hemodilution ↓ Bone marrow (response)
↓ Production
Anemia
Canadian Journal of Cardiology 2015 31, 3-16DOI: (10.1016/j.cjca.2014.10.022)
www.ccs.ca Heart Failure GuidelinesTreatment of anemia in HF Recommendation We suggest that for patients with documented iron deficiency, oral or intravenous iron supplement be initiated to improve functional capacity (Weak Recommendation, Low-Quality Evidence). We recommend erythropoiesis stimulating agents not be routinely used to treat anemia in HF (Strong Recommendation, High-Quality Evidence). www.ccs.ca Heart Failure Guidelines
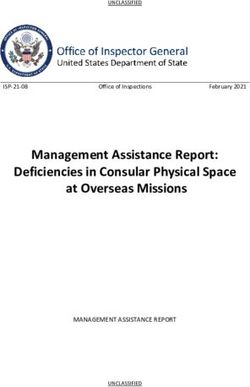
Patient Reported Outcomes
6MWT
Fatigue
KCCQ
EQ5D
Piotr Ponikowski et al. Eur Heart J 2014;
eurheartj.ehu385
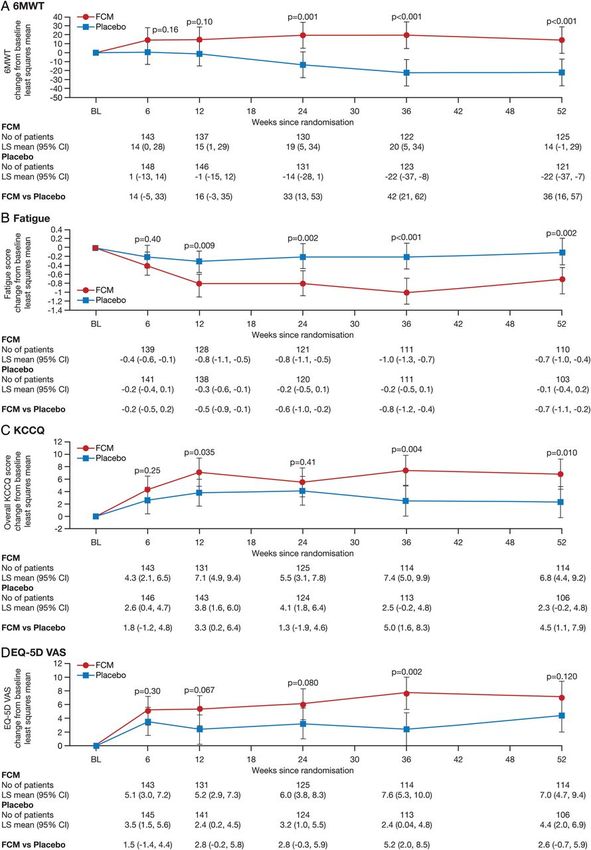
www.ccs.ca Heart Failure GuidelinesBeneficial effects of long-term intravenous iron
therapy with ferric carboxymaltose in patients
with symptomatic HF and iron deficiency
• Significant improvement
– 6MWT
– Fatigue
– Hospitalization
• Iron 10/150
• Placebo 32/151
– p=0.009
www.ccs.ca Heart Failure GuidelinesTime to first hospitalization
Piotr Ponikowski et al. Eur Heart J 2014;eurheartj.ehu385
www.ccs.ca Heart Failure GuidelinesAnemia
Values and Preferences:
The iron supplement recommendation was derived mostly from the
experience of clinicians, small clinical trials, and 2 large randomized
controlled trials (RCTs).
The recommendations against the use of erythropoiesis-stimulating
agents (ESAs) were derived from robust data from RCTs.
Practical Tip:
• Patients with severe chronic kidney disease and anemia should be
referred to a nephrologist to seek the optimal therapy for anemia.
• Symptomatic patients with low transferrin and/or ferritin levels
should be considered for supplementary iron therapy principally
with a goal of improving symptoms
www.ccs.ca Heart Failure GuidelinesAnemia Case
• 74 year old male Medications
– Known HF x 4 years • ASA 81 mg
– Ischemic etiology: 4vCABG
• Carvedilol 25 mg BID
1998
– Ejection fraction 36%, mild • Spironolactone 25 mg
MR • Enalapril 10 mg BID
– NYHA 2-3 [mostly 3]
– no recent admissions
www.ccs.ca Heart Failure GuidelinesAnemia Case
Physical Exam Investigations
• Vitals • Creatinine 124 umol/L
– BP 106/74, HR 60 – GFR = 49
– RR 14, O2sat 95% • K 4.9, Na 136
• CV: S1S2, soft MR • CBC:
murmur, JVP 3 cm ASA – Hb 122 g/L
• Chest: CTA – MCV 80 (L)
• Abdomen: no ascites – RDW 16.1% (H)
– Platelet 194
• No LEE
– WBC 7.2
www.ccs.ca Heart Failure GuidelinesAnemia Case – Question
What work-up should be considered?
1. GI blood loss
2. Nutritional deficiency
3. Hemolysis
4. Malaria
5. All of the above
0% 0% 0% 0% 0%
is
ss
ia
e
cy
ys
ov
ar
lo
en
ol
al
ab
od
ic i
m
M
lo
he
He
ef
b
ld
ft
GI
lo
na
Al
t io
tri
Nu
www.ccs.ca Heart Failure GuidelinesAnemia Case • You ask some f/u questions (all negative) • No recent travel • Dietician reviews, no MAJOR deficiencies • No obvious GI source by history Need to decide: • More work-up: yes or no? www.ccs.ca Heart Failure Guidelines
Anemia Case – Question
What labs should I send?
1. Ferritin, TIBC, iron
saturation
2. B12/folate
3. TSH
4. LDH, bilirubin,
reticulocytes
5. Thick/thin film for malaria 0% 0% 0% 0% 0%
H
e
s
r ia
.
at
TS
te
r. .
l
ala
cy
fo
tu
lo
2/
sa
rm
ic u
B1
n
fo
ro
et
m
i
r
C,
n,
fil
B
bi
n
TI
ru
hi
n,
/t
li
iti
bi
ick
rr
H,
Th
Fe
www.ccs.ca Heart Failure Guidelines LDAnemia Case
• Ferritin 40 [L, 12-300 ug/L]
• TIBC 46 [N, 40-80 umol/L]
• Iron saturation 13% [L, 20-50 %]
• GI consult:
• FIT test negative (or for rest of Canada: Colonoscopy
negative)
www.ccs.ca Heart Failure GuidelinesAnemia Case
• Decide its iron-deficiency anemia
• Options for Rx:
– Oral iron
– IV iron
– Nutritional improvement
• Patient did not previously tolerate oral iron
• Dietician says that other than moving to Alberta, cannot
add more iron to diet
www.ccs.ca Heart Failure GuidelinesAnemia Case Resolution
• Patient seen over next 6 months:
• IV iron sucrose x 3 doses, total = 900 mg
• Ferritin 40 231
• Iron sat 13%29%
• Hb 122138
• NYHA 2-32
• Feels can golf 18 holes (previously 9)
www.ccs.ca Heart Failure GuidelinesNatriuretic Peptides www.ccs.ca Heart Failure Guidelines
Optimal Use of Biomarkers
• Costs associated with HF diagnostic and therapeutic
strategies continue to rise
• Establishing diagnosis and selecting optimal therapy for
any given patient are current challenges
• Biomarkers may help stratify risk and individualize
therapy
• This update will review the role of circulating biomarkers for
the management of patients with HF with a focus on its
role in the monitoring for disease progression
www.ccs.ca Heart Failure GuidelinesB-type Natriuretic Peptides Increased myocardial wall stress due to volume or pressure overload activates the B-type natriuretic peptide (BNP) gene in cardiac myocytes, producing the intracellular precursor propeptide (proBNP) Cleavage releases the biologically active BNP and biologically inert amino-terminal fragment (NT-proBNP). BNP stimulates natriuresis and vasodilation ⇒ Afterload reduction ⇒ Inhibits renin-angiotensin-aldosterone release and sympathetic nervous activity ⇒ Reduces fibrosis. www.ccs.ca Heart Failure Guidelines
Optimal Use of Biomarkers • ER or primary use of NPs for Diagnosis Established Recommendation We recommend that B-type NP (BNP)/amino-terminal frament of propeptide BNP (NT-proBNP) levels be measured to help confirm or rule out a diagnosis of heart failure in the acute or ambulatory care setting in patients in whom the clinical diagnosis is in doubt (Strong Recommendation, High-Quality Evidence). Values and Preferences: These recommendations remain unchanged from previous CCS HF guidelines. www.ccs.ca Heart Failure Guidelines
Natriuretic Peptides for HF Diagnosis
Table 2. Natriuretic peptides cut points for the diagnosis of heart failure
Age (years) HF is unlikely HF is possible but HF is very likely
other diagnoses
need to be
considered
BNP All < 100 pg/ml 100-500 pg/ml > 500 pg/ml
NT-proBNP < 50 < 300 pg/ml 300-450 pg/ml > 450 pg/ml
50 - 75 < 300 pg/ml 450-900 pg/ml > 900 pg/ml
> 75 < 300 pg/ml 900 - 1800 pg/ml > 1800 pg/ml
HF, heart failure
www.ccs.ca Heart Failure GuidelinesThe Troubling Case of Mr. B
• Mr. B. is 70 y.o. and comes in your office in May 2012 for his follow-up
(q 4 months). He lives 7 hours from your hospital and is followed by his
GP and you, his cardiologist, for HF due to ischemic cardiomyopathy.
The last echo (4 months) showed and EF of 25%, severe functional
MR, Mild RV dysfunction, moderate to severe TR, PAPs 55mmHg
• He still smokes 10 cigarettes/day, has COPD, respects his water and
salt intake limits and takes his medications
• He has had prior myocardial infarctions and coronary bypasses in
2001, has no ischemia but a large scar on his nuclear scan done 4
months ago. His ICD was implanted in primary prevention in 2005, he
had a narrow QRS. He never had ICD therapies.
www.ccs.ca Heart Failure GuidelinesThe Troubling Case of Mr. B
• Current medications: ASA 80mg qd, Bisoprolol 10mg qd, Candesartan
16mg bid, Spironolactone 25mg qd, Furosemide 80mg bid
• Mr. B’s NYHA class often varies between 2 and 3. Today he reports
being more short of breath (definitely NYHA 3) for about 6 weeks but
he is stressed with financial and family issues. He seems depressed
and worried
• He did not cough more than usual and did not have fever
• On physical examination: well perfused, very thin, pulse 60 (NSR), BP
95/55mmHg (usual), JVP 12 (V wave nadir), S3+, holosystolic apical
murmur 3/6, clear lungs, mild peripheral oedema. ECG: SR, right
ventricular pacing
• His last labs were done with his GP 3 weeks ago and showed stable
Hb 125g/L and creatinine 120umol/L, K 4.0
www.ccs.ca Heart Failure GuidelinesWhat would you do?
A. Increase furosemide to 120mg
bid and see him next time (4-6
weeks)
B. Ask for NP levels today at your
hospital and then decide what to
do
C. Add digitalis to his therapy
D. Refer him for Mitra-Clip 0% 0% 0% 0% 0%
evaluation
e
y
..
E. All of the above
ov
.. .
...
ap
y
ab
da
ip
to
er
Cl
th
to
he
e
a-
id
is
ls
ft
itr
em
h
ve
lo
rM
to
le
Note: There is no HF clinic close to where os
Al
is
ur
NP
fo
al
ef
im
git
he lives and his GP (or you) is able to see or
as
rh
di
kf
re
d
As
fe
c
Ad
In
Re
him every 4-6 weeks
www.ccs.ca Heart Failure GuidelinesWhat we did:
Current NT-proBNP level =7500
Prior (2 months ago)NT-proBNP level = 3700
Creatinine =142 umoL/L
In clinic we:
– increase his diuretics
– added digitalis
– reevaluated all potential means of improving his outcome
www.ccs.ca Heart Failure GuidelinesNew Recommendations Recommendation 2. We recommend measurement of BNP/NT-proBNP levels be considered in patients with an established diagnosis of heart failure for prognostic stratification (Strong Recommendation, High-Quality Evidence). 3. We suggest, in ambulatory patients with heart failure due to systolic dysfunction, measurement of BNP or NT-proBNP to guide management should be considered to decrease heart failure- related hospitalizations and potentially reduce mortality. The benefit is uncertain in individuals older than 75 years of age (Weak Recommendation, Moderate-Quality Evidence). www.ccs.ca Heart Failure Guidelines
New Values and Preferences Values and Preferences: These recommendations are based on multiple small randomized controlled trials, most of which demonstrated benefit, and 3 meta- analyses, which universally demonstrated benefit. It is realized that there is still a large randomized controlled trial ongoing that may modify the conclusions. www.ccs.ca Heart Failure Guidelines
Evidence for NP-Guided Therapy • In the available trials, 3 systematic reviews and meta-analyses (Figures) synthesizing the RCT results, NP-guided therapy has been shown to improve survival and reduce hospitalizations • In these studies, NP-guided therapy had no benefits in 2 subgroups: age >75 years and those with HFpEF • Consequently, a larger multicenter trial of a single-target NP level (NT- proBNP 1000 pg/ml) and the use of guideline-approved therapies in both treatment arms is now underway, the Guiding Evidence Based Therapy Using Biomarker Intensified Treatment (GUIDE-IT, NCT01685840) • The ongoing single-centre EX-IMPROVE-CHF, NCT00601679) will also help clarify the role of NP-guided therapy in HF management www.ccs.ca Heart Failure Guidelines
Effect of NP-guided management on mortality:
hazard ratios from meta-analysis
www.ccs.ca Heart Failure GuidelinesEffect of NP-guided management on HF
hospitalizations: HRs from meta-analysis
www.ccs.ca Heart Failure GuidelinesWhat’s A Significant Change in NP
Level?
• A change of 30% in NP level likely exceeds the day to day variation
and is in general considered relevant.
• For ambulatory patients with HF evaluated in the clinic, a NP level that
increases more than 30% should therefore call for more intensive follow
up and/or intensified medical treatments, even if they are not congested
clinically.
• The latter can include diuretic therapy or intensification of ACE
inhibitors, β-blockers and mineralocorticoid receptor antagonists if their
doses are not yet at the targets defined by clinical trials.
www.ccs.ca Heart Failure GuidelinesPre-Discharge NP Levels
• Besides predicting prognosis of patients in general, BNP
level obtained pre-discharge has been associated with
mortality and rehospitalization.
• Indeed, predischarge NP in conjunction with change in NP
has now been incorporated into a risk score for death and
readmission of HF in patients admitted with HF.
Salah K, Kok WE, Eurlings LW et al. ELAN-HF Score. Heart 2014;100(2):115-125
www.ccs.ca Heart Failure GuidelinesPre-Discharge NP Levels Recommendation 4. We suggest that measurement of BNP or NT-proBNP in patients hospitalized for heart failure should be considered before discharge, because of the prognostic value of these biomarkers in predicting rehospitalization and mortality (Strong Recommendation, Moderate- Quality Evidence). Values and Preferences: This recommendation is based on multiple small randomized controlled trials, all of which demonstrated an association with clinical outcomes. Although the risk of readmission is decreased with lower natriuretic peptide levels, clinicians should also consider the limitations of delaying discharge from hospital for this purpose. www.ccs.ca Heart Failure Guidelines
Other biomarkers ready for clinic?
Biomarkers Pathophysiological HF populations Advantages Potential benefits Challenges before
pathways / comorbid targeted implementation
conditions with
prognostic implications
NGAL Renal Function Acute HF Early detection of renal Adjusting therapy to Unclear if using NGAL
function deterioration improve prognosis by in acute HF to modify
avoiding acute renal therapies improves
failure progression clinical outcomes
Cystatin C Renal Function Acute and chronic More sensitive Same as above Unclear if using
HF detection of changes in Cystatin C, over using
renal function eGFR, to modify clinical
management provides
further clinical benefit
Cardiac hs- Myocyte death Acute and Very sensitive marker Optimization of therapy Prognostication
troponins Chronic HF predicting higher risk of in patients with elevated improves only for
CV events regardless of hs-cTn should be more mortality and use to
etiology aggressive modify therapy has
not been tested
ST2 Fibrosis / inflammation / Acute and chronic Additional prognostic Could provide additional Unclear if using ST2 in
immunity HFrEF, HFpEF value beyond NPs value for short and long acute HF to modify
and previously suspected term prognostication, therapies improves
low EF recovered Low week-to-week regardless of LVEF clinical outcomes;
variations
Galectin-3 Cardiac and vascular Incident HF, Early detection of risk Preventive measures Recent study showed
fibrosis HFrEEF and and long term and therapy ST2 superior to
HFpEF prognostication in HF optimization based on Galectin-3 in a
levels could improve multivariable prediction
outcomes model
www.ccs.ca Heart Failure GuidelinesLCZ www.ccs.ca Heart Failure Guidelines
LCZ Case
• 71 year old female Medications
• Non-ischemic etiology • Bisoprolol 7.5 mg
– HTN • Spironolactone 12.5 mg
– DM
• Perindopril 4 mg
– Afib
• Lasix 40 mg BID
• NYHA 3
• Apixaban 5 mg BID
• EF 29%
• Diabetes meds
• One episode requiring
dayward IV lasix 10 months
ago • [prior attempts to increase
have not been effective]
www.ccs.ca Heart Failure GuidelinesLCZ Case
Physical Exam Investigations
• Vitals • Creatinine 132umol/L
– BP 98/74, HR 58 – GFR = 35
– RR 14, O2sat 96% • K 4.9, Na 134
• CV: S1S2, MR murmur • Hb 128 g/L
• JVP 4 cm ASA • ECG: AF, QRS 118 msec
• Chest: CTA
• Abdomen: no ascites
• No LEE
www.ccs.ca Heart Failure GuidelinesLCZ Case – Question
What changes should be considered?
1. Increase Bisoprolol to 10 mg
2. Cardiac rehabilitation
3. Increase spironolactone to
25 mg
4. Increase perindopril to 8 mg
5. Other
0% 0% 0% 0% 0% 0%
6. No change
r
ge
g
g
n
he
..
m
m
tio
an
Ot
ne
10
8
ta
ch
to
to
ili
to
No
ac
b
il
ol
ha
pr
ol
ol
do
n
re
ir o
pr
rin
ac
iso
sp
di
pe
eB
e
r
Ca
as
se
as
re
ea
re
c
cr
In
c
In
In
www.ccs.ca Heart Failure GuidelinesLCZ Case
• Patient’s daughter asks:
– “How long will she live? Can anything else be done?”
• Patient asks:
– “Can I travel to Palm Springs?”
• Calculated SHFM score = 90% survival x 1 year
• You increase the spironolactone to 25 mg
• Well tolerated, SBP 98, cr 134, K 4.9
• Returns from Palm Springs
• Fluctuates NYHA 2-3
Now what?
www.ccs.ca Heart Failure GuidelinesLCZ Case – Question
What changes should be considered?
1. Increase Bisoprolol to 10 mg
2. Cardiac rehabilitation
3. Switch perindopril to LCZ696
4. Other
5. No change
0% 0% 0% 0% 0%
r
ge
g
n
he
m
tio
...
an
Ot
10
LC
ta
ch
li
to
to
No
bi
ol
ha
il
pr
ol
re
do
pr
ac
rin
iso
di
pe
eB
r
Ca
h
as
itc
re
Sw
c
In
www.ccs.ca Heart Failure GuidelinesHF – Reduced Ejection Fraction
• Current GDMT (ACE or ARB, BB and MRA) reduces the
risk of mortality, hospitalization and improves quality of life
• Multiple, adequately powered RCT
• Residual risk despite GDMT
www.ccs.ca Heart Failure GuidelinesHF-REF: The R is for Risk
Annualized mortality rate:
NYHA 2* = 7%
Outpatient HF in Alberta = 7.5%
CHFN -2009 = 15%
SHFM ‘average’ Alberta HF patient:
• On ACE/BB/MRA = 5%
• Not ACE/BB/MRA = 14%
www.ccs.ca Heart Failure GuidelinesOther RAS Blockers
• RAS blockade:
– Renin inhibitors: No additional benefit
– Omapatrilat:
• IMPRESS: n=573 pts, 12 weeks
– omapatrilat fewer events than lisinopril
• OVERTURE: enalapril and omapatrilat similar event
rate
– Angioedema signal: 2.1% in black, 0.5% in non-black patients
– Other agents on cutting room floor: samipatrilat, gemopatrilat, MDL-
100240, fasidotril, z-13752a
IMPRESS, Lancet 2000
OVERTURE, circ 2002
www.ccs.ca Heart Failure GuidelinesNEP and NEP Inhibition
Relative ANP and CNP NEPi by itself:
affinity Angiotensin-2
for NEP Ang II
ET-1
Ang I
Bradykinin
Adrenomedullin
NEP cGMP
Substance P
Sodium excretion
Bradykinin Inactive
fragments
Endothelin or metabolites Fibrosis
BNP LVH
Fryer BJP 2008 153
www.ccs.ca Heart Failure GuidelinesSeriously, I just learned about BNP and now there
are other letters of the alphabet soup of NPs that
are important?
Cardiomyocytes1 Endothelial cells1
ANP and BNP
CNP
NPR-A NPR-B NPR-C
GTP GTP Receptor
cGMP cGMP
recycling
Internalization
• Vasodilation1,2 • Vasodilation1,2 Degradation
• Antihypertrophy1,2 • Antihypertrophy1,2 of NPs1,2,5
• Antiproliferation2 • Antiproliferation2
• Vascular regeneration1 • Vascular regeneration1
• Myocardial relaxation1 • Venodilation1
• Diuresis, natriuresis1,2 • Antifibrosis1
• Antiapoptosis1
• Anti-aldosterone1,2
• Renin secretion inhibition1,3 1. Mangiafico et al. Eur Heart J 2013;34:886–93;
• Reduced sympathetic tone4 2. Gardner et al. Hypertension 2007;49:419–26;
• Lipolysis1 3. Pandey. J Am Soc Hypertens 2008;2:210–26;
4. Levin et al. NEngl J Med1998;339;321–8;
5. Von Lueder et al. Pharmacol Ther 2014 [Epub ahead of print]
www.ccs.ca Heart Failure GuidelinesLCZ696
Vardeny CPT 2013
www.ccs.ca Heart Failure GuidelinesPARADIGM – HF
• International, multi-center, double-blind, placebo-controlled
RCT
• Randomization, 1:1
– LCZ696 200 mg BID
– Enalapril 10 mg BID
• Primary: composite of CV death from or hospitalization for
HF
McMurray NEJM 2014
www.ccs.ca Heart Failure GuidelinesPARADIGM-HF: Eligibility Criteria
Inclusion: Inclusion (cont)
• NYHA II-IV HF • Any ACEi or ARB, but
able to tolerate stable
• LVEF ≤40 % [≤35% dose equivalent to at
amend] least enalapril 10 mg
• Elevated NPs daily for at least 4 weeks
– BNP ≥150 pg/mL
– NT-proBNP ≥600 pg/mL Major Exclusion:
• Guideline-recommended • SBP < 95 mmHg
use of beta-blockers and • eGFR 5.4 mEq/L
McMurray NEJM 2014
www.ccs.ca Heart Failure GuidelinesPRADIGM-HF: Prior ACE / ARB Dose
16.4 20
67.1
18.2
60.1
5.9 181.5
7.0
www.ccs.ca Heart Failure GuidelinesPARADIGM-HF: Design
Single-blind run-in period Double-blind period
LCZ696 200 mg BID
Enalapril LCZ696
Rand’n
10 mg 100 mg 200 mg
BID BID BID
Enalapril 10 mg BID
2 weeks 1-2 weeks 2-4 weeks
N=1102 N=977 N=8399 patients
McMurray NEJM 2014
www.ccs.ca Heart Failure GuidelinesPARADIGM-HF: Baseline Characteristics
LCZ696 Enalapril
(n=4187) (n=4212)
Age (years) 63.8 ± 11.5 63.8 ± 11.3
Women (%) 21.0% 22.6%
Ischemic cardiomyopathy (%) 59.9% 60.1%
LV ejection fraction (%) 29.6 ± 6.1 29.4 ± 6.3
NYHA functional class II / III (%) 71.6% / 23.1% 69.4% / 24.9%
Systolic blood pressure (mm Hg) 122 ± 15 121 ± 15
Heart rate (beats/min) 72 ± 12 73 ± 12
N-terminal pro-BNP (pg/ml) 1631 (885-3154) 1594 (886-3305)
B-type natriuretic peptide (pg/ml) 255 (155-474) 251 (153-465)
History of diabetes 35% 35%
Beta-adrenergic blockers 93.1% 92.9%
Mineralocorticoid antagonists 54.2% 57.0%
ICD and/or CRT 16.5% 16.3%
McMurray NEJM 2014
www.ccs.ca Heart Failure GuidelinesPARADIGM-HF: Primary Endpoint
4
0
Enalapril 1117
Kaplan-Meier Estimate
Cumulative Rates (%)
3
(n=4212) 914
2
2
4 LCZ696
of
1
(n=4187)
6
8 HR = 0.80 (0.73-0.87)
P = 0.0000002
Number needed to treat = 21
0
0 180 360 540 720 900 1080 1260
Patients at Risk Days After Randomization
LCZ696 4187 3922 3663 3018 2257 1544 896 249
Enalapril 4212 3883 3579 2922 2123 1488 853 236
Primary = CV death or HF Hospitalization
McMurray NEJM 2014
www.ccs.ca Heart Failure GuidelinesPARADIGM-HF: CV Death
32
Enalapril
Kaplan-Meier Estimate of
Cumulative Rates (%)
24 HR = 0.80 (0.71-0.89) (n=4212) 693
P = 0.00004
Number need to treat = 32 558
16
LCZ696
8
(n=4187)
0
0 180 360 540 720 900 1080 1260
Patients at Risk Days After Randomization
LCZ696 4187 4056 3891 3282 2478 1716 1005 280
Enalapril 4212 4051 3860 3231 2410 1726 994 279
McMurray NEJM 2014
www.ccs.ca Heart Failure GuidelinesPARADIGM-HF: All Cause Mortality
32
Enalapril
HR = 0.84 (0.76-0.93)
(n=4212) 835
PPARADIGM-HF: Endpoints
Hazard
LCZ696 Enalapril P
Ratio
(n=4187) (n=4212) Value
(95% CI)
Primary 914 1117 0.80
0.0000002
endpoint (21.8%) (26.5%) (0.73-0.87)
Cardiovascular 558 693 0.80
0.00004
death (13.3%) (16.5%) (0.71-0.89)
Hospitalization 537 658 0.79
0.00004
for heart failure (12.8%) (15.6%) (0.71- 0.89)
McMurray NEJM 2014
www.ccs.ca Heart Failure GuidelinesPARADIGM-HF: Safety Endpoints
LCZ696 Enalapril P
(n=4187) (n=4212) Value
Prospectively identified adverse events
Symptomatic hypotension 588 388 < 0.001
Serum potassium > 6.0 mmol/l 181 236 0.007
Serum creatinine ≥ 2.5 mg/dl 139 188 0.007
Cough 474 601 < 0.001
Discontinuation for adverse event 449 516 0.02
Discontinuation for hypotension 36 29 NS
Discontinuation for hyperkalemia 11 15 NS
Discontinuation for renal impairment 29 59 0.001
Angioedema (adjudicated)
Medications, no hospitalization 16 9 NS
Hospitalized; no airway compromise 3 1 NS
Airway compromise 0 0 ----
McMurray NEJM 2014
www.ccs.ca Heart Failure GuidelinesPARADIGM-HF: Sec. Analyses
• Reduction in SCD by 20%
• Will this reduce need for referral for ICD?
• Reduction in repeat ED, repeat hosps and ICU days and
visits
• Will this drive the cost-effectiveness?
• Improved NYHA class
• Less decline in QOL (by KCCQ @ 8 months)
• Will this be the key for patients?
Packer, Circulation 2015
www.ccs.ca Heart Failure GuidelinesIs 1 trial enough?
0.00008
0.0000004
Based on formula (0.025)n x2 (personal communication Stuart Pocock)
Slide courtesy of J McMurray
www.ccs.ca Heart Failure GuidelinesHF – Reduced Ejection Fraction
Recommendation
We recommend that in patients with mild to moderate HF, an EF < 40%, an
elevated NP level or hospitalization for HF in the past 12 months, a serum
potassium < 5.2 mmol/L and an eGFR ≥ 30 mL/min and treated with appropriate
doses of guideline-directed medical therapy should be treated with LCZ696 in
place of an ACE inhibitor or an angiotensin receptor blocker, with close
surveillance of serum potassium and creatinine (Conditional Recommendation,
High-Quality Evidence).
Values and Preferences:
This recommendation places high value on medications proven in large trials to
reduce mortality, HF rehospitalization, and symptoms. It also considers the
health economic implications of new medications. The recommendation is
conditional because the drug is not yet approved for clinical use in Canada and
the price is still not known.
CCS HF Guidelines, Moe, Ezekowitz, et al CJC 2014
www.ccs.ca Heart Failure GuidelinesThe Anatomy of a Recommendation NPs mostly not available in Canada as EF < 40% until amendment outpt; no interaction of either of these to
LCZ Case – Question
What if the patient was 83 years old?
1. Same decision
2. Difference decision
0% 0%
on
n
io
i
cis
cis
de
de
e
e
m
nc
Sa
re
ffe
Di
www.ccs.ca Heart Failure GuidelinesLCZ Case Resolution
• You await new medication to come to Canada
• When it does, you discuss risk/benefit/cost with patient
• They ask:
– “Is it better than my current drug?”
– “Is it as safe, since I have not had trouble before?”
– “Will I be able to travel?”
– “If this was a relative (that you liked), what would you
recommend?”
• Shared-decision making requires evidence to share with
patient and for patient to interact.
www.ccs.ca Heart Failure GuidelinesQuestions? www.ccs.ca Heart Failure Guidelines
Looking for best practices in heart
failure diagnosis and management?
To access this tool, and to view all of our guideline
resources, please visit www.ccs.ca.
www.ccs.ca Heart Failure GuidelinesYou can also read