Changing Nappies / Changing Lives: Adjusting to Parenting Your New Baby - An Evaluation
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Changing Nappies / Changing Lives:
Adjusting to Parenting Your New Baby
An Evaluation
Evaluation of the
‘Changing Nappies / Changing Lives: Adjusting to
Parenting Your New Baby’ group
for new parents experiencing adjustment issues
with their babies in the first year of parenting
Jarrod Turner Regina Fogarty
Hey Dad WA, Ngala Parent Education, Ngala
This project was partly funded by the WA Perinatal Mental Health Unit,
Women and Newborn Health Service and Ngala. Some materials used were
provided by the WA Perinatal Mental Health Unit and beyondblue Australia.
Page | 1Summary Having a new baby is a major change for most parents. Many will struggle with the adjustment to parenting. Rates of depression and anxiety rise in the perinatal period for both males and females. This is a community-wide concern because poor mental health and wellbeing in parents can endure if ignored and can determine mental health outcomes for their children well into the future. This report describes the piloting of a community-based workshop that was aimed at helping parents adjust to parenting and improve their mental health and wellbeing. Overall, the participants had elevated levels of depression symptoms pre-workshop, higher in the males. Participants also rated themselves as potentially low in parenting confidence, especially the males. At four week follow-up there was an overall increase in parenting confidence across the participants, most notable for females; and there was an overall decrease in depression ratings across participants, clinically significant for males. Satisfaction ratings for different elements of the workshop were moderate to high. This piloted workshop provides an effective model for future community efforts to meet the needs of parents as they adjust to parenting in the first year. Introduction It is commonly accepted that having a baby is a significant transitional event, especially for women and men who are experiencing their first child. The birth of the child can lead to significant changes in possibly all of the significant life domains including but not limited to relationships, work and finances, health, housing, recreation, and the parents’ overall mental health and wellbeing. In Australia, it is estimated that approximately 16% of women experience depression in the 12-month period following birth (postnatal; Buist & Bilszta, 2006; Yelland, Sutherland, & Brown, 2010). The incidence of paternal depression in the first year following child birth may be as high as fifty percent among men whose partners were experiencing postnatal depression (Goodman, 2004). These rates are higher than for the general Australian adult population. For example, the general 12-month prevalence rates for depression in women and men are 5.1% and 3.1% respectively (Australian Bureau of Statistics, 2008). Further, the incidence of maternal anxiety in the postnatal period is Page | 2
estimated to be around 10% (Woolhouse, Brown, Krastev, Perlen, & Gunn, 2009; Yelland et al., 2010). Nearly forty percent of women with major depression in this period may experience a co-occurring anxiety-related disorder (Austin, Hadzi-Pavlovic, Priest, Reilly, Wilhelm et al., 2010). Therefore, there is an increased risk for depression and related disorders among new parents in the first twelve months following the birth of their child. Studies and clinical experiences have shown that poor mental health and wellbeing among parents can impair their adjustment to parenting in the postnatal period, and poor adjustment to early parenting can contribute to deterioration in parental mental health (National Research Council and Institute of Medicine, 2009). Child mental health also can be affected due to the parenting practices of the parent with depression. For example, Lovejoy, Gracyk, O’Hare, and Neuman (2000) found that the presence of maternal depression symptoms was associated with (maternal) hostile and negative parenting (e.g., coercive practices), disengaged parenting (e.g., ignoring), and decreased positive parenting practices (e.g., engaging with less affection). In terms of infant mental health, high levels of depressive symptoms tend to be associated with less maternal responsiveness and sensitivity, less verbal and visual engagement with the infant, and more intrusiveness (NRCIM, 2009). Therefore, in line with parent-child attachment models and clinical studies (e.g., Bowlby, 1988), there is the potential for a detrimental effect on the parent’s ability for the establishment of a positive social and emotional connection with the infant. Further, exposure to the types of negative parenting behaviours outlined above can represent a chronically stressful environment for the infant, leading to poor mental health outcomes. For example, infants of mothers with depression symptoms are considered to have more ‘difficult’ temperaments, are more bothersome, and are rated as being more difficult to care for than infants of mothers without depressive symptoms (Whiffen & Gotlib, 1989). These infants tend to show more negative affect (e.g., crying, fussing) and less seeking of emotional support from their parents at critical times (Field, 1992; Tronick & Gianino, 1986). Further, there has been a suggestion that there may be increased stress responses from infants in their underlying psychobiological systems with elevated autonomic activity (e.g., higher heart rate, increased respiration) and increased stress hormonal levels (e.g., cortisol) in response to the parenting behaviours associated with parental depression (Field, 1992). Page | 3
There is an obvious community-wide need for early intervention services for women, men and their families struggling during the perinatal period. Access to, and the effective provision of, focused services that provide support, education, and helpful techniques to assist parents in the perinatal period has been identified as a clear priority in Australia. Attention also has been given to potential barriers to services for mothers, including costs, childcare arrangements, and long waiting times (Beyondblue, 2011). Fathers might be unintentionally marginalised from services that lack well formed father-inclusive practices (Fletcher, Matthey, & Marley, 2006). This evaluation reports on the effectiveness of a pilot workshop, ‘Changing Nappies/Changing Lives: Adjusting to Parenting Your New Baby’ (CNCL), for parents who were experiencing adjustment issues within the first year of their child’s life. The workshop was designed and constructed based on the outcomes required for the project for the WA Perinatal Mental Health Unit. The workshop was also informed by contemporary understandings of adjustment to parenting and depression and related disorders (e.g., anxiety) within the perinatal period. The workshop was designed and piloted by the Hey Dad WA program at Ngala with support from Ngala’s Parent Education Services. Method Participants Eighteen parents agreed to attend the CNCL workshop, 10 females (m = 30.4 yrs) and 8 males (m = 33.75 yrs). The average age within the entire group was 32 years. Parents were recruited via an advertised flyer distributed through early parenting services, including Ngala, within the Perth metropolitan area. Procedure There were two identical workshops facilitated. Each was located in a comfortable, well- equipped (chairs, tables, kitchen, toilets, parking, crèche) community-based parenting centre in North and South regions of the Perth metropolitan area. Parents were selected for either workshop based on proximity to their home address. The workshops were facilitated in the evenings (6.00 to 8.30 pm) by a male Hey Dad WA staff member and a female Ngala Parent Education staff member. Each workshop was facilitated over two week-day evenings Page | 4
for a total of five hours (2.5 hrs per evening). Parents were required to attend both evenings. Upon arrival on the first evening, once informed consent was obtained, each participant was required to complete the Edinburgh Postnatal Depression Scale (EPDS; Cox, Holden, & Sagovsky, 1987) and the Karitane Parenting Confidence Scale (KPCS; Črnčec, Barnett, & Matthey, 2008). These instruments along with a specially constructed workshop evaluation and feedback questionnaire (Appendix A) were also completed by the participants at four weeks follow-up and returned by mail/email for inclusion in this report. Workshop Description The CNCL workshop was designed to provide participants with information, strategies, and support on 1) improving the adjustment to early parenting, 2) increasing confidence around day to day parenting, 3) identifying and meeting theirs’ and their infant’s social and emotional needs. The workshop also attempted to address mental health and wellbeing issues in the perinatal period. The workshop was comprised of two 2.5 hour interactive group presentations using Microsoft PowerPoint. The first evening’s content focused on the initial three aims outlined above. The second focused exclusively on perinatal mental health and wellbeing issues. The facilitators strictly adhered to the workshop protocol as outlined in the PowerPoint presentation. Materials were provided to participants including fact sheets, pamphlets, booklets, and other resources from the West Australian Perinatal Mental Health Unit beyondblue Australia, and Ngala (including Hey Dad WA). Overall, the workshop was informed by literature and guidelines consistent with best clinical practices within early parenting services and perinatal mental health services (e.g., beyondblue, 2011; Bowlby, 1988; Fletcher, 2011; Parker & Hunter, 2011). The approach taken was to present information and then to facilitate discussion in the form of questions, comments, and sharing of concerns from individual members of the group. The conversation could be directed either to the facilitators directly or through other group members (i.e., group discussion). Participants were provided with supplementary resources including a list of recommended community supports available to parents and writing materials for note taking. The use of a male and female facilitator was deliberate and aimed to provide an across-gender experience for the participants. Both facilitators were trained and experienced in father-inclusive practices (FaHCSIA, 2009) and in the delivery of education modules to new parents. Page | 5
Measurement The Edinburgh Postnatal Depression Scale (EPDS; Cox et al., 1987) is a 10-item self-report questionnaire designed to identify symptoms of depression in the perinatal period and is one of the most widely used measures of postnatal depression in clinical practice and research. The EPDS has strong, well-established psychometric properties (Cox et al., 1987, 1996; Leverton & Elliot, 2000). It has been used across clinical, non-clinical and community populations. Scores above nine are considered indicative of ‘possible depression’ with maximum sensitivity (‘probable depression’) occurring at scores of 12 or above. Others have suggested a score of seven or eight may be more appropriate to decrease the likelihood of false-negative results, with a male cut-off point two points lower due to males being less likely to endorse certain items (e.g., “I have been so unhappy that I have been crying”) compared to females (Matthey, Barnett, Kavanagh, & Howie, 2001). For the purposes of this evaluation, the authors have chosen to apply a clinical cut-off point of nine for female participants, and seven for males. The Karitane Parenting Confidence Scale (KPCS; Crncec et al., 2008) is a 15-item self-report questionnaire designed to measure parents’ subjective confidence in their parenting abilities, or ‘perceived parenting self-efficacy’. The KPCS was developed within the Australian context and is developed for use with mothers and fathers of infants aged 0 to 12 months. The KPCS has strong psychometric properties (see Crncec et al., 2008). To the best of our knowledge there has been no published evidence of any attempt to validate the scale exclusively among fathers. For the purposes of this evaluation, the authors have chosen to apply the recommended clinical cut-off point of 39 or less for both female and male participants (Crncec et al., 2008, p. 14). The Changing Nappies – Changing Lives Workshop Evaluation Form (CNCL-WEF; Appendix A) is an unpublished questionnaire developed by the authors. It utilises a subjective rating scale (1 = low satisfaction to 5 = high satisfaction) with the participants rating the completed CNCL workshop across a range of items (e.g., “How do you rate your satisfaction with this workshop?”). The CNCL-WEF also included items that required qualitative information from the respondents (e.g., “Which parts of the workshop were the most helpful?”). The questionnaire was based on typical workshop evaluation forms utilised within parent education services at Ngala. Page | 6
Results
10
9
8
7
6
5
4
3
2
1
0
Pre-Female F/Up Female Pre-Male F/Up Male
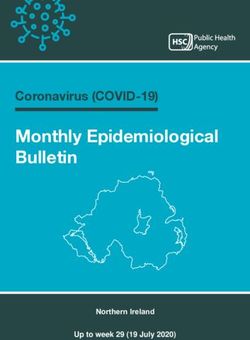
Figure 1: Participants’ EPDS mean scores at pre-workshop and four week follow-up. Note:
Female scores above nine = possible depression. Male scores above seven = possible
depression.
The participants’ pre-workshop and four week follow-up EPDS mean scores are presented in
Figure 1. Fifteen participants attended both evenings of the CNCL workshops and their data
were grouped for analysis. The pre-workshop data of the three non-completers (of the
original 18) were excluded from the analysis to preserve the integrity of the presented data.
The data in Figure 1 show a clinically significant difference between males and females such
that the male pre- scores, on average, exceeded the clinical-cut off point for ‘possible
depression’. The female scores were elevated yet, on average, within the non-clinical range.
Further analysis of individual scores revealed that pre-workshop 85.7% of male participants
exceeded the clinical cut-off point, compared to 25% of female participants. Overall, there
were reductions in average scores for both females and males at follow-up. In particular the
change in male scores, on average, was clinically significant such that as a group their scores
showed a move to below the clinical-cut off point for ‘possible depression’.
Page | 740
35
30
25
20
15
10
5
0
Pre-Female F/Up Female Pre-Male F/Up Male
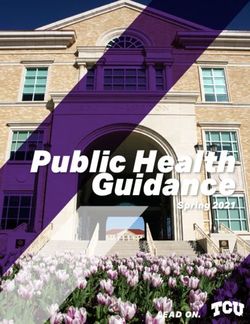
Figure 2: Participants’ KPCS mean scores at pre-workshop and four week follow-up. Note:
Scores 39 or less = possible low levels of parenting confidence.
The participants’ pre-workshop and follow-up KPCS mean scores are presented in Figure 2.
The data show that the pre- male and pre- female scores, on average, were below the
clinical cut-off point possibly indicating low levels of parenting confidence. Pre-workshop,
the female participants, on average, rated themselves higher in parenting confidence than
the males. Further analysis of individual scores revealed that 100% of male participants
were below the clinical cut-off point pre-workshop, compared to 33.3% of female
participants. At follow-up, the average female scores had improved to within the non-
clinical range. There was a slight improvement for males, pre-workshop to follow-up.
Page | 85
4
3
2
1
0
1 2 3 4 5 9 10
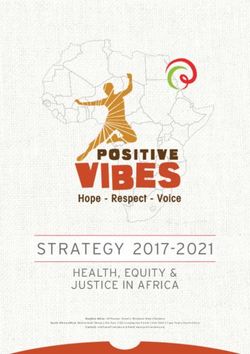
Figure 3: Participants’ mean scores on the individual CNCL-WEF items at 4-week follow-up.
Note: Scores range from 1 = low to 5 = high (the higher the rating, the more positive the
evaluation).
The participants’ responses to the individual CNCL-WEF items (see Appendix A for
descriptions) are shown in Figure 3. Converted to percentages, ratings ranged from 69%
(Item 2, workshop helping with adjustment) to 91% (Item 10, satisfaction with the setting).
Overall, the participants rated their satisfaction with the workshop at 78% (Item 1). In terms
of providing support and education around mental health issues (Item 5), the overall rating
was 83%.
Post-Workshop Participant Feedback
The following quotes are samples from the participants’ workshop evaluation forms.
Can you identify any changes that occurred after your attendance in this workshop?
‘Yes, acknowledging that I can only change things that are in my control and loving and
enjoying my baby now rather than wanting to change him or wishing that he’s older’.
‘I’ve become a lot more ‘in the moment’ and mindful and I’ve also started looking at the big
picture of parenting’.
‘Somewhat easier to keep an in-the-moment perspective’.
‘I’m learning to relax more’.
‘More discussion with my partner’.
Page | 9Which parts of the workshop were most helpful? ‘The discussion on self care was helpful’. ‘Values. This was something we had never thought about’. ‘Discussion with other parents. It was nice to hear that we are in the same boat and that our stresses are common’. ‘Information about where to get help and postnatal depression information’. ‘Validating what my husband and I are experiencing as common to others’ experiences’. ‘The information-pack regarding information on depression and how to get appropriate help’. ‘Talking to fellow parents and the presenters regarding issues, how people dealt with them and the feelings involved’. Which parts of the workshop were the most enjoyable? ‘Discussion around the group – good to hear other’s experiences and hearing that we’re not alone’. ‘Discussion with other parents’. ‘Sharing stories and experiences’. ‘Question and answer and discussions’. ‘Interactions with other parents’. ‘The second week. Learning to organise and the issues regarding mental health’. ‘I enjoyed the slow pace of it. It was a pleasant change from the fast pace of caring for our baby’. How could this workshop be improved in the future? ‘More examples and techniques for improving situations’. ‘Focus less on postnatal depression and add more parenting skills’. ‘Role plays and good/bad case studies and examples would be fun’. ‘More information on routine, sleeping, etc.’. ‘More (baby) age-specific information’. ‘Provide a more basic explanation of attachment’. Discussion This report described an evaluation of a piloted community workshop aimed at helping parents adjust to their first year of parenting. The results support a successful piloting of the workshop. Eighteen participants started and fifteen completed both evenings of the workshop. There was a reduction in average EPDS scores for the group pre-workshop to Page | 10
follow-up. Changes in EPDS scores were clinically significant for males because their scores moved from above the clinical cut-off point to within the normal range. Importantly, the male participants rated themselves as experiencing higher levels of depressive symptoms pre-workshop and at four week follow-up. Females were within the non-clinical range at both points, yet still reported elevated levels of symptoms. There was a slight improvement in the average level of parenting confidence for both the female and male participants pre-workshop to follow-up, more so for females for whom average parenting confidence scores improved to move to the non-clinical range. Overall, follow-up satisfaction ratings for six of the seven items relating to the workshop content and facilitation were above 70%. In particular, the overall workshop satisfaction rating for the group was high. In terms of helping with mental health issues, the satisfaction rating was very high. Qualitative feedback was thoughtful and encouraging, with many participants endorsing various components of the workshop. The only slight improvement in parenting confidence for parents was not entirely unexpected, given that others have found that effect sizes across the range of factors (e.g., parent self-efficacy) examined in the large scale meta-analysis of early parenting programs tend to be quite small (Pinquart & Teubert, 2010). However, the point has been made that with early parenting programs, small improvements in outcome measurement may still reflect meaningful change for the participant (Parker & Hunter, 2011). This point notwithstanding, integration of participant feedback from this pilot can be used to assist future efforts to modify the current workshop to increase the likelihood of significant improvements in the area of parenting confidence. There are limitations that need to be considered. First, caution must be taken before generalising to wider populations and clinical practitioners as only a relatively small group was involved with the workshops and evaluations were conducted by the same two practitioners. Secondly, there was no opportunity to randomise allocation of participants to the workshop or a comparison group. Changes may not be uniquely attributable to the CNCL workshop. Finally, the time period between the workshop and follow-up evaluation was relatively brief at four weeks. Page | 11
There were notable strengths to this evaluation. Multiple measurement instruments were used, some with strong psychometric properties (e.g., EPDS, KPCS). The workshop was clearly defined through its administration in PowerPoint and associated materials. Participants met criteria for poor adjustment to parenting. Some were experiencing clinically significant levels of PND-related symptoms. Efforts were made to ensure a period of time had elapsed before the participants were administered follow-up evaluations. The outcomes of this piloted CNCL workshop have important implications for community organisations seeking to provide an effective workshop or program for mothers and fathers adjusting to parenting. These findings suggest that PND symptoms might be at worrying levels for new parents, regardless of gender. Levels of parenting confidence might be low. The workshop model provided here represented a relatively straight-forward, easily accessible, community-based intervention for these types of parents. The fact that there was an overall improvement for the group as measured using standardised instruments is encouraging. Future efforts could include attempts to replicate the pilot while also integrating the findings here, especially the participants’ qualitative feedback, into what might be an improved workshop. The challenge for practitioners will be in satisfying the unique needs of each parenting dyad, without necessarily excluding the other members of the group at each point and failing to include other important aspects of content as suggested by the existing body of research. As was the aim with the current pilot, future efforts need to maintain a workable balance between client-centered and evidence-based practices. Author Information Dr Jarrod Turner has a background in Clinical Psychology and works in Ngala’s Hey Dad WA program providing support and education to fathers in the early parenting period. Regina Fogarty has a background in Child Health Nursing and works in Ngala’s Parent Education program providing support and education to parents in all areas of early parenting. Page | 12
References
Austin, M.P.V., Hadzi-Pavlovic, D., Priest, S. R., Reilly, N., Wilhelm, K., Saint, K., & Parker, G.
(2010). Depressive and anxiety disorders in the postpartum period: how prevalent
are they and can we improve their detection? Archives of Women's Mental Health,
13(5), 395-401.
Australian Bureau of Statistics. (2008). National survey of mental health and wellbeing:
Summary of results: 4326.0. Canberra: Australian Bureau of Statistics.
Bowlby, J. (1988). A secure base: Parent-child attachment and healthy human development.
New York: Basic Books.
Buist, A., & Bliszta, J. (2006). The beyondblue national postnatal screening program,
prevention and early intervention 2001-2005, Final report. Vol 1: National Screening
Program. Melbourne: beyondblue: the national depression initiative.
Cox, J.L., Chapman, G., Murray, D., & Jones, P. (1996). Validation of the Edinburgh Postnatal
Depression Scale (EPDS) in non postnatal women. Journal of Affective Disorders, 39,
185-189.
Cox, J.L., Holden, J.M., & Sagovsky, R. (1987). Detection of postnatal depression:
Development of the 10 item Edinburgh postnatal depression scale. British Journal of
Psychiatry, 150, 782-786.
Črnčec, R., Barnett, B., & Matthey, S. (2008). Karitane Parenting Confidence Scale: Manual.
Sydney South West Area Health Service. Sydney: Australia.
Families, Housing, Community Services, and Indigenous Affairs (FaHCSIA). (2009). Father-
inclusive practice guide. Canberra: Commonwealth Government.
Field, T. (1992). Infants of depressed mothers. Development and Psychopathology, 4, 49-66.
Page | 13Fletcher, R. (2011). The dad factor: How the father-baby bonding helps a child for life. NSW:
Finch Publishing.
Fletcher, R.J., Matthey, S., & Marley, C.G. (2006). Addressing depression and anxiety among
new fathers. Medical Journal of Australia, 185, 461-463.
Goodman, J. H. (2004). Paternal postpartum depression: Its relationship to maternal
postpartum depression, and implications for family health. Journal of Advanced
Nursing, 45(1), 26–35.
Leverton, T.J. & Elliott, S.A. (2000). Is the EPDS a magic wand: A comparison of the
Edinburgh Postnatal Depression Scale and health visitor report as predictors of
diagnosis on the Present State Examination. Journal of Reproductive and Infant
Psychology, 18, 279-296.
Lovejoy, M.C., Graczyk, P.A., O’Hare, E., & Neuman, G. (2000). Maternal depression and
parenting behaviour: A meta-analytic review. Clinical Psychology Review, 20, 561-
592.
Matthey, S., Barnett, B., Kavanagh, D.J., & Howie, P. (2001). Validation of the Edinburgh
Postnatal Depression Scale for men, and comparison of item endorsement with their
partners. Journal of Affective Disorders, 64, 175-184.
National Research Council and Institute of Medicine. (2009). Depression in parents,
parenting, and children: Opportunities to improve identification, treatment, and
prevention. Washington, DC: The National Academies Press.
Parker, R., & Hunter, C. (2011). Supporting couples across the transition to parenthood.
(Briefing No. 20). Australian Institute of Family Studies, 1-9.
Page | 14Tronick, E.Z., & Gianino, A.F. (1986). The transmission of maternal disturbance to the infant.
In E.Z. Tronick and T.Field (Eds.), Maternal depression and infant disturbance (pp. 5-
11). San Francisco: Jossey-Bass.
Whiffen, V.E., & Gotlib, I.H. (1989). Infants of postpartum depressed mothers:
Temperament and cognitive status. Journal of Abnormal Psychology, 98, 274-279.
Woolhouse, H., Brown, S., Krastev, A., Perlen, S., & Gunn, J. (2009). Seeking help for anxiety
and depression after childbirth: results of the Maternal Health Study. Archive of
Women’s Mental Health, 12, 75-83.
Yelland, J., Sutherland, G., & Brown, S.J. (2010). Postpartum anxiety, depression and social
health: Findings from a population-based survey of Australian women. BMC Public
Health, 10, 771.
Page | 15Appendix A
Changing Nappies – Changing Lives: Adjusting to parenting your new baby
Workshop Evaluation:
Completion of this form does not require personal information, just your gender
Male / Female (please circle)
Please circle the appropriate number: 1 = low, 5 = high
1. How do you rate your satisfaction with this workshop?
1 2 3 4 5
2. How do you rate this workshop as a means of helping your adjustment to
parenting?
1 2 3 4 5
3. How do you rate this workshop in helping you understand yours and your
child’s needs?
1 2 3 4 5
4. How do you rate this workshop as information around day to day parenting?
1 2 3 4 5
5. How do you rate this workshop as a means of helping you understand
mental health issues?
1 2 3 4 5
6. Can you identify any changes that occurred after your attendance in this
workshop?
Page | 16Appendix A
7. Which parts of the workshop were the most helpful?
Why?
8. Which parts of the workshop were the most enjoyable?
Why?
9. How satisfied were you with the presenters of this workshop?
1 2 3 4 5
10. How satisfied were you with the setting and facilities for the workshop?
1 2 3 4 5
11. How could this workshop be improved in the future?
12. Can we use your comments in future CNCL promotions?
Yes No (Please circle)
Date you completed this form:__________
THANK YOU FOR COMPLETING THIS FORM
Page | 17You can also read