Clinical pharmacology of the adenosine diphosphate (ADP) receptor antagonist, clopidogrel
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Vascular Medicine 1998; 3: 247–251
Clinical pharmacology of the adenosine diphosphate
(ADP) receptor antagonist, clopidogrel
Karsten Schrör
Abstract: Antiplatelet compounds interfere with the platelet activation cascade at different lev-
els. The antiplatelet effect of the thienopyridine, clopidogrel, results from antagonism of a plate-
let ADP receptor, P2T, resulting in inhibition of platelet activation. This antagonism is non-com-
petitive, irreversible, and results in a 50–70% inhibition of platelet fibrinogen binding.
Additionally, clopidogrel may also antagonize the ADP-induced inhibition of adenylate cyclase,
possibly resulting in an elevated platelet cyclic adenosine monophosphate level after stimu-
lation by an appropriate agonist, such as prostacyclin. This spectrum of antiplatelet activities
is different from that of aspirin. Further, clopidogrel is associated with a reduction in gastro-
intestinal hemorrhage, making it a valuable therapeutic alternative to aspirin in oral, long-term
prevention of atherothrombotic vascular occlusion.
Key words: ADP; atherosclerosis; clopidogrel; platelet; thrombosis
Atherosclerosis and atherothrombosis adhesive surfaces, to circulating blood.4 Soluble agonists,
such as adenosine diphosphate (ADP) and thromboxane A2
Atherosclerosis is a chronic vascular disease that develops (TxA2) synergistically accelerate platelet activation. This
over years and may remain asymptomatic for long periods results in platelet shape change, granule secretion,5 and
of time.1 Morphologically, there is a progressive narrowing exposure of platelet phospholipids to circulating blood,
of the arterial lumen, eventually resulting in regional which accelerates local thrombin formation. Finally, the
ischemia, such as transient ischemic attacks (TIA), effort platelet integrin, GpIIb/IIIa, is activated, undergoing a con-
angina, or intermittent claudication. Atherosclerotic vessels formational change at the surface of the platelet allowing
may potentially undergo a catastrophic event – acute throm- it to bind soluble fibrinogen. This results in the cross-link-
botic occlusion – with the corresponding clinical manifes- ing of platelets via fibrinogen bridges, termed platelet
tations of myocardial infarction, sudden death, or ischemic aggregation.
cerebral infarction. Each of these life-threatening events are
initiated by platelet-dependent thrombus formation, most
commonly at the thrombogenic surface of an atheroscler-
otic plaque. Antiplatelet therapy is a symptomatic and The significance of ADP in platelet
effective approach2 to preventing the consequences of activation
endothelial dysfunction in atherosclerotic vascular disease,
which could otherwise result in uncontrolled intravascular
platelet activation. Almost 40 years ago, ADP was found to cause red blood
cell-dependent sticking (adhesion) of platelets to glass.6,7
Shortly after that, it was also observed that ADP could
Pathophysiology of platelet-dependent induce platelet-to-platelet adhesion (aggregation). This
thrombus formation action was dependent on the presence of Ca++ and fibrino-
gen.8,9 Further, platelet-dependent hemostatic plug forma-
Thrombus formation at a site of arterial vascular injury is tion was inhibited in the presence of ADP-metabolizing
initiated by the adhesion of resting platelets to the vessel enzymes.10 Shear stress–induced platelet activation is larg-
wall. This response is mediated by the expression of plate- ely dependent on ADP11 and is resistant to aspirin,12 as is
let adhesion molecules, such as GpIb/IX and GpIIb/IIIa, ADP-induced platelet activation in vivo, i.e. in the presence
which bind to von Willebrand factor and other components of physiological Ca++ concentrations. These data and a
of the vascular subendothelium.3 The binding of these number of follow-up studies led to the view that ADP is
adhesion molecules, along with other integrins, is regulated one of the most important mediators of platelet activation
by accessibility of the subendothelial matrix, with its in vivo.13
There are several rich sources of extracellular nucleotides
in the blood, such as ADP. These include red blood cells,
Institut für Pharmakologie, Heinrich-Heine-Universität Düsseldorf, endothelial cells and platelet-dense granules.14–16 In the pla-
Düsseldorf, Germany telet aggregates formed after vascular injury, local extra-
Address for correspondence: Karsten Schrör, Institut für Pharmakologie, cellular nucleotide concentrations may temporarily exceed
Heinrich-Heine-Universität Düsseldorf, Moorenstr. 5, D-40225, Düssel- 100 M.17 Thus, ADP appears to be a potent, broad-spec-
dorf, Germany. trum, endogenous platelet-stimulatory agent in vivo.
Arnold 1998 1358-863X(98)VM244MP
Downloaded from vmj.sagepub.com by guest on November 7, 2015248 K Schrör
Mechanisms of ADP-induced platelet by aspirin may enhance the antiaggregatory nature of ADP
activation antagonists on platelets via this mechanism (Figure 1).
The most important cellular signal transduction pathway
ADP receptor(s) of ADP, however, may result from activation of the platelet
Biochemical and pharmacologic findings suggest the exist- GpIIb/IIIa complex, the final common pathway of platelet
ence of at least two different ADP receptors on the platelet aggregation used by all platelet agonists. Irreversible plate-
membrane belonging to the P2X1 and P2T subtypes of let aggregation requires the binding of fibrinogen to this
purinergic receptors (Figure 1). The P2X1 receptor is an receptor. As with other agonists, such as collagen and
ADP ligand associated with an ion channel. The P2T recep- thrombin, ADP initiates the activation of fibrinogen binding
tor is a heptahelical membrane receptor that is coupled to sites on platelet membranes. This occurs via conformational
intracellular signaling pathways via G-proteins. The P2T changes in the GpIIb/IIIa complex that are prerequisite to
receptor subtype mediates other, still unknown platelet-sti- stable platelet thrombus formation.
mulating actions of ADP. There are about 400–1000 ADP
receptors per platelet, a number comparable with those of
other G-protein–coupled platelet receptors, including vaso-
pressin, ␣-agonists and TxA2.18 Mode of action of clopidogrel
ADP receptor signal transduction
There are at least three different signal transduction path- Although most evidence suggests that the activity of clopi-
ways that may become activated after ligand binding to the dogrel is a direct result of its antagonism of the ADP recep-
platelet ADP receptor: activation of GpIIb/IIIa; inhibition tor, it may also interfere with a more distal step in the plate-
of adenylate cyclase activation; and stimulation of phos- let activation pathway, such as a ␣-protein response or
pholipase C (PLC). The significance of an ADP-stimu- tyrosine kinase phosphorylation.20 This mode of action is
lated increase in cytosolic Ca++ concentration via activation different from aspirin, which does not directly affect ADP-
of PLC and the subsequent formation of inositol triphosph- induced platelet functions, including platelet adhesion and
ate and release of Ca++ from intracellular storage sites has ␣-granule secretion. In contrast to aspirin, clopidogrel does
not been fully elucidated.19 It has been shown, however, not directly interfere with arachidonic acid metabolism.
that increases in cytosolic Ca++ levels are a consequence of Thus, the inhibition of platelet aggregation brought about
PLC stimulation by TxA2. Inhibition of TxA2 formation by clopidogrel is completely different from that of aspirin.
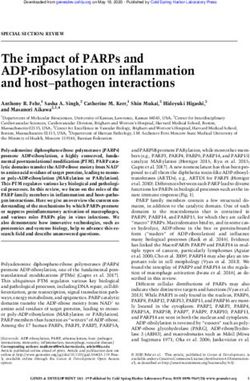
Figure 1 Signal transduction by ADP in platelets and its modification by clopidogrel. (Abbreviations: ADP, adenosine
diphosphate; P2X1, principal platelet ADP receptor (ADP-liganded ionic channel); AC, adenylate cyclase; cAMP, cyclic adenosine-
3′5′-monophosphate; IP3, inositol triphosphate; DAG, diacylglycerol; PLC, phospholipase C; Ca++, calcium; PIP2,
phosphatidylinositol 4,5-bisphosphate; TP, thromboxane receptor; IP, prostacyclin receptor; TxA2, thromboxane A2; Gq, Gs, Gi, G
proteins; P2T, purinergic platelet ADP receptor (high-affinity, G-protein-coupled heptahelical receptor); GP IIb/IIIa, glycoprotein
IIb/IIIa; ATP, adenosine triphosphate; PGI2, prostacyclin.)
Vascular Medicine 1998; 3: 247–251
Downloaded from vmj.sagepub.com by guest on November 7, 2015Pharmacology of clopidogrel 249
ADP receptors degranulation of platelets in contact with a collagen surface
Clopidogrel markedly reduces high-affinity ADP binding to and the subsequent formation of a thrombus. Since clopido-
a subset of ADP receptors (P2T) at the platelet membrane grel reduces fibrin deposition and thrombus formation, it
(Figure 1).21,22 The affinity of these receptors for ADP has been suggested that clopidogrel interferes with platelet-
remains unchanged during treatment with clopidogrel, to-platelet interactions26 through its effects on ADP-depen-
which causes a 60–70% reduction in ADP binding.18,22 A dent platelet activation.
similar, 70% reduction in ADP binding was observed in
one patient with a congenitally defective ADP response Adenylate cyclase activity
(Figure 2).21 Clopidogrel’s inhibition of ADP binding is Exposure of platelets to ADP causes inhibition of adenylate
non-competitive and irreversible,23 although 20–30% of cyclase at the platelet membrane.27 Clopidogrel suppresses
receptors are not affected. Since clopidogrel does not affect this inhibition of adenylate cyclase and the subsequent fall
the shape change associated with platelet activation, it has in cAMP levels.28,29 This action might be less significant
been suggested that the population of binding sites that in ex vivo conditions because of the short half-life of com-
remain unaffected after treatment might be specifically pounds that increase cAMP levels such as prostacyclin
involved in the platelet shape change.23 It has also been (PGI2). However, this response may contribute to clopidog-
suggested that clopidogrel has effects other than on plate- rel’s inhibition of platelet aggregation in vivo, particularly
lets, such as the modulation of vascular tone.24 in ischemic areas, where PGI2 production is increased.30
GpIIb/IIIa complex
As a consequence of reduced agonist binding at the P2T
ADP receptor, there is a marked inhibition of ADP-induced Active principle(s) of clopidogrel
conformational changes in the GpIIb/IIIa complex. This
activation is essential for the binding of soluble agonists, Clopidogrel is inactive in vitro in conventional assays of
such as fibrinogen, and subsequent platelet aggregate for- platelet activation. Ex vivo data suggest that the irreversible
mation.20,25 Insufficient fibrinogen bridging resulting from inhibition of platelet aggregation by clopidogrel is not
reduced numbers of platelet GpIIb/IIIa receptors will also mediated by metabolites detected in the plasma. More
result in less stable platelet aggregates and more rapid clot detailed studies of the mechanisms involved in clopidogrel
resolution.25 Fibrinogen binding after clopidogrel treatment bioactivation were conducted in animals, particularly the
is reduced by about 70%.25 The clinical result is a doubling rat. In this species, the antiaggregating potency of clopidog-
of the bleeding time. In contrast with ADP receptor antag- rel was similar after intravenous or oral administration, but
onists, selective GpIIb/IIIa antagonists, such as abciximab, was markedly reduced after functional hepatectomy.31 It
integrelin and tirofiban, bind directly to the integrin and was also seen that inhibition of cytochrome P450 (CYP) by
prevent the access of ligands, such as soluble fibrinogen, drugs or antibodies decreased the antiaggregating effect of
to the activated GpIIb/IIIa complex through competitive clopidogrel, while stimulators of the CYP1A1 enzyme
antagonism. subfamily had the opposite effect.23 Based on these data, it
was suggested that the active principle of clopidogrel is
Platelet secretion generated in the liver by an unknown metabolic change that
Studies in non-anticoagulated, ex vivo human blood have activates the native drug.31
shown that clopidogrel profoundly inhibits both the
Time-dependency of antiplatelet action
Clinical inhibition of platelet aggregation does not occur
immediately with administration of clopidogrel. A detect-
able antiplatelet effect can be observed within 2 h of treat-
ment;32 it becomes significant after 2 days of treatment and
maximum inhibition is achieved after 4–7 days.33 The velo-
city of the initial response may be increased with higher
doses.32 Interestingly, one preliminary report has suggested
that administration of a loading dose of clopidogrel
(375 mg) will result in a 55% inhibition of ADP-induced
platelet aggregation after 1 h and 80% inhibition after 5 h.
A maximal prolongation of bleeding time – approximately
twofold – was seen after 3 days.34 The half-life of clopidog-
rel (assessed with the metabolite SR 26334) is 7–8 h after
a single administration; full recovery of platelet activity is
seen about 1 week after treatment is ended. This suggests
normalization of platelet function through platelet turn-
over.21,33,35 The efficacy of clopidogrel (75 mg/day) was
comparable with that of ticlopidine (500 mg/day).36 The
ability of clopidogrel to inhibit platelet function and pro-
Figure 2 ADP binding sites in human platelets after oral long bleeding time was unchanged between weeks 1 and 4
clopidogrel (75 mg/day) compared with a patient with a
congenital defect in ADP response. ADP binding was of treatment.36 A study in healthy volunteers found that the
determined with the stable ligand 2MeS-ADP. (Source: data antiplatelet effects of clopidogrel (75 mg/day) increased by
from refs 21 and 22.) less than 10% after 3 months of therapy, compared with
Vascular Medicine 1998; 3: 247–251
Downloaded from vmj.sagepub.com by guest on November 7, 2015250 K Schrör
the level of steady-state inhibition achieved after 8–12 days To examine the potential in vivo inhibition and/or induc-
of therapy. There was no further prolongation of the bleed- tion of hepatic enzymes, clopidogrel use was studied in
ing time. Similarly, no significant differences in antiplatelet healthy male volunteers. After clopidogrel administration
efficacy were seen when clopidogrel was administered to (75 mg/day for 10 days), no statistically significant differ-
young and elderly patients with and without atheroscler- ence in the elimination half-life of antipyrine (non-specific
osis.37 Collectively, these data suggest that the prolonged isoenzyme substrate) was observed. Plasma levels of
half-life of clopidogrel after regular daily intake for several gamma-glutamyl transpeptidase (␥-GT) and cortisol were
weeks does not result in a potentiation of antiplatelet effects not affected by this treatment, nor was urinary excretion of
or additional prolongation of bleeding time. 6- OH-cortisol (CYP3A substrate). This led the authors
to conclude that clopidogrel, under the conditions of this
study, does not cause hepatic enzyme induction nor does it
Clopidogrel versus aspirin modify the activity of hepatic oxidative enzyme systems.44
No liver dysfunction was reported in the CAPRIE trial.38
In dose-ranging studies, clopidogrel (75 mg) was found to It should be noted, however, that the CAPRIE trial was a
have the same effect as ticlopidine (500 mg).36 The clinical phase III study with numerous exclusionary criteria for
efficacy of clopidogrel has been demonstrated in the CAP- patient selection, including a history of drug-induced hep-
RIE trial38 in which clopidogrel (75 mg/day) was found to atic abnormalities. Other studies have indicated that pharm-
cause a significant 8.7% relative risk reduction (p = 0.043) acologic interactions do not occur during co-administration
in the combined vascular endpoints of myocardial infarc- of clopidogrel and aspirin,45 digoxin,46 heparin,47 atenolol,48
tion, ischemic stroke and vascular death compared with or nifedipine.48
aspirin (350 mg/day). The mean duration of treatment was The results of studies performed with clopidogrel show
about 2 years. that it has antiplatelet activity and reduces the occurrence
The percentage of patients who dropped out of the study of thrombotic occlusive vascular disease. Clopidogrel has
early because of adverse events was 11.4%: 6.01% of these a greater efficacy than aspirin (8.7% relative risk reduction
came from the aspirin group and 5.38% came from the clo- compared with aspirin; p = 0.043), the current ‘gold stan-
pidogrel group.38 Not surprisingly, the side-effects associa- dard’ for antiplatelet activity, and a reduced association
ted with aspirin and clopidogrel were different. The most with gastrointestinal bleeding and discomfort; in addition,
common side-effects observed during clopidogrel therapy clopidogrel does not appear to cause neutropenia. Based on
were diarrhea and rash. Upper gastrointestinal discomfort results of the CAPRIE trial, clopidogrel appears to be an
and bleeding occurred more frequently during aspirin ther- efficacious and safe new agent for patients at risk of occlus-
apy. Importantly, the CAPRIE trial showed that the rate ive vascular events.
of neutropenia was similar in both groups. Because of the
different potencies, mechanisms of action and adverse Note added in proof
effect spectra, clopidogrel is considered to be a valuable Subsequent to the original submission of this paper, Weber
therapeutic alternative to aspirin. and co-workers49 have reported that clopidogrel specifically
An interesting approach to antiplatelet therapy is the inhibits ADP-induced aggregation of washed human plate-
combined use of clopidogrel and aspirin for prevention of lets in vitro without hepatic bioactivation.
thromboembolic stent occlusion. Several controlled clinical
trials have indicated that the combined use of ticlopidine
and aspirin is more effective and has fewer side-effects than References
conventional therapy with anticoagulants.39 Similar ben-
eficial results were obtained in patients who received stents 1 Ross R, Fuster V. The pathogenesis of atherosclerosis. In: Fuster V,
as a bail-out procedure for failed angioplasty or suboptimal Ross R, Topol EJ eds. Atherosclerosis and coronary artery disease.
PTCA results.40 However, to date these uses have not been Philadelphia: Lippincott-Raven, 1996: 411–60.
studied with clopidogrel in humans. Animal experiments 2 Antiplatelet Trialists’ Collaboration. Collaborative overview of ran-
clearly suggest that clopidogrel prevents thrombotic reoc- domized trials of antiplatelet therapy. I. Prevention of death, myocar-
dial infarction and stroke by prolonged antiplatelet therapy in various
clusion of coronary,41 femoral,41,42 and carotid arteries after
categories of patients. Br Med J 1994; 308: 81–106.
endothelial injury under conditions in which aspirin is inef- 3 Ruggeri ZM. Mechanisms initiating platelet thrombus formation.
fective. In addition, clopidogrel prevented coronary artery Thromb Haemost 1997; 78: 611–16.
reocclusion more effectively than aspirin.43 4 Du X, Ginsberg MH. Integrin ␣IIb3 and platelet function. Thromb
Haemost 1997; 78: 96–100.
5 Schafer AL. Antiplatelet therapy. Am J Med 1996; 101: 199–209.
Clopidogrel pharmacology 6 Hellem A. The adhesiveness of human blood platelets in vitro. Scand
J Clin Invest 1960; 12: 1–17.
Drug interactions 7 Gaarder A, Jonsen J, Laaland S, Hellem A, Owren PA. Adenosine
Data in animal experiments (rats) suggest that clopidogrel diphosphate in red cells as a factor in the adhesiveness of human blood
platelets. Nature 1961; 192: 531–32.
might interact with at least two components of the hepatic
8 Born GVR. Platelet aggregation and its reversal. Nature 1962; 194:
P450 system. Therefore, it is important to know whether
927–29.
similar events occur in humans, since this could eventually 9 O’Brien JR. Platelet aggregation. Part II. Some results from a new
prolong the drug’s half-life. Alternatively, ADP receptor method of study. J Clin Pathol 1962; 15: 446–51.
antagonists may interfere with the metabolism of other 10 Zawilska KM, Born GVR, Begent N. Effect of ADP-utilizing enzymes
compounds that are subject to extensive hepatic clearance, on the arterial bleeding time in rats and rabbits. Br J Haematol 1982;
such as phenytoin, theophylline and antipyrin. 50: 317–25.
Vascular Medicine 1998; 3: 247–251
Downloaded from vmj.sagepub.com by guest on November 7, 2015Pharmacology of clopidogrel 251
11 Moritz MW, Reimers RC, Baker RK, Sutera SP, Joist JH. Role of 31 Savi P, Herbert J-M, Pflieger AM et al. Importance of hepatic metab-
cytoplasmic and releasable ADP in platelet aggregation induced by olism in the antiaggregating activity of the thienopyridine clopidogrel.
laminar shear stress. J Lab Clin Med 1983; 101: 537–44. Biochem Pharmacol 1992; 44: 527–32.
12 Moake JL, Turner NA, Stathopoulos NA, Nolasco L, Hellums JD. 32 Kieffer G, Caplain H, Thiercelin JF, Thebault JJ. Tolerance and phar-
Shear-induced platelet aggregation can be mediated by vWF released macological activity of a new antiplatelet agent clopidogrel [SR 25990
from platelets, as well as by exogenous large or unusually large vWF C] in normal healthy volunteers after single increasing administrations.
multimers, requires adenosine diphosphate, and is resistant to aspirin. Thromb Haemost 1989; 62: 411 [abstract].
Blood 1988; 71: 1366–74. 33 Caplain H, Kieffer G, Thiercelin JF, Thebault JJ. Tolerance and clini-
13 Born GVR. Adenosine diphosphate is a mediator of platelet aggre- cal pharmacology of repeated administration of clopidogrel [SR 25990
gation in vivo: an editorial view. Circulation 1985; 72: 741–46. C], a new antiplatelet agent, at three dose levels in normal healthy
14 Rao AK, Willis J, Holmsen H. A major role of ADP in thromboxane volunteers. Thromb Haemost 1989; 62: 410 [abstract].
transfer experiments: studies in patients with platelet secretion defects. 34 Bachmann F, Savcic M, Hauert J, Geudelin B, Kieffer G, Cariou R.
J Lab Clin Med 1984; 104: 116–26. Rapid onset of inhibition of ADP-induced platelet aggregation by a
15 Valles J, Santos MT, Aznar J et al. Erythrocytes metabolically enhance loading dose of clopidogrel. Eur Heart J 1996; 17 (suppl): 263.
collagen-induced platelet responsiveness via increased thromboxane 35 Herbért JM, Frekel D, Vallee E et al. Clopidogrel, a novel antiplatelet
production, adenosine diphosphate release and recruitment. Blood and antithrombotic agent. Cardiovasc Drug Rev 1993; 11: 180–98.
1991; 78: 154–62. 36 Boneu B, Destelle G on behalf of the Study Group. Platelet anti-aggre-
16 Santos MT, Valles J, Marcus AJ et al. Enhancement of platelet reac- gating activity and tolerance of clopidogrel in atherosclerotic patients.
tivity and modulation of eicosanoid production by intact erythrocytes: Thromb Haemost 1996; 76: 939–43.
a new approach to platelet activation and recruitment. J Clin Invest 37 Guillin M-C, Bonnet G, Sissmann J, Neccian J, Dickinson JP. Pharma-
1991; 87: 571–80. codynamics and pharmacokinetics of the novel antiplatelet agent, clop-
17 Coade SB, Pearson JD. Metabolism of adenine nucleotides in human idogrel, in the young and the elderly with and without symptomatic
blood. Circ Res 1989; 65: 531–37. atherosclerosis. Eur Heart J 1996; 17 (suppl): 161.
18 Mills DC. ADP receptors on platelets. Thromb Haemost 1996; 76: 38 Gent M, CAPRIE Steering Committee. A randomised, blinded trial
835–55. of clopidogrel versus aspirin in patients at risk of ischaemic events
19 Gachet C, Hechler B, Léon C, Vial C, Ohlmann P, Cazenave J-P. [CAPRIE]. Lancet 1996; 348: 1329–39.
Purinergic receptors on blood platelets. Platelets 1996; 7: 261–67. 39 Schömig A, Neumann F-J, Kastrati A et al. A randomized comparison
20 Nurden AT. New thoughts on strategies for modulating platelet func- of antiplatelet and anticoagulant therapy after the placement of coron-
tion through the inhibition of surface receptors. Haemostasis 1996; 26 ary-artery stents. N Engl J Med 1996; 334: 1084–89.
(suppl 4): 78–88. 40 Lablanche J-M, McFadden EP, Bonnet J-L et al. Combined antiplatelet
21 Mills DCB, Puri RN, Hu CJ et al. Clopidogrel inhibits the binding of therapy with ticlopidine and aspirin. A simplified approach on intraco-
ADP analogues to the receptor mediating inhibition of platelet adenyl- ronary stent management. Eur Heart J 1996; 17: 1373–80.
ate cyclase. Arterioscler Thromb 1992; 12: 430–36. 41 Yao S-K, Ober JC, McNatt J et al. ADP plays an important role in
22 Gachet C, Cattaneo M, Ohlmann PO et al. Purinoceptors on blood mediating platelet aggregation and cyclic flow variations in vivo in
platelets: further pharmacological and clinical evidence to suggest the stenosed and endothelium-injured canine coronary arteries. Circ Res
presence of two ADP receptors. Br J Haematol 1995; 91: 434–44. 1992; 70: 39–48.
23 Savi P, Combalbert J, Graich C et al. The antiaggregating activity of 42 Samama CM, Bonnin P, Bonneau M et al. Comparative arterial
clopidogrel is due to metabolic activation by the hepatic cytochrome antithrombotic activity of clopidogrel and acetyl salicylic acid in the
P450–1A. Thromb Haemost 1994; 72: 313–17. pig. Thromb Haemost 1992; 68: 500–505.
24 Yang LH, Fareed J. Vasomodulatory action of clopidogrel and ticlopi- 43 Yao S-K, Ober JC, Ferguson JJ et al. Clopidogrel is more effective
dine. Thromb Res 1997; 86: 479–91. than aspirin as adjuvant treatment to prevent reocclusion after throm-
25 Humbert M, Nurden P, Bihour C et al. Ultrastructural studies of plate- bolysis. Am J Physiol 1994; 267: H488-H93.
let aggregates from human subjects receiving clopidogrel and from a 44 Pierce CH, Houle J-M, Kieffer G, Dickinson JP. Absence of effect of
patient with an inherited defect of an ADP-dependent pathway of plat- clopidogrel on human hepatic P-450 activities. Eur Heart J 1996; 17
elet activation. Arterioscler Thromb Vasc Biol 1996; 16: 1532–43. (suppl): 160 [abstract].
26 Roald HE, Barstad M, Kierulf P et al. Clopidogrel – a platelet inhibitor 45 Caplain H, D’Honneur G, Cariou R. Lack of interaction of aspirin
which inhibits thrombogenesis in non-anticoagulated human blood (100 mg) with chronic clopidogrel in volunteers. Haemostasis 1996;
independently of the blood flow conditions. Thromb Haemost 1994; 26 (suppl 3): 557.
71: 655–62. 46 Peeters PAM, Crijns WJ, Tamminga WJ et al. Absence of pharmacoki-
27 Cooper DMF, Rodbell M. ADP is a potent inhibitor of human platelet netic interaction between the novel antiplatelet agent, clopidogrel, and
plasma membrane adenylate cyclase. Nature 1979; 282: 517–18. digoxin. Eur Heart J 1996; 17 (suppl): 160 [abstract].
28 Gachet C, Stierle A, Cazenave JP et al. The thienopyridine PCR 4099 47 D’Honneur G, Caplain H, Cariou R, Brouard R. Interaction study
selectively inhibits ADP-induced platelet aggregation and fibrinogen between clopidogrel and prolonged intravenous heparin administration
binding without modifying the membrane glycoprotein IIb/IIIa com- in young healthy volunteers. Haemostasis 1996; 26 (suppl 3): 554.
plex in rat and man. Biochem Pharmacol 1990; 40: 229–38. 48 Forbes CD, Belch JJ, Bridges AB et al. Pharmacodynamic compat-
29 Defreyn G, Gachet C, Savi P, Driot F, Cazenave JP, Maffrand JP. ability of clopidogrel with atenolol and nifedipine co-medication in
Ticlopidine and clopidogrel [SR 25990C] selectively neutralize ADP patients with atherosclerotic disease. Eur Heart J 1996; 17 (suppl):
inhibition of PGE1-activated platelet adenylate cyclase in rats and rab- 160 [abstract].
bits. Thromb Haemost 1991; 65: 186–90. 49 Weber A-A, Reimann S, Schrör K. Specific inhibition of ADP-induced
30 Schrör K. The basic pharmacology of ticlopidine and clopidogrel. platelet aggregation by clopidogrel in vitro. Br J Pharmacol 1998
Platelets 1993; 4: 252–61. (in press).
Vascular Medicine 1998; 3: 247–251
Downloaded from vmj.sagepub.com by guest on November 7, 2015You can also read