Commentary: Oocyte degeneration after ICSI
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Oocyte degeneration 193
Commentary: Oocyte degeneration after ICSI
J Reprod Stem Cell Biotechnol 1(2):193-209, 2010
Oocyte degeneration following intracytoplasmic sperm injection
(ICSI): A commentary on seventeen years of ICSI experience
Marlane J Angle, PhD, HCLD
Laurel Fertility Care, 1700 California St, Suite 570, San Francisco, CA 94109, United States of
America. Email: drangle@Laurelfertility.com
Disclaimer: The author has nothing to declare.
of practice and training from the older
For many experienced embryologists, learning generation of embryologists who brought this
to do ICSI in the early 1990s was essentially a revolutionary technique into their individual
“self-taught” process. At best, the laboratories.
embryologist was able to observe ICSI for a
short time as a guest in a laboratory already Because fertilization is such a complex
performing the technique, or may have been process and requires several hours before
able to receive “hands-on” training by evidence of fertilization can be documented it
participating in a specialized workshop has been difficult to study cause and effect
(occasionally taught in large university relationships between subtle procedural
laboratories such as Cornell Medical School, changes and increased fertilization rates.
NY). However, after that brief exposure to a Consequently there has developed what could
complicated process, it was the responsibility be termed almost “mystical” beliefs or opinions
of the embryologist to master the technical about which aspect, or what modification, of
subtleties in his or her home laboratory. Since the process guarantees success. Scanning
then, most ICSI techniques have been taught recent responses to a question regarding
to new embryologists within the confines of oocyte degeneration after ICSI posted on
individual laboratories; new embryologists Embryomail (www.embryomail.net) in October
watch more experienced scientists perform the of 2010 can provide insight into what a cross
procedure then imitate the set-up and section of embryologists view as the crucial
processes that they have observed. elements in successful ICSI. Unfortunately,
Observation and subsequent performance, or little scientific evidence was presented to
mimicking, is a classic method for learning support most of these opinions.
complex techniques that require fine motor
skill development. Most embryologists, perhaps by nature, have
been willing to accept the mantle of
In the first years after ICSI’s introduction each responsibility for oocyte survival after ICSI.
practitioner had to develop a protocol that Or, as in many instances of conflict between
would guarantee successful fertilization, and at clinic and laboratory, have had the mantle of
the same time, limit the production of responsibility placed upon them, whether
degenerate or abnormally fertilized eggs. evidence of culpability exists or not.
There has always been a definite learning Consequently, there appears to be a
curve for each new embryologist associated commonly held belief that degeneration and/or
with the acquisition of sufficient skill to abnormal fertilization following ICSI are
penetrate the zona pellucida and the oolemma phenomenon solely dependent upon the
without irrevocably destroying the oocyte. technical skill of the embryologist.
Many embryologists can probably remember Furthermore, there appears to be the belief
months of low fertilization rates followed by a that degeneration or abnormal fertilization
steady climb in success as skills improved. In represents a failure to master the technical
particular, learning to recognize when the subtleties of a delicate procedure. To this
oolemma has been successfully breached is extent, some labs monitor 1 and 3 pronuclear
probably the most significant step in mastery (PN) rates and oocyte degeneration following
of ICSI. Happily, skill transfer to the next ICSI as a quality management indicator.
generation of technical personnel appears to When abnormal fertilization or degeneration
be happening at a much faster rate today rates rise too high the technician is required to
compared to those early days, thanks to years retrain, and demonstrate technical proficiency
Oocyte degeneration 194
to the satisfaction of the Laboratory Director or the cytoplasm into the ICSI microtool, and to
other regulatory body. avoid the spindle which we visualize before
and after injection using the Oosight™
Assignation of this type of quality management (Cambridge Research Instruments) on an
may overlook the primary source of variability Olympus IX71 scope with Hoffman Modulation
within the laboratory that an embryologist is optics, managed using the Oosight™ image
least capable of managing, i.e., the patient. analysis software, (Origio, Mount Laurel, NJ).
While it is certainly incumbent upon each Using the Oosight™ to orient the spindle
laboratory to ensure that the scientists apparatus relative to the ICSI microtool has
handling precious human oocytes are skilled given us satisfactory fertilization rates even
and capable of performing ICSI with a when polar bodies are at any point around the
reasonable assurance of successful figurative clock. Using this rather casual
fertilization, monitoring degeneration rates or approach, our rates of 1PN and 3PN
the formation of abnormally fertilized zygotes fertilizations have been relatively constant over
may not be logical indices to document the years at approximately 1-3% and our
maintenance of skill for the trained ICSI degeneration rates have been fairly low,
scientist. Oocyte degradation as a excluding the occasional random spikes for a
consequence of ICSI may have nothing to do given patient, and coast along at less than 4%
with such technical details as microspikes on year after year.
the ICSI needle; angle of incidence of the
needle, oocyte and dish; straight or angled Addition of the Oosight™ has been the most
tools; presence or absence of HEPES in the recent change associated with ICSI, and has
ICSI medium; holding pipette pressure or any potentially contributed most to our
other of a host of details that might be understanding of what modulates oocyte
attributed to the set-up and performance of survival following ICSI. Approximately 5 years
ICSI. Probably for every detail suggested as ago we began using the Oosight™ routinely
the foundational source of oocyte destruction, during ICSI to monitor placement of the
other scientists could argue that these details spindle apparatus. Due to an impression that
are irrelevant. survival after ICSI seemed to be associated
with the presence or absence of a spindle we
In my laboratory, after seventeen years of recently began to track outcomes more closely
performing ICSI, fertilization rates of rather than simply pooling all injected oocytes
approximately 78% (with a range of 0-100%) for culture. We now record whether an oocyte
appear to have increased little by 2010 contains a spindle and we culture oocytes
compared to where they settled after the initial without a spindle separately from oocytes that
trial-and-error period in the early period of ICSI possess a spindle. We have found that when
in 1993/1994. Over the years we have tried a spindle is present (in 82% of our MII
doing ICSI in media with HEPEs, bicarbonate, oocytes) the degeneration rate is 2.4%. If a
or MOPS and have seen little difference in spindle is absent we see a degeneration rate
outcomes. We have always used needles with of 5.7%. Occasionally, for patients with limited
spikes, and have never tried to rub them off on numbers of MII oocytes and/or high
the holding pipette. We have used angled and percentages of MI oocytes we have tried
straight tools with success, accepted a certain injecting MI oocytes in the hope of getting
amount of “slop” in the angle of approach to something usable, especially if the oocyte has
the oocyte relative to the surface of the dish, a spindle. For these eggs we see that 40% of
and have spent no time at all during set up the oocytes degenerate (4/10) even if a
trying to make sure that the tip of the ICSI spindle is present, but 60% (6/10) degenerate
microtool can be directly inserted into the when the spindle is absent. These
opening of the holding pipette in order to verify observations are recent and very preliminary,
common angles of approach for holding and but trend toward confirming the work from
ICSI tools. Although we have tried all of these David Keefe’s lab (Wang et al., 2001) that
approaches in the past, ignoring them seems suggested that increased rates of
to have minimal effect on fertilization outcome. degeneration tended to occur when the
In addition, we accept the angle of the bevel spindle was absent in an oocyte at the time of
as it comes out of the package and make no ICSI. However, their differences did not reach
effort to place the polar body at 12 o’clock or 6 significance and their degradation rates were
o’clock relative to the bevel. lower than ours for MI oocytes. Our study will
continue in an attempt to substantiate whether
Our only goals during ICSI are to document survival after ICSI is a consequence of the
penetration of the oolemma with movement of
Oocyte degeneration 195
health and developmental competence of the conclusion, but we view it as an intriguing
oocyte. possibility.
Additional information in the literature supports Therefore, it seems logical, based on our
the idea that ICSI degeneration is operator- personal experience and reports in the
independent. Rosen et al. (2006) compared literature to suggest that degradation of
ICSI outcomes for four skilled op operators, oocytes is likely to be independent of the skill
with 6-10 years of experience. No difference of the ICSI scientist, provided the operator is
was seen with regard to oocyte survival. trained, and has demonstrated an appropriate
However, day 3 FSH levels were positively mastery of the technique. This does not deny
associated with degeneration. In addition, the the necessity for appropriate quality control
number of mature oocytes retrieved and the and assumes that each laboratory has
estradiol levels on day of hCG negatively undertaken the correct QC for equipment and
correlated with degeneration. A logistic model tools used during ICSI (such as stage
excluding the ICSI operators predicted the warmers). But, when all other parameters
monthly ICSI degeneration rates similar to have been examined, monitored, tested and
actual degeneration rates for a single operator. found to be within acceptable ranges then
These findings would appear to verify that there must come a time when the embryologist
oocyte degeneration after ICSI is not operator will have to stand back and relinquish
dependent, for a skilled, fully trained scientist responsibility for an outcome they cannot
with several years of experience. control.
Palermo et al. (1996) have reported that References
oolemma characteristic can be correlated with Palermo GD, Alikani M, Bertoli M, Colombero
oocyte survival after ICSI. Oocytes with LT, Moy F, Cohen J, et al. Oolemma
oolemma that ruptured suddenly had a higher characteristics in relation to survival and
rate of degradation compared to oocytes with fertilization pattern of oocytes treated by
oolemma that were easy to pierce or even with intracytoplasmic sperm injection. Hum
oolemma that required multiple attempts to Reprod. 1996; 11: 172-6.
penetrate. We have also seen that oocytes Rosen M, Shen S, Dobson AT, Fujimoto VY,
missing a spindle often rupture immediately McCulloch CE, Cedars MI. Oocyte
upon insertion of the ICSI microtool, degeneration after intracytoplasmic sperm
accompanied by leakage of the cytoplasm into injection: a multivariate analysis to assess
the perivitelline space even prior to its importance as a laboratory or clinical
withdrawing the microtool. This type of marker. Fertil Steril. 2006; 85: 1736-43.
damage probably correlates to Palermo’s Strassburger D, Friedler S, Raziel A,
classification of “sudden breakage.” The Kasterstein E, Schachter M and Ron-El R.
combination of maturation arrest and lack of a The outcome of ICSI of immature MI
spindle apparatus at this juncture in our hands oocytes and rescued in vitro matured MII
seems to correlate with lower survival after oocytes. Hum Reprod. 2004; 19 (7): 1587-
ICSI. 1590.
Strassburger et al. (2004) also Wang WH, Meng L, Hackett RJ, Odenbourg R,
demonstrated impaired performance of MI Keefe DL. The spindle observation and its
oocytes after ICSI with higher degeneration relationship with fertilization after
rates, lower fertilization rates, and higher intracytoplasmic sperm injection in living
multipronuclear rates compared to MII or in human oocytes. Fertil Steril. 2001; 75: 348–
vitro matured MI oocytes that became MII 53.
oocytes prior to injection. Many laboratories
choose not to inject oocytes of this type;
however this group found that these arrested
MI oocytes could fertilize and divide, and one
subsequent embryo gave rise to a normal
pregnancy and healthy delivery. Perhaps
these types of observations justify injecting MI
oocytes, even given their higher propensity to
degenerate upon injection. It may be that MI
oocytes with visible spindles at the time of
injection will prove to be those MI oocytes that
are successful at producing babies. Our data
is too preliminary to support this type of
Oocyte degeneration 196
Oocyte degeneration after intracytoplasmic sperm injection
Martin Wilding PhD1, Antionio Scotto di Frega M.D.1,Genc Kabili
M.D.2,3,Loredana di Matteo B.Sc.1,4,Brian Dale D.Sc.1
1 2
Centro Fecondazione Assistita, Clinica Villa Del Sole, Via Manzoni 15, 80122 Napoli, ITALY; Klinika
‘EGIAN’, Rruga E Kavaje, Ish Parku I Autobuzeve, Tirana, Albania; 3Tirana Maternity Hospital,
Boulevard "B.Curri", Tirana, Albania; 4Facolta Di Medicina E Chirurgia, II Università Degli Studi Di
Napoli, Via Costantinopoli, 16, 80100 Napoli, Italy.
Correspondence: Dr Martin Wilding, Centro Fecondazione Assistita, Clinica Villa del Sole, Via Manzoni 15, 80122 Napoli.
Tel: 081641689. Fax: 0815479251,E-mail: martinwilding@hotmail.com
Disclaimer: The authors have nothing to declare.
Introduction particular cohort of oocytes. Once these
Intracytoplasmic sperm injection (ICSI) is a factors are elucidated, the degeneration of
physical technique whereby a living oocytes after ICSI can also be applied as a
spermatozoa is microinjected into the diagnostic factor for oocyte quality.
cytoplasm of an oocyte to enable the formation
of an embryo which will implant and produce a Mechanism of oocyte degeneration
viable foetus. Although most oocytes survive after ICSI
this process, some degeneration of oocytes The oocyte plasma membrane, as for
does occur. In this commentary, we describe all cell types, is designed to maintain an
the process of oocyte degeneration after ICSI. equilibrium between the cells' inner milieu (the
We further describe equipment and cytoplasm) and the extracellular environment
procedures which can influence the level of (which in the case of human fertilisation would
oocyte degeneration after ICSI. Oocyte be the follicular fluid and fluids of the fallopian
degeneration after ICSI is both a physical and tube). This is required to prevent the
physiological process. In the absence of dissipation of the cell contents, assist in the
physical factors, we describe some creation of energy for use in cell homeostasis
physiological processes which can cause the and development and to act as a barrier to
degeneration of oocytes. These processes pathogens. Cells achieve this through a
often give indications for the cause of infertility, variety of structures. In the human, the oocyte
and the probability of achieving pregnancy in plasma membrane is maintained integral
these patients. through a large actin-tubulin cytoskeleton that
acts as a scaffold to maintain the lipid bilayer
Intracytoplasmic sperm injection (ICSI) has, in place. During the ICSI process, the plasma
since its' development as a tool of assisted membrane is ruptured, leading to a brief influx
reproduction technology (ART), become of extracellular medium. This medium is
probably the major technique in use at the highly toxic to the oocyte since it contains a
present day (Palermo et al., 1995). It is high concentration of sodium and calcium
currently estimated that over 1 million children ions. The oocyte cytoplasm is therefore briefly
have been born with this technique. The depolarised and exposed to a transient peak
technique is applicable to almost all male of calcium. Successful oocyte repair after ICSI
factor pathologies in ART including semen then depends on the rapid restoration of the
samples devoid of motility, samples extracted plasma membrane and the ionic equilibrium
from testicular biopsies and in some cases between internal and external milieu. As can
immature spermatids where no mature therefore be expected, several factors can
spermatozoa are present. Therefore, almost contribute to the successful outcome of the
all male factor infertility diagnoses can now be ICSI technique.
treated with ICSI. However, the ICSI
technique does not result in 100% fertilisation Microtools and equipment
of oocytes injected with the technique. ICSI is a highly delicate technique in
Oocytes often remain unfertilised, or which a glass pipette is effectively inserted into
degenerate following the technique. Although an oocyte and a single spermatozoa
the degeneration of oocytes after ICSI is often deposited. None of these objects can be seen
attributed to the operator, other factors can under the naked eye since the oocyte is
influence the level of oocyte degeneration in a 0.08mm in diameter, the tip if the pipette
Oocyte degeneration 197
0.005mm in diameter and the spermatozoa decondense (observed through the presence
roughly 0.003mm in width. Therefore, of oocytes with 2 polar bodies but no
dedicated equipment and microtools are pronuclei, or a single pronucleus and 2 polar
necessary to permit the manipulation of these bodies). Other than the positioning of
objects with a fine degree of control. Initially, microtools, the operator should know how to
dedicated equipment was not available for set up and error check the microinjectors.
ICSI and therefore operators had to adapt This is because a great deal of control of the
similar equipment for this technique. This microtools is required in order to correctly
initially led to a greater level of oocyte complete the microinjection process. Lack of
degeneration after ICSI than the current day. control of the quantity of fluid injected into the
Now however, specific equipment can be oocyte can lead to oocyte lysis through the
purchased. An ICSI station generally consists mechanism described above. In fact,
of an inverted microscope equipped with up to microinjectors are usually oil filled to enable
400x magnification (i.e. 40X objective) to fine control of the sperm position. Leaks, or
which is attached a set of micromanipulators air pockets in the system can cause a loss of
and microinjectors providing the control of control, and therefore the injection of an
oocytes, microtools and the injection process. excess quantity of liquid into the oocyte
Most microscope manufacturers (Nikon, cytoplasm, with consequent degeneration. In
Olympus, Zeiss) offer suitable systems. practice, ICSI operators are usually trained for
Microtools for ICSI consist of a fine bevelled long periods prior to clinical practice in order to
pipette used to capture spermatozoa and ensure that these factors are eliminated in the
insert these into the oocyte cytoplasm (ICSI ICSI routine. Countries such as the UK for
pipette, usually 5-8um in diameter at the tip), example require operators to be licensed by
and a larger micropipette used to maintain the the controlling authority (Human Fertilisation
oocyte during manipulation (holding pipette, and Embryology Authority in the UK). In
usually with outer diameter 100um and inned countries where no licensing authority exists,
diameter 15-20um, blunt ended). Microtools operators are always required to have trained
are generally purchased from specialised for at least a year before clinical practice and
manufacturers (such as COOK, ORIGIO etc) all operators are closely monitored for
which today generally offer a range of technique and results. Therefore, operator
products for assisted reproduction. skill and technique are usually at a sufficient
level to complete the ICSI procedure without
Operator skill and technique excess oocyte damage (
Oocyte degeneration 198
brittle (and hence easily lysed) oocytes to Oocyte quality therefore can be defined as the
extremely flexible membranes which are physiological ability to recover after a
difficult to rupture during ICSI (Palermo et al., technically correct ICSI procedure. Oocyte
1996, Wilding et al., 2007). The cytoskeletal physiology is however influenced both by the
system that maintains the integrity of the patient characteristics and the preparation of
oocyte plasma membrane depends on patients for the ICSI cycle. Negative
microtubules (tubulin protein) and in particular influences on oocyte quality are known to be
microfilaments (composed mainly of actin). caused by conditions such as endometriosis or
Actin is a major component that maintains the polycystic ovarian syndrome. However, the
membrane together. Dissolution of actin controlled ovarian hyperstimulation (COH)
filaments with cytochalasin B renders the protocol itself can also determine oocyte
human oocyte membrane highly elastic quality (Palermo et al., 1996). This is because
without causing its' ultimate rupture, cytoplasmic maturity is often not completely
suggesting that the level of polymerisation of correlated with nuclear maturity (i.e. a mature,
actin filaments determines the elasticity of the metaphase II oocyte can often have immature,
membrane (lower levels of polymerisation germinal vesicle-like cytoplasm and hence a
leading to more elastic membranes). These brittle plasma membrane). Therefore, care
data suggest that the meiotic state of human should be exercised by the clinician to ensure
oocytes controls the level of actin COH protocols follow physiological
polymerisation and therefore the elasticity of mechanisms of oogenesis as closely as
the plasma membrane. The data suggest that possible.
actin polymerisation is influenced by the
oocyte cytoplasm, suggesting in turn a link Conclusions
between oocyte degeneration after ICSI and Oocyte degeneration after ICSI is a
oocyte maturity. physiological as well as physical process. The
quality of equipment, microtools and ICSI
Apart from the influence of the cytoplasm on practitioners is fundamental to the positive
the elasticity of the plasma membrane outcome of the technique. However, oocyte
suggesting a link between oocyte quality and quality is also a determinant. Oocyte quality
degeneration after ICSI, oocyte quality can can be defined in terms of the properties of the
also be defined in terms of the physiological oocyte plasma membrane, as well as the
response to the ICSI process. As mentioned ability of the oocyte to recover from the injury
above, a small quantity of the external milieu sustained during the process. In this way,
enters the cytoplasm during ICSI – either both the preparation of the patient for the ICSI
through the rupture of the plasma membrane technique as well as the physical completion
or injected together with the spermatozoa. of he process are fundamental determining
This milieu consists of extracellular medium factors.
(i.e. high sodium, low potassium and high
calcium with respect to the cell cytoplasm). References
This causes a depolarisation of the cell Palermo GD, Alikani M, Bertoli M, Colombero
together with a rapid increase of cytoplasmic LT, Moy F, Cohen J, Rosenwaks Z.
calcium. The ionic polarity of all cells is Oolemma characteristics in relation to
fundamental to cell physiology since the survival and fertilization patterns of oocytes
polarity provides a useful gradient for rapid treated by intracytoplasmic sperm injection.
transport of nutrients into the oocyte cytoplasm Hum Reprod. 1996 Jan;11(1):172-6.
as well as other processes. In the absence of Palermo GD, Cohen J, Alikani M, Adler A,
this gradient, cells rapidly degenerate. Cells Rosenwaks Z. Intracytoplasmic sperm
remove cytoplasmic sodium and retain injection: a novel treatment for all forms of
cytoplasmic potassium through a highly active male factor infertility. Fertil Steril. 1995
pump on the plasma membrane. Since this Jun;63(6):1231-40.
pump requires energy, the activity of the pump Wilding M, Di Matteo L, D'Andretti S,
is highly influenced by the ability of the cell to Montanaro N, Capobianco C, Dale B. An
create energy, and hence cell quality. Calcium oocyte score for use in assisted
ions are removed from the oocyte cytoplasm in reproduction. J Assist Reprod Genet. 2007
a similar way to sodium ions. The presence of Aug;24(8):350-8.
high levels of calcium in the oocyte cytoplasm
would also lead to oocyte degeneration and
these are removed by active transport to the
mitochondria or endoplasmic reticulum.
Oocyte degeneration 199
Oocyte degeneration following ICSI
Bryan Woodward PhD FRCPath; Locum Clinical Embryologist, UK
Correspondence: Dr Bryan Woodward, Email: theeggman68@hotmail.com
Disclaimer: The author has nothing to declare.
Introduction
Clinical ICSI is an increasingly common require a higher than usual negative pressure
treatment choice to allow fertilisation in vitro. to be exerted on the IP, resulting in a large
The technique can be applied to treat male volume of cytoplasm entering the IP. Both
infertility, to fertilise frozen-thawed oocytes, to types of oocyte are prone to a higher
prevent polyspermy and to avoid sperm-zona degeneration rate after ICSI. Sibling oocytes
binding for embryos scheduled for PGD for may display similar properties. The use of
monogenetic diseases. Some IVF clinics even laser-assisted ICSI has been reported for
advocate the use of ICSI for all patients in patients with atypical oolemma flexibility
order to maximise fertilisation rates (Nygren & (Demirol et al., 2006). This method utilises a
Anderson, 2002). laser to cut a hole into the zona immediately
before IP insertion. The IP is then passed
The aim of ICSI is to deposit a sperm cell through the hole and into the oolemma as per
safely within the cytoplasm of the oocyte conventional ICSI, thereby reducing oocyte
without causing any damage. The technique compression and the risk of damage.
involves inserting an injection pipette (IP)
through the zona pellucida in order to puncture Operator skill & learning curve
the oolemma. Once the IP has been inserted Operator-induced damage can be introduced
at least half way into the oocyte, a negative during oocyte preparation and during the
pressure is usually exerted to the IP to actual ICSI procedure. For cumulus
aspirate the oolemma into the lumen. This denudation prior to ICSI, the duration of
then causes a membrane breach, which is exposure to hyalurodinase needs to be as
commonly observed as a rush of cytoplasm short as possible and should include sufficient
into the IP. The cytoplasm is then injected rinsing steps to ensure thorough removal of
back into the oocyte together with a sperm, the acid post-denudation. The hyalurodinase
and the IP is withdrawn. For successful ICSI, concentration also needs to be considered, as
the breach in the oolemma must fully heal, the stock solution may need to be diluted prior
often leaving a characteristic funnel shape in to oocyte exposure. Both over-exposure and
the cytoplasm. However, if oolemma healing excessive concentration can adversely affect
is incomplete, oocyte degeneration is highly oocyte quality.
probable. This commentary examines various
factors that might influence oocyte survival Since cumulus removal also requires
before and during injection. mechanical manipulation of the cumulus
oocyte complex, the lumen size of the
Oocyte quality denuding pipette needs to be considered.
The intrinsic nature of different oocytes from Aspiring an oocyte surrounded by several
individual patients means that some oocytes tightly bound layers of cumulus cells into a
are less likely to survive the ICSI procedure. denuding pipette with a small lumen (e.g.
Metaphase II oocytes vary in physical 135µm diameter) may exert excessive stress
characteristics such as shape and size, the leading to zona breakage. Some
thickness and regularity of the zona, the size embryologists therefore use several
of the peri-vitelline space, the size and shape denudation pipettes of different lumen sizes to
of the first polar body, and the evenness of ensure minimal stress on the oocyte during
cytoplasmic granularity. Other attributes such gradual removal of the cumulus cells.
as oolemma elasticity cannot be assessed
until they are dynamically tested, most During cumulus denudation and actual ICSI,
probably in response to the initial insertion of the oocyte temperature should be maintained
the IP. at 37°C. Whilst some thermal fluctuations are
inevitable during the transfer of oocytes
Poor quality oocytes may have fragile zonae between dishes, the heated stages should be
and oolemmas which break easily upon IP adjusted such that the temperature of the
insertion. Other oocytes may have thicker media in the droplets is 37°C. This may
zonae and overly resistant oolemmas which require a slight increase to the heated stage
Oocyte degeneration 200
temperature to account for thermal loss due to further cytoplasm into the IP ‘to ensure a
conduction through the base of the dish in definite breach’. However, this may not be
which the oocytes are held. best practice as aspiring too much cytoplasm
may cause significant intracellular damage, as
Some embryologists perform any ‘out of the well as possibly creating a dangerously large
incubator’ manipulations using buffered breach in the oolemma.
medium to maintain pH. However, depending
of practitioner skill, both cumulus removal and Speed of injection and withdrawal is another
ICSI can be performed in pre-equilibrated variable. If the motion is too fast, then the
culture medium without a buffer. This relies on ICSI may not be fully completed before IP
efficient timing of the procedures to ensure the withdrawal. Conversely, if the motion is too
pH does not change. This has the possible slow, the risk of cytoplasmic leakage from the
advantage of not exposing the oocytes to a induced membrane wound may increase.
change in medium type, and ensures the
procedures are time-efficient. A possible Adaptations to the conventional ICSI
disadvantage of using buffered medium is technique include ‘priming ICSI’, whereby the
prolonged exposure of the oocytes to the IP is initially inserted into the oolemma to
buffer during micromanipulations, which may prime the membrane without penetration
adversely affect the oolemmas. (Shen et al., 2003). The IP is then withdrawn
and a second insertion is used to penetrate
As with any microsurgery, there is a skill level the oolemma in a line parallel to the first
that needs to be reached in order to perform insertion. The ‘pre-stretching’ of the oolemma
ICSI to an acceptable standard. Whilst the may aide a successful breach as a result.
primary ICSI key performance indicator (KPI)
is oocyte survival post-injection, other KPIs Another technique is piezo-ICSI. This involves
such as fertilisation rate, embryo development puncture of the zona using a flat-tipped IP
and implantation rate need to be considered. moved by a piezo-electrically activated impact
Changes to the ICSI technique by different device called a piezo-drill. The puncture is
embryologists may induce more subtle caused by a sudden piezo-pulse of adjustable
differences to the injected oocytes beyond frequency, amplitude and duration. Piezo-ICSI
survival. Variation between embryologists reduces oocyte deformation during ICSI and
performing ICSI is a controversial topic. The has been shown to improve survival rates in
survival rate after ICSI has been reported as mouse (Kimura & Yanagimachi, 1995). Piezo-
both dependent and independent of the ICSI has also been used clinically but is a less
embryologist, whilst a significant inter- common technique compared to conventional
embryologist difference in the fertilisation rate ICSI (Yanagida et al., 1999).
has been reported (Shen et al., 2003).
Microtools
The ICSI technique Poor workers often blame their tools, thus it is
Differences to ICSI technique may result in essential that embryologists have good tools
under-injection (i.e. not injecting the full to perform ICSI. There are various
amount of cytoplasm or the sperm) and over- commercially available IPs manufactured to
injection (injecting additional fluid/PVP into the different specifications (lumen sizes, angles,
oocyte). Cytoplasmic leakage or sperm ‘falling bevels, and with spiked or non-spiked tips).
out’ of the injection site may be observed with The IP diameter affects ICSI, since a small
the former, whilst large fluid-filled spaces diameter minimises disturbance, whilst a large
within the oocyte may result with the latter. diameter causes more disruption and
increases the likelihood of oocyte damage. IP
Depth of IP insertion needs consideration. diameter is dictated by the size of the sperm to
There is a risk that the distal oolemma on the be injected and is a standard size for most
opposite side of the oocyte may be commercially available IPs for clinical ICSI.
accidentally breached if the IP is inserted too
far into the oocyte, leading to an irreparable The IP angle depends on individual
membrane wound. Conversely, if the depth of preference, and should not affect lysis
insertion is too shallow, then the oolemma provided the angle of penetration is
may not be sufficiently stretched to permit a satisfactory. Optimal penetration should be
non-lethal breach. perpendicular to the equator of the oocyte.
This can be tested by moving the IP onto the
Some embryologists observe the initial zona, exerting a small pressure onto the
oolemma breach, but then continue to aspire oocyte and observing equal deformation in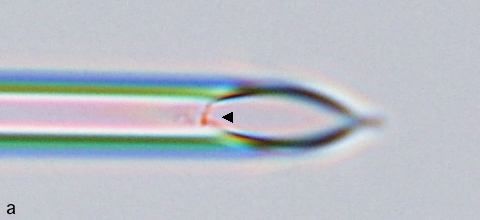
Oocyte degeneration 201
both halves of the oocyte above and below the and down the IP into fresh medium prior to
IP. ICSI can be performed at other latitudes, injection. It may be possible to clean the
but the risk of irreparable breaches is more outside of the IP by inserting it into the lumen
likely with increasing distance from the of the HP. However, if there is any doubt as to
equator. the cleanliness of the IP, then it should be
replaced prior to performing the ICSI.
The holding pipette (HP) should be of
sufficient size to secure the oocyte during Conclusion
ICSI, without deforming the oocyte shape. At present ICSI is typically associated with
However, a recent study of interspecies ICSI degeneration of a significant percentage (5-
using mouse oocytes reported use of a 10%) of the treated oocytes (Mansour et al.,
modified HP with a trumpet-shaped opening 2009; Richter et al., 2006). This commentary
(Lyu et al., 2010). This enabled the oocyte has discussed ways to minimise degeneration
shape to be partially deformed by aspiration after ICSI, including adjusting the injection
into the HP, thereby allowing a deeper technique to account for oocytes of differing
injection in the oocyte. This significantly quality. An evaluation of all oocyte
improved oocyte survival and fertilisation in a independent factors that might affect ICSI is
species with a notoriously high degeneration recommended to optimise survival rates.
rate after conventional ICSI.
References
Equipment Demirol A, Benkhalifa M, Sari T et al. (2006)
The ICSI workstation should be located in an Use of laser-assisted intracytoplasmic
isolated part of the IVF laboratory to minimise sperm injection (ICSI) in patients with a
distraction away from lab traffic and excessive history of poor ICSI outcome and limited
airflow. Minor vibrations during ICSI can metaphase II oocytes. Fertil Steril.;
increase the risk of oocyte degeneration. 86(1):256-8.
Thus, if the workstation is prone to vibrations, Kimura Y & Yanagimachi R. (1995)
then consideration should be given to Intracytoplasmic sperm injection in the
increasing stability via an anti-vibration table. mouse.Biol .Reprod.; 52(4):709-20.
Lyu QF, Deng L, Xue SG et al. (2010) New
The workstation should be regularly serviced technique for mouse oocyte injection via a
to ensure efficient control over all movements modified holding pipette. RBM Online.;
associated with micromanipulation. If the 21(5):663-6.
syringes become ‘looser’ this should be Mansour R, Fahmy I, Tawab NA et al. (2009)
immediately addressed, as this may lead to Electrical activation of oocytes after
less control of the sperm and cytoplasm intracytoplasmic sperm injection: a
movement in the IP. Similarly, complete controlled randomized study. Fert.Steril.;
control over micrometre movements in the x-, 91(1):133-9.
y- and z-planes is needed to allow optimal Nygren KG & Andersen AW (2002) The
micromanipulation.
European IVF‐monitoring programme (EIM)
for the European Society of Human
Other factors Reproduction and Embryology Assisted
Occasionally it may be necessary to re-inject reproductive technologies in Europe, 1999
an oocyte, if sperm deposition was Results generated from European registers
unsuccessful during the initial ICSI. A second by ESHRE. Hum Reprod.; 12:3260–3274.
ICSI may increase the risk of oocyte lysis, Richter KS, Davis A, Carter J et al. (2006) No
since the membrane may still be in a state of advantage of laser-assisted over
repair following the first injection. Rather than conventional intracytoplasmic sperm
immediate re-injection, a possible strategy to injection: a randomized controlled trial.
maximise survival might be to allow the oocyte J.Exp.Clin.Assist.Reprod.; 3: 5.
a period of time to recover before performing a Shen S, Khabani A, Klein N et al. (2003)
repeat ICSI. Statistical analysis of factors affecting
fertilization rates and clinical outcome
Care should also be taken to only inject the associated with intracytoplasmic sperm
sperm during ICSI using a clean IP. This is injection. Fertil Steril.; 79(2):355-60.
particularly important when selecting sperm Yanagida K, Katayose H, Yazawa H et al.
from a testicular biopsy preparation which may (1999) The usefulness of a piezo-
be laden with cellular debris that can stick to micromanipulator in intracytoplasmic sperm
the IP. It may be worthwhile subjecting the injection in humans. Hum Reprod.;
selected sperm to several repeated washes up 14(2):448-53.
Oocyte degeneration 202
Oocyte degeneration following ICSI
Dianna Payne, PhD
Director, The Pipette Company Pty. Ltd., Unit 13, 22 Ware Street, Thebarton, South Australia 5031
Telephone: +61-8-81520266, Facsimile: +61-8-81520277; Email: dianna@pipetteco.com
Correspondence: Dr Dianna Payne, Email: dianna@pipetteco.com
Disclaimer: The author declares her involvement in The Pipette Company that manufactures and markets ICSI microtools.
Editor’s Comments: This Commentary is accepted on the basis of its scientific merits irrespective of the author’s
involvement in commerce.
Introduction
ICSI is an invasive and crude technique. the oolemma so that the position of the tip and
During ICSI the oocyte is pierced by a large the movement of the oolemma and cytoplasm
hollow needle, approximately 5% of its can be clearly visualised during ICSI. If the
diameter, and 0.5% of the oocyte volume is oolemma cannot be seen as a clearly
drawn out and randomly replaced. The delineated fine line then the optical system is
oolemma, having been breached, reforms. If
the oocyte were simply an amorphous mass of inadequate, or the focus is incorrect.
cytoplasm, then this would not invite comment,
however, the oocyte does have structure Hoffman Modulation Contrast (HMC) was
(Figure 1). The granular area moves around invented in 1975 to mimic the optical image
the unfertilized oocyte with a regular achieved with the older, but more expensive,
periodicity; cytoplasmic organelles and Differential Interference Contrast (DIC). HMC
pronuclei are attached to a cytoskeleton, and has the advantage of being able to be used
drawn in centrally as pronuclear formation with plastic culture dishes, and is widely used
proceeds (Payne et al, 1997). These carefully
for ICSI, whereas DIC requires a glass
orchestrated events require precise
organisation and control, both spatial and substrate. Both require careful setting up to
temporal, to proceed correctly. Rough injection achieve an optimal image. DIC has the
can cause disturbance in the structure of the advantage of having a narrower depth of field
cytoplasm, and any force exceeding the elastic and thus the optical section achieved when the
limit of the membrane will cause the oocyte is properly focused allows for finer
membrane to sheer and the contents of the judgement during the course of ICSI because
oocyte to leak out.
the cytoplasm and plasma membrane can be
There may be many causes of oocyte
more easily delineated. The image quality
degeneration, however, this commentary will
obtained with DIC is superior to HMC and
only address technical aspects of ICSI which
therefore has always been my choice.
may lead to the uncontrolled mechanical
rupture of the oolemma, leakage of cytoplasm Alignment of pipettes
into the perivitelline space and lysis of the Pipettes should be set up and aligned so that
oocyte. a straight line can be drawn through the tip
sections of both the holding and injection
Quality of the image
pipette when viewed through the microscope.
Successful ICSI depends on carefully
This ensures that, when the injection pipette is
controlling the process, and that in turn
pushed into the oocyte, it is not entering at an
depends on being able to clearly see what is
angle relative to the holding pipette, causing
happening. Undue distortion of the oocyte,
increased tension to be placed on the
aspirating too much cytoplasm, and rough
oolemma and increasing the likelihood of
uncontrolled injection all lead to an increase in
tearing the oolemma. Furthermore, if they are
oocyte lysis, and this can occur when image
not in line, the oocyte may roll off the holding
quality is poor. The point of the injection
pipette must be visible in the same plane as pipette as the injection pipette is pushed into
the oocyte, and once again, the oolemma
stretches and is more liable to rupture.Oocyte degeneration 203
Similar tension occurs if the bent tip of the probability that it will not successfully re-form.
holding pipette is not parallel to the bottom of Positioning the sperm at the very tip of the
the Petri dish. More significantly though, pipette means that less injection vehicle is
holding the oocyte will become problematic, as injected, and also means the sperm is more
the bottom of the dish prevents the oocyte likely to enter the oocyte before the oolemma
from sitting squarely on the holding pipette. has healed.
To hold the oocyte securely therefore, higher
suction has to be used, and a small portion of Volume of injection vehicle
the oocyte is often sucked into the holding PVP is often used to slow the movement of the
pipette. This increases the tension in the sperm so that immobilization and capture can
membrane surrounding the oocyte and thus, be more easily performed. Inevitably, some
when the injection pipette is pushed against PVP will enter the oocyte during injection. In a
the oolemma, it may rupture. study of 16,500 injected oocytes over the
course of 5 years, we visually estimated the
These may seem to be relatively minor amount of PVP injected scored it as 0, 1 (~3
considerations when doing many ICSI pl), 2 (~10 pl) or 3 (~20 pl). This was
procedures in a day, however, those oocytes correlated with oocyte lysis rates, embryo
with slightly fragile membranes will be the first usage and implantation rate. While oocyte
to succumb if the pipettes are poorly aligned. lysis increased significantly as more PVP was
Careful alignment of pipettes not only makes injected, embryo usage and implantation rate
the technique much easier, but increases the of the surviving oocytes was not different. We
chance of most, if not all, oocytes surviving. concluded that the increase in oocyte lysis rate
was due to a more difficult injection which was
ICSI technique reflected by the amount of PVP injected into
ICSI is a three dimensional process that takes the oocyte and subsequent disturbance of the
place within a two dimensional framework. It cytoplasm, or trauma to the oolemma and not
is a challenging technique to master and the presence of PVP per se (Payne et al,
comes with its own set of unique problems, not 1998). It is inevitable that some oocytes will
least of which is aligning and using pipettes in be more difficult to inject than others, but
three dimensions. The key to a successful careful control while returning the aspirated
injection is getting an immobilised sperm to cytoplasm into the oocyte may reduce
reside in the body of the oocyte with an intact cytoplasmic and/or oolemma disturbance and
oolemma and very little disturbance created in thereby prevent oocyte lysis.
the body of the oocyte (Figure 1). All
movements of the injection pipette should be Pipettes
smooth; suction should be well controlled; the The quality of micromanipualtion pipettes is of
exact moment of membrane breakage paramount importance to the success of ICSI,
identified and suction immediately stopped; and the design and quality of both injection
the sperm should be injected into the oocyte and holding pipettes can affect outcomes. This
smoothly and quickly, and the injection pipette is often not considered or forgotten.
withdrawn evenly. Jerky movements of the
Injection pipettes – spikes and bevels
injection pipette place undue stress on the
The conformation of the spike on injection
oolemma and may exceed it’s elastic limit. pipettes is particularly important. The spike
Allowing a lot of cytoplasm to be withdrawn needs to be sharp enough to penetrate the
from the oocyte, by not identifying when the zona pellucida, without causing undue
oolemma has broken, increases the probability distortion of the oocyte, but not so sharp that it
that the oolemma will re-form before the sperm will immediately pierce the oolemma. I have
has been injected. This necessitates re- examined injection pipettes under high
magnification (500X), which have then been
aspiration of the cytoplasm to break the
used for ICSI. Those pipettes that had very
oolemma again, otherwise the sperm and fine spikes (Figure 2) universally caused
cytoplasm will be injected into an invagination oocyte lysis. Very fine spikes can be
and not into the oocyte cytoplasm. Each time visualised using DIC, but HMC, while suitable
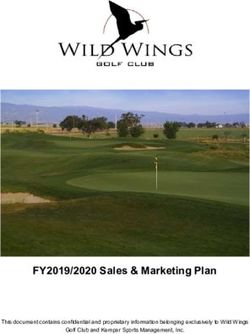
the oolemma is broken increases the for doing ICSI, does not have sufficientOocyte degeneration 204 Figure 1. A photomicrograph of an oocyte after ICSI using DIC at 200X. A sperm (S) is lying in the cytoplasm surrounded by a small pool of injection vehicle (P). The invagination (I) is bound by a re- formed oolemma (). The lower left quadrant of the oocyte has a more granular appearance (G) and the first polar body (PB) has fragmented.
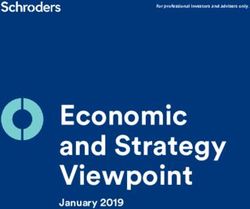
Oocyte degeneration 205 Figure 2. An injection pipette with a very long sharp spike is shown open-faced (a) and in profile (b). The fine spike almost disappears (), but would cause oocyte lysis if used for ICSI. These micrographs present an extreme case, but even pipettes with short but very fine spikes will cause similar problems.
Oocyte degeneration 206 Figure 3. An injection pipette with a jagged trailing edge () in open face (a) and profile (b). The jagged edge is almost impossible to see in profile.
Oocyte degeneration 207 Figure 4. An injection pipette with a blunt spike () shown open-faced (a) and in profile (b). The very blunt tip is difficult to distinguish in profile and only appears to be slightly square in profile. resolving power to adequately assess spikes under these conditions. The classic ICSI on injection pipettes. On the face of it, a very technique has been to force the oolemma to fine spike should aid in the penetration of the break, possibly at a labile point, as the zona pellucida and minimise oocyte distortion, membrane is being aspirated back into the however, a very fine spike will cut the injection pipette. As the cytoplasm is being oolemma on contact, and the oocyte returned to the oocyte, the pressure on this cytoplasm will immediately leak out. The part of the membrane is released and the oolemma has no opportunity to heal itself lability in this area of the membrane allows for
Oocyte degeneration 208
rapid melding. As the oolemma is drawn into inadequate washing, the pipette adheres to
the injection pipette it forms a sharp “V” lipid in the oolemma, and also to membrane-
around the shaft of the pipette. The moment bound organelles such as endoplasmic
the oolemma ruptures, it relaxes around the reticulum and Golgi. If organelles are drawn
pipette. In an oocyte in which the oolemma out of the oocyte with the injection pipette as it
has been pierced prior to suction by a fine is withdrawn from the oocyte, the oolemma will
spike, the oolemma will not become taut not be able to heal around the extruded
around the injection pipette. This oocyte will organelles. The pipette will also adhere to the
almost certainly lyse. It is possible to plasma membrane of the sperm. If the sperm
circumvent the problem of fine spikes, prior to is stuck to the wall of the pipette, and the
injection, by pressing the point of the injection cytoplasm has to be drawn in and out of the
pipette against the holding pipette and pipette several times to dislodge the sperm,
breaking the very tip of the spike away. then again, the oolemma may not have a
However, it is also possible to be over zealous chance to heal.
and the injection pipette can be badly blunted
(Figure 4), causing its own set of problems. A relatively parallel taper for at least 100
From 1993-1999, our ICSI laboratory routinely microns back from the tip of injection pipettes
broke off long fine spikes, and the oocyte lysis is important for good fluid control, and clear
rate was less than 4%. There are laboratories visualization of the sperm. If the taper of the
in which this is still being done, however, this pipette is too steep, then suction may be
is unnecessary with good quality injection “whooshy” and difficult to control. This in turn
pipettes. may result in too much cytoplasm being
aspirated such that the oolemma cannot heal
The bevel on injection pipettes is also and oocyte lysis occurs.
important. Technical difficulties during beveling
can give rise to pipettes with a jagged bevel Holding pipettes
trailing edge (Figure 3). The sperm tail can The holding pipette should hold the oocyte
catch on the rough area making aspirating the gently, but securely, during injection. Pipettes
sperm difficult, and this roughness can also with a large flat face, slightly smaller in
catch cytoplasmic organelles as they move diameter than that of the zona intact oocyte,
into the injection pipette. Most importantly provide added stability and prevent undue
however, it can cause the oolemma to tear as distortion of the oocyte during ICSI. Ensuring
it is stretching over the sharp irregular surface. that the oocyte is in contact with the petri dish
This defect is very difficult to see in profile gives a second point of support and increases
(Figure 3b), the only orientation that can be the stability of the oocyte during injection. This
viewed during ICSI, but will present as a can prevent the oocyte rolling off the pipette
slightly “sticky” pipette, with an increased rate during injection, and reduces tension in the
of oocyte lysis. oolemma that may result in rupture and oocyte
lysis.
Blunt injection pipettes (Figure 4a) will not
penetrate the zona pellucida easily, and Conclusions
increase the distortion of the oocyte during ICSI requires great skill and clinical outcomes
ICSI. Even very blunt spikes are not easily can be easily compromised by poor
identified in profile (Figure 4b), and the spike equipment, poor alignment of pipettes and
looks slightly square rather than pointed. poor technique. Being unable to clearly
Increased distortion of the oocyte during ICSI visualise the gametes and pipettes, or the
increases the rate of oocyte lysis. exact point of contact the injection pipette
These three manufacturing defects are not makes with the plasma membrane, using poor
easy to identify in the laboratory, as once the quality pipettes, having an unstable oocyte
injection pipette is set up for ICSI, it can only that is subject to distortion during ICSI, and not
be viewed in profile. Inspection of pipettes knowing when the membrane has ruptured
prior to ICSI may reduce the likelihood of can all contribute to an increased oocyte lysis
unsuitable pipettes being used, but in practice, rate.
this is time consuming and should not be
necessary if good quality injection pipettes are References
used. Payne D, Flaherty SP, Barry MF, Matthews
CD. Preliminary observations on polar body
Injection pipettes - other considerations extrusion and pronuclear formation in human
If the glass used to manufacture injection oocytes using time lapse video
pipettes is lipophilic, usually as a result ofOocyte degeneration 209 cinematography. Hum Reprod. 1997; 12: 532- 541 Payne D, Goodwin J, Flaherty SP. The effect of polyvinylpyrrolidone on fertilization, embryo quality and implantation rate. Hum Reprod. 1998; 13 (Abstract Book 1): 219.
You can also read