Common toxicity management guidelines - Authors Version (date) Review date Dr Hamish Sinclair
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

EGFR targeting tyrosine
kinase inhibitors.
Common toxicity management guidelines.
Dr Hamish Sinclair
Authors
Dr Juliet Brock
Version (date)
1.0 (July 2020)
Review date
July 2023
1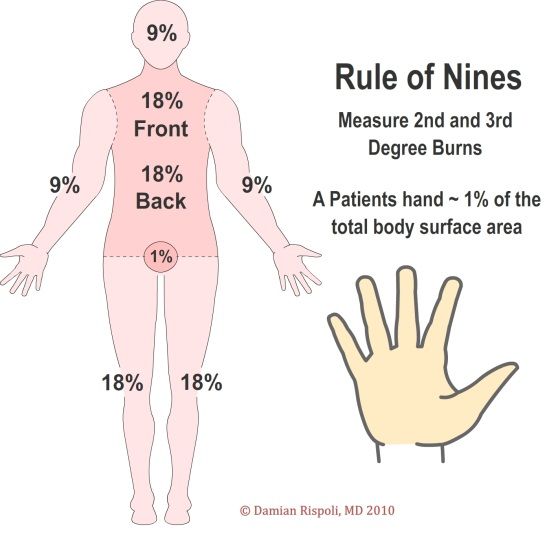
Overview
These guidelines cover the use of the following EGFR targeted tyrosine kinase inhibitors licensed for
use in EGFR positive non-small cell lung cancer.
• Afatinib (Giotrif)
• Erlotinib (Tarceva)
• Gefitinib (Iressa)
• Dacomatinib (Vizimpro)
• Osimertinib (Tagrisso)
The most common dose limiting toxicities are covered in these guidelines but less common adverse
events are not covered. For information on these, please consult the relevant SPC.
Drug Side effect frequency (Any grade / Grade 3+)
Skin toxicity Paronychia Diarrhoea Stomatitis ALT elevation
Afatinib (1) 80% / 7.5% 58% / 11% 90% / 14% 30% / 4% 11% / 2.4%
Erlotinib (2) 75% / 8% 4% / 0% 54% / 6% 13% / 1% 18% / *
Gefitinib (3) 70% / 3-13% 32% / 1% 34-50% / 1-4% 22% / 0% 60% / *
Dacomatinib (4) 77% / 24% 66% / 8% 87% / 8 % 70% / 5% 24% / 0%
Osimertinib (5) 47% / 1% 31% / 0.3% 49% / 1.2% 20% / 0.2% 5% / 1%
Concurrent medications
An up to date medication history must be taken prior to commencing therapy. Patients should be
encouraged to update the oncology team on any new or additional medications/supplements.
Metabolism.
The EGFR TKI’s are metabolised by the cytochrome P450 isoenzymes and their metabolism will be
affected by inhibitors and inducers (See relevant SPC for details).
Gastrointestinal absorption
Absorption of Erlotinib, Gefitinib, Dacomatinib is significantly reduced by drugs which lower gastric
pH. These drugs should be avoided if possible. There is no known effect on Afatinib or Osimertinib.
Proton pump inhibitors (Omeprazole, lansoprazole): Should be converted to Ranitidine. *there is
currently a shortage of Ranitidine and H2 antagonists. If gastric protection is required, discuss with
pharmacy regarding alternatives. If PPI use is unavoidable then advise patient to take their TKI 2
hours prior to proton pump inhibitor.
Ranitidine: Patients should be advised to take their TKI 2 hours before or 10 hours after Ranitidine.
Antacids (e.g Gaviscon,): If required should be taken 4 hours prior or 2 hours after TKI
administration
2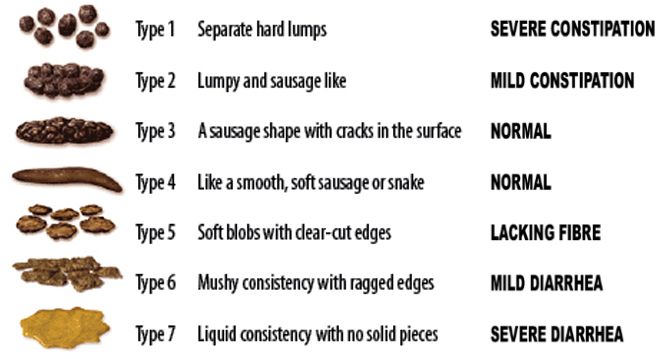
Skin toxicity
Adverse skin reactions are very common and range from mild dry skin and puritis to papulopustular
eruptions. (6,7)
Rashes should be graded using
• Body surface area (BSA) affected (Rule of 9s)
• Impact on Activities of daily living
• Symptoms (Itching, pain)
• Presence/absence of infection
Advice to patients:
• Avoid sun exposure (Use SPF 30+ sunscreen or
cover affected areas)
• Use regular non-scented moisturisers on
affected areas
• When washing, use tepid water and
mild/unscented soap or alternatively use soap substitute (e45/diprobase etc)
• Avoid use of over the counter acne treatment (e.g Benzoyl peroxide) as these may worsen
the rash
• Avoid skin care products containing alcohol
• Reassure patients that skin toxicity is common and manageable.
• Warn patients prior to commencing treatment that management of skin toxicity can involve
a dose reduction and this will not impair the efficacy of their treatment.
Development of an acneiform/papuloustular rash (see examples in pictures below) often occurs
within the first 2-4 weeks of treatment.(8)
Pictures – Lacouture M (2013)
3
Grade Symptoms/ Signs Management
Grade 1 • 7 days then hold TKI and treat
as grade 3, liase with consultant regarding dose reduction.
Grade 3 • >30% BSA 1. Hold TKI
• Limiting self-care ADLS 2. As per grade 1 and 2
• Itching/pain ✔ 3. If pustular rash then trial oral antibiotics
• Infection ✔(localised) • Minocycline 100mg OD for 4 weeks (consider long
term use)
4. If evidence of infection send swab for culture
5. Refer to consultant / SPR
6. Consider Dermatology review
Grade 4 • Any BSA Stop TKI
• Limiting self-care Urgent clinical assessment and consider admission if signs of
• ADLS systemic infection/sepsis.
• Itching/pain ✔ or ✘
• Infection ✔(extensive/
sepsis )
Paronychia
Inflammatory process of the periungual tissue. A common side effect of EGFR TKI therapy which can
affect over 50% of patients. Normally presents 1 – 6 months after initiation of therapy.
Advice to patients:
• Keep hands and feet dry, avoid prolonged submersion in soapy water (e.g. washing up)
• Moisturise hands and feet regularly
• Avoid nail trauma (particular care when cutting nails)
• Wear cotton gloves underneath washing up gloves to reduce nail trauma
• Dry feet thoroughly before putting on shoes
• Shoes should protect the nail but not be restrictive
• Avoid irritants
• Report nail issues so that they can be managed quickly and effectively
• Vinegar soaks can be recommended as prophylactic/preventative treatment.
4Grade Symptoms/ Signs Management
Grade 1 • Nail fold oedema/erythema ✔ 1. Continue TKI
• Pain ✘ 2. Give advice on self-management
• Discharge ✘ 3. Prescribe emollient and soap substitute
• Nail separation ✘ • E45/Dermol 500 apply twice daily
4. Antimicrobial soaks for 20 minutes 2-3 times daily
• White vinegar soaks - 1:1 ratio white vinegar
and warm water
• Potassium permangenate soak – Potasium
permanganate 400mg tablet diluted in 4 Litres
of water to make 1:10000 solution
Grade 2 • Nail fold oedema /erythema ✔ 1. Continue TKI
• Pain ✔ 2. As per grade 1.
• Discharge ✔ or ✘ 3. Send swab if discharge present
• Nail separation ✔ or ✘ 4. Prescribe potent topical corticosteroid
• Betametasone valerate apply twice daily for 7
days
5. If persists despite steroids, treat as G3
Grade 3 • Nail fold oedema /erythema ✔ • Discontinue TKI until grade ≤ 2
• Pain ✔ • Swab if evidence of infection
• Discharge ✔ • Contact Consultant/SPR
• Nail separation ✔ • Review the need for systemic antibiotics if
• Interrupting ADLs signs/symptoms of infection
(Requiring surgical intervention or IV • Consider silver nitrate/minor op (nail avulsion) under
antibiotics) care of GP.
Pictures – Chen-Wee Aw et al (2017)(9)
5Gastrointestinal toxicity
The most common TKI associated side effect.
When assessing diarrhoea it is important to obtain the following:
• Pre-treatment bowel habits
• Previous gastrointestinal disorders
• Toxicity grade (see below)
• Presence of any red flag symptoms requires urgent clinical review:
o Severe abdominal pain
o PR bleeding / bloody diarrhoea
o Pyrexia
o Concurrent vomiting and diarrhoea (risk of dehydration)
Grade Symptoms/ Signs
Grade 1 Increase ofObtain thorough history:
1. Thorough GI history
2. Record frequency and characteristic of stools
3. Rule out infection (if history of fevers, recent
hospital admission, course of antibiotics)
Grade 1 or 2: Persistent Grade 2 (>48hours) or
Grade ≥ 3.
• Start Loperamide 4mg followed by 2mg
after each loose stool (up to 16mg/day). • Hold TKI and inform treating
• Advise to maintain oral hydration consultant
• Avoid fatty or spicy foods. • Continue Loperamide
• Telephone followup within 48 hours • Consider adding codeine 30mg
QDS
• Send Stool culture
• If fevers, unwell, abdominal pain
arrange for bloods and medical
review, may need admission.
Resolution to Grade ≤1 Resolution to Grade ≤1
Continue TKI. No dose reduction Restart TKI after discussion with
required consultant. Consider does reduction
7Stomatitis
Inflammation of the mucous membranes of the mouth and lips.
All patients with stomatitis should be given advice on conservative measures:
• Choose foods that are easy to chew and swallow
• Avoid rough, spicy or acidic foods and ensure adequate fluid intake
• Maintain regular oral hygiene with soft bristle tooth brush and non alcoholic mouthwash.
• Switching to a childrens toothpaste may be more tolerable
• Supplement meals with high calorie drinks
Assessment of mucositis/stomatitis should include clinical examination and assessment of functional
status (ability to eat).
Grade Symptoms/ Signs Management
Grade 1 • Erythema of oral 1. Continue TKI at current dose
mucosa 2. Give conservative management advice as above
• Mild pain/sensitivity 3. Difflam mouth wash (Benzydamine 0.15% Take 10ml 4 hourly
as mouth wash. Do not swallow.
4. Prescribe analgesia e.g Soluble paracetamol 1g QDS
5. If oral candida: Nystatin suspension 1ml QDS 7days
Grade 2 • Patchy ulcerations or 1. Continue TKI at current dose, inform treating consultant.
pseudomembranes 2. Ensure adherence to conservative measures above
• Moderate pain 3. Consider escalating analgesia Co-codamol 30/500 dispersible
• Not interfering with oral tablets Take 2 tablets QDS as required. (Co-prescribe laxative
intake if required)
4. Topical corticosteroid e.g Hydrocortisone 2.5mg buccal
tablets. Take 1 tablet QDS as required. Allow tablet to dissolve
slowly in mouth in contact with painful ulcer.
Grade 3 • Confluent ulceration 1. Hold TKI therapy and inform treating consultant.
• Severe pain 2. If unable to manage oral intake or evidence of dehydration
• Limiting oral intake take bloods including FBC, U+E and CRP and medical advice.
• Risk of dehydration 3. Prescribe local anaesthetic to assist with oral intake.
Oxetecaine and antacid suspension Take 10ml QDS as
required.
4. Review analgesia and consider escalating.
5. Gelclair oral gel (15ml) can be used after all other oral
medications to provide symptomatic relief for up to 7 hours.
6. Dietician input to maintain oral intake.
7. Consultant decision to restart TKI once Grade 2 or less
with/without dose reduction.
Grade 4 • Tissue necrosis, 1. Stop TKI therapy and inform treating consultant
spontaneously bleeding 2. Urgent medical review and consider inpatient admission
• Severe pain 3. Take bloods including FBC, U+E, CRP , clotting
• Little/no oral intake 4. IV fluid resuscitation
• life threatening 5. Assess for potential infection and consider antibiotics
dehydration
8Liver function test abnormalities.
Cases of hepatitis/hepatic failure have been reported.
It is important that Liver function tests (LFT) are checked at baseline and with each cycle of
treatment.
Transient elevations in liver function tests (ALT and AST) are commonly seen when commencing
treatment.
Grade Test results Management
Grade 1 AST or ALT 20x ULN • Hold TKI treatment and inform
AST or ALT >20x abovebaseline if this was abnormal treating consultant.
Bilirubin >10x ULN • Discuss urgently with treating
consultant/SPR as may require
urgent investigation and treatment.
Renal Impairment
EGFR tyrosine kinase inhibitors are generally not excreted by the kidneys.
If a deterioration in renal function is noted on blood tests then these should be highlighted to the
relevant consultant/SPR, particularly if CrClInterstitial Lung Disease(10) Relatively uncommon side effect of EGFR tyrosine kinase inhibitors. Incidence of Grade 3+ toxicity
References
1. Giotrif 20 mg film-coated tablets - Summary of Product Characteristics (SmPC) - (emc) [Internet]. [cited 2020 Mar 14]. Available
from: https://www.medicines.org.uk/emc/product/5147/smpc
2. Tarceva 150 mg film-coated tablets - Summary of Product Characteristics (SmPC) - (emc) [Internet]. [cited 2020 Mar 14]. Available
from: https://www.medicines.org.uk/emc/product/8845/smpc
3. Iressa 250mg film-coated tablets - Summary of Product Characteristics (SmPC) - (emc) [Internet]. [cited 2020 Mar 14]. Available
from: https://www.medicines.org.uk/emc/product/6602/smpc
4. Vizimpro 45 mg film-coated tablets - Summary of Product Characteristics (SmPC) - (emc) [Internet]. [cited 2020 Mar 14]. Available
from: https://www.medicines.org.uk/emc/product/10356/smpc
5. TAGRISSO 40 mg film-coated tablets - Summary of Product Characteristics (SmPC) - (emc) [Internet]. [cited 2020 Mar 14]. Available
from: https://www.medicines.org.uk/emc/product/1985/smpc
6. Melosky B, Leighl NB, Rothenstein J, Sangha R, Stewart D, Papp K. Management of egfr tki–induced dermatologic adverse events.
Curr Oncol. 2015 Jan 8;22(2):123.
7. Califano R, Tariq N, Compton S, Fitzgerald DA, Harwood CA, Lal R, et al. Expert Consensus on the Management of Adverse Events
from EGFR Tyrosine Kinase Inhibitors in the UK. Drugs. 2015 Aug;75(12):1335–48.
8. Lacouture M. Prevention and Treatment of Acneiform Rash Caused by EGFR Inhibitors - The ASCO Post [Internet]. 2013 [cited 2020
Mar 14]. Available from: https://ascopost.com/issues/may-15-2013/prevention-and-treatment-of-acneiform-rash-caused-by-egfr-
inhibitors/
9. Aw DC-W, Tan EH, Chin TM, Lim HL, Lee HY, Soo RA. Management of epidermal growth factor receptor tyrosine kinase inhibitor-
related cutaneous and gastrointestinal toxicities. Asia Pac J Clin Oncol. 2018;14(1):23–31.
10. Płużański A, Piórek A. Side effects of tyrosine kinase inhibitors — management guidelines. Oncol Clin Pract. 2016;12(4):113–8.
11You can also read