Considerations for Choosing MIPS Quality Measures - July 2017
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Considerations for Choosing
MIPS Quality Measures
July 2017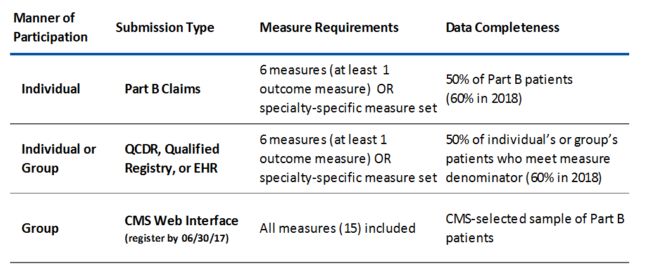
Overview of Contents
• First know yourself
• Finding measures
• Understanding scoring
• Special Considerations – about registries
• Special Considerations – ESRD patients
• Understanding the data that feeds measures – numerators, denominators,
and excluders – OH MY!
• Data capture in the typical workflow
• Data quality and integrity
• Notes and considerations on reporting
• 2018 proposed CMS updates
RPA Guide to QPP Participation 2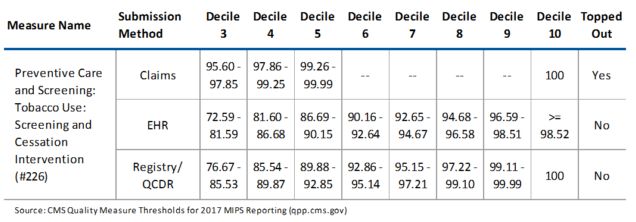
First Know Yourself
Quality measurement is dependent on making sure you are choosing
measures that:
• Reflect the most typical care you or your practice provide
• Have reasonable distributions of performance (decile range benchmarks) so
you can achieve high scores, even when you don’t have 100% performance
• Require data that your electronic health record system can easily and
discretely record
RPA Guide to QPP Participation 3Identifying and Choosing Measures
• Library of Measures at qpp.cms.gov
• 271 measures currently approved
• Must know the requirements for
complete data and choose the
method of how you or your group
want to submit data
• Important to remember that
measures are benchmarked and
earning a score is dependent on
deciles of performance and the
submission method.
• Decile of performance equals point
score; e.g. 9th decile = 9 points
4
All tables adapted from http://healthcareblog.pyapc.com/2017/01/articles/pay‐for‐performance/optimizing‐your‐mips‐score‐quality‐measure‐benchmarks‐and‐reporting‐mechanisms/Scores for MACRA/QPP – MIPS Quality Category
• Quality portion of MIPS composite score = 60 (out of 100) points for 2017
• Earning the 60 points is based on how well you (or your group) performs on
the 6 chosen quality measures, where each measure is worth a maximum
of 10 points.
• Groups of >16 clinicians will also be held accountable for a 7th measure –
the AHRQ all cause hospital readmission measure. No reporting is required
– data is aggregated and reported for you by CMS from claims data.
• There are bonus points achievable for choosing certain measures or using
certified EHR technology (CEHRT).
• The 60 points of the MIPS composite score is the % of points out of 60 (or
70 for groups >16) earned.
RPA Guide to QPP Participation 5MIPS – Quality Measure Score Card Example
Bonus
Measure
Measure
Type
# of
Cases
Performance Points For
Points High
Bonus
Points for Totals • Group >16 clinicians, therefore 70
Priority
CEHRT use
maximum possible points
• Did not meet the minimum # of reported
Outcome
0
Measure 1 Measure using 20 4.1 1 5.1
CEHRT (required)
cases for measure #6
Process using
Measure 2 21 9.3 N/A 1 10.3
CEHRT
• Earned bonus points for reporting via EHR
Measure 3
Process using
CEHRT 22 10 N/A 1 11 and choosing high priority measures
(#1,2,3, and 5)
Measure 4 Process 50 10 N/A N/A 10
• 53.9/70 = 77%
Measure 5 High Priority 43 8.5 1 N/A 9.5
Quality Category Score
Process below
Measure 6 case minimum 10 3 N/A N/A 3
• 77% of 60 possible MCS =
All‐Cause Hospital
Readmissions
Claims 205 5 N/A N/A 5 46.2 MIPS Composite Score Points
Total Points All Measures N/A 49.9 1 3 53.9
From MACRA final rule TABLE 19: Quality Performance Category Example with High Priority and CEHRT Bonus Points 6
https://www.federalregister.gov/documents/2016/11/04/2016-25240/medicare-program-merit-based-incentive-payment-system-and-alternative-payment-model-incentive-underNotes on Scoring of Measures
• Score is based on the performance
decile achieved according to
published, benchmarked distribution.
• CMS publishes benchmarks for all
measures on QPP.CMS.GOV
• Many measures are topped‐out,
meaning there are very small
performance differences separating
the deciles.
• The same measure often has different
benchmarks, depending on method of
submission
• For 2017‐2018 EHR submission has
the lowest percentage of topped out
measures
7
All tables adapted from http://healthcareblog.pyapc.com/2017/01/articles/pay‐for‐performance/optimizing‐your‐mips‐score‐quality‐measure‐benchmarks‐and‐reporting‐mechanisms/Notes on Registries • Qualified Registries (QRs) are approved vendors that aggregate and report quality data on behalf of subscribing clinicians and practices. MIPSwizard is an example. • QCDRs (Qualified Clinical Data Registry) are databases that allow the collection and submission of the data needed to report on quality measures. • QCDRs differ from Qualified Registries (QRs) in that QCDRs will offer both standard quality measures as well as custom, CMS‐approved quality measures that are not available in standard MIPS library of measures published by CMS. These custom measures may be specific to a disease or specialty of medicine. RPA’s Kidney Quality Improvement Registry (a QCDR) is an example. • Both QRs and QCDRs typically charge subscription fees and may offer various visualization and other tools, beyond simple data aggregation and reporting RPA Guide to QPP Participation 8
Notes about ESRD patients There is a lot of confusion about the ”requirements” for reporting across MIPS categories on ESRD patients. • At a minimum (and depending on how a clinician or group reports data), CMS requires reporting on 50% of Part B patients who fall in the denominator of a chosen measure. • When choosing measures, the types of encounters (based on CPT code) and/or disease state based on (ICD‐10) will determine which patients count in the denominator. • There are very few measures that include the dialysis CPT codes (909XX) or N18.6 in the denominator. • However, if a chosen measure does include ESRD services or patients, how to capture other needed data for the measure on enough patients will have to be considered given that EHR system use and robust data capture are not as easy in the dialysis setting. RPA Guide to QPP Participation 9
Understanding the data that feeds measures –
numerators, denominators, excluders, OH MY!
• For each chosen measure, it is important to ensure that for each data
element required the following is known:
• Where it is captured in the practice workflow?
• Who is responsible for capturing it?
• Which field‐specific data must be entered in the EHR?
• What the acceptable range of responses are for each specific data
element needed?
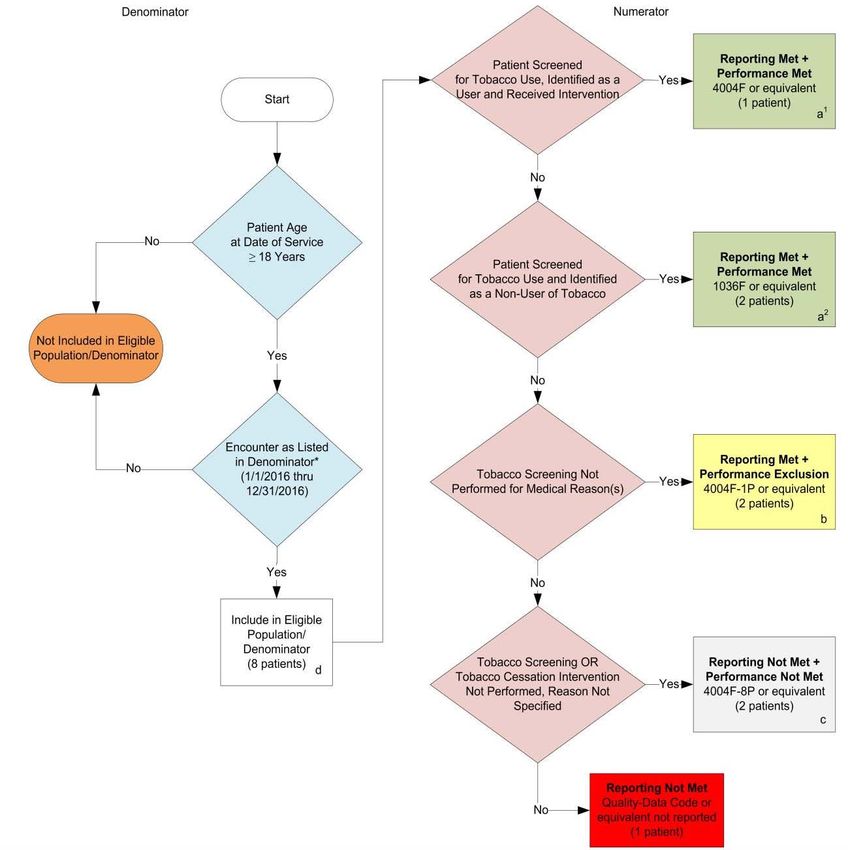
RPA Guide to QPP Participation 10Example – Smoking Cessation – CMS #226
Preventative Care and Screening: Tobacco Use
Measure: Percentage of patients aged 18 years and older who were screened for tobacco use one or more
times within 24 months AND who received cessation counseling intervention if identified as a tobacco user
Denominator Inclusion Numerator Inclusion Numerator Exclusion
• NOT Screened for tobacco use
and
Age > 18 on or after time of visit • reports no tobacco use
• circumstances document (terminal
illness, etc.)
and or or
A patient encounter resulting in a No Screening and/or no intervention
CPT list defined by CMS* • Reports current tobacco use
for other documented reason
and or
*90791, 90792, 90832, 90834, 90837, 90845, 92002, 92004,
92012, 92014, 96150, 96151, 96152, 97003, 97004, 99201, No Screening and/or no intervention
99202, 99203, 99204, 99205, 99212, 99213, 99214, 99215, • received counseling (3 min or less),
without documentation(measure
99406, 99407, G0438, G0439
pharmacotherapy, or both
not met) 11
RPA Guide to QPP ParticipationReport CPT 4004F
Measure
#226
Data Report CPT 1036F
Workflow
and CPTs Report CPT 4004F‐1P
to be
reported
Report CPT 4004F‐8P
12
From https://pqrs.cms.gov/dataset/2016‐PQRS‐Measure‐226‐11‐17‐2015/s8gr‐6b6i/dataMatching Data Requirements to Workflow:
Measure #226 Example
How and Where is this data typically
Required Data Who Captures the data?
captured?
Age≥ 18 @ time of visit Typically calculated from DOB in EHR Front office staff
Chosen by provider @ time of
Visit CPT code Provider (possibly coder)
encounter completion/bill generation
Automatically calculated based on
Date of visit Auto generated
date of service
Typically a checkbox or part of social
Reports current tobacco use? Provider/Medical Assistant/Nurse
history – varies on EHR
If tobacco user, was counseling May be a CPT code, may be a separate
Provider
provided? checkbox – varies by EHR
May be a checkbox, may be based on
If tobacco user, was pharmacotherapy
specific Rx given during or after the Provider
prescribed?
visit completion – varies by EHR 13Considerations on Data Capture
• What practice‐level incentives are in place to ensure staff and clinicians are
capturing the right data, in the right place, and at the right time?
• What and how often are reports reviewing the quality and completeness of
the data captured being run? Who reviews these reports? How is feedback
offered to correct or praise people in the practice?
• What mechanisms, policies, and/or procedures are in place to amend the
medical record if problems of missing or inaccurate data are discovered?
• For your EHR and other data tools, what is the time lag between when data
is recorded/entered in the EHR to when scorecards or quality measure
reports are updated for review?
RPA Guide to QPP Participation 14Considerations on Reporting Data to CMS…
Before allowing your registry vendor (QR, QCDR, or your EHR acting in the role of QR)
to submit data, consider the following:
• Have you sent test versions of your data to CMS? (will be available in some software in late
2017)
• Have you confirmed what measures will be reported to CMS?
• Have you reviewed the data to be submitted for each clinician and checked it against
internal reports?
• Will you have confirmation of transmission to CMS AND a copy of the exact data
file(s) sent?
• Are you aware of when and how CMS will report their calculated MIPS score for
your practice and/or clinicians?
• Are you aware of the deadlines and steps CMS offers to appeal/amend scoring on
submitted quality (and other) data?
RPA Guide to QPP Participation 15Possible Changes for 2018:
Updates From the proposed rule released in June 2017
(see https://qpp.cms.gov/about/resource‐library)
• The quality category of MIPS will remain worth 60/100 points of the MIPS
composite score for 2018.
• CMS has now proposed a nephrology specific quality measure bundle (See
appendix table B.21 in the proposed rule and the next slide)
• CMS has proposed a bonus of up to 10 points for clinicians or groups that show
significant year to year improvement between 2018 and 2019 reporting years.
• CMS proposes to accept data from more than one submission method for a single
category. This may ease some burden of reporting quality on ESRD patients when
data is gathered in multiple EHRs (office and dialysis unit‐based).
• CMS has proposed 1 possible change to scoring – measures with incomplete data
may be scored at 1 point as opposed to 3 points (except for small and rural
practices).
• CMS has proposed to sunset topped‐out measures over 4 year period starting in
2018. RPA Guide to QPP Participation 162018 Proposed Rule:
Possible Nephrology‐
Specific Quality Measure
Bundle
Table B.21 in the
proposed rule
RPA Guide to QPP ParticipationFor additional resources, including a list of
MIPS measures relevant to nephrology, visit
www.renalmd.org/physiciandevelopment
RPA Guide to QPP Participation 18You can also read