Controlled Trial of Aerobic Exercise in Hypertension
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

1560
Controlled Trial of Aerobic Exercise
in Hypertension
John E. Martin, PhD, Patricia M. Dubbert, PhD, and William C. Cushman, MD, FACP
To determine the antihypertensive efficacy of aerobic exercise training in mild essential
hypertension, a prospective randomized controlled trial was conducted comparing an aerobic
exercise regimen to a placebo exercise regimen, with a crossover replication of the aerobic
regimen in the placebo exercise group. The study took place in an outpatient research clinic in
a university-affiliated Veterans Administration medical center. Twenty-seven men with
untreated diastolic blood pressure (DBP) of 90-104 mm Hg were randomized to the two
exercise regimens. Ten patients completed the aerobic regimen. Nine patients completed the
control regimen, seven of whom subsequently entered and completed the aerobic regimen. The
aerobic regimen consisted of walking, jogging, stationary bicycling, or any combination of these
activities for 30 minutes, four times a week, at 65-80% maximal heart rate. The control regimen
consisted of slow calisthenics and stretching for the same duration and frequency but
maintaining less than 601% maximal heart rate. DBP decreased 9.6+±4.7 mm Hg in the aerobic
exercise group but increased 0.8±+6.2 mm Hg in the placebo control exercise group (p=0.02).
Systolic blood pressure (SBP) decreased 6.4±9.1 mm Hg in the aerobic group and increased
0.9±9.7 mm Hg in the control group (p =0.11). Subsequently, seven of the nine controls entered
a treatment crossover and completed the aerobic regimen with significant reductions in both
DBP (-6.1+3.2 mm Hg, pMartin et al Exercise in Hypertension 1561
resting or exercise electrocardiogram (ECG). Also ords of exercise sessions completed outside the lab-
excluded were any individuals who were adhering to oratory, and these records were reviewed in detail
a weight loss or a sodium-restricted diet or who were each week by the therapists.
currently exercising. For subjects who were taking Resting BP was assessed before each exercise
antihypertensive medications at the time they were session; if the DBP exceeded 104 mm Hg on three
screened, drug therapy was gradually tapered and consecutive visits, the subject was dropped from
discontinued for a minimum of 2 weeks before they treatment and referred for alternate therapy. Other-
entered the prerandomization period. They could be wise, subjects were not told their level of BP during
followed longer than 2 weeks, if necessary, for the the study and they were instructed not to have their
DBP to rise into the 90-104 mm Hg range. BP checked outside the laboratory until the study was
After signing consent forms approved by the Insti- completed.
tutional Review Board, subjects were seen at weekly Before randomization, subjects were told the pur-
intervals for at least 1 month for baseline assessment. pose of the study was to test the effects of different
Cuff size was determined at the initial visit according kinds of exercise on BP and that they would be
to arm circumference. At the beginning of each visit, assigned to one of two levels of exercise, that is, "high
after 5 minutes of rest, two seated BP readings were intensity" or "low intensity." Subjects in both groups
taken with a Hawksley random-zero sphygmoma- received equivalent attention from therapists and
nometer, and the mean systolic blood pressure (SBP) were assessed at the same intervals. Two weeks after
and DBP were recorded as the visit BP. BPs were beginning the exercise program and then at 4-week
assessed by a nurse specialist or one of two trained intervals, subjects in both groups had a random-zero
technicians. To be eligible for randomization, the sphygmomanometer BP reading and were weighed.
average DBP of the last three pretreatment visits and To enhance treatment credibility and compliance to
the final pretreatment DBP had to be 90-104 the two respective regimens, at the same 4-week
mm Hg. Additionally, the final pretreatment DBP intervals participants were tested for improvements
could not represent a clinically significant increasing in fitness and flexibility. Aerobic exercise subjects
or decreasing trend (e.g., 5 mm Hg or more) beyond were given submaximal GXT at these intervals,
the two previous measures. whereas control exercise subjects were given "flexi-
Other baseline measures included body weight, bility" assessments, which consisted of measuring
height, resting heart rate (HR), percentage of body changes in the distance they could reach in several of
fat, 24-hour urine sodium, potassium, and creatinine the stretching exercises. For aerobic exercise sub-
excretion, resting ECG, and a maximal graded exer- jects, improvements (decreases) in HR at the various
cise test (GXT) using the Bruce protocol. With the stages of the submaximal GXT and, for control
exception of height, these measures were repeated at exercise subjects, improvements in stretching ability
the end of treatment. Percentage of body fat was were pointed out as evidence of progress. To further
estimated from skinfold thickness obtained at four ensure the comparability of treatments with respect
sites (triceps, biceps, subscapular, and suprailiac). to nonspecific expectation and belief-mediated
Subjects were asked to refrain from changes in diet, effects on blood pressure and other measures, ratings
alcohol intake, or exercise (except for the prescribed of treatment credibility and satisfaction37 were
program) during the 10-week training period. obtained for all subjects after 1 month of treatment
After completion of baseline assessment, subjects and after treatment cessation using five-point and
were randomly assigned to aerobic exercise training nine-point qualitative ratings.
or the control exercise condition. The treatment All subjects received a maximal GXT again after
programs for both groups consisted of four 30- the 10-week treatment phase. Subsequently, subjects
minute sessions per week, with two of the four who completed the control exercise regimen, and
supervised by the project staff at the laboratory and who had not achieved a significant decline in their BP
the remaining two sessions performed by the subjects by the end of the initial treatment period, were
independently, outside the laboratory. The program offered the aerobic exercise regimen to serve as a
for the aerobic exercise group consisted of fast replication of the aerobic training conducted with the
walking, jogging, cycling, or any combination of these original experimental group.
activities at an intensity to maintain HR at 65-80% Group-by-time-of-assessment (2 x 4) repeated
of the maximum HR attained at the pretreatment measures analysis of variance (ANOVA) was used to
GXT. The program for the control exercise group test for significance of differences in the primary
consisted of stretching and easy calisthenics at an dependent measure, DBP, as well as SBP, between
intensity maintaining an HR not to exceed 60% of the two treatment groups at pretreatment and after
the maximum attained during the GXT. HR was 2, 6, and 10 weeks of exercise. Thus, a repeated
monitored throughout each laboratory and home measures across time ANOVA was used, with treat-
exercise session with a portable HR monitor ment as a grouping factor. Specific multiple compar-
(Exersentry model EX-3, Respironics, Inc., Monroe- isons were then performed using Bonferroni inequal-
ville, Pennsylvania), which had been preset to sound ities with the overall alpha set at p=0.05. The
a tone if the HR exceeded or declined below the interaction term in the repeated measures ANOVA
prescribed range. Subjects were asked to keep rec- estimates the treatment effect of differential change
Downloaded from http://circ.ahajournals.org/ by guest on September 22, 20151562 Circulation Vol 81, No 5, May 1990
TABLE 1. Pretreatment Subject Characteristics one subject became nonadherent to the regimen
Aerobic Control after a job-shift change. Therefore, after randomiza-
exercise exercise tion, 77% of the aerobic exercise group and 65% of
group group the control group completed the 10-week program.
n 13 14 Data from the credibility-and-satisfaction-with-
Race (% white) 84.7 71.4 treatment ratings were analyzed for between-group
Age (yr) 44.4± 10.1 42.6±7.7 differences using t tests, and Pearson product-
Range (yr) 21-54 32-53 moment correlations. It was found that the two
Body weight (kg) 90.3±16.2 93.3±16.2 groups were comparable in terms of credibility and
Weight/ideal weight (%) 124.8±17.9 128.0±17.6 expectation for success, that is, all ratings were
Systolic BP (mm Hg) 138.9±10.8 136.1±5.4 nonsignificantly different (t>0.05) and highly corre-
Diastolic BP (mm Hg) 95.0±4.4 94.1±3.7 lated (r=0.97) across the two groups. Thus, treat-
Sodium excretion (meq/24 hr) 238.4±82.2 283.4±149.3 ment credibility and satisfaction ratings indicated
Potassium excretion (meq/24 hr) 78.7±31.4 71.5±36.5 that subjects' beliefs regarding the potential effec-
Resting heart rate (beats/min) 80.9±7.8 81.4±10.5 tiveness of the treatments and their willingness to
Work capacity (METS) 11.6±2.2 10.4±2.1 recommend the treatments to a friend with a similar
problem did not differ.
Data expressed as the mean±SD.
Groups were not significantly different (pMartin et al Exercise in Hypertension 1563
TABLE 2. Mean Pretreatment, Posttreatment, and Changes in Values* for Aerobic and Control Groups
Significance
of time X
Aerobic exercise group Control exercise group group
(n = 10) (n =9) interaction
Diastolic BP (mm Hg)
Pre 94.8+4.6 93.7±3.6
Post 85.2±5.0 94.4±4.3
Change -9.6±4.7 +0.8±6.2 0.02
Systolic BP (mm Hg)
Pre 136.6±9.4 134.9+5.7
Post 130.2±10.2 135.8±7.9
Change -6.4±9.1 +0.9±9.7 0.11
Resting heart (beats/min)
Pre 80.7±8.5 78.8±9.8
Post 72.4±9.4 76.8±10.3
Change -8.3±9.7 -2.4±15.9 0.34
Work capacity (METS)
Pret 11.2±2.3 9.7± 1.7
Postt 13.2±1.8 11.2± 1.4
Changet +2.0±2.2 +1.5±1.2 0.55
Body weight (kg)
Pre 90.3±18.0 92.0±15.8
Post 89.9±17.0 92.4±16.9
Change -0.4±1.9 +0.4±1.4 0.32
Body fat (%)
Pre 29.8+5.8 34.2±4.6
Post 29.1±6.7 33.9±4.0
Change -0.7±2.8 -0.2±1.6 0.78
Sodium excretion (mEq/24 hr)
Pre 235.8±7.4 283.0±137.6
Post 202.5±36.3 258.4+101.5
Change -33.4±91.3 -24.6±+148.6 0.58
Potassium excretion (mEq/24 hr)
Pre 81.6±33.7 76.3±41.0
Post 74.8±32.4 97.1±66.5
Change -6.8±25.0 +20.7±66.5 0.70
Pre, pretreatment; Post, posttreatment.
*Groups were not significantly different (p1564 Circulation Vol 81, No 5, May 1990
Aerobic Exercise Control Exercise X
l---
Base
5
160r 160
r=
142- line
Exercise Crossover
E
150 150 138
2 - Exercise
06 - - Control
40 140 134-
0)
I
E 130 =3a30 130
1
E ° 126 l a *
a) c
c. 4 0 4 8 1 2 1 6 20 24
20 i19n
teu
CD) Treatment Week
00
CD)
CL
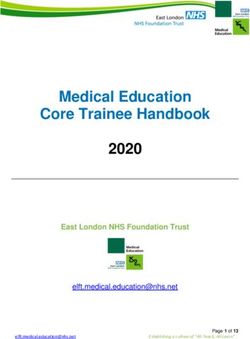
FIGURE 3. Plotting of mean systolic blood pressures in
110 110 millimeters of mercury (mm Hg) for aerobic exercise group
-o0
m
0 (n=10) and nonaerobic exercise controls (n=9) across pre-
100 100 treatment baseline and treatment (weeks 2 6, and 10), and
crossover replication (weeks 14, 18, and 22) for control
90 2 90 exercise subjects (n = 7) who were subsequently provided aer-
obic exercise training.
80 80
panied by changes in weight, body fat, or 24-hour
701 to
J70 urine sodium or potassium excretion. We believe this
-2 10 -2
study provides evidence for the independent antihy-
Treatment Week pertensive effect of aerobic exercise in mild essential
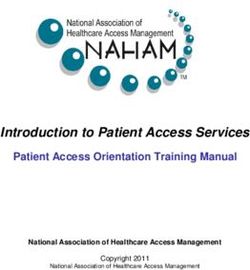
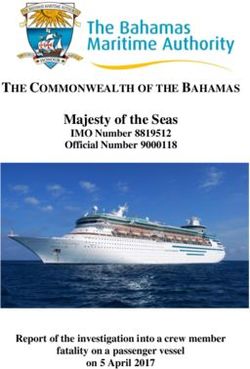
FIGURE 1. Plotting of individual diastolic (O) and systolic hypertension.
(o) blood pressures in millimeters of mercury (mm Hg) before Although habitual practice of vigorous exercise has
and after treatment. been shown in epidemiological surveys to be inversely
related to hypertension risk, independent of other
Resting HR, body weight, and sodium and potas- known risk factors for hypertension,1-4 and although
sium excretion did not change for these subjects prospective clinical studies have suggested the BP
(Table 3). Work capacity, however, increased lowering potential of exercise,5-31 the evidence for
1.2+1.3 METS between ending the control exercise the efficacy of exercise in the treatment of high BP
treatment and completing the subsequent aerobic has been inconsistent. In normotensive subjects, sev-
training regimen (p=0.025). eral studies have failed to show any BP lowering
effect from exercise,3942 whereas others suggest a
Discussion moderate BP lowering effect.7910"1123-25,43 In hyper-
In this study, subjects were randomly assigned to tensive patients, of the 30 studies conducted to date
either aerobic training or a placebo control treatment on exercise treatment,5-31,44-46 seven,10,l3,23,24,44-46 or
consisting of stretching and easy calisthenics. Signif- 23%, found no significant antihypertensive effect of
icant reductions in BP occurred only with aerobic exercise, and many failed to rule out the confounding
exercise. Importantly, BP reduction was not accom- effects of dietary sodium or potassium intake, body
weight, or body fat changes as an alternative expla-
nation for the BP changes. Additionally, of the 30
studies, only nine were randomized controlled stud-
E 98 Base Exercise Crossover ies using hypertensive controls.10,12,17,19,21,22,29-31
None compared exercise to a credible alternative
n94- treatment or attention/placebo. Furthermore, in two
of these controlled studies,12,17 the untreated hyper-
90 90-
Exer
tensive controls exhibited significant average reduc-
-a--- ~~~~~~~~~~~~~~~~Control
tions in BP (mainly DBP) similar to their exercised
c 86 counterparts. This is consistent with the experience
in the Australian National Blood Pressure Study in
which 48% of the mild hypertensive subjects were
= -4 0 4 8 12 16 20 24 normotensive on placebos after 3 years, with most of
Treatment Week the BP change occurring within the first few
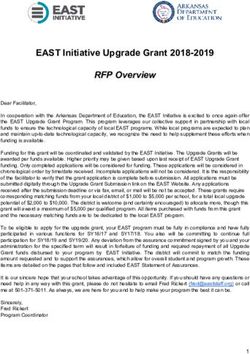
FIGURE 2. Plotting of mean diastolic blood pressures in months.47
millimeters of mercuty (mm Hg) for aerobic exercise group The present study was designed with these limita-
(n=10) and nonaerobic exercise controls (n=9) across pre- tions in mind and, therefore, included a randomized
treatment baseline and treatment (weeks 2, 6, and 10), and control group of hypertensives who received an exer-
crossover replication (weeks 14, 18, and 22) for control cise placebo treatment for comparison with the aer-
exercise subjects (n= 7) who were subsequently provided aer- obic exercise regimen. As such, this study represents
obic exercise training. an evaluation of the efficacy of aerobic exercise in
Downloaded from http://circ.ahajournals.org/ by guest on September 22, 2015Martin et al Exercise in Hypertension 1565
TABLE 3. Before and After Aerobic Exercise Data for Crossover Replication Subjects
Baseline After aerobic training Change p
n 7
Race (% white) 71.4
Systolic BP (mm Hg) 139.1±+10.6 130.0+7.9 -9.1±5.7 0.005
Diastolic BP (mm Hg) 96.0±3.7 89.6±3.2 -6.1±3.2 0.007
Resting heart rate (beats/min) 76.2±11.1 73.5±6.0 -2.7±13.0 0.301
Work capacity (METS) 11.3±1.6 12.6±1.9 +1.2±1.3 0.025
Body weight (kg) 86.6±9.5 86.1±8.4 -0.5±1.8 0.246
Sodium excretion (meq/24 hr) 266.9±109.7 279.6±118.1 +12.7+116.3 0.391
Potassium excretion (meq/24 hr) 83.6±80.2 104.2±68.3 +20.1+64.5 0.222
BP, blood pressure.
mild hypertensive subjects that isolates the effects of training after the ineffective control protocol completed
exercise from nonspecific treatment effects such as the second 10-week program. The recent popularity
amount of therapist attention, patient expectation of and increase in facilities and equipment for aerobic
treatment success, and repeated measurement of BP. exercise should make this form of nonpharmacological
The relative size of the DBP reduction found in treatment reasonably practical for the mildly hyperten-
the present evaluation (9.6 mm Hg) is very similar to sive population. Additionally, in recent years behavioral
that of previous studies of exercise in hypertension. strategies have been developed and validated for
This effect was replicated by using a partial crossover enhancing the acquisition and maintenance of the
to further evaluate its reliability. That is, when the exercise habit.48-52
aerobic training was offered and subsequently pro- The subjects in this study were young-to-
vided to the seven control exercise subjects who middle-aged untreated mildly hypertensive men who
agreed to continue participation in the project, sig- were, on average, 25-30% overweight. This study
nificant reductions occurred once again in DBP (6.1 does not address the potential response of women,
mm Hg) and, this time also, in SBP (9.1 mm Hg). the elderly, nonvolunteers, thin hypertensive sub-
Furthermore, of the 17 subjects who received the 10 jects, moderate-to-severe hypertensive subjects, or
weeks of aerobic training (10 randomly assigned medicated hypertensive subjects at any level, nor is it
originally to aerobic exercise and seven who crossed necessarily representative of the response expected
over to aerobic training after completing the control in less systematically conducted or supervised pro-
exercise protocol), 14 (82%) achieved DBP levels less grams. Our study was not designed to examine the
than or equal to 90 mm Hg. mechanisms by which exercise might decrease BP;
The fact that the reduction in SBP of -6.4±9.1 however, the changes observed could not be
mm Hg, although clinically meaningful, did not reach explained by any changes in body weight, body fat, or
statistical significance can be attributed to the rela- urinary sodium or potassium excretion although this
tively higher variability in SBP as compared with was a relatively obese population with high sodium
DBP, and because a priori power analyses to deter- intakes (consistent with that found in the southeast-
mine minimum group sizes were only conducted on ern U.S.). Larger-scale controlled studies might now
DBP, the primary dependent variable. Not surpris- be warranted to further establish the safety and
ingly, a post-hoc power analysis indicated that much effectiveness, as well as the reliability and ability to
larger groups would have been required to detect generalize the antihypertensive effects of exercise.
SBP change differences of the magnitude of those Additional questions that need to be addressed in
found in this study. Despite this limitation, in the these studies include the necessary dose and duration
crossover replication, aerobic exercise was associated of treatment and the mechanism or mechanisms of
with a statistically as well as clinically significant antihypertensive effect.
reduction in SBP of -9.1 mm Hg. Thus, SBP should The present study provides evidence for the inde-
be investigated as a primary dependent variable in pendent BP lowering effect of aerobic exercise in
future studies with larger sample sizes. unmedicated mildly hypertensive men. A systematic
One limitation of the present study concerns the program of vigorous exercise might be an acceptable
ability to generalize these findings for the treatment alternative to drug treatment in select hypertensive
and early control of elevated BP in a large population. subjects. The role of exercise as adjunctive therapy
Given the well-documented problems in achieving ade- with drugs is an attractive alternative to adding new
quate medication compliance in treated hypertensive drugs or increasing doses of current medication;
subjects, it might be expected that there would be more however, this has not been adequately investigated.
significant problems with a more complex and time- Despite the potential difficulty of attempting to
consuming exercise regimen. Yet, 77% of the subjects obtain long-term adherence to exercise regimens, the
who were randomized completed the 10-week pro- apparent beneficial effects of exercise on hypertension,
gram, and 100% of those who crossed over to aerobic as well as on other important cardiovascular risk factors
Downloaded from http://circ.ahajournals.org/ by guest on September 22, 20151566 Circulation Vol 81, No 5, May 1990
such as obesity,53,54 dyslipidemia,55 diabetes,56 and per- 16. Cade R, Mars D, Wagemaker H, Zauner C, Packer D, Privette
haps "Type A-coronary prone" behavior,57 should be M, Cade M, Peterson J, Hood-Lewis D: Effect of aerobic
considered. We believe that the present study demon- exercise training on patients with systemic arterial hyperten-
sion.AmJ Med 1984;77:785-790
strates that moderate aerobic exercise lowers BP in 17. Kukkonen K, Rauramaa R, Voutilainen E, Lansimies E:
some hypertensive subjects and might be an important Physical training of middle-aged men with borderline hyper-
modality in the control of hypertension. tension. Ann Clin Res 1982;14(suppl 34):139-145
18. Nomura G, Kumagai E, Midorikawa K, Kitano T, Tashiro H,
Acknowledgments Toshima H: Physical training in essential hypertension: Alone
and in combination with dietary salt restriction. J Cardiac
We wish to thank the following consultants for Rehab 1984;4:467-475
their contributions to the design and implementation 19. Hagberg JM, Goldring D, Ehsani AA, Heath GW, Hernandez
of this study: Drs. Leonard H. Epstein, Herbert G. A, Schectman K, Holloszy JO: Effect of exercise training on
Langford, Richard G. Hutchinson, and Neil B. Old- the blood pressure and hemodynamic features of hypertensive
adolescents. Am J Cardiol 1983;52:763-768
ridge. Appreciation is also expressed to Drs. Edward 20. Dubbert PM, Martin JE, Zimering RT, Burkett PA, Lake M,
Meydrech for his assistance on the statistical analyses Cushman WC: Behavioral control of mild hypertension with
and Robert M. Kaplan for his most helpful comments aerobic exercise: Two case studies. Behav Ther 1984;
on a later draft and revision of this manuscript; we 15:373-380
are also grateful to Donald Slymen for his statistical 21. Hagberg JM, Goldberg AP, Ehsani A, Heath GW, Delmez JA,
Haner HR: Exercise training improves hypertension in hemo-
consultation during the final revision of the manu- dialysis patients. Am J Nephrol 1983;3:209-212
script. Mary Elizabeth Lake and Paul A. Burkett are 22. Duncan JJ, Farr JE, Upton J, Hagan RD, Oglesby ME, Blair
acknowledged for their extensive roles in the assess- SN: The effects of aerobic exercise on plasma catecholamines
ment and exercise training portions of the project. and blood pressure in patients with mild essential hyperten-
sion. JAMA 1985;254:2609-2613
Finally, appreciation is expressed to Ann Walker and 23. Buccola V, Stone W: Effects of jogging and cycling programs
especially to Karen Freeman for their considerable on physiological and personality variables in aged men. Res Q
assistance with the technical preparation and revision 1975;46:134-139
of the current manuscript. 24. Sidney K, Shephard R: Perception of exertion in the elderly,
effects of aging, mode of exercise and physical training. Percept
Mot Skills 1977;44:999-1010
References 25. Emes C: The effects of a regular program of light exercise on
1. Montoye HJ, Metzner HL, Keller JB, Johnson BD, Epstein seniors. J Sports Med Phys Fitness 1979;19:185-190
FH: Habitual physical activity and blood pressure. Med Sci 26. Kiyonaga A, Arakawa K, Tanaka H, Shindo M: Blood pres-
Sports Exerc 1972;4:175-181 sure and hormonal responses to aerobic exercise. Hypertension
2. Gyntelberg F: Physical fitness and coronary heart disease in 1985;7:125-131
Copenhagen men aged 40-59. III. Factors related to working 27. Westheim A, Simonsen K, Schamaun D, Qvigstand E: Effect
capacity. Dan Med Bull 1974;21:49-56 of exercise training in patients with essential hypertension. J
3. Paffenbarger RS, Wing AL, Hyde RT, Jung DL: Physical Hypertens 1985;3:S479-S481
activity as an index of hypertension in college alumni. Am J 28. Attina D, Giuliano G, Arcangeli G, Musante R, Cupelli V:
Epidemiol 1983;117:245-257 Effects of one year of physical training on borderline hyper-
4. Blair SN, Goodyear NN, Gibbons LW, Cooper KH: Physical tension: An evaluation by bicycle ergometer exercise testing. J
fitness and incidence of hypertension in healthy normotensive Cardiovasc Pharmacol 1986;8(suppl 5):S145-S147
men and women. JAMA 1984;252:487-490 29. Nelson S, Esler M, Jennings G, Korner P: Effect of changing
5. Hanson JS, Neede WH: Preliminary observations on physical levels of physical activity on blood-pressure and hemodynam-
training for hypertensive males. Circ Res 1970;27:29-57 ics in essential hypertension. Lancet 1986;473-476
6. Barry A, Daly I, Pruett E, Steinmetz JR, Page HF, Birkhead 30. Cleroux J, Peronnet F, deChamplain J: Effects of exercise
NC, Rodal K: The effects of physical conditioning on older training on plasma catecholamines and blood pressure in
individuals. J Gerontol 1966;21:182-191 labile hypertensive subjects. Eur J Appl Physiol 1987;
7. Boyer JL, Kasch FW: Exercise therapy in hypertensive men. 56:550-554
JAMA4 1970;211:1668-1671 31. Urata H, Tamabe Y, Kiyonaga A, Ikeda M, Tanaka H, Shindo
8. Rudd JL, Day WD: A physical fitness program for patients M, Arakawa K: Antihypertensive and volume-depleting effects
with hypertension. J Geriatr Soc 1967;15:373-379 of mild exercise on essential hypertension. Hypertension 1987;
9. Wilmore JH, Royce J, Girandola RN, Katch FI, Katch VL: 9:245-252
Physiological alterations resulting from a 10-week program of 32. Leon AS, Blackburn H: Physical activity and hypertension, in
jogging. Med Sci Sports Exerc 1970;2:7-14 Freis E (ed): Cardiology I: Hypertension. New York, Butter-
10. deVries HA: Physiological effects of an exercise training worth & Co, 1982, pp 14-36
regimen upon men aged 52 to 88. J Gerontol 1970,25:325-340 33. Tipton CM: Exercise training and hypertension. Exerc Sport
11. Choquette G, Ferguson RJ: Blood pressure reduction in Sci Rev 1984;12:245-306
"borderline" hypertensives following physical training. Can 34. Martin JE, Dubbert PM: Exercise in hypertension. Ann Behav
Med Assoc J 1973;108:699-703 Med 1985;7:13-18
12. Bonanno JA, Lies JE: Effects of physical training on coronary 35. Seals DR, Hagberg JM: The effect of exercise training on
risk factors. Am J Cardiol 1974;33:760-763 human hypertension: A review. Med Sci Sports Exerc 1984;
13. Ressl J, Chrastek J, Jandova R: Hemodynamic effects of 16:207-215
physical training in essential hypertension. Acta Cardiol (Brux) 36. Joint National Committee (JNC) on Detection, Evaluation,
1977;32:121-133 and Treatment of High Blood Pressure: The 1988 report of the
14. Krotkiewski M, Mandroukas K, Sjostrom L, Sullivan L, Wet- JNC on detection, evaluation, and treatment of high blood
terquist H, Bjorntorp P: Effects of long-term physical training pressure. Arch Intern Med 1988;148:1023-1038
on body fat, metabolism, and blood pressure in obesity. 37. Biran M, Wilson GT: Treatment of phobic disorders using
Metabolism 1979;28:650-658 cognitive and exposure methods: A self-efficacy analysis. J
15. Roman 0, Camuzzi AL, Villanlon E, Klenner C: Physical Consult Clin Psychol 1981;49:886-899
training program in arterial hypertension: A long-term pro- 38. Fleiss: The Design and Analysis of Clinical Experiments. New
spective follow-up. Cardiology 1981;67:230-243 York, John Wiley & Sons, Inc, 1986
Downloaded from http://circ.ahajournals.org/ by guest on September 22, 2015Martin et al Exercise in Hypertension 1567
39. Cureton T: The Physiological Effects ofExercise Programs Upon 50. Martin JE, Dubbert PM, Katell A, Thompson JK, Raczynski
Adults. Springfield, Ill, Charles C Thomas Publishing, 1969 JR, Lake M, Smith PO, Webster JS, Sikora T, Cohen R: The
40. Buskirk ER, Counsilman JE: Special exercise problems in behavioral control of exercise in sedentary adults: Studies 1
middle age, in Johnson WR (ed): Science and Medicine of through 6. J Consult Clin Psychol 1984;52:795-811
Exercise and Sports. New York, Harper & Row Publishers, Inc, 51. Martin JE, Dubbert PM: Behavioral management strategies
1960, pp 491-507 for improving health and fitness. J Cardiol Rehab 1984;
41. Ekblom B, Astrand PO, Saltin B: Effect of training on 4:200-208
circulatory response to exercise. J Appl Physiol 1968; 52. Martin JE, Dubbert PM: Exercise Promotion, in Blumenthal
24:518-528 JA, McKee DC (eds): Applications in Behavioral Medicine and
42. Frick MH, Konttinen A, Sarajas HSS: Effects of physical
training on circulation at rest and during exercise. Am J Health Psychology: A Clinicians' Source Book. Sarasota, Fla,
Cardiol 1963;12:142-147 Professional Resource Exchange, 1987
43. Kasch FW: Physiological changes with swimming and running 53. Brownell KD, Stunkard AJ: Physical activity in the develop-
during two years of training. Scand J Sports Sci 1981;3:23-26 ment and control of obesity, in Stunkard AJ (ed): Obesity.
44. Johnson WP, Grover JA: Hemodynamic and metabolic effects Philadelphia, WB Saunders Co, 1980, pp 300-324
of physical training in four patients with essential hyperten- 54. Thompson JK, Jarvie GJ, Lahey BB, Cureton A: Exercise and
sion. Can Med Assoc J 1967;96:842-845 obesity: Etiology, physiology and intervention. Psychol Bull
45. Sannerstedt R, Waisir H, Henning R, Werko L: Systemic 1982;91:55-78
hemodynamics in mild arterial hypertension before and after 55. Wood PD, Haskell WL: The effect of exercise on plasma high
physical training. Clin Sci 1973;45:145s-149s density lipoproteins. Lipids 1979;14:417-427
46. DePlaen JF, Detry JM: Hemodynamic effects of physical 56. Vranic M, Berger M: Exercise and diabetes. Diabetes 1979;
training in established arterial hypertension. Acta Cardiol 28:147-167
1980;35:179-188 57. Blumenthal JA, Emery CF, Walsh MA, Cox DR, Kuhn CM,
47. Doyle AE: Response to placebo treatment in hypertension. Williams RB, Williams RS: Exercise training in healthy type A
Hypertension 1983;5(suppl III):III-3-III-4 middle-aged men: Effects on behavioral and cardiovascular
48. Martin JE, Dubbert PM: Exercise applications and promotion responses. Psychosom Med 1988;50:418-433
in behavioral medicine: Current status and future directions. J
Consult Clin Psychol 1982;50:1004-1017
49. Martin JE, Dubbert PM: Adherence to exercise, in Terjung RJ
(ed): Exercise and Sport Sciences Reviews. New York, Mac- KEY WORDS * hypertension * aerobic exercise * blood
millan Publishing Co, Inc, 1985;13:137-167 pressure * fitness
Downloaded from http://circ.ahajournals.org/ by guest on September 22, 2015Controlled trial of aerobic exercise in hypertension.
J E Martin, P M Dubbert and W C Cushman
Circulation. 1990;81:1560-1567
doi: 10.1161/01.CIR.81.5.1560
Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231
Copyright © 1990 American Heart Association, Inc. All rights reserved.
Print ISSN: 0009-7322. Online ISSN: 1524-4539
The online version of this article, along with updated information and services, is located on
the World Wide Web at:
http://circ.ahajournals.org/content/81/5/1560
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally
published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the
Editorial Office. Once the online version of the published article for which permission is being requested is
located, click Request Permissions in the middle column of the Web page under Services. Further
information about this process is available in the Permissions and Rights Question and Answer document.
Reprints: Information about reprints can be found online at:
http://www.lww.com/reprints
Subscriptions: Information about subscribing to Circulation is online at:
http://circ.ahajournals.org//subscriptions/
Downloaded from http://circ.ahajournals.org/ by guest on September 22, 2015You can also read