COVID-19 and Imaging - Positions and Statements of Radiological Societies - radiology.bayer.com
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
COVID-19 and Imaging – Positions & Statements of Radiological Societies provided by Medical & Clinical Affairs,
Radiology R&D, Bayer AG
COVID-19 and Imaging – Positions and Statements
of Radiological Societies
R&D Radiology, Medical & Clinical Affairs
Status July 8th, 2020
American College of Radiology (ACR)
The ACR recommends that the following factors be considered regarding use of imaging:
• CT should not be used to screen for or as a first-line test to diagnose COVID-19.
• CT should be used sparingly and reserved for hospitalized, symptomatic patients with
specific clinical indications for CT. Appropriate infection control procedures should be
followed before scanning subsequent patients.
• Facilities may consider deploying portable radiography units in ambulatory care facilities
for use when CXRs are considered medically necessary. The surfaces of these
machines can be easily cleaned, avoiding the need to bring patients into radiography
rooms.
• Radiologists should familiarize themselves with the CT appearance of COVID-19
infection in order to be able to identify findings consistent with infection in patients
imaged for other reasons.
As an interim measure, until more widespread COVID-19 testing is available, some medical
practices are requesting chest CT to inform decisions on whether to test a patient for COVID-
19, admit a patient or provide other treatment. The ACR strongly urges caution in taking this
approach. A normal chest CT does not mean a person does not have COVID-19 infection -
and an abnormal CT is not specific for COVID-19 diagnosis. A normal CT should not
dissuade a patient from being quarantined or provided other clinically indicated treatment
when otherwise medically appropriate. Clearly, locally constrained resources may be a factor
in such decision making. (Updated March 22, 2020).
ACR has also put out a statement on the safe resumption of non-urgent routine radiology
care, with emphasis on safety measures, local pandemic statistics, managing fear ,
addressing deferred and delayed care and risk-benefit based decision making.
ACR 2020, ACR recommendations for the use of Chest Radiography and Computed Tomography (CT) for
suspected COVID-19 infection, accessed 26 March 2020.
ACR Statement on Safe Resumption of Routine Radiology Care During the COVID-19 Pandemic.
https://doi.org/10.1016/j.jacr.2020.05.001
ACR recommendations for CT in COVID-19
ACR COVID-19-Radiology-Resources
PP-CTP-ALL-0014-3 1COVID-19 and Imaging – Positions & Statements of Radiological Societies provided by Medical & Clinical Affairs,
Radiology R&D, Bayer AG
ACR/RSNA/STR (Society of Thoracic Radiology)
The combined joint consensus from the three societies primarily addresses COVID-19 from
the radiologist reporting perspective. It provides guidance on reporting of CT findings and
attribution to COVID-19 (Simpson et al. 2020 Radiological Society of North America Expert
Consensus Statement on Reporting Chest CT Findings Related to COVID-19. Endorsed by
the Society of Thoracic Radiology, the American College of Radiology, and RSNA.)
Summary of the joint consensus: At this time CT screening for the detection of COVID-19
is not recommended by most radiological societies.
1) CT imaging features:
a. COVID-19 typically present with GGO with or without consolidation in peripheral,
posterior and lower lung zone. GGO frequently reported with round morphology or
crazy paving pattern. Peripheral distribution of GGO correctly distinguished
COVID-19 in 63-80% of cases.
b. The frequency of imaging findings also depends on when infected patients are
imaged. A slight majority of patients had a negative CT during the first two days
after symptom onset with GGO usually developing between day 0 and 4 after
symptom onset and peaking at 6-13 days.
c. Accuracy of the viral testing used should be considered carefully as throat swabs
are less sensitive than nasopharyngeal swabs. Rapid antigen tests have poor
sensitivity.
2) Reporting:
a. When typical or indeterminate features of COVID-19 are present as incidental
findings, they recommend contacting the referring providers to discuss viral
infection.
b. Suggest using “viral pneumonia” as an alternate to reporting as COVID-19
pneumonia.
c. Consult with clinical colleagues to establish consensus reporting approach.
Simpson presentation
Simpson S, et al. Radiological Society of North America Expert Consensus Statement on Reporting Chest CT
Findings to COVID-19. Endorsed by the Society of Thoracic Radiology, the American College of Radiology, and
RSNA. Radiology: Cardiothoracic Imaging 2020;2(2):e200152
Radiological Society of North America (RSNA) on their dedicated website has additional
consensus papers on best practices for radiology departments, with focus on elective
imaging, Covid- confirmed precautions, PPE for staff, Post imaging room cleaning and
screening of COVID-19 patients with Chest imaging guidelines and radiologist workflow.
Additional consensus on how to prepare for the radiology surge which is expected to come in
the coming months.
PP-CTP-ALL-0014-3 2COVID-19 and Imaging – Positions & Statements of Radiological Societies provided by Medical & Clinical Affairs,
Radiology R&D, Bayer AG
Radiology workflow figure from the best practices task force shown above.
Radiology Task Force Best practices link
RSNA-COVID-19-PostSurgePreparedness
Fleischner Society
Thoracic imaging with chest radiography (CXR) and computed tomography (CT) are key
tools for pulmonary disease diagnosis and management, but their role in the management of
COVID-19 has not been considered within the multivariable context of the severity of
respiratory disease, pre-test probability, risk factors for disease progression, and critical
resource constraints.
• Imaging is not routinely indicated as a screening test for COVID-19 in asymptomatic
individuals.
• Imaging is not indicated in patients with suspected COVID-19 and mild clinical
features unless they are at risk for disease progression.
• Imaging is indicated in a patient with COVID-19 and worsening respiratory status.
• Daily chest radiographs are NOT indicated in stable intubated patients with COVID-
19.
• CT is indicated in patients with functional impairment and/or hypoxemia after recovery
from COVID-19.
• COVID-19 testing is indicated in patients incidentally found to have findings
suggestive of COVID-19 on a CT scan.
PP-CTP-ALL-0014-3 3COVID-19 and Imaging – Positions & Statements of Radiological Societies provided by Medical & Clinical Affairs,
Radiology R&D, Bayer AG
In a resource-constrained environment, imaging is indicated for medical triage of patients
with suspected COVID-19 who present with moderate-severe clinical features and a high
pre-test probability of disease.
Fleischner Society report
STR/ASER (Society of Thoracic Radiology/American Society of Emergency Radiology)
STR and ASER do not recommend routine CT screening for the diagnosis of patients under
investigation for COVID-19. Chest CT can be restricted to patients who test positive for
COVID-19 and who are suspected of having complicating features such as abscess or
empyema.
STR position
Chinese Society of Radiology (Expert Recommendations)
Radiological diagnosis is an important part of the diagnosis and treatment of Pneumonia
caused by novel coronavirus infection.
Summary:
1) DR Exam: Pneumonia plain films of novel coronavirus infection has a high frequency of
missed diagnosis of pneumonia. No abnormal findings used to be observed in the early
stage of the disease, so it is not recommended.
2) CT Exam: The volumetric CT scan is the preferred choice. The thickness of the scan is 5
mm and reconstruction is 1 to 1.5 mm.
• The common CT manifestations of the two lungs are multiple patchy ground glass
shadows and consolidation shadows, which are mainly distributed along the
bronchovascular bundle and the subpleural, among which there are thickened
vascular shadows, which are shown as fine grid like shadows, presenting "paving
stone sign".It can also be manifested as extremely thin ground glass shadows, limited
ground glass shadows around small blood vessels.
• In the progressive stage, multiple lesions such as ground glass shadow,
consolidation, nodule and other pathological changes co-exist & are mainly
distributed in the outer zone of the lung, subpleural and pulmonary floor.; there may
be fibrotic lesions. In the consolidation shadow, the common air bronchogram and the
wall of the bronchioles are thickened, while in the fibrosis focus, the local lung texture
is thickened and twisted, the wall of the inner bronchus is columnar, the adjacent
pleura or interlobar pleura is thickened, there is a small amount of pleural effusion,
and there is no obvious lymphadenopathy.
A positive nucleic acid detection for the new coronavirus is the gold standard and the
radiologic diagnosis value lies in the detection of lesions, the evaluation of disease severity
and clinical classification.
Korean Society of Radiology (KSR)/ KSTR (Korean Society
of Thoracic Radiology)
PP-CTP-ALL-0014-3 4COVID-19 and Imaging – Positions & Statements of Radiological Societies provided by Medical & Clinical Affairs,
Radiology R&D, Bayer AG
The Korean Society of Radiology and the Korean Society of Thoracic Radiology have
prepared recommendations for the use of diagnostic imaging for COVID-19 in various clinical
scenarios.
Screening Imaging test
• Chest radiographs (CXR) or chest CT is not recommended for asymptomatic
individuals.
• CXR may be considered for patients with respiratory symptoms.
• CXR is recommended for patients with fever or respiratory symptoms
• Chest CT can be done after weighting individual risk and benefit, usually non-contrast
Diagnostic Imaging test in COVID-19 patients in Community treatment centers
• Chest radiographs (CXR) or chest CT may be considered for asymptomatic or mild
symptom individuals.
• Portable CXR may be appropriate in community centers.
• CXR is recommended for patients with fever or respiratory symptoms
• Chest CT can be done after weighting individual risk and benefit, usually non-contrast
Imaging studies for admitted patients with COVID-19
• Imaging follow-up with Chest radiographs (CXR) is recommended for patients with
pneumonia.
• Chest CT may be considered if complications are suspected, based on risks and
benefits.
• non-contrast CT is recommended but contrast may be considered when
complications or other diseases are suspected.
Chest CT findings
• Typical chest CT findings for COVID-19 pneumonia is multifocal peripheral ground-
glass opacities (GGO) in both lungs, and they tend to affect the posterior and lower
lungs rather than anterior and upper lungs. Crazy paving appearance and air-
bronchogram may be combined.
• Pure consolidation, pleural effusion, cavitation, calcification or lymphadenopathy are
rare, while a revered halo sign may be seen occasionally.
• Chest CT should only be performed when there are clear indications for CT,
weighting risks and benefits.
Japanese Society of Radiology
Although the definitive diagnosis of COVID-19 is made by viral polymerase chain reaction
(PCR) testing, the PCR testing system is not sufficient in Japan. For this reason, diagnostic
imaging for patients suspected of being infected with COVID-19 is drawing attention.
Recommendations:
(1) It is necessary to postpone non-urgent examinations and treatments and reduce the
absolute number of examinations and treatments.
(2) The use of CT as a screening test for COVID-19 is not recommended.
PP-CTP-ALL-0014-3 5COVID-19 and Imaging – Positions & Statements of Radiological Societies provided by Medical & Clinical Affairs,
Radiology R&D, Bayer AG
(3) As a tentative measure while viral testing is not widely available, it is acceptable to use
chest CT in order to make a decision on medical practice for patients suspected of having
COVID-19.
(4) Perform imaging examinations for COVID-19 patients after taking into careful consideration
the indications of each examination.
(5) Implement infection protection measures thoroughly in the imaging examination room.
(6) The radiology department needs to thoroughly implement infection protection measures
for radiologists and other staff and make a business continuity plan (BCP) to prepare for
an emergency in case an infected person is discovered in the department.
(7) It is necessary for radiologists to become familiar with characteristic CT findings of COVID-
19.
(8) To detect ground-glass opacities thin-slice CT scanning with slice thickness of less than
2mm is essential.
CT usage guidelines:
Specific circumstances under which a clinician judges that CT examination is required are as
follows:
1) Plain chest x-ray shows abnormal shadows, and it is necessary to differentiate from other
diseases.
2) COVID-19 is strongly suspected based on clinical manifestations and the prevalence of
infection in the region, but cannot be confirmed by PCR testing, and the risk of disease
progression is considered to be high.
3) Although plain chest x-ray does not show an abnormal shadow, PCR test is positive and
CT is expected to provide useful information.
When diagnosing a patient who is suspected of having moderate to severe pneumonia that
requires oxygenation, regardless of whether plain chest x-ray has been performed.
Typical CT findings
1) Unilateral or bilateral, subpleural ground-glass opacities that are predominant in the
posterior segments or lower lobes at an early stage
2) Round, multifocal ground-glass opacities
3) The extent of crazy-paving pattern or consolidation increases with the progression of
pneumonia.
4) Coexistence of trabecular shadows suggestive of organizing changes
Atypical CT findings
1) Segmental infiltrative shadows without ground-glass opacities
2) Hollow, well-defined nodules or masses
3) Centrilobular nodular shadows with tree-in-bud appearance
4) Pleural effusion (sometimes seen in severe cases)
JRS link (Japanese language)
JRS CT guidance (Japanese language)
PP-CTP-ALL-0014-3 6COVID-19 and Imaging – Positions & Statements of Radiological Societies provided by Medical & Clinical Affairs,
Radiology R&D, Bayer AG
European Society of Radiology (ESR) and European
Society of Thoracic imaging (ESTI)
Summary
• Chest radiography is not sensitive for the detection of ground glass opacities and
should not be used as first line technique.
• CT should not be used as screening test in patients with mild or no symptoms.
• CT findings of COVID-19 are characteristic, final diagnosis requiring a positive RT-
PCR test.
• CT allows disease evaluation extent at baseline and help predict a poor outcome and
need for ventilation
• The precautions to protect radiologists and technologists from infection included in
the guidance.
Key CT features
• Bilateral ground glass opacities are typical CT manifestations of COVID-19.
• Crazy paving and organising pneumonia pattern are seen at a later stage.
• Extensive consolidation is associated with a poor prognosis.
If US is unlikely to be diagnostic, CT should be preferred (even in circumstances where US
might be used first in ordinary circumstances), to minimise staff exposure. CT use must be
balanced by the knowledge that those staff engaged in patient transportation to the CT unit
may be exposed, and must be protected. Where US is appropriate and needed (e.g.
pregnant women, children, ICU patients), it should ideally be performed at the bedside, to
avoid patient transport and consequent staff exposure.
CT should not be performed as a screening test in patients with mild or no symptoms. Final
diagnosis of COVID-19 requires a positive RT-PCR test.
Revel M-P, et al. COVID-19 patients and the Radiology department – advice from the European Society of
Radiology (ESR) and the European Society of Thoracic Imaging (ESTI), Eur Radiology, 2 April 2020.
COVID and Radiology advice from ESR and ESTI
European Society of Radiology (ESR)
The society provided a very important resource (Radiology resource Hub) including 6
publications and review articles and the most important is the guidance from countries
including a flow chart how to deal with the COVID in the Radiology department country by
country e.g. Belgium, France, Germany, Italy, Hungary, check republic and other European
countries.
They also include resources from all the journal and universities e.g. AJR, British medical
journal and investigative radiology.
ESR COVID resources
European Association of Cardiovascular imaging (EACVI)
PP-CTP-ALL-0014-3 7COVID-19 and Imaging – Positions & Statements of Radiological Societies provided by Medical & Clinical Affairs,
Radiology R&D, Bayer AG
EACVI recommendations on precautions, indications and other related items to COVID-19
are published in an article in European Heart Journal (see link below).
Advice for cardiac imaging
• Echocardiography should not routinely be performed in patients with COVID-19
disease.
• A range of different cardiovascular manifestations can be found in COVID-19 which
may require cardiac imaging, including a bedside echocardiographic study.
• A focused cardiac ultrasound study (FoCUS) is recommended to reduce the duration
of exposure.
• The risk of contamination of equipment and personnel is very high during TOE—
consider repeat TTE, CT scan, or CMR as alternatives.
• Chest CT is frequently used to confirm COVID-19 pneumonia and might provide
possible synergies and opportunities of cardiac imaging.
• Coronary CT angiography can exclude or confirm an acute coronary syndrome in
COVID-19 pneumonia where elevated troponins are common.
• LV function can be assessed by LV angiogram in patients with acute coronary
syndromes during the invasive revascularization procedure.
• Positive troponins and myocardial dysfunction or severe arrhythmia suggestive of
Tako-tsubo or myocarditis may be an indication for acute CMR if of vital importance
for treatment,
• and patient can be safely transferred for imaging.
• Indications for feotal echocardiography remain the same as outside the COVID-19
pandemic.
Skulstad et al. 2020. COVID-19 pandemic and cardiac imaging: EACVI recommendations on precautions,
indications, prioritization, and protection for patients and healthcare personnel, European Heart Journal -
Cardiovascular Imaging
Skulstad et al. 2020 EHJ
European Society of Cardiology and COVID-19
BSTI (British society of Thoracic imaging)
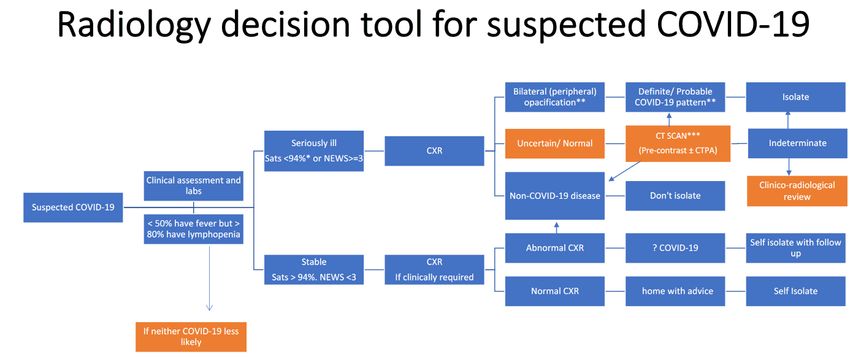
BSTI published guidelines in a Q&A format with focus on role of CT in the management of
cases. CT and CXR are discussed in regard to detection and management of COVID-19
cases. The paper also includes a decision support tool for suspected COVID-19 cases. They
state that the role of CT thorax in guiding management would be to triage patients into the
three categories of a) self-isolation at home with repeat testing , b) admission and isolation or
c) evaluation of alternative diagnosis and potentially aiding of unwell patients.
PP-CTP-ALL-0014-3 8COVID-19 and Imaging – Positions & Statements of Radiological Societies provided by Medical & Clinical Affairs,
Radiology R&D, Bayer AG
BSTI Consensus Statement
BSTI Decision Support tool
DRG (German Roentgen Society)
On March 26, 2020, the DRG posted a statement in German language: DRG COVID-19
position
English translation:
In summary of the information on imaging of COVID 19, the Thoracic Imaging group of DRG
explains the following:
• The primary test for the diagnosis of SARS Cov-2 is PCR.
• If the PCR test is negative and COVID-19 is suspected, serial PCR tests are the
method of choice.
• Low Dose CT (LDCT) characters are not specific for COVID-19 and may also be
present in other viral pneumonia. However, there are reports from China that in the
situation of: 1. appropriate clinical symptoms, 2. negative PCR test, 3. high local
prevalence of SARS-Cov-2 and 4. clinical consequence (i.e. in patients with
pronounced symptoms requiring hospitalization), native LDCT can make the
diagnosis, which must then be confirmed by serial PCR tests.
• A negative LDCT does not exclude COVID-19.
• Native LDCT or chest x-ray can be useful for assessing the severity of the disease
and for monitoring the clinical indication in severe cases.
• The radiologist must be familiar with the typical LDCT findings of COVID-19 in order
to recognize it as a random finding in CTs with another indication (e.g. exclusion of
pulmonary artery embolism).
Dutch Healthcare (NIPH) Guidelines: Diagnostic and
therapeutic management of thromboembolic Complications
PP-CTP-ALL-0014-3 9COVID-19 and Imaging – Positions & Statements of Radiological Societies provided by Medical & Clinical Affairs,
Radiology R&D, Bayer AG
A potential link between mortality, D-dimer values and a prothrombotic syndrome has been
reported in patients with COVID-19 infection. The report summarizes evidence for
thromboembolic disease, potential diagnostic and preventive actions as well as
recommendations for patients with COVID-19 infection.
1. Prophylactic-dose low-molecular-weight heparin should be initiated in all patients with
(suspected) COVID-19 admitted to the hospital, irrespective of risk scores (e.g. Padua
score).
2. A baseline (non-contrast) chest CT should be considered in all patients with
suspected COVID-19 who have an indication for hospital admission (Dutch
Healthcare).
3. In patients with suspected COVID-19 as well as a high clinical suspicion for PE (e.g.
based on hemoptysis, unexplained tachycardia, or signs/symptoms of DVT, acute
deterioration upon moving patient), CT pulmonary angiography should be considered
if the D-dimer level is elevated. The D-dimer threshold used should follow locally used
algorithms, i.e. ≥500 mg/L, age-adjusted threshold, or ≥1,000 mg/L when no YEARS
criteria are present. If PE is confirmed, therapeutic anticoagulation is indicated.
4. In patients with COVID-19 admitted to the hospital, routine D-dimer testing on
admission and serially during hospital stay should be considered for prognostic
stratification with additional imaging as available at local level.
• In patients with a D-dimerCOVID-19 and Imaging – Positions & Statements of Radiological Societies provided by Medical & Clinical Affairs,
Radiology R&D, Bayer AG
Prokop et al. CO-RADS – A categorical CT assessment scheme for patients with suspected COVID-19: definition
and evaluation. Radiology 2020. https://pubs.rsna.org/doi/10.1148/radiol.2020201473
The International Pulmonologist Society
The Society provides a consensus document regarding the COVID-19 infection and provided
the below regarding Radiology. There is the recommendation of the CDC, supporting the fact
that chest radiography or computed tomography are not recommended to diagnose the
COVID-19 infection. CDC Covid-19 resources
Chest Radiography (CXR). The findings on CXR are not specific, could overlap with other
entities, such as influenza and in the initial phases of the disease the studies could be
normal. The most common features include lobar/ multi-lobar / bilateral lung consolidation. It
is better to avoid the movement of the patient within the hospitals.
Computed Tomography (CT Chest)
• Early stage (0-4 days after the onset of the symptoms), in which ground glass
opacities (GGO) are frequent, with sub-pleural distribution and involving
predominantly the lower lobes. Some patients in this stage could have a normal CT.
• Progressive stage (5-8 days after the onset of the symptoms), the findings usually
evolved to rapidly involvement of the two lungs or multi-lobe distribution with GGO,
crazy-paving and consolidation of airspaces.
• Peak stage (9-13 days after the onset of the symptoms), the consolidation becomes
denser and it was present in almost all the cases. Other finding was residual
parenchymal bands.
• Absorption stage (>14 days after the onset of the symptoms), no crazy paving
pattern was observed, the GGO could remain. Shi et al [66] also described the CT
findings in 81 patients in Wuhan, China. All the patients had an abnormal CT, and
the features include: GGO, smooth and irregular interlobular septal thickening, crazy
paving pattern, air bronchogram and irregular pleural thickening. Usually affecting
the subpleural regions and the lower lobes.
Lung ultrasound. The USG findings are also not specific for COVID-19 infection. Little
information is available to date on this matter. The findings include: Irregular pleural lines,
sub-pleural areas of consolidation, areas of White lung and thick B lines. It is a tool that could
be used at bed side avoiding the need for shifting infected patients to a Radiology suite.
SIR (Society of Interventional Radiology) Guidelines
PP-CTP-ALL-0014-3 11COVID-19 and Imaging – Positions & Statements of Radiological Societies provided by Medical & Clinical Affairs,
Radiology R&D, Bayer AG
There is no available data for the role of IR in management of COVID-19 patients and
persons under investigation (PUI). Nonetheless, IR has a critical role in the management of
patients within the healthcare system and could conceivably be called to assist in the
management of a COVID-19 positive patient. IR suites may also be located near radiology
services where COVID-19 patients may undergo imaging. Proper, and early, preparation is
therefore crucial to reduce exposure to health care workers and other patients in IR.
Planning
• Regardless of the number of COVID-19 patients at the facility, we recommend
immediate plans be put in place to screen and/or manage COVID-19 patients
• We recommend IR teams be involved with their local COVID-19 response teams, or
equivalent. Early involvement can help to streamline the flow of patients and minimize
unnecessary patient and healthcare provider exposure.
• Develop plans with guidance from local resources, including infection control
• Emphasize to staff and visitors that CDC recommendations to protect yourself and
others must be followed
• Staffing models should be discussed to consider minimizing exposures and working
with reduced staffing
Personal Protective Equipment (PPE)
• Refer to CDC and WHO guidelines for appropriate use of PPE and ensure local
policy is followed
• Conservation of PPE through training and appropriate use is critical during the
COVID-19 pandemic as the CDC is reporting “increased volume of orders and
challenges in meeting order demands”
• Advice on mask use and hygiene outside and within the healthcare setting is
described by WHO
• Develop a plan for cleaning of isolation areas if utilized by screen positive persons
using droplet cleaning protocols
• Identify air negative rooms for procedures (if available) or designate rooms to be used
for procedures on COVID-19 patients
The society guidelines stratify work geographic areas as low, moderate and substantial risk,
based on inpatient and outpatient facilities. They provide some guidance for those regions
and recommend, cancelling all elective and non-urgent procedures for substantial risk labs.
Additional recent guidelines from SIR include:
• Cancel all procedures except for those that are urgent or emergent
• Minimize the use of essential items that will be needed to care for patients in the
event of a surge of cases.
• Screen all patients for high-risk exposure or symptoms according to the CDC
guidelines.
• If local guidance requires testing prior to surgical procedures, this same standard
should apply to procedures performed in the IR suite.
PP-CTP-ALL-0014-3 12COVID-19 and Imaging – Positions & Statements of Radiological Societies provided by Medical & Clinical Affairs,
Radiology R&D, Bayer AG
• Optimize-staffing and consider cohorting teams to facilitate social distancing and limit
risk of community spread.
• Utilize telehealth services for IR clinic and follow-up visits when appropriate to limit
exposure.
SIR Clinical Notification
SIR Covid-19-toolkit
SNMMI ( Society on Nuclear medicine & Molecular Imaging)
COVID-19 and Ventilation/Perfusion (V/Q) Lung Studies:
As we all do our best to avoid the spread of COVID-19 while continuing to provide the best
care for our patients, we would like to respond to concerns regarding ventilation/perfusion
(V/Q) lung scans and the risk inherent in the V/Q scan for spread of COVID-19 to patients
and staff alike.
Because many ventilation systems are difficult to completely disinfect and because there are
still unknowns about the transmissibility of COVID-19, some institutions have elected to
eliminate entirely the ventilation portion of the V/Q study. When lung perfusion images show
no evidence of pulmonary thromboembolism, it essentially rules out acute pulmonary
embolism, and no further studies are needed. While it is recognized that not performing
paired ventilation images will eliminate important information about airway physiology, it is
felt by some to be the most judicious action until the COVID-19 pandemic can be better
understood.
Local health care facility policy should be the primary source of guidance as to the handling
of patients with and without suspected COVID-19 infection.
SNMMI and V/Q studies
Additional Opinions and Editorials
Kanne et al. 2020 Essentials for Radiologists on COVID-19: An Update—Radiology Scientific
Expert Panel
• Up to approximately 50% of patients with COVID-19 infection may have normal CT
scans 0–2 days after onset of flu-like symptoms from COVID-19
• COVID-19 RT-PCR sensitivity may be as low as 60-70%; therefore, patients with
pneumonia due to COVID-19 may have lung abnormalities on chest CT but an initially
negative RT-PCR.
• Lung abnormalities during the early course of COVID-19 infection usually are
peripheral focal or multifocal ground-glass opacities affecting both lungs in
approximately 50%–75% of patients.
• As the disease progresses, crazy paving and consolidation become the dominant CT
findings, peaking around 9–13 days followed by slow clearing at approximately 1
month and beyond.
PP-CTP-ALL-0014-3 13COVID-19 and Imaging – Positions & Statements of Radiological Societies provided by Medical & Clinical Affairs,
Radiology R&D, Bayer AG
Achenbach S. (chair of the department of cardiology at Friedrich-Alexander-University
Erlangen-Nürnberg, Germany) noted in a recent European Society of Cardiology (ESC)
webinar that “CT can help with treatment decisions for COVID-19 patients”.
https://www.escardio.org/Education/COVID-19-and-Cardiology
Yang et al. Novel Coronavirus infection and Pregnancy
Summary:
• Based on the available clinical and research data, the clinical characteristics of
patients with COVID-19 infection presenting from the mid-trimester onwards are
similar to those of non-pregnant adults.
• There is not evidence that pregnant women are more susceptible to COVID-19
infection and that those with COVID-19 infection are more prone to developing severe
pneumonia.
• There is no evidence of vertical mother-to-baby transmission of COVID-19 infection
when the maternal infection manifests in the third trimester.
• Ongoing collection of clinical data and research is underway with the aim of
answering questions in relation to the risk of congenital infection and the optimal
intrapartum management and timing and mode of delivery.
Ultrasound Obstet Gynecol 2020; 55: 435–437
Yang Ultrasound & pregnancy
Foust et al. International Expert Consensus Statement on Chest Imaging in Pediatric COVID-
19 Patient Management: Imaging Findings, Imaging Study Reporting and Imaging Study
Recommendations.
Chest imaging plays an important role in evaluation of pediatric patients with COVID-
19, however there is currently little information available describing imaging manifestations of
pediatric COVID-19 and even less discussing utilization of imaging studies in pediatric
patients. The goal of this study is to generate a consensus statement for chest imaging in
pediatric patients with COVID-19 infection by international experts from 5 continents. The
document provides guidance in the structured reporting of imaging findings for both CXR and
Chest CT
CXR Imaging findings:
In the clinical experience of this expert panel of pediatric chest radiologists, both
unilateral and bilateral opacities have been observed in pediatric COVID-19, although
bilateral opacities are more typical. CXR is essential in this patient population due to
increased radiation sensitivity of children and hesitancy to pursue cross-sectional
imaging such as CT. In children not responding to outpatient management, requires
hospitalization or is suspected of having hospital acquired pneumonia, CXR is
considered the most appropriate first step in imaging evaluation.
Sequential CXRs are appropriate in moderate-to-severe pediatric COVID-19 patients
on an as clinically needed basis to monitor response to supportive measures, assess
clinical deterioration or evaluate positioning of life support devices. For asymptomatic
pediatric patients who had a mild disease course, no long term imaging follow-up is
recommended. However, even pediatric patients with a mild disease course may
develop long standing pulmonary injury and thus a follow-up standard two-view (PA
PP-CTP-ALL-0014-3 14COVID-19 and Imaging – Positions & Statements of Radiological Societies provided by Medical & Clinical Affairs,
Radiology R&D, Bayer AG
and lateral). CXR should be considered in symptomatic patients with prior mild
COVID-19.
Chest CT imaging findings:
Studies in pediatric patients have found loer total number of pulmonary lesions and
smaller size of pulmonary lesions compared to adults and significantly lower rate of
positive CT findings. The most common findings are bilateral peripheral and/or
subpleural ground-glass and/or consolidative opacities often in the lower lobes of the
lungs .
Based on experience of the expert panel, three phases of evolution have been
observed in pediatric COVID-19 cases the “halo” sign: the “halo” sign is generally
observed early in the disease course (early phase) and progresses to ground-glass
(progressive phase) and eventually develops into consolidative opacities (developed
phase).
Chest CT is not recommended as the initial diagnostic test in pediatric patients with
suspected COVID-19. However, it may be considered to answer a specific clinical
question in
the acute setting (for example to exclude a pulmonary embolism in a patient with an
elevated D-dimer level). Additionally, chest CT may be considered in pediatric
COVID-19 patients with a worsening clinical course and/or who are not responding
appropriately to supportive therapy. Finally, follow-up chest CT may be helpful to
assess for development and/or evolution of fibrotic lung disease in patients with
persistent alterations in PFTs following resolution of the acute infection. A chest CT in
the moderate-to-severe group may be considered, especially if not pursued at the
time of initial presentation, in pediatric patients who are not responding appropriately
to supportive care or demonstrate clinical deterioration.
Radiology Cardiothoracic ImagingVol. 2, No. 2.
Foust et al Radiology
Rotzinger et al. Pulmonary embolism in patients with COVID-19: Time to change the
paradigm of computed Tomography. Thrombosis Research 190 (2020) 58–59
The exact role of CT imaging in the management of COVID-19 is still being debated, and
evidence-based guidance regarding acquisition protocols is lacking. Current guidelines
advocate the use of non-contrast chest CT for the diagnosis, severity assessment, and
monitoring of COVID-19. When CT is indicated, the examination should be carried out with
as little harm as possible to the patient; this implies that contrast agent injection should be
performed only when needed to prevent possible complications, such as acute renal
insufficiency or allergic reactions. Though detection of typical lung imaging features of
COVID-19 does not require intravenous contrast agent use, patients with known COVID-19
and sudden onset clinical deterioration with unexplained worsening of dyspnea or chest pain,
may benefit from vascular enhancement to be appropriately diagnosed and managed.
Recently two studies by Zhou et al. and Tang et al. reported a positive correlation between
elevated D-dimer levels on admission and in-hospital COVID-19 mortality, raising questions
regarding potentially unknown pulmonary embolism and outlining the possible role of CT
pulmonary angiography in patients with COVID-19 and rapid clinical worsening.
Conclusion: In the case of elevated D-dimer levels on admission or sudden clinical
worsening, CT pulmonary angiography should be considered since pulmonary embolism is a
life-threatening but potentially treatable condition.
Rotzinger et al. Thrombosis research
PP-CTP-ALL-0014-3 15COVID-19 and Imaging – Positions & Statements of Radiological Societies provided by Medical & Clinical Affairs, Radiology R&D, Bayer AG Manna et al. COVID-19: A Multimodality Review of Radiologic Techniques, Clinical Utility, and Imaging Features. This review describes the clinical utility and imaging features of chest radiology (CXR) and Computed tomography (CT) in the diagnosis and evaluation of COVID-19. Additionally, it describes the modalities less commonly used, namely magnetic resonance imaging (MRI) and positron emission tomography/computed tomography (PET/CT). Point of care evaluation in the ER and intensive care setting of chest ultrasonography and echocardiography in COVID are described for diagnosis and evaluation of extent of lung disease and complications such as pulmonary embolism and right heart strain. Finally, AI applications and thromboembolic and extra-thoracic imaging features are examined. Manna et al. Radiology Bavishi et al. Acute Myocardial Injury in Patients Hospitalized with COVID-19 Infection: A Review. In this review of clinical studies, we found that in 26 studies including 11,685 patients, the weighted pooled prevalence of acute myocardial injury was 20% (ranged from 5% to 38% depending on the criteria used). The plausible mechanisms of myocardial injury include, 1) hyperinflammation and cytokine storm mediated through pathologic T-cells and monocytes leading to myocarditis, 2) respiratory failure and hypoxemia resulting in damage to cardiac myocytes, 3) down regulation of ACE2 expression and subsequent protective signaling pathways in cardiac myocytes, 4) hypercoagulability and development of coronary microvascular thrombosis, 5) diffuse endothelial injury and ‘endotheliitis’ in several organs including heart, and, 6) inflammation and/or stress causing coronary plaque rupture or supply demand mismatch leading to myocardial ischemia/infarction. In patients with elevated hs- troponin, clinical context is important and myocarditis as well as stress induced cardiomyopathy should be considered in the differential, along with type I and type II myocardial infarction. Irrespective of etiology, patients with acute myocardial injury should be prioritized for treatment. Clinical decisions including interventions should be individualized and carefully tailored after thorough review of risks/benefits. Bavishi et al. Radiology PP-CTP-ALL-0014-3 16
You can also read