HOW TO FIGHT THE CORONAVIRUS SARS-COV-2 AND ITS DISEASE, COVID-19 MICHAEL LIN, PHD-MD STANFORD UNIVERSITY WARNING: CONTAINS FACTS BONUS: HAND ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
How to fight the coronavirus
SARS-CoV-2 and its disease,
COVID-19
Michael Lin, PhD-MD
Stanford University
Warning: Contains facts
Bonus: Hand sanitizer recipe
Continuously updated
(Original version 2020-03-13)
3/31/20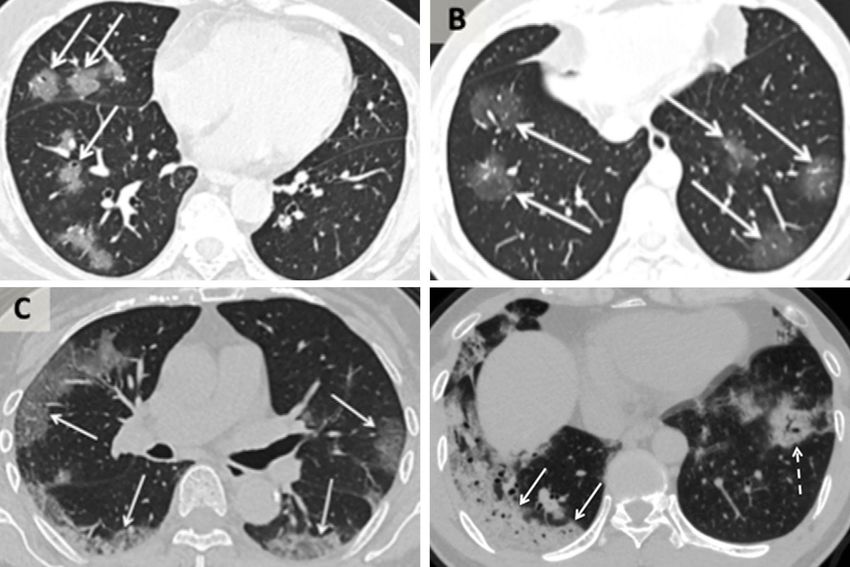
This is not a pretty powerpoint • This is an informational document. • This is not a TED talk. It is not meant to entertain or dazzle or push an idea with beautiful graphics. • So there will be a lot of text, because there is a lot of info that needs to be explained. Graphics will be used as data primarily. You will have to do some reading. 3/31/20 Michael Lin, PhD-MD 2
Some context for the numbers you will see
Total population
• 330M USA
1.2M heart disease and
• 40M California (CA) ➔
cancer deaths per year
Flu (influenza) deaths this season
• 40,000 USA (range 20,000 to ➔
60,000) ~60,000 flu + pneumonia deaths per year
(www.cdc.gov/flu/about/burden/
preliminary-in-season-
estimates.htm)
• 5,000 CA, estimated. From a
population of 40M, if 25%
infected with flu virus, this means
an infection fatality rate (IFR) of All-cause deaths: 2.8M per year
0.05%. If 12.5% infected, then IFR
= 0.1%.
3/31/20 Michael Lin, PhD-MD 3
Some definitions
COVID-19 stands for “coronavirus disease 2019”
• It refers to the disease, not the virus. But in practice, is used
to refer to having a positive lab test for the virus regardless
of symptoms.
• WHO introduced the disease name COVID-19 with great
Example of COVID-19
fanfare (after weeks of discussions) at a time when there
was no virus name, so it got used by many people as the
virus name, incorrectly.
• COVID-19 breaks a convention of naming diseases based
on major symptom, e.g. severe acute respiratory syndrome
= SARS. Also we didn’t previously have dates in disease
names. We don’t say someone is suffering from AIDS-81,
for example.
• The lack of information in the name makes the term doi.org/10.1101/2020.03.15.20036707
”COVID-19 virus” awkward, as this means “coronavirus
disease 2019 virus”.
• Given the similarity in clinical presentation, SARS2 would
have been an accurate name, but WHO wants to avoid any
reference to SARS for political reasons
(https://qz.com/1820422).
3/31/20 Michael Lin, PhD-MD 4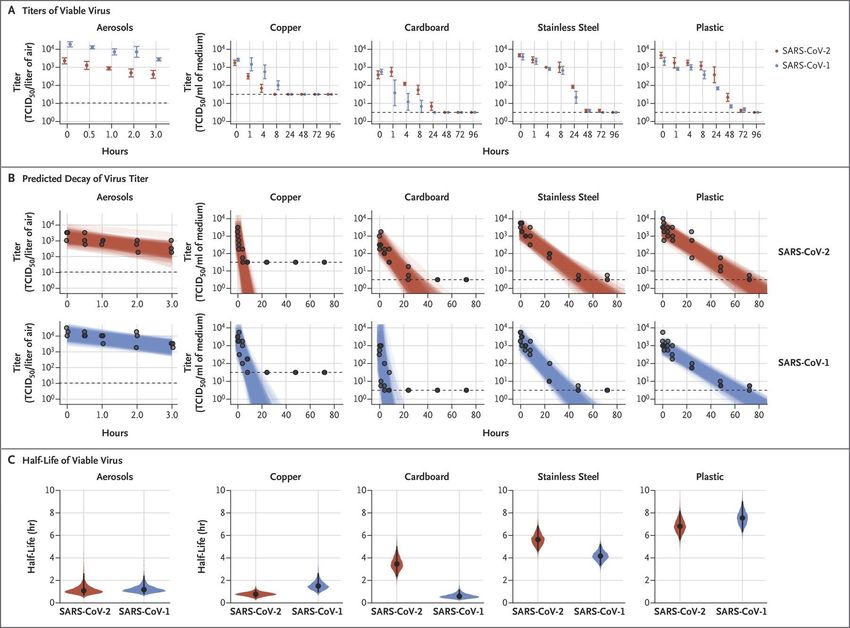
Some definitions
2019-nCOV was WHO’s provisional name for the virus, where nCOV stands
for novel coronavirus (https://www.who.int/docs/default- SARS-CoV-2
source/coronaviruse/situation-reports/20200130-sitrep-10-
ncov.pdf?sfvrsn=d0b2e480_2).
• Like the name COVID-19, this name is also misleading, because it
suggests the virus is especially novel. It’s not. In fact it’s the least
novel of the respiratory disease-causing viruses isolated in the
molecular age. Its defining feature is its NON-novelty...
SARS-CoV-2 is the name for the virus selected by the International
Committee on Taxonomy of Viruses, because it is 80% identical in overall
nucleotide sequence to SARS-CoV, the cause of SARS in 2003 (Pubmed wapo.st/coronavirus-structure
32123347).
• This name is accurate and informative, revealing the high similarity
between these two pathogens. It reminds us that we can infer a lot
about SARS-CoV-2 from existing data on SARS-CoV.
• Ironically, the WHO continues to not call the virus SARS-CoV-2 for
precisely this reason – to obscure the relationship between the two
viral diseases (flip.it/t7rdU7). However we are scientists, we want
clarity not obfuscation.
3/31/20 Michael Lin, PhD-MD 5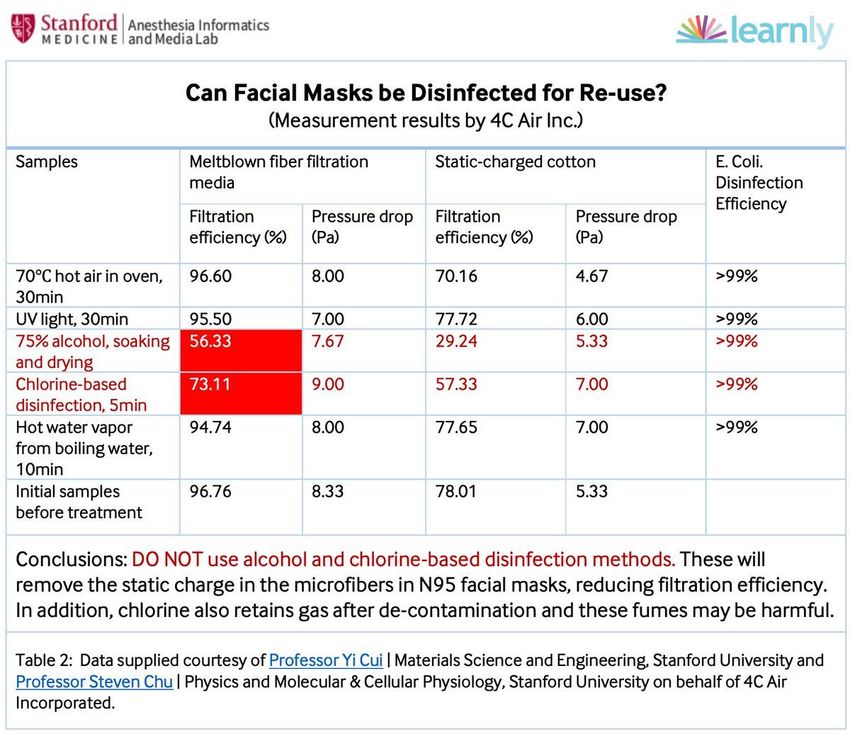
Coronaviruses (CoVs)
• Coronaviruses are positive-strand RNA
viruses with large genomes (≥27,000
bases).
• Both alpha and beta types cause disease Alpha
in humans, account for 10-30% of cases
of the common cold (Pubmed 31971553).
• Very stable for RNA viruses – CoV OC43
isolates from 1960s and 2001 had only 2
MERS-CoV
amino acid changes (Pubmed 15280490)!
• Easily hops between species SARS-CoV
– MERS-CoV hopped from camels to Bat relatives
humans Beta
– SARS-CoV hopped from bats to
civets and humans
SARS-CoV-2
– SARS-CoV-2 hopped from bats to
humans Bat relatives
– It seems humans with colds gave
mice hepatitis, or vice versa
https://www.sciencemag.org/news/2020/01/mining-coronavirus-genomes-clues-outbreak-s-origins
3/31/20 Michael Lin, PhD-MD 6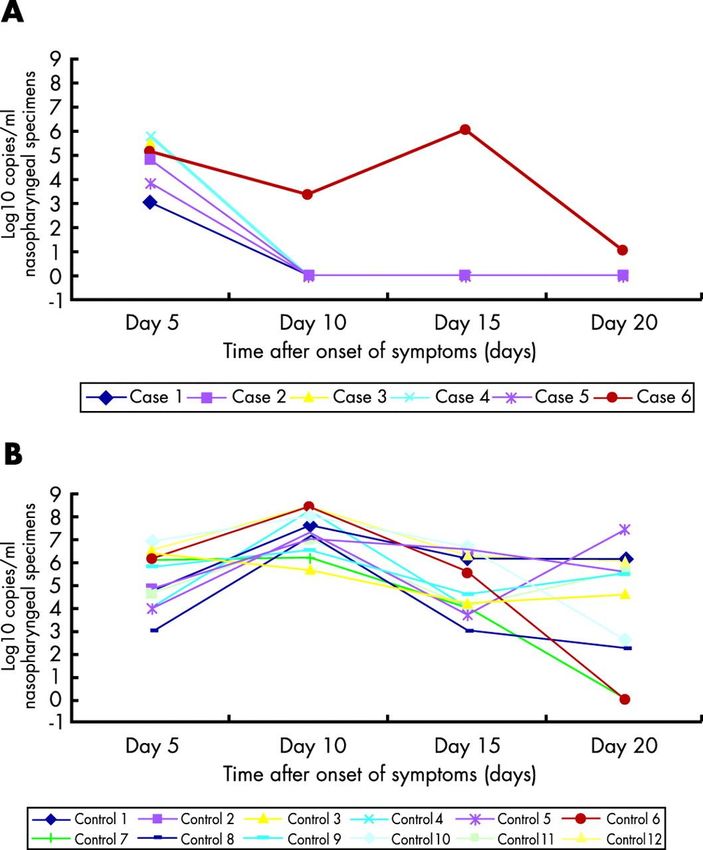
SARS-CoV-1/2 life cycle
doi.org/10.1038/nrmicro2090 1. Spike protein (S) binds to host ACE2*.
2. Host transmembrane protease
TMPRSS* or endosomal cathepsin L*
cleaves S to activate membrane fusion.
* 3. Cellular ribosomes translate a
Spike cleavage by TMPRSS or cathepsin L
*
nonstructural polyprotein from the
positive-strand RNA.
4. Embedded viral proteases* process the
polyprotein to create the replicase.
5. The replicase* produces full-length
copies of both strands and subgenomic
mRNAs.
* * 6. Ribosomes translate the subgenomic
mRNAs to produce structural proteins.
7. Structural proteins package the positive-
strand RNA and bud off into exocytic
veicles.
* Targets of investigational medicines
3/31/20 Michael Lin, PhD-MD 7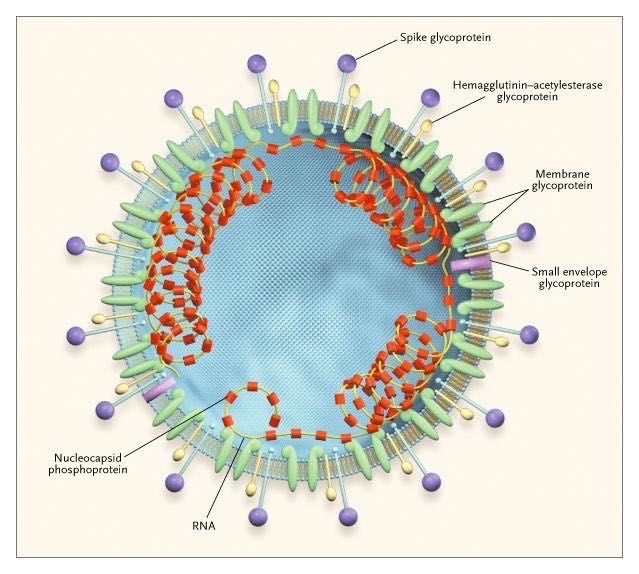
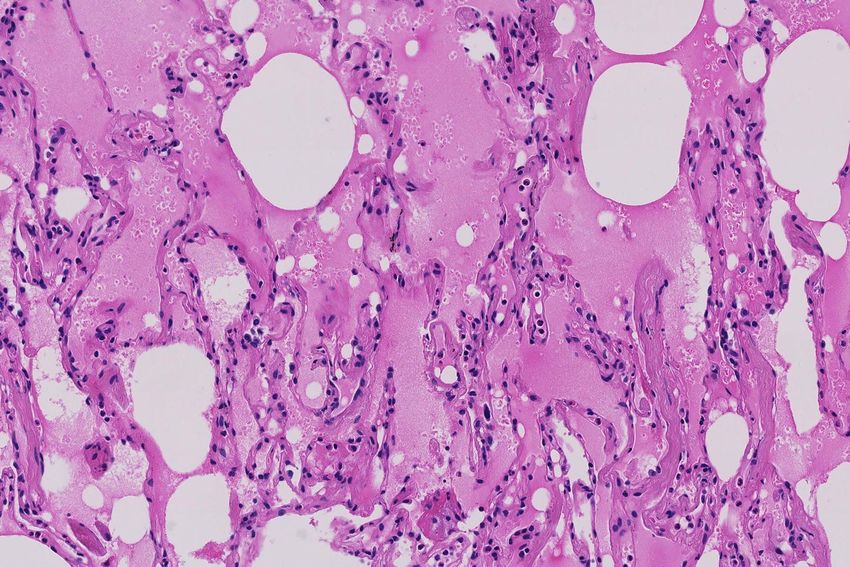
How might SARS-CoV-2 kill you?
• Initial flu-like symptoms of sore throat, cough, fever, aches,
shortness of breath, anosmia are common. In severe cases it
spreads to lungs causing pneumonia (top image).
• Symptom onset 4-8 days (mean 6 days) after infection
(doi.org/10.1101/2020.03.15.20036707).
• Wide variety in symptom severity:
– 33%–50% asymptomatic
– 5%–10% severe, requiring hospitalization and
supplemental O2
– 2.5% critical, requiring ICU and mechanical ventilation
– 1% fatal due either to alveolar breakdown (ARDS, bottom) ±
cytokine release syndrome and multiorgan failure
• Good summaries: nyti.ms/38HYt8Y, www.usatoday.com/in-
depth/news/2020/03/13/what-coronavirus-does-body-covid-
19-infection-process-symptoms/5009057002
3/31/20 Michael Lin, PhD-MD 8
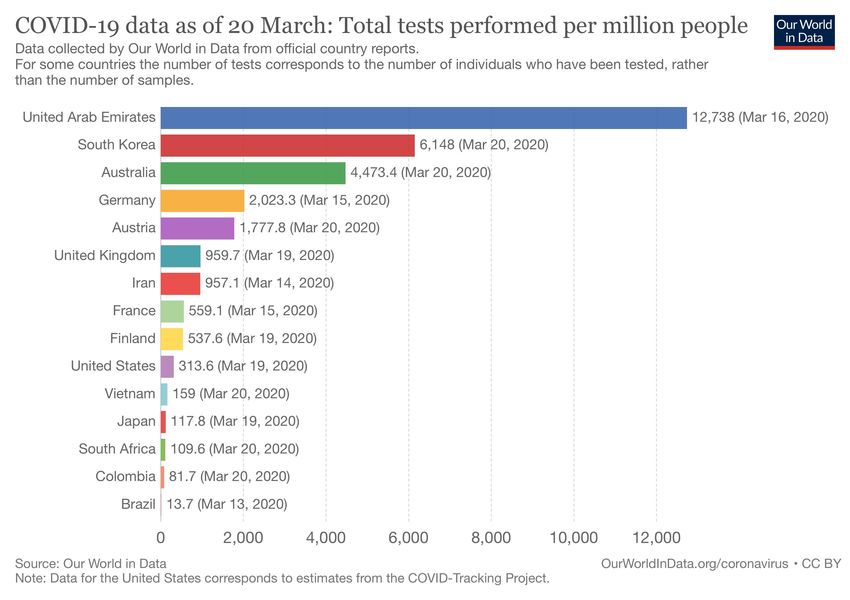
Estimating infection (not disease) numbers
• What matters is # of SARS-COV-2 infections, not diagnosed COVID-19 cases, because infections determine
transmission and immunity rate: The higher it is, the more transmission risk but also the more immunity.
• South Korea (SK) has done extensive testing and tracking (left), and has a large enough epidemic to provide data.
• Deaths on average will lag diagnosis by 20 days, (doi.org/10.1038/s41591-020-0822-7). This matches case and
death numbers (below) for SK, confirming testing coverage is in steady-state.
• Current total deaths in SK (~139 total on 3/27) occurred from cases diagnosed on 3/7 or earlier (cumulative
7041). This means case fatality rate (CFR) ~ 139/7041 = 2.0%
• However infections > diagnosed cases, so IFR < 2.0%, depending on what fraction of infections were diagnosed
on 3/7.
“Patient 31”
diagnosed, actual
Tests per infections probably
million people already >1000,
wide testing begins
www.worldometers.info/coronavirus
3/31/20 Michael Lin, PhD-MD 9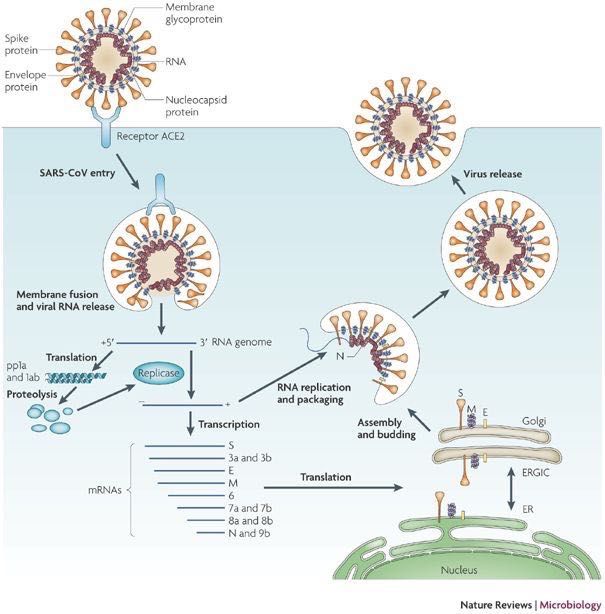
Estimating infection (not disease) numbers • Analyses of China and Diamond Princess (DP) cases gave an IFR of 0.5% for all-China and 1.2% for DP (cmmid.github.io/topics/covid19/severity/diamond_cruise_cfr_estimates.html). • DP passengers skewed old but four may have been helped by the drug remdesivir (www.nhlbi.nih.gov/news/2020/experimental-drug-shows-promise-severely-ill-ship-passengers-coronavirus). • How would US IFR compare to 0.5% for China and
Deaths are mostly in older patients
This is true for both flu and COVID-19
3/31/20 Michael Lin, PhD-MD 11We are entering the middle phase of the epidemic
Estimating new case rates in CA (updated 2020/3/27)
• 82 deaths cumulative: 60 this week (Sat-Fri), 17 last week, 4 last week, 1 two weeks ago
(www.kcra.com/article/coronavirus-covid19-california-sacramento-latest-
information/31406140#).
• Deaths will lag infections by 3–4 weeks (18 days after symptoms but that’s 3–10 days after
infection: www.medrxiv.org/content/10.1101/2020.03.09.20033357v1).
• Assuming constant IFR = 1% with 3- to 4-week delay, there were 6k–12k people in CA infected in
the week ending 3/6. Let’s use a midpoint of 9k.
• After this initial burst, infections would be expected to double each week (average of countries
outside China, wwwnc.cdc.gov/eid/article/26/5/20-0146_article). That means there could have
been 18k new infections in the week ending 3/13, 36k in the week ending 3/20.
• With population 40M, this means up to 1 in 1111 could have gotten infected in CA in the week
ending 3/20. For easy calculation, let’s use 1 in 1024 (you’ll see why).
3/31/20 Michael Lin, PhD-MD 12What if we do nothing?
• If we had done and continue to do nothing, then doubling rate likely 1 week. In worst case, deaths and
infections will grow exponentially until virus runs out of people to infect (using CA-only numbers now):
week ending new infection rate (1/n) new infection rate (%) total infectd (%) weekly deaths total deaths notes
2020-03-20 1024 0.1% 0.4% 17 22
2020-03-27 512 0.2% 0.6% 60 82
2020-04-03 256 0.4% 1.0% 120 202
2020-04-10 128 0.8% 1.8% 240 442
2020-04-17 64 1.6% 3.3% 480 922
2020-04-24 32 3.1% 6.5% 960 1882
2020-05-01 16 6.3% 12.7% 1920 3802
2020-05-08 8 12.5% 25.2% 3840 7642 Cumulative deaths exceed flu, caused by infections before 4/17
2020-05-15 4 25.0% 50.2% 7680 15322 Virus runs out of targets (CA officials estimate 56% final)
2020-05-22 15360 30682
2020-05-29 30720 61402
Deaths continue as they result from infections 3-4 weeks earlier
2020-06-05 61440 122842
2020-06-12 122880 245722
• For US numbers, multiply by 8: ~2M cumulative deaths.
• This is just a simple model for illustration, but it fits the worst-case scenarios by CDC
(nyti.ms/2w1vRKE) and a professional disease modeler (nyti.ms/3a7S2xC).
• You can follow cases (not infection) and fatalities at www.worldometers.info/coronavirus/country/us.
• Compare to Spanish flu of 1917-1918: Cumulative infection rate 27%, IFR 2%. Spanish flu might have
higher IFR than COVID-19, but medical care was much worse then (no ventilators, no drugs). In reality
COVID-19 is likely the more severe disease. In any case, Spanish flu was devastating.
3/31/20 Michael Lin, PhD-MD 13We need to ‘flatten the curve’ now
• Estimated 5% of total infected (not diagnosed cases) require hospitalization (nyti.ms/2w1vRKE) and 2.5% require
ICU. Average hospital stay is 3 weeks, and starts 1 week after diagnosis (2 weeks after infection):
www.vox.com/2020/3/12/21176783/coronavirus-covid-19-deaths-china-treatment-cytokine-storm-syndrome
• Wuhan numbers are 15%/5% of cases, but that is with smoking (60% of males) and pollution (everyone), also
infection rate underdetected by 50% (doi.org/10.1101/2020.03.03.20030593).
• Biggest infection surge occurs in the weeks of 5/1, 5/8, and 5/15, when 6.3%, 12.5%, and 25% of population = 20M,
40M, and 80M get infected. This will result in 1M, 2M, and 4M patients in a hospitalization surge starting 5/15, 5/23,
and 5/30. As patients need to stay ~3 weeks, 7M will overlap on the week starting 5/30.
–We need to ‘flatten the curve’ now The next few weeks are critical: We must do whatever we can to reduce R0 or increase doubling time. Social distancing efforts in CA started 3/20. Since cases are undercounted, we will only know if efforts are working by looking at weekly hospitalization trends 2–3 weeks later (4/10). If hospitalizations are still doubling each week on 4/10, we have only another 3 weeks to get a second chance. If that doesn’t work by 5/1, there will be no third chance. We would have to immediately clamp down to avoid hospital overflow. This would require Wuhan-like measures such as central quarantine for sick and enforced home-isolation for everyone. 3/31/20 Michael Lin, PhD-MD 15
What can flatten the curve?
• Goal is to reduce the reproductive number R0 (how many people infected by each patient).
– Current R0 rate ~ 2 (one person infects 2 others. If they do this in 7 days, it explains doubling time of 1 week).
– Drop R0 to 1.5: Doubling time would increase ~2-fold.
– Drop R0 to 1.25: Doubling time would increase ~4-fold.
– Drop R0 to 1.125: Doubling time would increase ~8-fold.
– Drop R0 to 1.0: Doubling time would become infinite (constant rate of new cases).
• Strict hygiene (including face masks for all), social distancing, extensive testing and tracing, home quarantine of
sick and possible contacts, but continue to work
– This is the approach in SK, Taiwan, Singapore, HK. This seems to have dropped R0 to 1.0 (constant rate of new
cases, www.worldometers.info/coronavirus/country/south-korea/).
• Strict hygiene (including face masks for all), centralized quarantine of sick, strict household isolation and no work.
– In Wuhan, this dropped R0 from 3.9 to 0.32 (www.medrxiv.org/content/10.1101/2020.03.03.20030593v1).
• Is presymptomatic or asymptomatic transmission a factor? Yes, but how much is unclear.
– In Wuhan, R0 fell from 1.3 when symptomatics stayed at home to 0.32 when they were centrally quarantined.
This suggests 24% (0.32/1.3) of transmission events occurred before symptoms. Another study estimates
44% of transmission is by presymptomatics (www.medrxiv.org/content/10.1101/2020.03.15.20036707v2).
– How about asymptomatics? Undiagnosed infected estimated to be ~55% as infectious as diagnosed cases
(doi.org/10.1126/science.abb3221). As undiagnosed infected are more likely asymptomatic than diagnosed
cases, this suggests asymptomatics are not as infectious as symptomatics.
3/31/20 Michael Lin, PhD-MD 16It’s not easy, but good hygiene, social distancing,
fast testing, and immediate quarantining can work!
Cases Deaths
www.bloomberg.com/graphics/2020-coronavirus-cases-world-map
Asian countries have stopped exponential growth more quickly, despite being denser and nearly
completely reliant on public transportation. Why? Some possibilities: faster government response, more
extensive testing, more intrusive tracking, better hygiene (including face masks)...
Note log scale, so straight line = exponential growth. Reliability of case numbers varies a lot – cases are
from testing, the extent of which varies. Death data are more reliable.
3/31/20 Michael Lin, PhD-MD 17SARS-CoV is spread by multiple routes
Virus emission routes Virus reception routes
Direct: Direct:
Emitting airborne droplets Inhaling respiratory
from sneezing, coughing, droplets from infected
talking, mouth-breathing person
Indirect: Indirect:
Touching mouth/nose Touching objects
then touching objects, or contaminated by others,
emitting droplets onto then touching
objects mouth/nose.
Images adapted from science.howstuffworks.com/life/cellular-microscopic/flu2.htm
3/31/20 Michael Lin, PhD-MD 18How might you kill SARS-CoV-2?
SARS-CoV-1
SARS-CoV-2
(Pubmed 32182409)
Survival of SARS-CoV-2 depends on the surface (above)
• 3500 infectious particles (5000 TCID50 units) in 50μL applied, allowed to dry. 1mL cell-culture
media applied and tested.
• On steel and plastic, 10% survives after 12h–24h. No detectable virus (How might you kill SARS-CoV-2?
SARS-CoV-1 dried on tissue-culture plastic
(log10)
(Pubmed 22312351).
38ºC
33ºC
28ºC
20
• Sensitive to temperature (above)
– 10-fold survival decrease with 5ºC
temperature increase (above).
– Killed by 30min 75ºC heat (Pubmed
14631830). 10.1056/NEJMp030078
• Sensitive to UV
– 2–3x more sensitive than influenza virus to • Enveloped virus (with a plasma membrane,
UV (Pubmed 17880524, 16254359). above), dissolved by surfactants/detergents
or 60-80% alcohol, reacted away by bleach.
– Estimated 10-fold survival decrease after 2–
3h direct sunlight.
Michael Lin, PhD-MDHand sanitizer recipe
• Hand sanitizer is just 60-70% ethanol with moisturizers.
• The ethanol you want to use is 95% non-denatured ethanol
– 95% denatured ethanol has toxic additives to prevent drinking (will have a health hazard logo).
– 100%/dehydrated/absolute/anhydrous ethanol has benzene, also toxic, from the purification
process.
• Isopropanol can be substituted for ethanol, but just takes longer to evaporate
– 60-70% isopropanol is just as effective as 60-70% ethanol as a disinfectant.
– 99-100% isopropanol (rubbing alcohol) can be purchased by the consumer as a cleaning and
disinfecting agent.
• The moisturizer can be aloe vera gel (available in drugstores) or glycerol (a common lab reagent,
and an ingredient in moisturizers and makeup).
Lin Lab recipe: Mix two parts 95% non-denatured ethanol or 99-100% isopropanol with 1
part aloe vera gel or 90-100% glycerol. That’s it!
(Thanks to Yichi Su for testing, and Michael Westberg for the safety tips)
3/31/20 Michael Lin, PhD-MD 21Recommendations - hygiene
• Transmission may begin 2 days before symptoms, which is on average 5 days after infection
(doi.org/10.1101/2020.03.15.20036707).
• About 50% of patients will be asymptomatic, based on an estimate from Wuhan data
(doi.org/10.1101/2020.03.03.20030593), and an estimate from passengers on evacuation flights
(doi.org/10.1101/2020.03.09.20033357). Asymptomatic people might be contagious as well for a
short amount of time.
• Thus assume anyone you encounter might be infected and contagious. Exceptions are people in
your household whose hygiene habits you can vouch for.
• Health officials say don’t shake hands and stay 6 ft away from people outside your household –
these are easy.
• But ”wash your hands often” and “don’t touch your face” are confusing without context – how
often is often? Why can’t I touch my face? Should I ask someone to scratch my itchy nose for me?
Shouldn’t I also worry about what I’m touching, not just my hands? If so, what cleaning solutions
should I use?
• I’ll provide some answers in the next slides.
3/31/20 Michael Lin, PhD-MD 22Detailed recommendations - hygiene
I recommend paying strict attention to keeping both hands and objects clean:
• Avoid touching commonly touched objects, e.g. open doors with your body or foot, and use paper
towels to handle faucets or knobs if convenient.
• When you do touch something that is not yours, sanitize your hands immediately. Also sanitize objects
you get from others. For example, I have hand sanitizer open and ready to clean my credit card right
after I get them back from cashiers, before I put it back in my wallet.
• Sanitization can be done by soap and water (hands) or hand sanitizer (hands or objects) or Windex or
60%–80% alcohol (objects). Cardboard items are hard to sanitize, so I suggest “quarantining” them for
2 days (and sanitizing your hands after handling them).
• If you cannot avoid touching some surface repeatedly (e.g. tables and chair edges, wherever you put
your phone and computer) sanitize the surface.
• Keep track of whether hands/objects are clean. As long as they have not encounted unknown/dirty
things after their last cleaning, they don’t need to be recleaned. This is why I suggest immediate
sanitation of hands after touching unknown/dirty things, so you can resume using your own clean
things without worry. Create clean zones, e.g. your house, your car.
• “Disinfectants” like bleach or quarternary amines are for large areas hard to cover with soap or alcohol.
If you can use soap or alcohol, you don’t need them, e.g. no need to dip your hands in bleach.
• To protect others, use clean hands to touch others’ things or when handling things to others. Hand
others only things you know to be clean.
• Finally, if your hands are clean, you can touch your face! But remember to sanitize them before
touching other people’s stuff.
3/31/20 Michael Lin, PhD-MD 23Detailed recommendations – face masks
Face masks: yes or no?
• You will see news articles saying that you don’t need face masks as they are largely ineffective, or
that you shouldn’t buy face masks because caregivers need them.
• These statements cannot both be true! If face masks are ineffective why do caregivers need them?
• Well, they are effective (nyti.ms/2GeMUMy)
– In addition to spreading through contact and then ingestion, SARS-CoV-2 also spreads
through inhalation of airborne droplets.
– Disposable masks are filters, causing bacteria and droplets to be caught in a meshwork of
polypropylene. They are not rated for completely filtering out aerosolized viruses, i.e.
individual viruses in a small water shell. There is some evidence SARS-CoV-2 can be
aerosolized, but its mode of spread is mostly through larger droplets.
– Masks absorb 95% of exhaled droplets from infected people (Pubmed 23505369).
– Masks also absorb droplets during inhalation; this is harder to quantify but certainly
substantial, as masks cut transmission within households by 60-80%, a situation with lots of
viral droplets around (Pubmed 19193267) .
– Both surgical masks and N95 respirators are effective (Pubmed 19797474), although it’s
assumed the N95 are better.
– Update 3/28: In the SARS epidemic, wearing face masks was more effective than washing
hands 10 times daily (nyti.ms/2UAodz6)
3/31/20 Michael Lin, PhD-MD 24Detailed recommendations – face masks
• My recommendations for mask usage are based on relative risks:
– Wearing masks may make a small difference if you see only a few people, and they are healthy.
– But masks are useful when trapped with many strangers (airplane, train, especially hospital/clinic), or
when encountering someone more likely to contract the virus (Uber/Lyft driver, cashier).
– They are warranted for at-risk people, i.e. the immunocompromised or elderly, in public.
– If infection rates climb then they would be useful for everybody out in public.
– They are essential for people who are sick to avoid transmitting viruses.
• Mask use is controversial only because of limited supply:
– To assure those who need masks most get them, try to conserve them, and buy a small supply.
– It is better to do social distancing without masks than social crowding with masks. In Asia, where
most people take public transport, masks are considered necessary and are provided by authorities.
– Given that some people are more at-risk, there should be no stigma/shaming for wearing masks.
– 3/19 update: my views have now been validated by former FDA commissioner Scott Gottlieb
(twitter.com/ScottGottliebMD/status/1240243298725486592). You can only deny facts for so long.
• What if you don’t have masks, and the stranger next to you is coughing?
– You can breathe through the sleeve of your shirt in your elbow.
– You do this in a smelly or smoky location, right? That means it’s effective at blocking small particles.
– Indeed, a T-shirt blocks 70% of virus-sized particles, which is better than nothing (Pubmed 24229526)
3/31/20 Michael Lin, PhD-MD 25Detailed recommendations – face masks
• How to use masks
– Make sure to clean your hands well before putting on or taking off masks.
– For the soft surgical masks, bend the hard edge to fit your nose (colored side out), put on your
nose and pull the straps over your ears, then stretch the mask down to cover your chin.
• How to conserve face masks
– Disposable masks are meant to be worn “once” then throw away, but once is not defined. To
conserve, it’s reasonable to use one mask one day if you’re not seeing patients. (Quarantine
officials forced Grand Princess passengers to use one mask for 9 days: reut.rs/39RVWuy. I
would not recommend that at all.)
– When alone, use clean hands to lower the mask to your chin. This gives a chance for the mask
to dry out, which makes it more effective. You can also do the same when you need to drink.
– When eating, you don’t want stuff dropping from the mask onto your food, so remove the mask
completely and set in a clean place outside-up.
– As the outside of a used mask is potentially dirty, you should clean your hands after touching it,
or you can have your hands wet with hand sanitizer the whole time you handle it.
3/31/20 Michael Lin, PhD-MD 26Face masks can be reused How to decontaminate masks • Alternate use among several masks. After using one, put it in its own bag to let virus decay for several days. This is best if you aren’t sharing your mask with anybody else to avoid unsavory bacteria. • For rapid decontamination: place in oven at 70ºC = 160ºF for 30-60min, or put in a steamer (not in boiling water, but the staem above it) for 10min, or expose both sides in a UV sterilizer (40W 2ft away). Mask efficacy is unaffected by these treatments (right). • Alcohol and bleach are not recommended as they affect the electrostatic membrane that assists with virus filtration (right). 3/20 update: To protect against objections of rule-lovers, I’ll point out that UV sterilization and reuse of masks is now being done by hospitals (nyti.ms/3b8C1HQ). 3/31/20 Michael Lin, PhD-MD 27
Summary: knowing how SARS-CoV-2 is
spread enables rational countermeasures
Virus emission routes Virus reception routes
Direct: Direct:
Emitting airborne droplets 1 4 Inhaling respiratory
from sneezing, coughing, droplets from infected
talking, mouth-breathing person
① Wear a mask! ④ Wear a mask!
Indirect: Indirect:
Touching mouth/nose Touching objects
then touching objects, or contaminated by others,
emitting droplets onto then touching
objects mouth/nose.
② Clean hands before 2 1 5 ⑤ Clean your hands after
touching shared objects! 3 6 touching shared objects!
③ Clean shared objects ⑥ Clean shared objects
after touching! before touching!
Images adapted from science.howstuffworks.com/life/cellular-microscopic/flu2.htm
3/31/20 Michael Lin, PhD-MD 28Recommendations - activities
• It’s okay to go out to buy essentials, get takeout, but assume anything can be carrying virus, so
practice good hygiene as above, i.e. maintain 6ft separation, wear a mask, sanitize hands in between
touching others’ things and your own things, pass only clean objects, and treat objects you acquire as
dirty. Visiting the workplace should be fine if you work mostly alone and can take the same hygiene
steps above. (3/19 update: CA citizens cannot go to workplaces except for some essential jobs.)
• It’s okay to see relatives who are not sick to provide help, but again only if you can practice good
hygiene. Limit duration and closeness of visits to elderly or immunocompromised relatives.
• I have reversed my allowance for social visits to friends, given that many feel it’s uncool to practice
good hygiene such as wearing face masks, not touching common objects. (3/19 update: Also not
allowed in CA anymore.)
• Buy groceries online. Ironically stay-in orders increase transmission risk at grocery stores, which are
now packed. My estimate is 1 in ~1000 carried infections in mid-March. That number can pass
through one store daily. If you must go, stay 6ft from others, wear a mask, and sanitize hands and
purchases!
• I suggest avoiding prepared salads or sandwiches, and retoasting/microwaving pastries.
• Don’t share food, obviously.
• Go outside – sunlight is the best disinfectant.
• Do safer activities – this is not the time you want to break a leg and have to go to the hospital.
3/31/20 Michael Lin, PhD-MD 29Recommendations – travel
• Large meetings that bring people from around the country are were obviously a big risk:
– Large numbers of people who might breath the same air and touch the same things (e.g. at
Biogen meeting, attendants used the same serving utensils at a buffet, and 70 got infected).
– These people tend to travel many times so they can spread viruses further.
– Viruses can be collected from many locations and transmitted to many others (e.g. Biogen).
– Thus non-urgent meetings should be cancelled.
– 3/16 update: Obviously no more conferences/festivals for a while.
• Travel if you must, e.g. to help care for family (3/17 update: removed nonessential travel in
compliance with most health officials’ directives). Students also need to go home! But due to the
many points when exposure from strangers can occur, travel requires high vigilance. For example,
sanitizing items that others give to you now includes your ID at the TSA checkpoint and the can
of soda from the flight attendant. Sanitizing surfaces you touch now include tray tables, seat
belts, armrests. Keeping your hands clean when touching your own things now means washing
hands after closing the airplane bathroom door (because you don’t want germs on your zippers)
and, after washing hands after finishing, opening the same door with your elbow (or a napkin).
Make sure the ventilation nozzle is on full blast (it puts out HEPA-filtered air), and sanitize your
hands after touching it, of course.
• Similar hygienic tips apply to trains and buses and cars that are not your own.
• A face mask is useful in cars with others, trains, planes, crowded waiting areas.
3/31/20 Michael Lin, PhD-MD 30Recommendations - health
• Be on the lookout for CoVID19
symptoms (right).
• Some have anosmia (loss of
sense of smell) as the only
symptom, but this can also occur
with colds Common**
(slate.com/technology/2020/03/
coronavirus-sense-of-smell-
nytimes-fact-check.html).
• If you have any symptoms, try to
get tested. Meanwhile,
quarantine yourself to the Sometimes**
greatest extent possible, or at
least practice strict hygiene, until
you know your test results.
• Recall that even if you have mild
symptoms you do not want to
transmit the virus to others. ** My corrections, original chart said “No” or ”Rare”
3/31/20 Michael Lin, PhD-MD 31No need to worry about supplies • 90–95% of infected people recover without going to the hospital • 33–50% will have no symptoms but will become immune • The workforce is not threatened • Farmers and truck drivers and store workers can still work • You don’t need to buy everything in sight • This is not the zombie apocalypse 3/31/20 Michael Lin, PhD-MD 32
Previous research suggests potentially
useful drugs
MERS-CoV SARS-CoV-1 in mice
SARS-CoV-1 SARS-CoV-2
Camostat
• Inhibits TMPRSS2, one of two host proteases that cleave the spike protein to initiate membrane fusion.
• Inhibits SARS-CoV-2 cell entry with EC50 = 1000 nM (left, from doi.org/10.1016/j.cell.2020.02.052).
• Also helps prevent death in mice with SARS-CoV-1 (right, Pubmed 25666761).
• Camostat approved in Japan for pancreatitis.
• In trials in Denmark (clinicaltrials.gov/ct2/show/NCT04321096)
3/31/20 Michael Lin, PhD-MD 33Previous research suggests potentially
useful drugs
SARS-CoV-2 in human cells Chloroquine (CQ) and hydroxychloroquine (HCQ)
• Inhibits endosome acidification, used worldwide to prevent malaria.
• Inhibits SARS-CoV-2 in human cells, EC50 = 1.13 μM (top).
• Inhibits cold virus CoV OC43 in mice (Pubmed 19506054) but not
SARS-CoV-1 in mice (Pubmed 17176632).
• Results in patients lack details or not well controlled:
Pubmed
– 2020-02-17: Chinese health authorities announced CQ superior to
32020029
control in improving lung imaging, clearing virus, and shortening
disease in trials with >100 patients, but data not shown (Pubmed
SARS-CoV-2 in humans 32074550).
– 2020-03-17: Patients receiving HCQ + azithromycin reduced viral
titers faster in a 21-patient French trial (bottom), but not blinded or
randomized (bottom).
– 2020-03-31: None of 31 patients on HCQ progressed to severe
disease vs 5 of 31 patients in control arm in a blinded and randomized
trial (doi.org/10.1101/2020.03.22.20040758).
• In 23 trials globally, including prevention trials in MN
(abcn.ws/2xnanIA), treatment trials in NY and MN (abcn.ws/2xnanIA).
doi.org/10.1016/j.ijantimicag.2020.105949) • Both CQ and HCQ in MGH treatment guidelines
(www.massgeneral.org/news/coronavirus/treatment-guidances)
3/31/20 Michael Lin, PhD-MD 34Previous research suggests potentially
useful drugs
SARS-CoV-2 in human cells
Favipiravir/favilavir/Avigan/T-705 (Fujifilm Toyama)
• Purine analog, conjugated to ribose to make a ribonucleoside
analog, broad activity against RNA viral polymerases
(RpRd’s/replicases)
• Activity against SARS-CoV-2 in human cells, EC50 = 61.88 μM
(right). Cmax = 400 μM in humans with oral dosing (Pubmed
26798032). Pubmed
32020029
• Reported results in patients not well controlled:
– 2020-03-17: Chinese authorities announced efficacy against COVID-19, with 8% favipiravir patients vs
17% control requiring ventilators, and 91% vs 62% improving on lung imaging, but not randomized, not
blinded (www.medicalnewstoday.com/articles/anti-flu-drug-effective-in-treating-covid-19).
– Superior to influenza inhibitor arbidol in a randomized open-label trial
(doi.org/10.1101/2020.03.17.20037432).
– Stockpiled for influenza outbreaks in Japan, but not available for general prescription.
– In 11 trials in Asia
3/31/20 Michael Lin, PhD-MD 35Previous research suggests potentially
useful drugs
SARS-CoV-2 in human cells Remdesivir (Gilead)
• Inhibits many viral RNA-dependent RNA polymerases
(RdRp’s/replicases).
• Works against SARS-CoV-2 in cells, EC50 = 0.77 μM (top)
• Inhibits SARS-CoV-1 replication in mice (bottom)
Pubmed • SARS-CoV-1 RdRp and SARS-CoV-2 RdRp are 96% identical
32020029 • Inhibits MERS virus in rhesus monkeys (Pubmed 32054787)
• Anecdotal benefits in COVID-19 patients
(science.sciencemag.org/content/367/6485/1412).
SARS-CoV-1 • In randomized controlled trials in USA and globally, China results due
in mice mid-April (www.google.com/search?q=usatoday+2934583001),
• Widely recommended in treatment guidelines if obtainable
(www.massgeneral.org/news/coronavirus/treatment-guidances)
Pubmed
28931657
3/31/20 Michael Lin, PhD-MD 36Previous research suggests potentially
useful drugs
SARS-CoV-1 in cells Kaletra (lopinavir+ritonavir)
• HIV protease inhibitor approved worldwide.
• Lopinavir nhibits SARS-CoV-1 in cells (top).
• Patients receiving lopinavir+ritonavir had better
Pubmed outcomes vs historical controls (bottom).
14985565 • Proposed to inhibit SARS-CoV-2 M protease
(doi.org/10.1101/2020.01.29.924100), but this
lacks homology with HIV protease.
• Failed in 199-patient randomized controlled trial
SARS patients in China (Pubmed 32187464).
• Not recommended by MGH
lopinavir
(www.massgeneral.org/news/coronavirus/treat
+ ritonavir ment-guidances)
+ ribavirin
Pubmed • In 6 trials in Asia, in INSERM Discovery trials, and
14985565 in WHO SOLIDARITY trials (shar.es/aH7mNg,
NCT04315948).
ribavirin
historical
control
3/31/20 Michael Lin, PhD-MD 37Existing drugs may be useful for COVID-19
complications
• With high virus levels in the lungs, death is often from cytokine release syndrome (CRS, cytokine storm)
– Massive cytokine release by immune cells causes multi-organ failure (Pubmed 32192578).
– Anti-IL-6 mAb tocilizumab (Roche) recommended in China (pharmaphorum.com/?p=64910)
– Anti-IL-6 mAb sarilumab (Sanofi) recommended by MGH
(www.massgeneral.org/news/coronavirus/treatment-guidances)
• Losartan proposed to be either beneficial and harmful for COVID-19 patients. Losartan blocks AT1R,
causing cells to upregulate ACE2, the receptor for SARS-CoV-2, in response.
– SARS lethality had been proposed to be from downregulation of ACE2 contributing to acute
respiratory distress syndrome (www.nature.com/articles/nrd1830). However, the only evidence is
one study in mice; how well mice model human disease physiology is unclear.
– Some propose that SARS-CoV-2 will also downregulate ACE2 and restoring it may be beneficial
(Pubmed 32129518). Thus losartan is being tested in COVID-19 (strib.mn/2IFZ2Wz) and
recombinant ACE2 in China (NCT04287686).
– Others have suggested the opposite, that upregulating ACE2 with losartan might increase
susceptibility to the infection (Pubmed 32171062). However it’s not clear that virus entry is limited by
the number of ACE2 molecules per cell once the virus is on oral and lung epithelia.
– I predict losartan’s not going to make a significant difference either way; it’s like arguing over
deck chair arrangements on the Titanic. It’s better to concentrate on specific antiviral
medications and not fiddle with the complex ACE2/AT1R pathway.
3/31/20 Michael Lin, PhD-MD 38New treatments and vaccines are in
development
• Specific anti-viral antibodies (Vir Biotechnology, Regeneron) made by cloning Ig genes from recovered
COVID-19 patients can be used for prophylatic immunization or therapy.
• Synthetic antibody-like molecules isolated against the SARS-CoV-2 spike protein by phage display are
possible.
• Additional SARS-CoV-1 replicase/polymerase and protease inhibitors had been developed and can be quickly
resurrected for clinical trials (doi.org/10.1021/acscentsci.0c00272) or further improved.
• Multiple drug hits from virtual screens (www.google.com/search?q=covid+virtual+drug+screening).
• Many vaccines in development (www.nature.com/articles/d41587-020-00005-z):
– Among the fastest are RNA-based (CureVac, Moderna), efficacy readout as soon as 2020 summer.
– Whole-killed/inactivated virus vaccines may be just as fast, but there is concern that some viral
components may elicit an undesirable Th2-type allergic response (Pubmed 23252385).
• Some more summary and speculation here: doi.org/10.1021/acscentsci.0c00272
3/31/20 Michael Lin, PhD-MD 39Summary 1. The causative agent of COVID-19, SARS-CoV-2, is very similar to the SARS virus SARS-CoV-1. 2. The virus life cycle reveals possible targets for inhibition 3. Disease outcomes range from asymptomatic to flu-like to fatal; presymptomatic transmission is possible. 4. COVID-19 transmission likely occurs similarly to SARS and influenza. 5. As an enveloped virus, SARS-CoV-2 is environmentally sensitive and directly disrupted by surfactants/detergents and solvents. 6. Keeping hands and objects clean, and avoiding inhaling contaminated droplets, will dramatically cut down transmission. 7. No drugs have proven benefit for COVID-19 yet, but there are several promising candidates from past work on SARS and MERS. 3/31/20 Michael Lin, PhD-MD 40
You can also read