COVID-19 Monoclonal Antibody Infusions: A Multidisciplinary Initiative to Operationalize EUA Novel Treatment Options - MDedge
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Reports From the Field
COVID-19 Monoclonal Antibody Infusions:
A Multidisciplinary Initiative to Operationalize
EUA Novel Treatment Options
Kathleen Jodoin, PharmD, BCPS, David Farcy, MD, Ana Caldera, PharmD, Michael Dalley, DO,
Brijesh Patel, MD, Wendy Stuart, RN, Gustavo Tejas, RN, Michael Atisha, RN,
Tarang Kheradia, MBBS, Erich Glasbrenner, RN, and Robert Goldszer, MD, MBA
ABSTRACT and measuring and reporting quality improvement on a
regular basis.
Objective: To develop and implement a process for
administering COVID-19 monoclonal antibody infusions for Results: A total of 790 COVID-19 monoclonal antibody infusions
outpatients with mild or moderate COVID-19 at high risk were administered from November 20, 2020 to March 5,
for hospitalization, using multidisciplinary collaboration, 2021. Steps to minimize the likelihood of adverse drug
US Food and Drug Administration (FDA) guidance, and reactions were implemented and a low incidence (<
infection prevention standards. 1%) has occurred. There has been no concern from staff
regarding infection during the process. Rarely, patients have
Methods: When monoclonal antibody therapy became
raised cost-related concerns, typically due to incomplete
available for mild or moderate COVID-19 outpatients
communication regarding billing prior to the infusion. Patients,
via Emergency Use Authorization (EUA), our institution
families, nursing staff, physicians, pharmacy, and hospital
sought to provide this therapy option to our patients.
administration have expressed satisfaction with the program.
We describe the process for planning, implementing,
and maintaining a successful program for administering Conclusion: This process can provide a template for other
novel therapies based on FDA guidance and infection hospitals or health care delivery facilities to provide novel
prevention standards. Keys components of our therapies to patients with mild or moderate COVID-19 in a
implementation process were multidisciplinary planning safe and effective manner.
involving decision makers and stakeholders; setting Keywords: COVID-19; monoclonal antibody; infusion;
emergency use authorization.
realistic goals in the process; team communication;
S
ARS-CoV-2 and the disease it causes, COVID- which more than 527,000 deaths have occurred in the
19, have transformed from scientific vernacular to United States.1 This novel virus has resulted in a flurry of
common household terms. It began with a cluster literature, research, therapies, and collaboration across
of pneumonia cases of unknown etiology in December multiple disciplines in an effort to prevent, treat, and mit-
2019 in Wuhan, China, with physicians there reporting igate cases and complications of this disease.
a novel coronavirus strain (2019-nCoV), now referred to On November 9, 2020, and November 21, 2020,
as SARS-CoV-2. Rapid spread of this virus resulted in the US Food and Drug Administration (FDA) issued
the World Health Organization (WHO) declaring an inter- Emergency Use Authorizations (EUA) for 2 novel COVID-
national public health emergency. Since this time, the 19 monoclonal therapies, bamlanivimab2-3 and casiriv-
virus has evolved into a worldwide pandemic. COVID- imab/imdevimab,3-4 respectively. The EUAs granted
19 has dramatically impacted our society, resulting in
more than 2.63 million global deaths as of this writing, of From Mount Sinai Medical Center, Miami Beach, FL.
70 JCOM March/April 2021 Vol. 28, No. 2 www.mdedge.com/jcomjournal
Reports From the Field
permission for these therapies to be administered for patients who are hospitalized or who require oxygen
the treatment of mild to moderate COVID-19 in adult therapy due to COVID-19. Therefore, options for out-
and pediatric patients (≥ 12 years and weighing at least patient administration needed to be evaluated. Directly
40 kg) with positive results of direct SARS-CoV-2 viral following the first EUA press release, a task force of
testing and who are at high risk for progressing to severe key stakeholders was assembled to brainstorm and
COVID-19 and/or hospitalization. The therapies work by develop a process to offer this therapy to the commu-
targeting the SARS-CoV-2 spike protein and subsequent nity. A multidisciplinary task force with representation
attachment to human angiotensin-converting enzyme 2 from the ED, nursing, primary care, hospital medicine,
receptors. Clinical trial data leading to the EUA demon- pharmacy, risk management, billing, information tech-
strated a reduction in viral load, safe outcome, and most nology, infection prevention, and senior level leadership
importantly, fewer hospitalization and emergency room participated (Table).
visits, as compared to the placebo group.5-7 The use of The task force reviewed institutional outpatient loca-
monoclonal antibodies is not new and gained recognition tions to determine whether offering this service would
during the Ebola crisis, when the monoclonal antibody be feasible (eg, ED, ambulatory care facilities, cancer
to the Ebola virus showed a significant survival bene- center). The ED was selected because it would offer
fit.8 Providing monoclonal antibody therapy soon after the largest array of appointment times to meet the
symptom onset aligns with a shift from the onset of the community needs with around-the-clock availability.
pandemic to the current focus on the administration of While Mount Sinai Medical Center offers care in 3
pharmaceutical therapy early in the disease course. This emergency center locations in Aventura, Hialeah, and
shift prevents progression to severe COVID-19, with the Miami Beach, it was determined to initiate the infusions
goal of reducing patient mortality, hospitalizations, and at the main campus center in Miami Beach only. The
strain on health care systems. main campus affords an onsite pharmacy with suitable
The availability of novel neutralizing monoclonal staffing to prepare the anticipated volume of infusions in
antibodies for COVID-19 led to discussions of how to a timely manner, as both therapies have short stabilities
incorporate these therapies as new options for patients. following preparation. Thus, it was decided that patients
Our institution networked with colleagues from multiple from freestanding emergency centers in Aventura and
disciplines to discuss processes and policies for the Hialeah would be moved to the Miami Beach ED loca-
safe administration of the monoclonal antibody infu- tion to receive therapy. Operating at a single site also
sion therapies. Federal health leaders urge more use allowed for more rapid implementation, monitoring, and
of monoclonal antibodies, but many hospitals have ability to make modifications more easily. Discussions
been unable to successfully implement infusions due to for the possible expansion of COVID-19 monoclonal
staff and logistical challenges.9 This article presents a antibody infusions at satellite locations are underway.
viable process that hospitals can use to provide these On November 20, 2020, 11 days after the formation
novel therapies to outpatients with mild to moderate of the multidisciplinary task force, the first COVID-19
COVID-19. monoclonal infusion was successfully administered.
Figure 1 depicts the timeline from assessment to pro-
The Mount Sinai Medical Center, gram implementation. Critical to implementation was
Florida Experience the involvement of decision makers from all necessary
Mount Sinai Medical Center in Miami Beach, Florida, is departments early in the planning process to ensure that
the largest private, independent, not-for-profit teaching standard operating procedures were followed and that
hospital in South Florida, comprising 672 licensed beds the patients, community, and organization had a posi-
and supporting 150,000 emergency department (ED) tive experience. This allowed for simultaneous planning
visits annually. Per the EUA criteria for use, COVID-19 of electronic health record (Epic; EHR) builds, depart-
monoclonal antibody therapies are not authorized for mental workflows, and staff education, as described in
www.mdedge.com/jcomjournal Vol. 28, No. 2 March/April 2021 JCOM 71
COVID-19 Monoclonal Antibody Infusions
Table. List of Key Stakeholders and Responsibilities
Department or position Responsibility
Chief Nursing Officer Decision maker on go or no go, nursing involvement
Chief Medical Officer Decision maker on go or no go, physician involvement
Director of Pharmacy Decision maker on go or no go, pharmacy involvement
Pharmacy Clinical Coordinator Implementation process including preparation, delivery, patient safety and peer education
Chair of Emergency Medicine ED process and physician education and oversight
Chief of General Medicine Referring physician education and oversight
Emergency Medicine Nursing ED nursing staffing, education, safety and process
Emergency Medicine Residents ED process, learning, clinician input, peer education
Infection Prevention Infection prevention and education
Information Technology Medication order, order sets, documentation, interfaces as needed, and clinician education
Patient Registration Correctly and safely register and schedule all patients
Revenue Cycle Appropriate billing and assessment of expenses
Security Patient and staff safety
ED, emergency department.
the following section. Figure 2 shows the patient safety developed and reviewed by pharmacy administration
activities included in the implementation process. and ED nursing leadership for input, prior to submit-
ting to the information technology team for implemen-
Key Stakeholder Involvement and Workflow tation. Building the COVID-19 monoclonal medication
On the day of bamlanivimab EUA release, email com- records into the EHR allowed for detailed direction
munication was shared among hospital leadership with (ie, administration and preparation instructions) to be
details of the press release. Departments were quickly consistently applied. The medication records were also
involved to initiate a task force to assess if and how this built into hospital smart pumps so that nurses could
therapy could be offered at Mount Sinai Medical Center. access prepopulated, accurate volumes and infusion
The following sections explain the role of each stake- rates to minimize errors.
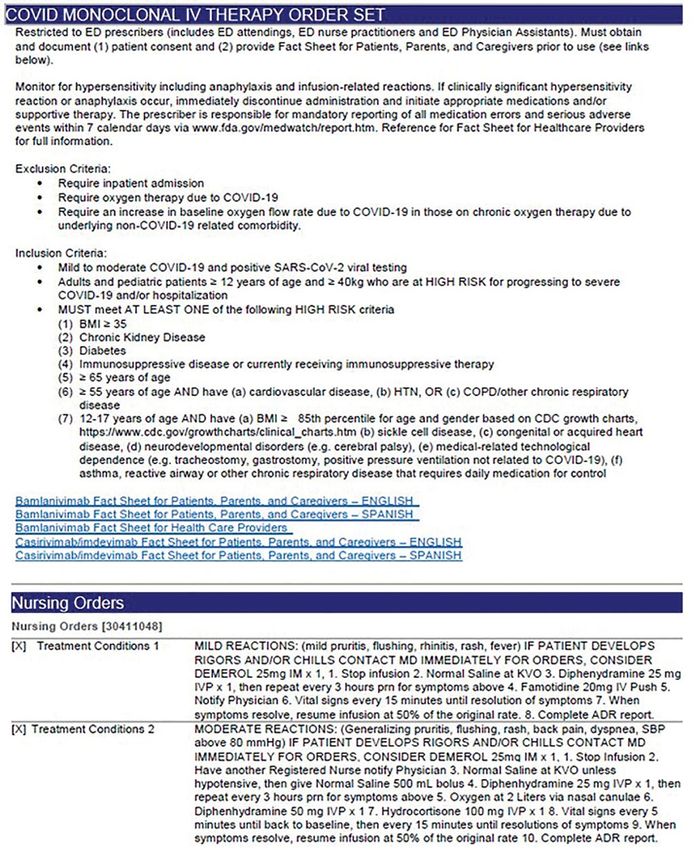
holder and their essential role to operationalize these Order Set Development. The pharmacy medication
novel EUA treatment options. The task force was orga- build was added to a comprehensive order set (Figure
nized and led by our chief medical officer and chief nurs- 3), which was then developed to guide prescribers and
ing officer. standardize the process around ordering of COVID-19
monoclonal therapies. While these therapies are new,
Information Technology oncology monoclonal therapies are regularly adminis-
Medication Ordering and Documentation EHR tered to outpatients at Mount Sinai Cancer Center. The
and Smart Pumps. Early in the pandemic, the antimi- cancer center was therefore consulted on their process
crobial stewardship (ASP) clinical coordinator became surrounding best practices in administration of mono-
the designated point person for pharmacy assessment clonal antibody therapies. This included protocols for
of novel COVID-19 therapies. As such, this pharma- medications used in pretreatment and management of
cist began reviewing the bamlanivimab and, later, the hypersensitivity reactions and potential adverse drug
casirivimab/imdevimab EUA Fact Sheet for Health Care reactions of both COVID-19 monoclonal therapies.
Providers. All necessary elements for the complete and These medication orders were selected by default in the
safe ordering and dispensing of the medication were order set to ensure that all patients received premedi-
72 JCOM March/April 2021 Vol. 28, No. 2 www.mdedge.com/jcomjournal
Reports From the Field
11/09/20 11/10/20 11/10/20-11/18/20
Bamlanivimab Multidisciplinary task Stakeholders create
receives EUA force established and finalize workflow
11/19/20
11/20/20 11/18/20
Order set live in EHR
First infusion P&T committee
and medication delivered
administered approves order set
from DOH
Figure 1. Process implementation timeline. EUA, Emergency Use Authorization; P&T, Pharmacy and Therapeutics; DOH, department
of health; EHR, electronic health record.
cations aimed at minimizing the risk of hypersensitivity Preliminary Assessment Tool. A provider assess-
reaction, and had as-needed medication orders, in the ment tool was developed to document patient-specific
event a hypersensitivity reaction occurred. Reducing EUA criteria for use during initial assessment (Figure 4).
hypersensitivity reaction risk is important as well to This tool serves as a checklist and is visible to the full
increase the likelihood that the patient would receive full multidisciplinary team in the patient’s EHR. It is used as
therapy, as management of this adverse drug reactions a resource at the time of pharmacist verification and ED
involves possible cessation of therapy depending on physician assessment to ensure criteria for use are met.
the level of severity. The pharmacy department also
ensured these medications were stocked in ED auto- Outpatient Offices
mated dispensing cabinets to promote quick access. Patient Referral. Patients with symptoms or concerns
In addition to the aforementioned nursing orders, we of COVID-19 exposure can make physician appoint-
added EUA criteria for use and hyperlinks to the Fact ments via telemedicine or in person at Mount Sinai
Sheets for Patients and Caregivers and Health Care Medical Center’s primary care and specialty offices.
Providers for each monoclonal therapy, and restricted At the time of patient encounter, physicians suspecting
ordering to ED physicians, nurse practitioners, and phy- a COVID-19 diagnosis will refer patients for outpatient
sician assistants. COVID-19 polymerase chain reaction (PCR) laboratory
The order set underwent multidisciplinary review by testing, which has an approximate 24-hour turnaround
pharmacy administration, the chair of emergency medi- to results. Physicians also assess whether the patient
cine, physicians, and ED nursing leadership prior to pre- meets EUA criteria for use, pending results of testing.
sentation and approval by the Pharmacy and Therapeutics In the event a patient meets EUA criteria for use, the
Committee. Lastly, at time of implementation, the order physician provides patient counseling and requests ver-
set was added to the ED preference list, preventing inpa- bal consent. Following this, the physician enters a note
tient access. Additionally, as a patient safety action, free- in the EHR describing the patient’s condition, criteria
standing orders of COVID-19 monoclonal therapies were for use evaluation, and the patient’s verbal agreement
disabled, so providers could only order therapies via the to therapy. This preliminary screening is beneficial to
approved, comprehensive order set. begin planning with both the patient and ED to minimize
www.mdedge.com/jcomjournal Vol. 28, No. 2 March/April 2021 JCOM 73
COVID-19 Monoclonal Antibody Infusions
Order set includes
Order set includes pre-
EUA criteria and easily Freestanding orders
Medication order and meds and as needed
accessible information disabled; medication
comprehensive order set medications to minimize
for staff, prescribers, and orders must be placed as
developed in EHR the risk of ADR (eg,
patients (eg, hyperlinks for part of an order set
hypersensitivity reactions)
FDA fact sheets)
Key screening questions ED clinician to assess
included as hard stops each patient prior to
Ordering restrictions Timely appointments
in physician ordering infusion to ensure patient
implemented to limit to available to initiate therapy
to support real time meets criteria and does
specific prescribers only early (eg, same or next day)
documentation and not need inpatient
education admission
Each COVID-19
Observe staff carefully for monoclonal antibody
Establish a safe place
Ensure all staff have signs of exhaustion, fatigue, therapy is offered on a
for a COVID-19-positive
designated day
patient to stay for the adequate PPE and are and mental and physical
(eg, bamlanivimab on
duration of the encounter trained in proper use stress; provide prevention Tue/Thu/Sat/Sun and
(approximately 4 hours) and relief options casirivimab/imdevimab
on Mon/Wed/Fri)
Vials assembled into kits
Pharmacist reviews notes, Initial and ongoing
(1 kit = 1 dose); kits are
criteria for use, and orders staff education on
labeled with medication
prior to verification and process provided to all
name, number of vials, and
compounding stakeholders
pharmacist signature
Figure 2. Important patient safety initiatives. ADR, adverse drug reaction; ED, emergency department; EHR, electronic health record; EUA, Emergency
Use Authorization; FDA, US Food and Drug Administration; PPE, personal protective equipment.
delays. Patients are notified of the results of their test pretreated with medication that may potentially impair
once available. If the COVID-19 PCR test returns posi- driving, they are instructed that they cannot drive them-
tive, the physician will call the ED at the main campus selves home; ride shares also are not allowed in order to
and schedule the patient for COVID-19 monoclonal ther- limit the spread of infection.
apy. As the desired timeframe for administering COVID-
19 monoclonal therapies is within less than 10 days of Emergency Department
symptom onset, timely scheduling of appointments is Patient Arrival and Screening. A COVID-19 patient can
crucial. Infusion appointments are typically provided the be evaluated in the ED 1 of 2 ways. The first option is via
same or next day. The patients are informed that they outpatient office referral, as described previously. Upon
must bring documentation of their positive COVID-19 arrival to the ED, a second screening is performed to
PCR test to their ED visit. Lastly, because patients are ensure the patient still meets EUA criteria for use and
74 JCOM March/April 2021 Vol. 28, No. 2 www.mdedge.com/jcomjournal
Reports From the Field
Figure 3. COVID-19 monoclonal antibody order set.
© 2021 Epic Systems Corporation.
www.mdedge.com/jcomjournal Vol. 28, No. 2 March/April 2021 JCOM 75COVID-19 Monoclonal Antibody Infusions
Figure 3. (continued)
the positive COVID-19 PCR test result is confirmed. If Otherwise, an in-house COVID-19 PCR test will be per-
the patient no longer meets criteria, the patient is triaged formed, which has a 2-hour turnaround time.
accordingly, including evaluation for higher-level care (eg, Infusion Schedule. The ED offers a total of 16
supplemental oxygen, hospital admission). The second COVID-19 monoclonal infusions slots daily. These are
optoion is via new patient walk-ins without outpatient phy- broken up into 4 infusion time blocks (eg, 8 am, 12 pm,
sician referral (Figure 4). In these cases, an initial screening 4 pm, 8 pm), with each infusion time block consisting
is performed, documenting EUA criteria for use in the pre- of 4 available patient appointments. A list of sched-
liminary assessment (Figure 5). Physicians will consider uled infusions for the day is emailed to the pharmacy
an outside COVID-19 test as valid, so long as documen- department every morning, and patients are instructed
tation is readily available confirming a positive PCR result. to arrive 1 hour prior to their appointment time. This
76 JCOM March/April 2021 Vol. 28, No. 2 www.mdedge.com/jcomjournalReports From the Field
ED triage Overflow ED
Pharmacy notification
of prescheduled
PCP referral infusions
(appointment Infusion ordering
prescheduled)
Patient registration
Medication
Walk-in
administration
Higher level
Patient assessment Main ED
ED referral care needed?
Patient
(appointment
observation
prescheduled) Meets EUA criteria for use?
Patient education
Figure 4. Workflow for COVID-19 monoclonal antibody infusion. This graphic depicts how patients arrive to Mount Sinai Medical Center’s
emergency department (ED) for COVID-19 monoclonal antibody infusion and the associated workflow. Patients are referred from their primary
care provider (PCP), from an ED on a previous visit, or as a walk-in. In the triage area, the patient’s eligibility is assessed. If it is determined the
patient requires higher-level of care, the patient is triaged to a room within our main ED. If it is determined that the patient is a candidate for
COVID-19 monoclonal antibody therapy, the patient is escorted to the overflow ED, which has become a dedicated station within the ED for
treatment, administration, and observation.
allows time for patient registration, assessment, and patients with the option of participating in the institutional
pharmacy notification in advance of order entry. For review board (IRB) approved study. Details of this are dis-
logistical purposes, and as a patient safety initiative to cussed in the risk management and IRB sections of the
reduce the likelihood of medication errors, each of the article. Nursing staff also provides the medication-specific
available COVID-19 monoclonal antibodies is offered on Fact Sheet for Patients and Caregivers in either Spanish
a designated day. Bamlanivimab is offered on Tuesday, or English, which is also included as a hyperlink on the
Thursday, Saturday, and Sunday, while casirivimab/ COVID-19 Monoclonal Antibody Order Set for ease of
imdevimab is offered Monday, Wednesday, and Friday. access. Interpreter services are available for patients who
This provides flexibility to adjust should supply deviate speak other languages. An ED decentralized pharmacist is
based on Department of Health allocation or should also available onsite Monday through Friday from 12 pm to
new therapy options within this class of medication 8:30 pm to supplement education and serve as a resource
become available. for any questions.
Patient Education. Prior to administration of the Infusion Ordering. Once the patient is ready to
monoclonal therapy, physician and nursing staff obtain begin therapy, the he/she is brought to a dedicated
a formal, written patient consent for therapy and provide overflow area of the ED. There are few, if any, patients in
www.mdedge.com/jcomjournal Vol. 28, No. 2 March/April 2021 JCOM 77COVID-19 Monoclonal Antibody Infusions
Figure 5. Electronic health record preliminary assessment.
© 2021 Epic Systems Corporation.
this location, and it is adjacent to the main emergency administer in the event they occur, are detailed in the
center for easy access by the patients, nurses, pharma- nursing orders of the COVID-19 Monoclonal Antibody
cists, and physicians. The physician then enters orders Order Set (Figure 3). Prior to administration, the nurse
in the EHR using the COVID-19 Monoclonal Antibody scans each medication and the patient’s wrist identifi-
Order Set (Figure 3). Three discrete questions were cation band, and documents the time of administration
built into the medication order: (1) Was patient consent within the EHR medication administration report.
obtained? (2) Was the Fact Sheet for Patient/Caregiver
provided to the patient? (3) Is the patient COVID-19 Pharmacy Department
PCR-positive? These questions were built as hard stops Medication Receipt Process. Inventory is currently
so that the medication orders cannot be placed without allocated biweekly from the state department of health
a response. This serves as another double-check to and will soon be transitioning to a direct order system.
ensure processes are followed and helps facilitate timely The pharmacy technician in charge of deliveries notifies
verification by the pharmacist. the pharmacy Antimicrobial Stewardship Program (ASP)
Medication Administration. One nurse is dedicated clinical coordinator upon receipt of the monoclonal
to administering the monoclonal therapies scheduled therapies. Bamlanivimab is supplied as 1 vial per dose,
at 8 am and 12 pm and another at 4 pm and 8 pm. whereas casirivimab/imdevimab is supplied as 4 vials or
Each appointment block is 4 hours in duration to allow 8 vials per dose, depending how it is shipped. To reduce
adequate time for patient registration, infusion, and the likelihood of medication errors, the ASP clinical coor-
postinfusion observation. The nurse administers the dinator assembles each of the casirivimab/imdevimab
premedications and COVID-19 monoclonal therapy, and vials into kits, where 1 kit equals 1 dose. Labels are
observes the patient for the required 1-hour postadmin- then affixed to each kit indicating the medication name,
istration observation period. Nursing orders detailing number of vials which equal a full dose, and pharmacist
monitoring parameters for mild, moderate, and severe signature. The kits are stored in a dedicated refrigerator,
reactions, along with associated medication orders to and inventory logs are affixed to the outside of the refrig-
78 JCOM March/April 2021 Vol. 28, No. 2 www.mdedge.com/jcomjournalReports From the Field
erator and updated daily. This inventory is also commu- nity through teaching, research, charity care, and finan-
nicated daily to ED physician, nursing, and pharmacy cial responsibility, it was determined that this therapy
leadership, as well as the director of patient safety, who would be provided to all patients regardless of insurance
reports weekly usage to the state Department of Health type, including those who are uninsured. The billing and
and Human Services. These weekly reports are used to finance department was consulted prior to this service
determine allocation amounts. being offered, to provide patients with accurate and per-
Medication Verification and Delivery. The Mount tinent information. The billing and finance department
Sinai Medical Center pharmacist staffing model consists provided guidance on how to document patient encoun-
of centralized order entry and specialized, decentralized ters at time of registration to facilitate appropriate billing.
positions. All orders are verified by the ED pharmacist At this time, the medication is free of charge, but non-
when scheduled (not a 24/7 service) and by the designated medication-related ED fees apply. This is explained to
pharmacist for all other times. At the time of medication patients so there is a clear understanding prior to book-
verification, the pharmacist documents patient-specific ing their appointment.
EUA criteria for use and confirms that consent was
obtained and the Fact Sheet for Patients/Caregivers was Infection Prevention
provided. A pharmacist intervention was developed to As patients receiving COVID-19 monoclonal therapies
assist with this documentation. Pharmacists input smart can transmit the virus to others, measures to ensure
text “.COVIDmonoclonal” and a drop-down menu of protection for other patients and staff are vital. To mini-
EUA criteria for use appears. The pharmacist reviews mize exposure, specific nursing and physician staff from
the patient care notes and medication order question the ED are assigned to the treatment of these patients,
responses to ascertain this information, contacting the ED and patients receive infusions and postobservation
prescriber if further clarification is required. This verification monitoring in a designated wing of the ED. Additionally,
serves as another check to ensure processes put in place all staff who interact with these patients are required to
are followed. Lastly, intravenous preparation and delivery don full personal protective equipment. This includes not
are electronically recorded in the EHR, and the medica- only physicians and nurses but all specialties such as
tions require nursing signature at the time of delivery to physician assistants, nurse practitioners, pharmacists,
ensure a formal chain of custody. and laboratory technicians. Moreover, patients are not
permitted to go home in a ride share and are counseled
Risk Management on Centers for Disease Control and Prevention quaran-
At Mount Sinai Medical Center, all EUA and investiga- tining following infusion.
tional therapies require patient consent. Consistent
with this requirement, a COVID-19 monoclonal specific Measurement of Process and Outcomes
consent was developed by risk management. This is and Reporting
provided to every patient receiving a COVID-19 mono- IRB approval was sought and obtained early during
clonal infusion, in addition to the FDA EUA Fact Sheet initiation of this service, allowing study consent to be
for Patients and Caregivers, and documented as part offered to patients at the time general consent was
of their EHR. The questions providers must answer are obtained, which maximized patient recruitment and
built into the order set to ensure this process is followed streamlined workflow. The study is a prospective
and these patient safety checks are incorporated into observational research study to determine the impact of
the workflow. administration of COVID-19 monoclonal antibody ther-
apy on length of symptoms, chronic illness, and rate of
Billing and Finance Department hospitalization. Most patients were eager to participate
In alignment with Mount Sinai Medical Center’s mission and offer their assistance to the scientific community
to provide high-quality health care to its diverse commu- during this pandemic.
www.mdedge.com/jcomjournal Vol. 28, No. 2 March/April 2021 JCOM 79COVID-19 Monoclonal Antibody Infusions
Staff Education of IRB approval allowed the experience to be assessed
In order to successfully implement this multidisciplinary and considered for contribution to the scientific literature to
EUA treatment option, comprehensive staff education tackle this novel virus that has impacted our communities
was paramount after the workflow was developed. locally, nationally, and abroad. Moreover, continued mea-
Prior to the first day of infusions, nurses, and pharma- surement and reporting on a regular basis leads to per-
cists were provided education during multiple huddle formance improvement. The process outlined here can be
announcements. The pharmacy team also provided adapted to incorporate other new therapies in the future,
screen captures via email to the pharmacists so they such as the recent February 9, 2021, EUA of the COVID-
could become familiar with the order set, intervention 19 monoclonal antibody combination bamlanivimab and
documentation, and location of the preliminary assess- etesevimab.10
ment of EUA criteria for use at the time of order ver-
ification. The emergency medicine department chair Conclusion
and chief medical officer also provided education via We administered 790 COVID-19 monoclonal antibody infu-
several virtual meetings and email to referring physi- sions between November 20, 2020 and March 5, 2021.
cians (specialists and primary care) and residents in the Steps to minimize the likelihood of hypersensitivity reac-
emergency centers involved in COVID-19 monoclonal tions were implemented, and a low incidence (< 1%) has
therapy-related patient care. been observed. There has been no incidence of infection,
concern from staff about infection prevention, or risk of
Factors Contributing to Success infection during the processes. There have been very infre-
We believe the reasons for continued success of this pro- quent cost-related concerns raised by patients, typically
cess are multifactorial and include the following key ele- due to incomplete communication regarding billing prior to
ments. Multidisciplinary planning, which included decision the infusion. To address these issues, staff education has
makers and all stakeholders, began at the time the idea was been provided to enhance patient instruction on this topic.
conceived. This allowed quick implementation of this ser- The program has provided patient and family satisfaction,
vice by efficiently navigating barriers to engaging impacted as well nursing, physician, pharmacist, clinical staff, and
staff early on. Throughout this process, the authors set hospital administration pride and gratification. Setting up
realistic step-wise goals. While navigating through the a new program to provide a 4-hour patient encounter to
many details to implementation described, we also kept in infuse therapy to high-risk patients with COVID-19 requires
mind the big picture, which was to provide this potentially commitment and effort. This article describes the experi-
lifesaving therapy to as many qualifying members of our ence, ideas, and formula others may consider using to set
community as possible. This included being flexible with up such a program. Through networking and formal phone
the process and adapting when needed to achieve this calls and meetings about monoclonal antibody therapy,
ultimate goal. A focus on safety remained a priority to min- we have heard about other institutions who have not
imize possible errors and enhance patient and staff satis- been able to institute this program due to various barriers
faction. The optimization of the EHR streamlined workflow, to implementation. We hope our experience serves as a
provided point-of-care resources, and enhanced patient resource for others to provide this therapy to their patients
safety. Additionally, the target date set for implementation and expand access in an effort to mitigate COVID-19 con-
allowed staff and department leads adequate time to plan sequences and cases affecting our communities.
for and anticipate the changes. Serving only 1 patient on
the first day allowed time for staff to experience this new
process hands-on and provided opportunity for focused Corresponding Author: Kathleen Jodoin, PharmD, BCPS, Mount
education. This team communication was essential to Sinai Medical Center, 4300 Alton Rd, Miami Beach, FL 33140;
kathleen.jodoin@msmc.com.
implementing this project, including staff training of pro-
cesses and procedures prior to go-live. Early incorporation Financial Disclosures: None.
80 JCOM March/April 2021 Vol. 28, No. 2 www.mdedge.com/jcomjournalReports From the Field
References 6. Gottlieb RL, Nirula A, Chen P, et al. Effect of bamlanivimab
1. COVID Data Tracker. Center for Disease Control and Prevention. as monotherapy or in combination with etesevimab on viral
https://covid.cdc.gov/covid-data-tracker/#global-counts-rates. load in patients with mild to moderate COVID-19: a random-
Accessed March 12, 2021. ized clinical trial. JAMA. 2021;325(7):632-644. doi:10.1001/
2. Fact Sheet for Health Care Providers Emergency Use Authorization jama.2021.0202
(EUA) of Bamlanivimab. US Food and Drug Administration. Updated 7. Weinreich DM, Sivapalasingam S, Norton T, et al. REGN-COV2,
February 2021. Accessed March 9, 2021. https://www.fda.gov/ a neutralizing antibody cocktail, in outpatients with COVID-19.
media/143603/download N Engl J Med. 2021;384:238-251. doi:10.1056/nejmoa2035002
3. Coronavirus (COVID-19) Update: FDA Authorizes Monoclonal 8. Mulangu S, Dodd LE, Davey RT Jr, et al. A randomized, controlled trial
Antibodies for Treatment of COVID-19 | FDA. https://www.fda. of Ebola virus disease therapeutics. N Engl J Med. 2019;381:2293-
gov/news-events/press-announcements/coronavirus-covid-19-up- 2303. doi:10.1056/NEJMoa1910993
date-fda-authorizes-monoclonal-antibodies-treatment-covid-19. 9. Boyle, P. Can an experimental treatment keep COVID-19 patients out
Accessed February 14, 2021. of hospitals? Association of American Medical Colleges. January 29,
4. Fact Sheet for Health Care Providers Emergency Use Authorization 2021. Accessed March 9, 2021. https://www.aamc.org/news-insights/
(EUA) of Casirivimab and Imdevimab. US Food and Drug can-experimental-treatment-keep-covid-19-patients-out-hospitals
Administration. Updated December 2020. Accessed March 9, 10. Fact Sheet for Health Care Providers Emergency Use
2021. https://www.fda.gov/media/143892/download Authorization (EUA) of Bamlanivimab and Etesevimab. US
5. Chen P, Nirula A, Heller B, et al. SARS-CoV-2 Neutralizing anti- Food and Drug Administration. Updated February 2021.
body LY-CoV555 in outpatients with COVID-19. N Engl J Med. Accessed March 9, 2021. https://www.fda.gov/media/145802/
2021;384(3):229-237. doi:10.1056/NEJMoa2029849 download
www.mdedge.com/jcomjournal Vol. 28, No. 2 March/April 2021 JCOM 81You can also read

















































