Initiation of Allopurinol at First Medical Contact for Acute Attacks of Gout: A Randomized Clinical Trial
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
BRIEF OBSERVATION
Initiation of Allopurinol at First Medical Contact for
Acute Attacks of Gout: A Randomized Clinical Trial
Thomas H. Taylor, MD,a,b,c John N. Mecchella, DO,b,c Robin J. Larson, MD,a,b Kevin D. Kerin, MD,a,b
Todd A. MacKenzie, PhDb
a
White River Junction VA Regional Medical Center, White River Junction, Vt; bDartmouth Medical School, Lebanon, NH; cDartmouth
Hitchcock Medical Center, Lebanon, NH.
ABSTRACT
OBJECTIVE: Streamlining the initiation of allopurinol could result in a cost benefit for a common medical
problem and obviate the perception that no treatment is required once acute attacks have resolved. Our
objective was to test the hypothesis that there is no difference in patient daily pain or subsequent attacks
with early versus delayed initiation of allopurinol for an acute gout attack.
METHODS: A total of 57 men with crystal-proven gout were randomized to allopurinol 300 mg daily or
matching placebo for 10 days. All subjects received indomethacin 50 mg 3 times per day for 10 days, a
prophylactic dose of colchicine 0.6 mg 2 times per day for 90 days, and open-label allopurinol starting at
day 11. Primary outcome measures were pain on visual analogue scale (VAS) for the primary joint on days
1 to 10 and self-reported flares in any joint through day 30.
RESULTS: On the basis of 51 evaluable subjects (allopurinol in 26, placebo in 25), mean daily VAS pain
scores did not differ significantly between study groups at any point between days 1 and 10. Initial VAS
pain scores for allopurinol and placebo arms were 6.72 versus 6.28 (P ⫽ .37), declining to 0.18 versus 0.27
(P ⫽ .54) at day 10, with neither group consistently having more daily pain. Subsequent flares occurred
in 2 subjects taking allopurinol and 3 subjects taking placebo (P ⫽ .60). Although urate levels decreased
rapidly in the allopurinol group (from 7.8 mg/dL at baseline to 5.9 mg/dL at day 3), sedimentation rates
and C-reactive protein levels did not differ between groups at any point.
CONCLUSIONS: Allopurinol initiation during an acute gout attack caused no significant difference in daily
pain, recurrent flares, or inflammatory markers.
Published by Elsevier Inc. • The American Journal of Medicine (2012) 125, 1126-1134
KEYWORDS: Allopurinol; Gout; Gout outcomes
Medical teaching suggests that allopurinol should not be
initiated in the setting of an acute gout attack, because
Funding: none. rapid lowering of serum urate may exacerbate the attack.
Conflict of Interest: None. The views expressed herein do not neces- Delayed initiation may come at a price, as many patients
sarily represent the views of the Department of Veterans Affairs or the US
Government.
never start definitive urate-lowering therapy and are
Authorship: All authors had access to the data and played a role in skeptical of chronic therapy after acute symptoms re-
writing this manuscript. Reproducible Research Statement: Research study solve. Since the introduction of allopurinol in 1964, re-
protocol, STATA statistical code, and data set, without personal identifiers, views have attributed acute attacks of gout or worsening
available from Thomas H. Taylor (e-mail: Tom.Taylor@va.gov). This
of ongoing attacks to the initiation of allopurinol.1 Infer-
study was reviewed by the Veterans Affairs Research and Development
Committee and received approval from the Dartmouth Medical School ence may be implied, because gout attacks continue to
Institutional Review Board. occur during the first few months after allopurinol is
ClinicalTrials.gov registration number: NCT01310673. started2 and are proportional to the rate of uric acid
Requests for reprints should be addressed to Thomas H. Taylor, MD, lowering.3,4 Theories to explain allopurinol-induced ex-
White River Jct VA Regional Medical Center, Department of Medicine,
Dartmouth Medical School, 215 N. Main St, White River Junction, VT
acerbation of gout are controversial and lack evidence,
05009. but they generally implicate urate concentration flux and
E-mail address: Tom.Taylor@va.gov. remodeling of microscopic tophi.3,5
0002-9343/$ -see front matter Published by Elsevier Inc.
http://dx.doi.org/10.1016/j.amjmed.2012.05.025Taylor et al Allopurinol in Acute Gout Attacks 1127
Recommendations have come to include complex The trial was conducted between 1998 and 2009 at the
guidelines for delayed and incremental initiation of de- Veteran’s Affairs Medical Center in White River Junction,
finitive treatment, commencing after the acute attack has Vermont. Patients presenting within 7 days of onset of an
subsided, for both allopurinol and uricosurics.6,7 Despite acute gout attack were evaluated, and American College of
these well-intentioned guidelines, recent studies have im- Rheumatology criteria for acute arthritis of gout were met,19
plicated poor compliance, defi- including the presence of monoso-
cits in patient and physician dium urate crystals on arthrocen-
knowledge, and complexity of tesis of the primary joint on the
CLINICAL SIGNIFICANCE
present regimens requiring pa- day of study entry. Exclusion cri-
tients to return for graded in- ● Guidelines recommend delayed and teria included secondary gout (be-
creases of allopurinol as factors graded initiation of allopurinol. Poor out- cause it is dependent on the treat-
impeding better outcomes.8-13 If comes for gout treatment might be im- ment of the underlying disease);
initiation of allopurinol could be the presence of tophaceous gout
proved if allopurinol could be initiated at
simplified and administered in an (because of concern that tophi
adequate dose of 300 mg at the
the initial presentation of acute attacks. could make evaluation of resolu-
first medical encounter during an ● No difference in pain by daily visual tion and exacerbations difficult); a
acute attack, then opportunity analogue scale was seen when allopuri- history of congestive heart failure;
for education, improved outcomes, nol was administered during the acute anticoagulant use; a recent serum
and cost containment might be attack. creatinine greater than 1.3 mg/dL
realized. (because these patients should not
Evidence in support of delayed ● The percentage of recurrent attacks was receive indomethacin); or the use
and stepped increase of allopuri- similar to that in studies in which fe- of steroids, colchicine, allopuri-
nol treatment is poor and sup- buxostat, allopurinol, or placebo was nol, uricosuric drugs, chemother-
ported by 2 studies describing initiated after the attack. apy, or immunosuppressive ther-
case series.14,15 No study has eval- apy in the past 6 months. Although
uated the initiation of allopurinol all subjects brought to the atten-
during attacks in patients with pri- tion of the principal investigator
mary gout as they present in primary care settings, concom- were screened consecutively, primary providers also made
itantly treated with both indomethacin and colchicine. Pro- decisions regarding eligibility and subjects were highly se-
phylactic colchicine has been shown to reduce the lected by study criteria; thus, information regarding the
16
frequency of gout flares in patients with interval gout and number and characteristics of those excluded could not be
17
in patients beginning treatment with uricosurics and allopuri- reliably tracked.
nol.18 Should allopurinol predispose to exacerbation, it is
equally conceivable that the best time to initiate allopurinol Randomization and Interventions
would be during the acute attack, when patients also receive Fifty-seven eligible subjects were randomized, in a 1:1 ratio
treatment doses of indomethacin and prophylactic doses of without stratification, to receive allopurinol 300 mg daily
colchicine. We challenge current teaching by testing the for 10 days (allopurinol group) or placebo for 10 days
hypothesis that there is no difference in patient-reported (placebo group). Subjects and evaluators had no access to
pain or subsequent attacks with early initiation of allopuri- the randomization sequence. The randomization sequence
nol given during the acute attack, concomitant with indo- was determined by the study pharmacist using a random
methacin treatment and a prophylactic dose of colchicine. number generator and kept in the pharmacy vault. Study
drugs were given directly to study patients through the
pharmacy, and neither patients nor evaluators were aware of
MATERIALS AND METHODS which medication was given. In addition to the 10-day
We designed a randomized, double-blind, placebo-con- course of allopurinol or placebo, all patients received indo-
trolled, parallel-arm, single-center, noninferiority study of methacin 50 mg 3 times per day for 10 days and colchicine
the early initiation of full-dose allopurinol (300 mg) versus 0.6 mg 2 times per day for 90 days. All patients were started
placebo in adults with acute gout, both arms receiving on open-label allopurinol 300 mg daily on day 11 and
indomethacin treatment and a prophylactic dose of colchi- followed for 30 days.
cine. The Research and Development Committee at the
White River Junction Veteran’s Affairs Medical Center and Outcomes and Follow-up
the Committee for the Protection of Human Subjects at Two primary outcomes included pain scores at each of days
Dartmouth College approved the original protocol and re- 1 to 10, as measured by a visual analogue scale (VAS)
viewed the trial annually. All subjects provided written standardized to 10 cm for the primary affected joint, and
informed consent. There was no pharmaceutical industry self-reported subsequent gout flares in any joint during days
participation or support. 1 to 30. For VAS scoring, subjects were given a diary in1128 The American Journal of Medicine, Vol 125, No 11, November 2012
which they indicated their daily pain level on lines anchored Statistical Analysis
by “no pain at all” and “worst pain imaginable.” For sub- All outcome measures were prespecified and prospectively
sequent gout flares, subjects recorded events in their diary collected. The final analysis plan was determined after com-
and were asked at each follow-up visit whether they had any pletion of the trial but before reviewing the data. We com-
new or recurrent gout flares since their last visit. Clinical pared baseline characteristics between study arms using the
confirmation of such events was not required because of t test for continuous variables and the chi-square test for
concern for underreporting. dichotomous variables. Because no “minimally important
Secondary outcomes included erythrocyte sedimentation difference” in VAS pain scores has been established in
rates, and C-reactive protein levels were added when they acute gout,21 we asserted that a 2-cm difference in 10-cm
became available in 2005. Complete blood counts, liver VAS pain scores would be clinically relevant in our study
function tests, and creatinine levels were followed to mon- and assessed whether the 95% confidence intervals (CIs)
itor for toxicity. Serum urate levels were followed to con- around the differences in mean VAS pain scores for days 1
firm compliance and to document the expected early rapid to 10 contained this value. In addition, we assessed for
decline with allopurinol initiation. Follow-up visits for all statistically significant differences in VAS pain scores at
each of days 1 to 10 and performed a longitudinal analysis
outcomes occurred on days 3, 10, and 30 plus or minus 3
in which VAS, measured at days 2 to 10, was compared
days to accommodate weekends or conflicts.
between the 2 study arms while adjusting for VAS on day 1
using a linear mixed-effects model with fixed effects for
Sample Size study arm, day, baseline VAS (day 1), and random intercept
In noninferiority terms, there is 92% power to detect an for each subject. This model was run with and without an
inferiority margin of 2.0 cm assuming an actual inferiority interaction of study arm and day (ie, different slopes for
margin of 0.5 cm, based on a 5% 1-sided type I error rate. both study arms). In addition, we considered a model that
Because there were no studies using the VAS in acute gout, also had a random slope for each patient.
we chose 2.0 cm as a clinically relevant difference. This is
consistent with the reproducibility of the VAS in patients Subgroup and Sensitivity Analysis
with rheumatoid arthritis, 1.5 cm.20 If this were a superiority Because first attacks of gout may respond differently to
trial, 57 subjects provided 90% power to detect a 1.5-cm treatment than subsequent attacks, we performed a post
difference in mean VAS pain scores with a standard devi- hoc subgroup analysis in which we repeated each of the
ation of 1.8 cm using a 2-sided P value of .05. VAS pain score comparisons according to whether the
Figure 1 Flow diagram of enrolled subjects.Taylor et al Allopurinol in Acute Gout Attacks 1129
subjects were having their first gout attack or had had Table 1 Characteristics of Study Participants
previous attacks. Because intention-to-treat analysis can
bias results toward falsely underestimating treatment ef- Allopurinol Placebo
fects, which would favor our hypothesis of no difference
in daily pain or flares, we chose to report our per-protocol Group Group
Characteristic (n ⫽ 26) (n ⫽ 25) P Value
analysis (restricted to randomized subjects who were
adherent to study treatment and completed 10-day and Mean age (SD), y 57 (14) 61 (11) .23
30-day follow-ups) as the primary result. However, to Men, n (%) 26 (100) 25 (100)
also address the possibility that subjects with incomplete History of diabetes, n (%) 4 (15) 5 (20) .67
data or follow-up were not missing at random, we per- Hypertension, n (%) 15 (58) 19 (76) .17
formed 3 sensitivity analyses for our VAS pain score Hyperlipidemia, n (%) 17 (65) 14 (56) .49
Mean BMI (SD), kg/m2 32 (5) 32 (6) .79
outcome—an intention-to-treat analysis based on avail-
Current alcohol use, n (%) 7 (27) 10 (40) .32
able data, an intention-to-treat analysis substituting miss- Use of diuretics, n (%) 5 (19) 7 (28) .46
ing values with the mean VAS score of the subjects in the Mean entry creatinine 1.1 (0.18) 1.1 (0.21) .77
same arm who reported the outcome for that day, and an (SD), mg/dL
intention-to-treat analysis substituting missing values Mean entry urate (SD), 7.8 (1.12) 7.6 (1.72) .76
with the highest VAS score reported by another subject mg/dL
for that day. To evaluate the effect of compliance, we Mean age of first attack 53.9 (16.9) 54.5 (11.5) .87
performed a compliance-adjusted analysis,22 in which we (SD), y*
used the mean serum urate level measured at days 3 and Attack No., n (%) .12†
10 (both post-randomization) as a measure of compli- First attack 9 (35) 4 (16)
ance. We derived a compliance-adjusted treatment effect 2-9 attacks 14 (54) 13 (52)
ⱖ10 attacks 3 (12) 8 (32)
using the study arm as the instrumental variable.23
Study joint, n (%) .41†
Joints of the hand 2 (8) 2 (8)
RESULTS Wrist 1 (4) 2 (8)
Of 57 subjects randomized, 31 were allocated to the allo- Elbow 2 (8) 0 (0)
Knee 5 (19) 5 (20)
purinol group and 26 were allocated to the placebo group.
Ankle 7 (27) 4 (16)
For the per-protocol analysis, 6 subjects were excluded MTP 9 (35) 9 (36)
post-randomization because of failure to adequately comply Multiple joints 0 (0) 3 (12)
with the study medication or follow-up visits (Figure 1).
BMI ⫽ body mass index; MTP ⫽ metatarsophalangeal; SD ⫽ standard
The baseline characteristics of the participants were similar deviation.
between study arms for both the intention-to-treat (Supple- *n ⫽ 25 for allopurinol group and n ⫽ 23 for placebo group.
mental Table 1) and per-protocol populations (Table 1), †Categoric P values are listed for categoric variables by chi-square
neither of whom contained any statistically significant dif- analysis.
ferences. For the per-protocol population, the mean duration
of incident attack before entry was 4.2 days for the allo-
purinol group and 3.9 days for the placebo group. Nine of in the 95% CIs was 1.55 cm seen on day 2. Mean VAS
the patients in the allopurinol group and 4 patients in the pain scores did not statistically significantly differ be-
placebo group presented with their first attack of gout. tween study groups at any point between days 1 and 10,
and longitudinal analysis found that VAS pain across
Compliance days 2 to 10, adjusting for baseline VAS and restricting
During the placebo-controlled portion of the study (days to identical slopes between the allopurinol and placebo
1-10), serum urate levels decreased rapidly in the allopuri- study arms, was not different (⫺0.16 cm; 95% CI, ⫺0.50
nol group, reaching ⱕ 6.5 mg/dL by day 10 for all but 1 of to 0.83; P ⫽ .62).
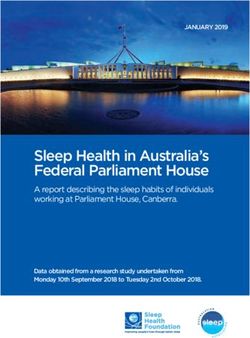
the per-protocol subjects (Figure 2). Conversely, urate lev- All 3 intention-to-treat sensitivity analyses showed sim-
els remained elevated in the placebo group until day 11 ilar findings, with the maximum difference in mean VAS
when a similar rapid decline was observed after initiation of pain scores between the allopurinol and placebo groups
open-label allopurinol in all patients. always occurring on the day of randomization and never
exceeding 0.62 cm (the value from the extreme assumptions
Pain on Daily Visual Analogue Scale analysis). Likewise, the largest value contained in the 95%
On the basis of per-protocol analysis, initial mean VAS CIs was 1.63 cm on day 2 (the value based on extreme
pain scores for the allopurinol and placebo groups were assumptions), and there were no statistically significant dif-
6.72 versus 6.28 (P ⫽ .37) decreasing to 0.18 versus 0.27 ferences at any individual time point or longitudinally.
(P ⫽ .54) at day 10 (Figure 3). The largest difference in Compliance-adjusted analysis showed that subjects receiv-
mean VAS pain scores between groups was 0.44 cm on ing allopurinol had lower VAS pain scores, but the differ-
the day of randomization, and the largest value included ences were not significant (P ⬎ .10). Subgroup analysis1130 The American Journal of Medicine, Vol 125, No 11, November 2012
Figure 2 Mean serum urate over study period. Error bars represent 95% CIs.
according to whether the subject was having a first gout arm. Colchicine reductions due to gastrointestinal symp-
attack versus having had prior attacks revealed similar toms occurred in 8 subjects (31%) in the allopurinol
small, nonsignificant differences (Supplemental Appendix). group and 12 subjects (48%) in the placebo group. There
was 1 unexpected death in an 80-year-old subject in the
Gout Flares allopurinol group who developed gastroenteritis, pneu-
The rate of new or recurrent gout flares between days 1 and monia, fever, dehydration, and acute renal failure. Sup-
30 was 2 of 26 (7.7%) in the allopurinol group and 3 of 25 port was withdrawn in accordance with his advanced
(12.0%) in the placebo group (P ⫽ .61). Stratified by the directives. He had taken 4 doses of study medication and
timing of the events, a single gout flare occurred between is not included in the per-protocol analysis. Another
days 1 and 10 in a subject in the allopurinol group at day 8, patient in the placebo group had a hypersensitivity reac-
whereas 4 gout flares occurred between days 11 and 30, 1 in tion with rash, fever, and mild transaminitis, leading to
a subject in the allopurinol group at day 30 and 3 in subjects discontinuation of allopurinol at day 30. All data for this
in the placebo group at days 16, 20, and 30. All flares were subject were collected and included in both per-protocol
at least 5 days removed from the initiation of allopurinol, and intention-to-treat analyses.
and none involved exacerbation of the index joint. Only 1
flare resulted in the patient seeking care. Subgroup analysis
was not performed because all flares occurred in subjects DISCUSSION
with prior attacks. This first randomized, double-blind, placebo-controlled
study of patients started on an adequate dose (300 mg) of
Secondary End Points allopurinol during the acute gout attack, while simulta-
Mean erythrocyte sedimentation rate and C-reactive protein neously treated with indomethacin and colchicine, pro-
levels declined over the study period in both groups and duced surprisingly similar declines in VAS and self-
were not statistically significantly different at any point determined gout flares, with narrow CIs. Although an
(Figure 4). adequate dose of allopurinol is whatever dose is required
to achieve a serum urate below the goal of 6.0 mg/
Adverse Events dL,24,25 a starting dose of 300 mg of allopurinol avoids
Among per-protocol subjects, elevation of serum creati- the complex stepped increments recommended by guide-
nine ⬎ 1.5 mg/dL occurred in 1 subject from each study lines.6,7 Secondary outcomes, rate of erythrocyte sedi-Taylor et al Allopurinol in Acute Gout Attacks 1131
Figure 3 Mean VAS scores on days 1 to 10 for allopurinol versus placebo. Error bars represent 95% CI. The
longitudinal analysis found that the VAS in the allopurinol arm was lower by 0.16 cm (95% CI, ⫺0.50 to 0.83;
P ⫽ .62) across days 2 to 10, adjusting for baseline VAS and restricting to identical slopes between the 2 study
arms. CI ⫽ confidence interval; VAS ⫽ visual analogue scale.
mentation rate and C-reactive protein decline, did not phate crystals can be mixed with monocytes or macro-
significantly differ between immediate versus delayed phages, in vitro, without induction of cytokines; inflam-
groups. All 26 patients in the immediate allopurinol treat- matory cytokine induction in this model first requires cell
ment group demonstrated a rapid decrease in serum urate priming to activate the inflammasome platform.28 Thus,
level, testament to a high degree of compliance and urate flux, as an instigator of the acute gout attack,
adequate urate flux to test the hypothesis. requires adjunct events,31 possibly modifiable with ad-
Per-protocol analysis was chosen over intention-to- junct therapy.
treat analysis, although we report both. Because a rapid The number of self-reported acute attacks was low and
decrease in serum urate is considered to be an explana- similar in both groups. All attacks were in joints other than
tion for allopurinol-induced precipitation of gout attacks, the primary joint, and only 1 was severe enough to seek
we evaluated patients who actually took allopurinol and treatment. The rate of recurrent gout attack was 10% over 1
returned for 10- and 30-day visits. Flux in serum urate month for the entire group, 8% in the allopurinol group, and
levels, as occurred in recent febuxostat studies, when a 12% in the placebo group. This 1-month attack rate com-
potent inhibitor of xanthine oxidase caused a precipitous pares with that in recent febuxostat studies: Febuxostat
decrease in uric acid, exemplifies the association of rap- Versus Allopurinol Control Trial (FACT) trial,3 Allopurinol
idly lowering urate with more frequent attacks of gout.26 and Placebo-Controlled, Efficacy Study of Febuxostat
Urate flux as a sole explanation seems unlikely, because (APEX) trial,32 Efficacy and Safety of Oral Febuxostat in
many patients with asymptomatic hyperuricemia never Participants With Gout (CONFIRMS) trial,33 and a phase II
develop gout.27 Dialysis rapidly decreases serum urate dose study26 (Table 2). All patients in these comparison
levels but is not associated with attacks of gout. Varying groups also were taking prophylactic colchicine or non-
concentrations of urate crystals can be injected into mu- steroidal anti-inflammatory drugs. Our first month 8% re-
rin knee joints without causing gout.28 Urate crystals are current attack rate after allopurinol administration during
seen in asymptomatic intercritical gout joints and other the acute attack compared favorably to that in the allopuri-
asymptomatic joints.29,30 Urate or calcium pyrophos- nol groups in previous studies3,26,32,33 (11.5%-13%) that did1132 The American Journal of Medicine, Vol 125, No 11, November 2012
Figure 4 Mean erythrocyte sedimentation rates over the study period. Error bars represent 95% CIs.
ESR ⫽ erythrocyte sedimentation rate.
not receive the drug during an acute attack. The recurrence
Table 2 Percentage of Acute Attacks in the First Month of rates in those studies also compared favorably with their
Urate-Lowering Therapy
own placebo groups (10%-11%), which corroborates our
Gout Flairs/ results. Given the low incidence and severity of subsequent
Study Drug and Daily Dose First Month attacks, and results aligned with prior studies, a larger study
FACT trial Febuxostat 80 mg 15% designed to detect smaller statistical differences is not likely
756 patients Febuxostat 120 mg 22% to show clinical significance.
Allopurinol 300 mg 13%
APEX trial† Febuxostat 80 mg 14% Study Limitations
799 patients Febuxostat 120 mg 18% Limitations include a study population recruited from a
Allopurinol 300/100 mg* 11.5%
single Veterans Affairs Medical Center, all male, and
Placebo 10%
possibly not generalizable to a non–Veterans Affairs pop-
CONFIRMS trial Febuxostat 40 mg 12.5%
2268 patients Febuxostat 80 mg 13.5% ulation. Exclusion criteria limiting comorbidities and
Allopurinol 300/200 mg* 11.5% treatment of primary gout on presentation mitigate pos-
Phase II dose study Febuxostat 40 mg 8% sible differences between populations. We studied pa-
153 patients Febuxostat 80 mg 8% tients with relatively newly diagnosed gout, as seen in the
Febuxostat 120 mg 13% primary care setting. All cases of gout were crystal
Placebo 11% proven on the day of entry, some for the first time, but
All patients were taking prophylaxis with colchicine or nonsteroidal this may not be similar to patients with long-standing
anti-inflammatory drug, and none were started on allopurinol during the gout. Although the average number of prior attacks on
acute attack. entry was 3.6, allopurinol was started in some patients on
*Dose adjusted for renal failure. their first attack of gout. This may be controversial, but a
†Reported 8-week incidence divided by 2.
spontaneous attack, without a predisposing conditionTaylor et al Allopurinol in Acute Gout Attacks 1133
(surgery, diuretic initiation, trauma), is cause for defini- 7. Jordan KM, Cameron JS, Snaith M, et al. British society for rheuma-
tive urate-lowering therapy. Treatment of the first spon- tology and British health professionals in rheumatology guideline for
the management of gout. Rheumatology (Oxford). 2007;46:1372-1374.
taneous attack is based on the fact that 60% of individuals 8. Mikuls TR, Farrar JT, Bilker WB, Fernandes S, Saag KG. Suboptimal
with an initial attack experience a second flare within 1 physician adherence to quality indicators for the management of gout
year.34,35 The cost associated with gout flares and uncon- and asymptomatic hyperuricaemia: results from the UK General Prac-
trolled hyperuricemia is double the cost of gout flares tice Research Database (GPRD). Rheumatology (Oxford). 2005;44:
1038-1042.
with treated hyperuricemia ⬍ 6.0 mg/dL.36 Early stream-
9. Barber C, Thompson K, Hanly JG. Impact of a rheumatology consul-
lined treatment with allopurinol might mollify side ef- tation service on the diagnostic accuracy and management of gout in
fects from more extensive use of nonsteroidal anti-in- hospitalized patients. J Rheumatol. 2009;36:1699-1704.
flammatory drugs, therapeutic doses of colchicine, and 10. Cannella AC, Mikuls TR. Understanding treatments for gout. Am J
new expensive treatments with febuxostat, pegloticase, Manag Care. 2005;11(15 Suppl):S451-S458; quiz S465-S468.
11. Taylor WJ, Schumacher HR Jr, Singh JA, Grainger R, Dalbeth N.
anakinra, rilonacept, and canakinumab, meant for ad- Assessment of outcome in clinical trials of gout–a review of current
vanced cases of gout. measures. Rheumatology (Oxford). 2007;46:1751-1756.
New treatment strategies should suggest future re- 12. Singh JA, Hodges JS, Toscano JP, Asch SM. Quality of care for gout
search directions. There is a need to study the initiation in the US needs improvement. Arthritis Rheum. 2007;57:822-829.
of allopurinol in chronic tophaceous gout and secondary 13. Sarawate CA, Brewer KK, Yang W, et al. Gout medication treatment
patterns and adherence to standards of care from a managed care
gout. Patients unable to take indomethacin because of perspective. Mayo Clin Proc. 2006;81:925-934.
renal failure, heart failure, or anticoagulation are often 14. Yue TF, Gutman AB. Effect of allopurinol (4-hydroxypyrazolo-(3,4-
treated with alternative strategies: oral colchicine, pred- D)pyrimidine) on serum and urinary uric acid in primary and second-
nisone, intra-articular steroid, and interleukin-1 antago- ary gout. Am J Med. 1964;37:885-898.
15. Excess of amphicillin rashes associated with allopurinol or hyperuri-
nist anakinra. Simplified allopurinol administration in a
cemia. A report from the Boston collaborative drug surveillance pro-
more complex population with gout might better address gram, Boston University Medical Center. N Engl J Med. 1972;286:
issues of compliance and cost-effectiveness. There are 505-507.
epidemiologic suggestions that hyperuricemia is a medi- 16. Yu T. The efficacy of colchicine prophylaxis in articular gout–a
ator of a variety of cardiovascular conditions.37 Early reappraisal after 20 years. Semin Arthritis Rheum. 1982;12:256-264.
17. Hollingworth P, Reardon JA, Scott JT. Acute gout during hypouricae-
initiation of allopurinol, for the first gout attack, might mic therapy: prophylaxis with colchicine. Ann Rheum Dis. 1980;39:
improve cardiovascular outcomes. 529.
18. Borstad GC, Bryant LR, Abel MP, Scroggie DA, Harris MD, Alloway
JA. Colchicine for prophylaxis of acute flares when initiating allopuri-
CONCLUSIONS nol for chronic gouty arthritis. J Rheumatol. 2004;31:2429-2432.
In uncomplicated gout, all 3 drugs, nonsteroidal anti-inflam- 19. Wallace SL, Robinson H, Masi AT, Decker JL, McCarty DJ, Yu TF.
matory drug of choice, a prophylactic dose of colchicine 0.6 Preliminary criteria for the classification of the acute arthritis of pri-
mary gout. Arthritis Rheum. 1977;20:895-900.
mg once daily, and adequately dosed allopurinol 300 mg 20. Massy-Westropp N, Ahern M, Krishnan J. A visual analogue scale for
once daily, may be started during the acute attack. Graded assessment of the impact of rheumatoid arthritis in the hand: validity
incremental dosing of allopurinol was not used because we and repeatability. J Hand Ther. 2005;18:30-33.
21. Grainger R, Taylor WJ, Dalbeth N, et al. Progress in measurement
wanted to show that the initiation of treatment can be done
instruments for acute and chronic gout studies. J Rheumatol. 2009;36:
to advantage with an adequate 300 mg dose, saving unnec- 2346-2355.
essary visits, expense, chronic underdosing, and complexity 22. Little RJ, Long Q, Lin X. A comparison of methods for estimating the
of therapy. causal effect of a treatment in randomized clinical trials subject to
noncompliance. Biometrics. 2009;65:640-649.
23. Fischer K, Goetghebeur E, Vrijens B, White IR. A structural mean
References model to allow for noncompliance in a randomized trial comparing 2
1. Neogi T. Clinical practice. Gout. N Engl J Med. 2011;364:443-452. active treatments. Biostatistics. 2011;12:247-257.
2. Grahame R, Scott JT. Clinical survey of 354 patients with gout. Ann 24. Perez-Ruiz F. Treating to target: a strategy to cure gout. Rheumatology
Rheum Dis. 1970;29:461-468. (Oxford). 2009;48(Suppl 2):ii9-ii14.
3. Becker MA, Schumacher HR Jr, Wortmann RL, et al. Febuxostat 25. Stamp LK, O’Donnell JL, Zhang M, et al. Using allopurinol above the
compared with allopurinol in patients with hyperuricemia and gout: dose based on creatinine clearance is effective and safe in patients with
FACT trial. N Engl J Med. 2005;353:2450-2461. chronic gout, including those with renal impairment. Arthritis Rheum.
4. Sundy JS, Becker MA, Baraf HS, et al. Reduction of plasma urate 2011;63:412-421.
levels following treatment with multiple doses of pegloticase (poly- 26. Becker MA, Schumacher HR Jr, Wortmann RL, et al. Febuxostat, a
ethylene glycol-conjugated uricase) in patients with treatment-failure novel nonpurine selective inhibitor of xanthine oxidase: a twenty-
gout: results of a phase II randomized study. Arthritis Rheum. 2008; eight-day, multicenter, phase II, randomized, double-blind, placebo-
58:2882-2891. controlled, dose-response clinical trial examining safety and efficacy
5. Terkeltaub RA. Clinical practice. Gout. N Engl J Med. 2003;349:1647- in patients with gout. Arthritis Rheum. 2005;52:916-923.
1655. 27. Chen LX, Schumacher HR. Gout: can we create an evidence-based
6. Zhang W, Doherty M, Bardin T, et al. EULAR evidence based rec- systematic approach to diagnosis and management? Best Pract Res
ommendations for gout. part II: Management. report of a task force of Clin Rheumatol. 2006;20:673-684.
the EULAR standing committee for international clinical studies in- 28. Joosten LA, Netea MG, Mylona E, et al. Engagement of fatty acids
cluding therapeutics (ESCISIT). Ann Rheum Dis. 2006;65:1312-1324. with toll-like receptor 2 drives interleukin-1beta production via the1134 The American Journal of Medicine, Vol 125, No 11, November 2012
ASC/caspase 1 pathway in monosodium urate monohydrate 33. Becker MA, Schumacher HR, Espinoza LR, et al. The urate-low-
crystal-induced gouty arthritis. Arthritis Rheum. 2010;62:3237-3248. ering efficacy and safety of febuxostat in the treatment of the
29. Pascual E, Batlle-Gualda E, Martinez A, Rosas J, Vela P. Synovial hyperuricemia of gout: the CONFIRMS trial. Arthritis Res Ther.
fluid analysis for diagnosis of intercritical gout. Ann Intern Med. 2010;12:R63.
1999;131:756-759. 34. Brixner DI, Ho MJ. Clinical, humanistic, and economic outcomes of gout.
30. Abeles M. Monosodium urate crystals in asymptomatic joints. Arthri- Am J Manag Care. 2005;11(15 Suppl):S459-S464; quiz S465-468
tis Rheum. 1980;23:124. 35. Neogi T, Hunter DJ, Chaisson CE, Allensworth-Davies D, Zhang Y.
31. Dinarello CA. How interleukin-1beta induces gouty arthritis. Arthritis Frequency and predictors of inappropriate management of recurrent
Rheum. 2010;62:3140-3144. gout attacks in a longitudinal study. J Rheumatol. 2006;33:104-109.
32. Schumacher HR Jr, Becker MA, Wortmann RL, et al. Effects of 36. Halpern R, Fuldeore MJ, Mody RR, Patel PA, Mikuls TR. The effect
febuxostat versus allopurinol and placebo in reducing serum urate in of serum urate on gout flares and their associated costs: an adminis-
subjects with hyperuricemia and gout: a 28-week, phase III, random- trative claims analysis. J Clin Rheumatol. 2009;15:3-7.
ized, double-blind, parallel-group trial: APEX trial. Arthritis Rheum. 37. Feig DI, Kang DH, Johnson RJ. Uric acid and cardiovascular risk.
2008;59:1540-1548. N Engl J Med. 2008;359:1811-1821.Taylor et al Allopurinol in Acute Gout Attacks 1134.e1
Supplemental Table 1 Characteristics of Study Participants
Randomized
Allopurinol Placebo
Group Group
Characteristic (n ⫽ 31) (n ⫽ 26) P Value
Mean age (SD), y 58 (13) 62 (12) .23
Men, n (%) 31 (100) 26 (100)
History of diabetes, n (%) 4 (13) 5 (19) .51
Hypertension, n (%) 17 (55) 20 (77) .08
Hyperlipidemia, n (%) 19 (61) 14 (54) .57
Mean BMI (SD), kg/m2 31 (5) 32 (6) .7
Current alcohol use, n (%) 9 (29) 11 (42) .3
Use of diuretics, n (%) 6 (19) 7 (27) .78
Mean entry creatinine (SD), 1.09 (0.18) 1.13 (0.21) .44
mg/dL
Mean entry urate (SD), mg/dL 7.5 (1.33) 7.7 (1.72) .65
Mean age of first attack 54.5 (15.8) 55.6 (12.4) .8
(SD), y*
Attack No., n (%) .15†
First attack 10 (32) 4 (16)
2-9 attacks 17 (55) 13 (52)
ⱖ10 attacks 4 (13) 8 (32)
Study joint, n (%) .33†
Joints of the hand 5 (16) 3 (12)
Wrist 1 (3) 2 (8)
Elbow 2 (6) 0 (0)
Knee 5 (16) 5 (19)
Ankle 8 (26) 4 (15)
MTP 10 (32) 9 (35)
Multiple joints 0 (0) 3 (12)
BMI ⫽ body mass index; MTP ⫽ metatarsophalangeal; SD ⫽ standard
deviation.
*n ⫽ 29 for allopurinol group and n ⫽ 24 for placebo group.
†Categoric P values are listed for categoric variables by chi-square
analysis.1134.e2 The American Journal of Medicine, Vol 125, No 11, November 2012
Supplemental Figure 1 Mean serum urate over study period including all patients randomized (intention to treat
analysis). Error bars represent 95% CIs.Taylor et al Allopurinol in Acute Gout Attacks 1134.e3
Supplemental Figure 2 Mean serum Erythrocyte Sedimentation Rates (ESR) over the study period including all
patients randomized (intention to treat analysis). Error bars represent 95% CIs.1134.e4 The American Journal of Medicine, Vol 125, No 11, November 2012
Supplemental Figure 3 Mean serum C-reactive Protein (CRP) over study period including all patients randomized
(intention to treat analysis). Error bars represent 95% CIs.Taylor et al Allopurinol in Acute Gout Attacks 1134.e5
Supplemental Figure 4 Mean serum creatinine over study period including all patients randomized (intention to
treat analysis). Error bars represent 95% CIs.1134.e6 The American Journal of Medicine, Vol 125, No 11, November 2012
Supplemental Figure 5 Mean VAS Scores on Days 1-10 Allopurinol vs. Placebo for all patients randomized
(intention to treat analysis).
Supplemental Figure 6 Sensitivity analysis displaying extreme versus average assumptions for Visual Analog Pain
Scale (VAS) scores on Days 1-10 Allopurinol vs. Placebo for all patients randomized (intention to treat analysis).Taylor et al Allopurinol in Acute Gout Attacks 1134.e7
Supplemental Figure 7 Visual Analog Pain Scale (VAS) scores on Days 1-10 Allopurinol vs. Placebo for all
patients with their first attack.
Supplemental Figure 8 Visual Analog Pain Scale (VAS) scores on Days 1-10 Allopurinol vs. Placebo for all
patients whom have had multiple attacks.You can also read