Crack Cocaine and HIV: What Clinicians Need to Know - Trainer Guide
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Crack Cocaine and HIV:
What Clinicians Need to Know
Trainer Guide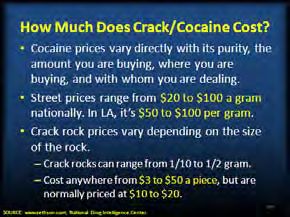
Crack Cocaine and HIV:
What Clinicians Need to Know
Table of Contents
Background Information ..................................................................................................................... 3
What Does the Training Package Contain? ....................................................................................... 4
What Does This Trainer’s Manual Contain? ...................................................................................... 4
How is This Trainer’s Guide Organized? ........................................................................................... 4
General Information about Conducting the Training........................................................................ 4
Materials Needed to Conduct the Training ........................................................................................ 5
Overall Trainer Notes ........................................................................................................................... 5
Slide-By-Slide Trainer Notes ............................................................................................................... 6
Title Slide and Training Collaborators (Slides 1-2) .................................................................. 6-7
Pre-Test Questions and Educational Objectives (Slides 3-11) ..............................................7-9
Introduction to Psychoactive Drugs (Slides 12-15) .............................................................10-12
What is a Substance Use Disorder? (Slides 16-22) ............................................................13-15
Crack/Cocaine (Slides 23-36) .............................................................................................15-25
How Does Crack/Cocaine Differ from Methamphetamine? (Slides 37-42) .........................25-28
The Epidemiology of Crack/Cocaine (Slides 43-60)............................................................28-36
“Linked Epidemics”: Substance Use Disorders and HIV/AIDS (Slides 61-64) ....................36-39
The Intersection of Crack/Cocaine and HIV/AIDS (Slides 65-77) .......................................39-43
Effective Treatment Interventions for Crack/Cocaine Use (Slides 78-91) ...........................44-54
Post-Test Questions, Take Home Points, and Key Resources (Slides 92-101) .................54-56
-2-
Crack Cocaine and HIV:
What Clinicians Need to Know
Background Information
The purpose of The Crack Cocaine Training Package is to provide HIV clinicians
(including, but not limited to physicians, dentists, nurses, and other allied medical staff,
therapists and social workers, and counselors, specialists, and case mangers) with a
detailed overview of crack cocaine and HIV. The package was developed for the Pacific
AIDS Education and Training Center, based at Charles R. Drew University of Medicine
and Science. Principle authorship was by Beth Rutkowski, M.P.H., Associate Director
of Training of UCLA ISAP, and Thomas Freese, Ph.D., Director of Training of UCLA
ISAP and Principal Investigator/Director of the Pacific Southwest ATTC. We wish to
acknowledge Phil Meyer, LCSW, Elissa Bradley, MPH, and Tom Donohoe, MBA from
the PAETC.
The introductory training includes a 101-slide PowerPoint presentation, this Trainer’s
Guide, and a companion 2-page fact sheet. The duration of the training is
approximately 90-120 minutes, depending on whether the trainer chooses to present all
of the slides, or a selection of slides.
Slides 12-22 have been included for audiences who have little or no familiarity with
psychoactive drugs and substance use disorder-related terminology. If you are
presenting to an audience that is knowledgeable about SUD, you may decide to hide
these slides when presenting the information.
Pre- and post-test questions have been inserted at the beginning and end of the
presentation to assess a change in the audience’s level knowledge after the information
has been presented. An answer key is provided in the Trainer’s notes in slides 4-8 and
slides 93-97.
Audience Response System (ARS) can be utilized, if available, when facilitating the pre-
and post-test question sessions, as well as the questions contained on slides 49, 56,
and 66.
In addition, a series of case studies have been inserted throughout the presentation to
encourage dialogue among the training participants, and to illustrate how the
information contained within the presentation can be used clinically.
-3-
What Does the Training Package Contain?
PowerPoint Training Slides (with notes)
Trainer’s Guide with detailed instructions for how to convey the information and
conduct the interactive exercises
Two-page fact sheet entitled, “Tips for HIV Clinicians Working with Crack Cocaine
Users”
What Does This Trainer’s Manual Contain?
Slide-by-slide notes designed to help the trainer effectively convey the content of the
slides themselves
Supplemental information for select material to enhance the quality of instruction
Suggestions for facilitating the pre- and post-test questions and case studies
How is This Trainer’s Guide Organized?
For this manual, text that is shown in bold italics is a “Note to the Trainer.” Text that is
shown in normal font relates to the “Trainer’s Script” for the slide.
It is important to note that some slides in the PowerPoint presentation contain
animation. Animations are used to call attention to particular aspects of the information
or to present the information in a stepwise fashion to facilitate both the presentation of
information and participant understanding. Getting acquainted with the slides, and
practicing delivering the content of the presentation are essential steps for ensuring a
successful, live training experience. In addition, slide 28 contains a video. Please refer
to the instructions that accompany slide 28 for additional information regarding this
video.
General Information about Conducting the Training
The training is designed to be conducted in small- to medium-sized groups (10-25
people). It is possible to use these materials with larger groups, but the trainer may
have to adapt the small group exercises (case studies) to ensure that there is adequate
time to cover all of the material.
-4-
Materials Needed to Conduct the Training
Computer with PowerPoint software installed (2003 or higher version) and LCD
projector to project the PowerPoint training slides.
Flip chart paper and easel/white board, and markers/pens to write down relevant
information, including key case study discussion points.
Overall Trainer Notes
It is critical that prior to conducting the actual training, the trainer practice using this
guide while showing the slide presentation in Slideshow Mode in order to be prepared to
use the slides in the most effective manner.
-5-
Crack Cocaine and HIV:
What Clinicians Need to Know
Slide-By-Slide Trainer Notes
The notes below contain information that can be presented with each slide. This
information is designed as a guidepost and can be adapted to meet the needs of the
local training situation. Information can be added or deleted at the discretion of the
trainer(s).
Slide 1: Title Slide
The purpose of this introductory training is to provide HIV clinicians
(including, but not limited to physicians, dentists, nurses, and other
allied medical staff, therapists and social workers, and counselors,
specialists, and case managers) with an overview of crack cocaine and
HIV. The duration of the training is approximately 90-120 minutes,
depending on whether the trainer chooses to present all of the slides,
or a selection of slides.
Slides 12-22 have been included for audiences who have little or no
familiarity with psychoactive drugs and substance use disorder-related
terminology. If you are presenting to an audience that is
knowledgeable about SUD, you may decide to hide these slides when
presenting the information.
Pre- and post-test questions have been inserted at the beginning and
end of the presentation to assess a change in the audience’s level of
knowledge following presentation of the training content. An answer
key is provided in the Trainer’s notes for slides 4-8 and slides 93-97.
Audience Response System can be utilized, if available, when
facilitating the pre- and post-test question sessions, as well as the
questions contained on slides 49, 56, and 66.
In addition, a series of case studies have been inserted throughout the
presentation to encourage dialogue among the training participants,
and to illustrate how the information contained within the presentation
can be used clinically.
-6-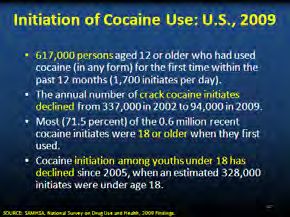
Slide 2: Training Collaborators
This PowerPoint presentation, Trainer’s Guide, and companion fact sheet
were developed by Beth Rutkowski, M.P.H. (Associate Director of Training of
UCLA ISAP) and Thomas Freese, Ph.D. (Director of Training of UCLA ISAP
and Principal Investigator/Director of the Pacific Southwest ATTC) through
supplemental funding provided by the Pacific AIDS Education and Training
Center, based at Charles R. Drew University of Medicine and Science. We
wish to acknowledge Phil Meyer, LCSW, Elissa Bradley, MPH, and Tom
Donohoe, MBA, from the PAETC.
Slide 3: [Transition Slide] Pre-Test Questions
The purpose of the following five pre-test questions is to test the
current level of crack cocaine and HIV knowledge among training
participants. The five questions are formatted as either multiple choice
or true/false questions.
INSTRUCTIONS
Read each question and the possible responses aloud, and give
training participants adequate time to jot down their response before
moving on to the next question.
Do not reveal the answers to the questions until the end of the training
session (when you administer the post-test).
Slide 4: Pre-Test Question #1
Answer Key:
Correct response: B (False)
**Audience Response System (ARS)-compatible slide
Slide 5: Pre-Test Question #2
Answer Key:
Correct response: B (Blocking dopamine transporters)
**Audience Response System (ARS)-compatible slide
-7-
Slide 6: Pre-Test Question #3
Answer Key:
Correct response: A (True)
**Audience Response System (ARS)-compatible slide
Slide 7: Pre-Test Question #4
Answer Key:
Correct response: C (Dysphoric mood)
**Audience Response System (ARS)-compatible slide
Slide 8: Pre-Test Question #5
Answer Key:
Correct response: A (True)
**Audience Response System (ARS)-compatible slide
Slide 9: Introductions
INSTRUCTIONS
In an effort to break the ice and encourage group interaction, take a few
minutes to ask training participants to briefly share the answers to
these four questions. You can ask for several volunteers to share their
responses, if the size of your audience prevents all participants from
sharing.
-8-
Slide 10: Educational Objectives
INSTRUCTIONS
Briefly review each of the educational objectives with the audience.
Slide 11: Educational Objectives, continued
INSTRUCTIONS
Continue by briefly reviewing the remaining two educational objectives
with the audience.
-9-
Slide 12: [Transition Slide] Introduction to Psychoactive Drugs
The first topic of the presentation is a brief introduction to psychoactive drugs
and key terminology. Several of the slides in this section have been adapted
from the “Drugs 101” presentation developed for the United Nations Office of
Drugs and Crime’s Treatnet international training program.
More Information on Treatnet
Treatnet is a network of drug dependence treatment and rehabilitation
centres covering all regions of the world. An initiative of United Nations
Office on Drugs and Crime (UNODC), Treatnet aims to provide
diversified, effective and quality drug dependence treatment and
rehabilitation services, including HIV/AIDS prevention and care. Its
main strategy is to promote dialogue and the sharing of experience
amongst its members and with its partners.
Twenty selected resource centres, together with a capacity-building
consortium and UNODC constitute Treatnet, also known as the
"International network of drug dependence treatment and rehabilitation
resource centres". Participating centres are located in Australia, Brazil,
Canada, China, Colombia, Egypt, Germany, India Indonesia, Iran,
Kazakhstan, Kenya, Mexico, Nigeria, Russia, Spain, Sweden, United
Kingdom and United States. Treatnet collaborates with a variety of
partners including other drug dependence treatment centres
(Associated Treatment Providers) and international organizations.
During its first two years, the network focused on two main goals:
identifying and sharing good practices for drug dependence treatment
and rehabilitation, and improving the capacity to deliver quality
services.
- 10 -Slide 13: What are Psychoactive Drugs?
INSTRUCTIONS
Explain that psychoactive drugs achieve their effects by interacting
with the central nervous system (CNS).
Provide some examples from the following:
• Examples of affected mental processes and behavior:
memory, attention, the way people talk, increased
impulsiveness or aggressiveness.
• Examples of altered perceptions of reality. For instance,
psychoactive drugs change alertness, response time, and
perception of the world. For example, they can slow down
reaction time while driving. Some can cause
visual/auditory hallucinations.
Additional Information for the Trainer
When absorbed into the body, drugs interact with and modify cells,
organs, and bodily systems by:
• Altering the way the body normally functions (increasing,
slowing, or enhancing bodily processes, or level or
quality of functioning)
• Altering the operation of tissues, organs, and systems
• Affecting hormones and enzymes
• Impacting processes such as digestion, respiration,
circulation, and mental functioning
Slide 14: Why Do People Initiate Drug Use?
1. While there are many reasons for the initiation into and continued use of
both licit and illicit drugs, key motivators pivot around the main factors
included in the slide.
2. These motivators are not mutually exclusive. They may co-occur for
many people. A person may take drugs for any or all of the reasons
shown.
3. A person may not be aware that these are the underpinning drivers of
drug use. For example, a young woman who finally gets into treatment,
after being referred by her general practitioner, may realize during
treatment that traumatic events that happened to her in childhood
(childhood sexual abuse is very common among women in AOD
treatment) are integrally linked to her problematic drug use.
- 11 -Slide 15: [No Title]
1. Drug addiction is considered a brain disease because drugs change the
structure of the brain and how it works.
2. As a result of scientific research, we also know that addiction is a disease
that affects behavior.
3. These brain changes can be long lasting, and can lead to the harmful
behaviors seen in people who abuse drugs.
4. We have identified many of the biological and environmental factors and
are beginning to search for the genetic variations that contribute to the
development and progression of the disease.
5. Scientists use this knowledge to develop effective prevention and
treatment approaches that reduce the toll drug abuse takes on
individuals, families, and communities.
6. Despite these advances, many people today do not understand why
individuals become addicted to drugs or how drugs change the brain to
foster compulsive drug abuse.
Additional Information for the Trainer
At first, people may perceive what seem to be positive effects with drug
use. They also may believe that they can control their use; however,
drugs can quickly take over their lives. Over time, if drug use
continues, pleasurable activities become less pleasurable, and drug
abuse becomes necessary for abusers to simply feel "normal." Drug
abusers reach a point where they seek and take drugs, despite the
tremendous problems caused for themselves and their loved ones.
Some individuals may start to feel the need to take higher or more
frequent doses, even in the early stages of their drug use.
The initial decision to take drugs is mostly voluntary. However, when
drug abuse takes over, a person's ability to exert self control can
become seriously impaired. Brain imaging studies from drug-addicted
individuals show physical changes in areas of the brain that are critical
to judgment, decision making, learning and memory, and behavior
control. Scientists believe that these changes alter the way the brain
works, and may help explain the compulsive and destructive behaviors
of addiction.
- 12 -Slide 16: Substance Use Disorder (SUD)
1. This slide provides several examples of terms that are used to describe
the act of ingesting alcohol and other drugs, and terms to describe the
individual who is ingesting these substances.
2. There is a movement within the alcohol and other drug treatment field to
use the term “substance use disorder,” as opposed to substance misuse
or addiction.
Slide 17: [Transition Slide] What is a Substance Use Disorder?
The next topic of the presentation is a definition and key characteristics of a
substance use disorder.
Slide 18: What is a Substance Use Disorder?
1. The term “drug addiction” has been replaced with “substance use
disorder” in the definition provided.
2. A substance use disorder is a state in which an individual engages in a
compulsive behavior, even when faced with negative consequences.
This behavior is reinforcing, or rewarding. A major feature of a
substance use disorder is the loss of control in limiting intake of the
addictive substance.
3. The most recent research indicates that the reward pathway may be
even more important in the craving associated with addiction, compared
to the reward itself. Scientists have learned a great deal about the
biochemical, cellular and molecular bases of addiction; it is clear that
substance use disorders are a disease of the brain.
Slide 19: Some Additional Important Terminology
1. This slide reviews three important concepts related to substance use
disorders.
2. Each concept will be reviewed in more detail in the subsequent slides.
- 13 -Slide 20: Psychological Craving
INSTRUCTIONS
Review the definition of psychological craving.
Provide some examples. For instance, a woman who quit smoking
years ago, but who still feels cravings when exposed to certain
situations (friends who smoke, parties, coffee time).
Slide 21: Tolerance
INSTRUCTIONS
Review the definition of tolerance.
Provide some examples. For instance, a man who has been drinking
heavily for a while who is able to drink more than other people and not
feel the effects of alcohol because he has developed a tolerance for the
drug.
Ask your audience to provide some examples, as well.
Additional Information for the Trainer
“The most common change produced by prior experience with a drug
is a decrease in responsiveness to its effects. When an organism
becomes less sensitive to the actions of a drug by virtue of past
experience with the drug, we refer to this change as acquired
tolerance.”
- 14 -Slide 22: Withdrawal
INSTRUCTIONS
Review the list of possible withdrawal symptoms.
Ask participants to provide examples of withdrawal symptoms from
their experience with clients.
1. You can think of the effects of withdrawal as the opposite of those seen
with intoxication.
Additional Information for the Trainer
“The essential feature of Substance Withdrawal is the development of a
substance-specific maladaptive behavioural change, with physiological
and cognitive concomitants, that is due to the cessation, or reduction
in, heavy and prolonged substance use (Criterion A). The substance-
specific syndrome causes clinically significant distress or impairment
in social, occupational, or other important areas of functioning
(Criterion B). The symptoms are not due to a general medical condition
and are not better accounted for by another mental disorder (Criterion
C)” (APA, 1995, p. 184-185).
Slide 23: [Transition Slide] Crack/Cocaine
The next section of the presentation describes, in detail, crack cocaine.
Cocaine is plant-derived, and falls within the broader classification of a
stimulant, which also includes synthetic drugs (amphetamine-type
stimulants).
Crack cocaine is highly addictive and powerful and is derived from powdered
cocaine using a simple conversion process. Crack emerged as a drug of
abuse in the mid-1980s. It is abused because it produces an immediate high
and because it is easy and inexpensive to produce--rendering it readily
available and affordable. Cocaine interferes with the re-absorption process of
dopamine, a chemical messenger associated with pleasure and movement.
The build-up of dopamine causes continuous stimulation of receiving
neurons, which is associated with the euphoria commonly reported by
cocaine users. Stimulants can be ingested in a variety of ways, and the
duration and intensity of the effect differ by the route of administration.
Crack cocaine is a Schedule II substance under the Controlled Substances
Act. Schedule II drugs, which also include PCP and methamphetamine, have
a high potential for abuse. Abuse of these drugs may lead to severe
psychological or physical dependence (NDIC, Crack Cocaine Fast Facts).
- 15 -Slide 24: The Broader Classification: Stimulants
1. The main types of stimulants are methamphetamine, amphetamines (not
pictured), crack cocaine, and powder cocaine.
2. Stimulants increase alertness and arousal by stimulating the central
nervous system.
Slide 25: Forms of Cocaine
1. The powdered hydrochloride salt form of cocaine can be snorted or
dissolved in water and injected. Powder cocaine is most often snorted.
2. Crack is the form of cocaine that has not been neutralized by an acid to
make the hydrochloride salt. This form of cocaine comes in a rock crystal
that can be heated and its vapors smoked.
3. Crack may be smoked in a pipe bowl containing 50-100 mg or in a
cigarette with as much as 300 mg. The cocaine high is most intense if
you smoke or inject cocaine.
4. Smoking crack bypasses the vasoconstriction that results when cocaine
is snorted; therefore, the effects are similar to taking cocaine
intravenously.
Additional Information for the Trainer regarding Cocaine Half-Life
The half-life of cocaine depends on the route of administration. The
following table summarizes the duration of effects and half-life, by
route of administration.
Peak Effect Duration Half-Life
Route Onset
(min) (min) (min)
40-60
7 seconds 1-5 minutes 20 minutes
Smoking minutes
20-30 40-60
15 seconds 3-5 minutes
Injection minutes minutes
45-90 60-90
3 minutes 15 minutes
Nasal minutes minutes
60-90
10 minutes 60 minutes 60 minutes
Oral minutes
- 16 -Slide 26: Forms of Cocaine
1. The term "crack" refers to the crackling sound heard when the mixture is
smoked (heated).
2. The photos included on this slide illustrate different forms of cocaine.
3. Common street names can differ by region. Ask the audience to offer
additional street names.
Additional Information for the Trainer
There are many other street names for crack, and the popularity of
these names varies by geographic region of the U.S. Additional street
names include: 24-7; Badrock; Beat; Candy; Chemical; Cloud; Cookies;
Crumbs; Crunch & munch; Devil drug; Dice; Electric kool-aid; Fat bags;
French fries; Glo; Gravel; Grit; Hail; Hard ball; Hard rock; Hotcakes; Ice
cube; Jelly beans; Nuggets; Paste; Piece; Prime time; Product; Raw;
Rock(s); Scrabble; Sleet; Snow coke; Tornado; and Troop.
- 17 -Slide 27: Crack in More Detail
1. Crack can be administered in many ways, but is most often smoked.
2. Crack is widely available in various geographic regions.
3. The crack high is quick, intense, and short term, and requires the use of
more crack almost immediately to maintain the high.
Additional Information for the Trainer
The intensity and duration of cocaine’s effects—which include
increased energy, reduced fatigue, and mental alertness—depend on
the route of drug administration. The faster cocaine is absorbed into
the bloodstream and delivered to the brain, the more intense the high.
TAKING COCAINE BY MOUTH
This is the safest way to do coke, but by far the least efficient. Users
can absorb cocaine through the mucous membrane of the inner cheeks
and gums. It can also be swallowed but the drug loses much of its
effectiveness in the stomach. While the rate of absorption is slow, the
effects last longer.
SNORTING COCAINE
Snorting, or sniffing through the nose, is the next safest method. The
effects peak sooner and don’t last as long this way. It can lead to a
burning sensation in the nostrils after cocaine’s anaesthetic effects
wear off. Cocaine highly constricts blood vessels and prolonged use
can lead to nasal tissue being destroyed.
Cocaine powder must be divided into very fine particles. Snorters
should be careful to use a clean instrument to snort with, such as a
straw or hollowed out pen. Don’t share this with others as blood-borne
viruses and infections can result as the nasal linings are quite fragile.
Don’t use paper money, it will have all sorts of bacteria on it (and
possibly viruses) and can lead to infections.
SMOKING COCAINE
Freebase or crack cocaine is most often accomplished using a glass
pipe or a small length of a radio antenna or similar metal tube. Like
injecting, smoking leads to intense short-lived effects but it does
bypass some of the risks posed by injecting, like infections from
bacteria or viruses. The danger of overdose is lowered to some extent,
but still risky.
- 18 -[Notes continue for Slide Slide 27: Crack in More Detail
27]
INJECTING COCAINE
Injecting cocaine provides the highest blood levels of drug in the
shortest amount of time. Upon injection, cocaine reaches the brain in a
matter of seconds, and the exhilarating rush that follows can be so
intense that it induces some users to vomit uncontrollably. The
euphoria passes quickly. Make sure you use a 0.2 wheel filter to get rid
of bacteria and fillers.
One effect of cocaine is a restricting of your veins. They get harder to
find, so rotate your sites and take care if you are on a binge. An
injected mixture of cocaine and heroin is a dangerous combination, as
the converse effects of the drugs actually complement each other, but
may also mask the symptoms of an overdose.
Slide 28: Let’s Take a Look at Normal Dopamine Functioning
INSTRUCTIONS
In order to understand the impact of crack/cocaine on the brain, you
first need to understand the way that the brain works normally (in the
absence of these substances). It is then possible to see how
stimulants like crack change this functioning. A movie will play here
depicting the normal dopamine transmission process.
[This slide contains a movie clip that will play when the trainer clicks
on the happy face. In order for this to work, the connection between
the PowerPoint presentation and the video file must be maintained.
When moving the PowerPoint file to another location on your computer
or to another computer, make sure to always move the video file along
with it. If the link becomes broken, the video will need to be reinserted.
Delete the black box that appears behind the happy face. From the
insert menu in PowerPoint, select “movie.” Select the video file that
was included for this training. When asked, indicate that the movie
should play automatically. It will appear as a black box on the screen.
Move the black box behind the happy face and it should play when the
slide show is being viewed when the trainer clicks on the happy face].
- 19 -Slide 29: When You Add Crack to the Mix…
1. This is a cartoon depiction of what happens when crack or powder
cocaine is ingested. The next slide explains the effect of cocaine on the
brain in more detail.
Slide 30: How Does Crack/Cocaine Work in the Brain?
1. The most extensively studied effect of cocaine on the central nervous
system is the blockage of the dopamine transporter protein. In the normal
communication process, dopamine is released by a neuron into the
synapse, where it can bind to dopamine receptors on neighboring
neurons.
2. Normally, dopamine is then recycled back into the transmitting neuron by
a specialized protein called the dopamine transporter.
3. Cocaine acts by preventing the dopamine from being recycled, causing
excessive amounts of the neurotransmitter to build up, amplifying the
message to and response of the receiving neuron, and ultimately
disrupting normal communication. It is this excess of dopamine that is
responsible for cocaine’s euphoric effects.
4. With repeated use, cocaine can cause long-term changes in the brain’s
reward system and in other brain systems as well, which may eventually
lead to addiction. With repeated use, tolerance to the cocaine high also
often develops. Many cocaine abusers report that they seek but fail to
achieve as much pleasure as they did from their first exposure. Some
users will increase their dose in an attempt to intensify and prolong the
euphoria, but this can also increase the risk of adverse psychological or
physiological effects.
5. Dopamine-rich brain regions such as the ventral tegmental area, nucleus
accumbens, and prefrontal cortex are frequent targets of cocaine
addiction research.
- 20 -Slide 31: Dopamine (D2) Receptor Availability
1. This slide features brain images showing decreased dopamine (D2)
receptors in the brain of a person addicted to cocaine versus D2
receptors in the brain of a non-drug user.
2. The dopamine system is important for conditioning and motivation, and
alterations such as this are likely responsible, in part, for the diminished
sensitivity to natural rewards that develops with addiction.
3. The scan on the left side of the screen depicts the brain of a non-drug
using control. Notice the bright colors (red and orange) in the reward
center (the egg-shaped areas towards the top of the scan). Bright colors
indicate that there is a lot of activity occurring in the scanned individual’s
reward center.
4. The scan on the right side of the screen depicts the brain of a cocaine
abuser who has been matched to the control in terms of age, race, etc.
Notice that there are no bright red and orange colors in the reward
center. Essentially, you see virtually no dopamine activity in the reward
centers of the cocaine abuser’s brain, suggesting very severe disruption
of the dopamine neurons.
5. If you were to apply emotions to the cocaine abuser, how would he/she
be feeling? He/she would feel depressed, sad, distraught, etc.
- 21 -Slide 32: Crack/Cocaine Intoxication
1. Acute intoxication with stimulants resembles hypermania or a manic
state. In low doses, a user’s libido is stimulated and sexual performance
is enhanced. In high doses, spontaneous ejaculation and orgasm can
occur. With increasing doses comes poor judgment, indiscretions, sexual
acting-out, and other bizarre behaviors or mental alterations. Acute
stimulant intoxication can result in seizures, confusion, respiratory
depression, chest pain, or cardiac arrhythmias (Gold and Miller, 1997).
2. The acute physical effects of cocaine intoxication include constricted
blood vessels, dilated pupils, and increased temperature, heart rate, and
blood pressure. The duration of cocaine’s immediate euphoric effects,
which include hyperstimulation, reduced fatigue, and mental alertness,
depends on the route of administration. The faster the absorption, the
more intense the high. On the other hand, the faster the absorption, the
shorter the duration of action. The high from snorting may last 15 to 30
minutes, while that from smoking may last 5 to 10 minutes. Increased
use can reduce the period of time a user feels high and increases the risk
of addiction.
3. Taken in small amounts, cocaine usually makes the user feel euphoric,
energetic, talkative, and mentally alert, especially to the sensations of
sight, sound, and touch.
4. Cocaine can also temporarily decrease the need for food and sleep.
Some users find that the drug helps them perform simple physical and
intellectual tasks more quickly, while others experience the opposite
effect.
5. Acute effects of cocaine are similar to other stimulants, such as
methamphetamine.
6. Cocaine users are hypervigilant.
7. Cocaine users will initially feel as if their thinking is ‘clear and focused.’
- 22 -Slide 33: Long-Term Effects of Crack/Cocaine
1. As a result of long-term use of cocaine, an appreciable tolerance to
cocaine’s high may develop, with many addicts reporting that they seek
but fail to achieve as much pleasure as they did from their first
experience.
2. Some users will frequently increase their doses to intensify and prolong
the euphoric effects.
3. While tolerance to the high can occur, users can also become more
sensitive (sensitization) to cocaine’s anesthetic and convulsing effects,
without increasing the dose taken. This increased sensitivity may explain
some deaths occurring after apparently low doses of cocaine.
4. Long-term effects can lead to long-term mental health problems, legal
problems, and problems with SUD and HIV treatment adherence.
Slide 34: Medical Consequences of Crack/Cocaine Abuse
1. Cocaine is a powerful stimulant that causes the heart to work harder and
strains the vascular system.
2. Chronic use can cause heart attacks and strokes.
3. Cocaine increases blood pressure.
- 23 -Slide 35: Crack/Cocaine and Other Stimulant Intoxication &
Withdrawal Syndromes
1. Stimulant withdrawal is not medically life threatening and, unlike alcohol
or barbiturate withdrawal, does not require pharmacological intervention.
2. A characteristic withdrawal-type syndrome usually develops within hours
to days after cessation of prolonged and heavy stimulant use.
3. Stimulant withdrawal symptoms seem to be most severe in the initial
days following cessation of use (Cornish and O'Brien, 1996; Gold and
Miller, 1997).
4. Cocaine intoxication is characterized by the presence of two or more
symptoms listed in the left column.
5. Cocaine withdrawal often has no visible physical symptoms, like the
vomiting and shaking that accompanies withdrawal from heroin or
alcohol.
6. Dysphoric mood must ALWAYS be present when assessing for cocaine
withdrawal, plus at least 2 of the other withdrawal symptoms listed in the
right column.
7. The level of craving, irritability, delayed depression, and other symptoms
produced by cocaine withdrawal rivals or exceeds that felt with other
withdrawal syndromes.
8. A common symptom of cocaine withdrawal is the “cocaine crash,” which
is the craving for another dose of cocaine. Other common withdrawal
symptoms include fatigue, depression, restless behavior, and a feeling of
anxiety or paranoia.
9. During withdrawal, individuals may also experience a period of malaise
when they just do not feel like doing anything at all.
10. Many individuals who have experienced cocaine withdrawal report very
unpleasant and vivid dreams.
- 24 -Slide 36: Adverse Effects of Cocaine Differ by Route of
Administration
1. Different methods of taking cocaine can produce different adverse
effects. Regular intranasal use (snorting) of cocaine, for example, can
lead to loss of the sense of smell; nosebleeds; problems with swallowing;
hoarseness; and a chronically runny nose. Ingesting cocaine can cause
severe bowel gangrene as a result of reduced blood flow. Injecting
cocaine can bring about severe allergic reactions and increased risk for
contracting HIV/AIDS and other blood-borne diseases. Binge-patterned
cocaine use may lead to irritability, restlessness, and anxiety. Cocaine
abusers can also experience severe paranoia—a temporary state of full-
blown paranoid psychosis—in which they lose touch with reality and
experience auditory hallucinations. (NIDA InfoFacts).
2. Snorting can cause short term and long term adverse affects on
nose/lungs.
3. Ingesting can cause severe stomach problems.
4. Injection increases the risk of HIV and other infectious diseases.
Slide 37: [Transition Slide] How Does Crack/Cocaine Differ from
Methamphetamine?
The next few slides pertain to key information to describe the differences
between the two major stimulants of abuse – crack/cocaine and
methamphetamine.
- 25 -Slide 38: Crack/Cocaine vs. Methamphetamine
1. Methamphetamine is structurally similar to amphetamine, but it is quite
different from cocaine. Although these stimulants have similar behavioral
and physiological effects, there are some major differences in their basic
mechanisms of action.
2. In contrast to cocaine, which is quickly removed and almost completely
metabolized in the body, methamphetamine has a much longer duration
of action and a larger percentage of the drug remains unchanged in the
body. This results in methamphetamine being present in the brain longer,
which ultimately leads to prolonged stimulant effects. The half-life of
methamphetamine is about 10 hours, vs. a half-life of cocaine of
approximately 2 hours.
3. Although both methamphetamine and cocaine increase levels of the
brain chemical dopamine, animal studies reveal much higher levels of
dopamine following administration of methamphetamine due to the
different mechanisms of action within nerve cells in response to these
drugs.
4. Cocaine prolongs dopamine’s action in the brain by blocking dopamine
re-uptake. While at low doses, methamphetamine blocks dopamine re-
uptake, methamphetamine also increases the release of dopamine,
leading to much higher concentrations in the synapse, which can be toxic
to nerve terminals.
5. Methamphetamine is neurotoxic, but cocaine does not appear to be
neurotoxic.
6. Methamphetamine-induced paranoia can last as long as 7 to 14 days (or
longer), whereas cocaine paranoia usually subsides within about 4-8
hours following drug cessation.
Slide 39: How Much Does Crack/Cocaine Cost?
1. According to the Drug Enforcement Administration, from January 2007 to
January 2009, the national average price per pure (uncut) gram of
cocaine increased 75%, from $99.24 to $174.03, and the purity
decreased 32%, from 67% to 46%.
2. In Los Angeles, the price for a rock of crack ranges from $30 to $50.
- 26 -Slide 40: A Note Regarding Poly Drug Use
1. Poly drug use often carries with it more risk than use of a single drug,
due to an increase in side effects and drug synergy. The potentiating
effect of one drug on another is sometimes considerable and licit drugs
and medicines – such as alcohol, nicotine and prescription
medications/HIV antiretrovirals – have to be considered in conjunction
with controlled psychoactive substances.
2. The risk level will depend on the dosage level of the ingested
substances. Concerns exist about a number of pharmacological pairings:
alcohol and cocaine can increase cardiovascular toxicity; alcohol or
depressant drugs, when taken with opioids, lead to an increased risk of
overdose; and opioids or cocaine taken with ecstasy or amphetamines
also result in additional acute toxicity.
3. Between 30% and 60% of individuals who take cocaine combine it with
alcohol. Clinical data indicate that the concurrent use of alcohol and
cocaine is associated with increased mortality and morbidity from
cardiovascular complications, hepatotoxicity, and behaviors leading to
personal injury.
4. In 74% of cocaine-related fatalities in the United States, another drug,
usually ethanol, had been co-ingested. The addition of alcohol to cocaine
increases the risk of sudden death 25-fold.
Slide 41: Added Danger: Cocaethylene
1. Cocaethylene is a psychoactive ethyl homologue of cocaine, and is
formed exclusively during the co-administration of cocaine and alcohol
(Landry, 1992).
2. With a pharmacologic profile similar to cocaine, cocaethylene can block
dopamine transporters (Landry, 1992).
3. Cocaethylene formation has been associated with enhanced subjective
euphoria, increased heart rate, and increased plasma cocaine
concentration. These findings suggest that cocaethylene may play a role
in the morbidity and mortality associated with concurrent cocaine/alcohol
abuse (McCance et al., 1995).
- 27 -Slide 42: Added Danger: Levamisole as a Cutting Agent
1. The presence of levamisole with cocaine was reported by several
Community Epidemiology Work Group (CEWG) representatives at the
June 2009 meeting.
2. It is used in veterinary medicine as an anti-parasitic, but is no longer
approved for use in humans.
3. According to some CEWG representatives, the price of cocaine is up,
while other indicators have decreased in recent reporting periods.
Levamisole is being added as filler to make it seem like the same
amount. Also, there are some unsubstantiated/anecdotal comments that
levamisole has some euphoric effects.
Slide 43: [Transition Slide] The Epidemiology of Crack/Cocaine
The next portion of the presentation will provide training participants with a
detailed overview of patterns and trends in crack/cocaine abuse in the United
States. No single drug abuse indicator can tell the full story of the extent or
impact of crack/cocaine use. Therefore, data from several available
indicators are presented in an attempt to paint a comprehensive picture of
who uses crack/cocaine, and the populations in which it is most prevalent.
Slide 44: Past Month Illicit Drug Use among Persons Aged 12 or
Older: U.S. 2009
1. In 2009, 21.8 million individuals aged 12 or older reported past month
use of any illicit drug.
2. Crack/cocaine was the third most prevalent drug, following marijuana and
prescription medications (psychotherapeutics). Approximately 1.6 million
individuals used crack/cocaine at least once in the past month.
3. Alcohol is not included on this graph. As a point of reference, in 2009,
there were a reported 59.6 million past month alcohol users in the U.S.
Additional Information for the Trainer
With regards to long-term trends among persons aged 12 or older, the
prevalence of past month crack/cocaine use was 0.9 percent in 2002,
1.0 percent in 2003, 0.8 percent in 2004, 1.0 percent in both 2005 and
2006, 0.8 percent in 2007, and 0.7 percent in both 2008 and 2009. The
differences between the 2009 estimate and the 2002 through 2007
estimates were statistically significant.
- 28 -Slide 45: Powder and Crack/Cocaine Use: U.S., 2008-2009
1. The past-month estimates for crack/cocaine were similar to the number
and rate in 2008 (1.9 million or 0.7%), but lower than the estimates in
2006 (2.4 million or 1.0%).
2. A total of 7.1 millions persons aged 12 or older was classified with
dependence on or abuse of illicit drugs in 2009.
3. Marijuana was the illicit drug with the highest rate of past year
dependence or abuse in 2009, followed by prescription pain relievers and
cocaine.
Slide 46: Past Year Cocaine and Crack Use among Persons Aged
12 or older, by Race/Ethnicity: 2008-2009
1. Multi-racially identified individuals have highest reported use rates for
powder cocaine.
2. Pacific Islanders, Hispanics/Latinos, and African American rates follow
for powder cocaine.
3. Crack rates are highest among African Americans, followed by multi-
ethnic individuals and Whites.
Additional Information for the Trainer regarding crack/cocaine use by
age group
Individuals in all age groups (12-17 year olds, 18-25 year olds, and
those individuals aged 26 and older) are more likely to report past year
powder cocaine use than crack use.
Both cocaine and crack show highest rates in the 18-25 year old age
group (5.4% for powder cocaine and 0.6% for crack), than persons aged
26 or older (1.5% for powder cocaine and 0.4% for crack) and youth
aged 12 to 17 (1.1% for powder cocaine and 0.1% for crack).
- 29 -Slide 47: Initiation of Cocaine Use: U.S., 2009
1. In 2009, the specific drug categories with the largest number of recent
initiates among persons aged 12 or older were marijuana use (2.4
million) and non-medical use of pain relievers (2.2 million), followed by
non-medical use of tranquilizers (1.2 million), Ecstasy (1.1 million),
inhalants (0.8 million), stimulants (0.7 million), and cocaine (0.6 million).
2. The average age at first use among recent initiates aged 12 to 49 was
20.0 years, which was similar to the average age in 2008 (19.8 years).
3. In 2009, among persons aged 12 or older, there were an estimated
176,000 first-time past year cocaine users who initiated use prior to age
18. This estimate was significantly lower than the estimate in 2008
(239,000).
Slide 48: Treatment Admissions for Crack/Cocaine: U.S., 2007
1. The proportion of crack/cocaine-related treatment admissions is lower
than in the past.
2. The majority of cocaine-related treatment admissions reported smoking
as their preferred route of administration (over time, smoking has
prevailed as the most frequently reported route of administration among
primary cocaine treatment admissions).
3. The majority of cocaine-related treatment admissions were men,
especially the non-smokers.
Additional Information for the Trainer
In 2007, 49% of crack admissions were non-Hispanic Black, 40% were
non-Hispanic White, and 8% were of Hispanic origin.
Average age at admission for crack was 39 years (compared with 34
years for powder cocaine).
Crack cocaine users are an aging population. In 1995, 63% of primary
smoked cocaine (crack) treatment admissions were younger than age
35. By 2005, only 32% of primary crack admissions were in this age
group.
81% of non-crack cocaine admissions reported inhalation as the route
of administration, 11% reported injection, and 5% reported oral
administration.
- 30 -Slide 49: Race/Ethnicity of Crack Treatment Admissions
Answer Key:
Correct response: C (Black/African American)
**Audience Response System (ARS)-compatible slide
Slide 50: Race/Ethnicity of Crack/Cocaine Treatment Admissions:
U.S., 1992 vs. 2008
1. Despite the fact that Blacks/African Americans are the predominant
racial/ethnic group among primary crack cocaine treatment admissions,
the proportion of Black/African American crack-related treatment
admissions has decreased since the early 1990s. Crack use has
increased, however, among Whites and Hispanics/Latinos during the
same time frame.
2. A smaller percentage of Black/African American treatment admissions
also report injecting or snorting cocaine in 2008 vs. 1992, while larger
percentages of Whites and Hispanics/Latinos now report injecting or
snorting cocaine.
- 31 -Slide 51: Treatment Admissions—Trends in Race/Ethnicity for
Four Most Prevalent Illicit Drugs: LA County, CA, 2004 (July-Dec)
vs. 2009 (Jan-June)
1. The racial/ethnic breakdown of local crack/cocaine treatment admissions
differs from that seen at the national level. In 2004 in Los Angeles
County, 56% of the primary crack/cocaine treatment admissions were
Black/African American. By 2009, the proportion of Black/African
American crack/cocaine treatment admissions increased to 61%.
2. This increase in the proportion of Black/African American crack/cocaine
treatment admissions locally is in contrast to data presented on the
previous slide, which indicated a national decline in the proportion of
Black/African American cocaine treatment admissions (for all routes of
administration) from 1992-2008.
3. The vast majority of primary cocaine treatment admissions in Los
Angeles County report smoking as their preferred route of administration,
so the increase in the proportion of Black/African American cocaine
admissions is likely being driven by crack treatment admissions,
specifically.
Slide 52: Lifetime and Past Year Crack Cocaine Use, by
Geographic Region: 2009
1. This figure presents regional estimates of the percentage of lifetime and
past year crack cocaine use in 2009.
2. The national rate of lifetime crack cocaine use was 3.38%, and the past
year rate of crack use was 0.4%.
3. The lifetime rate of crack use was highest in the West (4.37%), followed
by the mid-west (3.2%), south (3.1%), and northeast (2.6%).
4. The past year rate of crack use has a slightly different pattern, however.
The highest past year rate was seen in the northeast and south (0.5%
each), followed by the west and mid-west (0.3% each).
- 32 -Slide 53: Percentages of Persons Aged 12 or Older Reporting
Past Year Cocaine Use, by State
1. This figure presents State-level estimates of the rate of cocaine use in
the year 2002-2003 (the most recent time frame for which this type of
state level figure is available).
2. Five states with the highest rates fall into the top quintile (fifth) and are
shown in red; States with the lowest rates are in the bottom quintile and
are shown in dark blue.
3. Cocaine use rates ranged from a low of 1.6% in Idaho to a high of 3.9%
in Colorado.
4. Colorado, Arizona, New Mexico, Louisiana, Missouri, and a few
Northeast states have highest rates.
5. California next highest rate.
6. For crack specifically (data not shown), the highest % were seen in
Missouri (1.5%), the District of Columbia (1.3%), and Rhode Island
(1.4%) (2002-04).
Slide 54: U.S. Cocaine-Related Emergency Department Visits:
2007
1. Cocaine accounted for 29% of drug misuse and abuse emergency
department visits.
2. When the margin of error is taken into account, cocaine was involved
significantly more often than any other illicit drug.
3. Cocaine involvement was more common for patients aged 21 to 54 and
less common for younger and older patients.
4. Males were more likely than females to have a drug-related ED visit
involving cocaine, marijuana, heroin, or stimulants.
Additional Information for the Trainer
The Drug Abuse Warning Network also has a drug-related mortality
component. The mortality component of DAWN does not rely on a
statistical sample of ME/Cs. Findings cannot be considered
representative of ME/Cs that did not participate, and results cannot be
extrapolated to the United States as a whole. The 2008 full report,
including area profiles, is available at:
https://dawninfo.samhsa.gov/files/ME2008/ME08_Complete.pdf.
- 33 -Slide 55: Crack/Cocaine Use among Adolescents: 2009
1. According to the 2009 Monitoring the Future survey—a national survey of
8th, 10th, and 12th graders—there were continuing declines reported in
the use of crack/cocaine.
2. Among 8th and 10th graders, crack use rose gradually in the 1990s: from
0.7% in 1991 to 2.1% by 1998 among 8th graders, and from 0.9% in
1992 to 2.5% in 1998 among 10th graders. And, as just discussed, use
among 12th graders peaked in 1999 at 2.7% and among young adults at
1.4%.
3. Since those peak years, crack use has declined appreciably—by about
half among 8th, 10th, and 12th graders—yet it has held fairly steady
among college students and young adults, at least until 2007, when use
among college students finally appeared to decline. In general, the 2009
prevalence rates for this drug are relatively low—between 0.3% and
1.3% in all five groups.
4. Twelfth graders have the highest prevalence rate, and within that group
annual crack prevalence among the college-bound is considerably lower
than among those not bound for college (0.9% for college-bound vs.
2.8% for non-college-bound in 2009). (MTF 2009 report).
5. Crack currently has a relatively low lifetime prevalence rate in all grade
levels: 1.7% for 8th, 2.1% for 10th, and 2.4% for 12th graders.
6. Of all students reporting any cocaine use, significant proportions have
some experience with crack: nearly two thirds of 8th grade cocaine users
(65%), and about two fifths of 10th grade (46%) and 12th grade users
(40%) reported using crack (Data not shown).
7. Powder cocaine is more prevalent among secondary school students
than crack (data not shown).
Additional Information for the Trainer
According to the CDC-funded Youth Risk Behavior Surveillance Survey
(data not shown), Overall, the prevalence of lifetime cocaine use was
higher among White and Hispanic than Black students, and higher
among Hispanic than White students. In addition, the prevalence of
current cocaine use was higher among Hispanic (4.3%) than white
(2.4%) and black (1.9%) students.
- 34 -Slide 56: Gender Differences in Cocaine Use
Answer Key:
Correct response: B (Men have a greater number of intense
effects)
**Audience Response System (ARS)-compatible slide
Slide 57: Gender Difference in Cocaine Use
1. Gender differences exist in plasma peak levels.
2. Males report increased/rapid effects.
Slide 58: Gender Difference in Cocaine Use
1. Men and women both experienced impairment in several areas, including
attention, concentration, memory, and academic attainment.
2. Men experienced a greater level of impairment with regards to visual-
spatial, motor, language, and executive functioning measures.
3. These gender differences may impact treatment plans for both genders.
Slide 59: Gender Differences in Cocaine Addiction and Recovery
1. In the first brain imaging study of cocaine craving by cocaine-addicted
women, NIDA-funded researchers have made observations that, if borne
out in larger studies, may point to neurological sources of these
differences (see next slide for more info).
2. Women are more likely than men to seek treatment for their cocaine
addiction in response to depression symptoms.
3. Women are more likely than men to relapse because of interpersonal
problems.
4. It is important to address craving and internal and external triggers to
help prevent further relapse.
- 35 -Slide 60: Men and Women May Process Cocaine Cues Differently
1. In both men and women, cue-induced cocaine craving activated several
brain areas involved in determining a cue's reward value and controlling
reward-related behaviors, including the right nucleus accumbens—a
structure that processes anticipated and attained rewards, and seems to
produce the expectation of pleasure during drug craving. Increased
activity in the nucleus accumbens was seen for both men and women.
2. The amygdala generates and regulates emotional responses, and
assesses the positive or negative value of experiences and forms
associations between experiences and emotional consequences.
Reduced neural responses in the amygdala may result from greater
activation of the frontal cortex in women. In men, however, increased
activity was seen in the amygdala during cocaine craving.
3. The frontal cortex monitors the relationship of drug cue to drug
availability, and inhibits or controls the activity of structures involved in
emotional responding to drug cues. Observations were consistent with
previously reported sex differences in frontal cortical areas. Activity in this
region increased at a greater extent for women than men.
4. "This research reveals that men and women differ in a critical brain area
in their responses to cocaine craving," says Dr. Steven Grant of NIDA's
Division of Clinical Neuroscience, Development, and Behavioral
Treatments. "Differences in the amygdala may indicate that male and
female abusers crave the drug for different reasons or hope to achieve
different results from taking the drug. Imaging studies that examine
gender differences in specific behavioral aspects of drug craving will
provide insight on how to tailor treatment programs to meet the needs of
men and women."
Slide 61: [Transition Slide] “Linked Epidemics”: Substance Use
Disorders and HIV/AIDS
The next portion of the presentation corresponds to the relationship between
substance use disorders in general and HIV/AIDS. Injection of drugs such as
heroin, cocaine, and methamphetamine accounts for more than a third of
new AIDS cases. Injection drug use is also a major factor in the spread of
hepatitis C, a serious, potentially fatal liver disease. Injection drug use is not
the only way that drug abuse contributes to the spread of infectious
diseases. All drugs of abuse cause some form of intoxication, which
interferes with judgment and increases the likelihood of risky sexual
behaviors. This, in turn, contributes to the spread of HIV/AIDS, hepatitis B
and C, and other sexually transmitted diseases.
- 36 -Slide 62: Substance Use Disorders are a Significant Risk Factor
for HIV/AIDS in the U.S.
1. Early in the epidemic, it became apparent that the HIV virus was being
spread, not only through sexual contact with infected people, but also
through the sharing of injection equipment and drug solutions by injection
drug users (IDUs). With such a significant number of HIV cases acquired
through injection drug use, effective prevention interventions were
needed. NIDA's research showed that comprehensive HIV prevention--
including drug addiction treatment and community-based outreach, in
combination with testing and counseling for HIV and other infections- -is
an effective approach. Such an approach continues to be important in
reducing HIV infection risk and preventing the spread of HIV and other
blood-borne infections in drug-abusing populations.
2. In addition to injection drug use, drug abuse plays other, less recognized,
roles in HIV transmission. First, drug intoxication affects users' mental
status and judgment, which, in turn, can increase the likelihood that they
will engage in high-risk sexual behavior. Further, addiction to drugs, as
documented for crack cocaine, can further increase users' exposure to
unprotected sex as a means to obtain drugs. Finally, physiological
consequences of drug abuse may alter susceptibility to infection and
interact with HIV treatment drugs.
3. Of AIDS diagnoses in 2008 among male adults and adolescents, 64%
were attributed to male-to-male sexual contact and 13% were attributed
to injection drug use. Approximately 16% of AIDS diagnoses were
attributed to heterosexual contact and 6% were attributed to male-to-
male sexual contact and injection drug use.
4. Most (74%) of the AIDS diagnoses in 2008 among female adults and
adolescents were attributed to heterosexual contact, and 24% were
attributed to injection drug use.
5. All displayed data have been estimated. Estimated numbers resulted
from statistical adjustment that accounted for reporting delays and
missing risk-factor information, but not for incomplete reporting.
6. Heterosexual contact is with a person known to have, or to be at high risk
for, HIV infection.
- 37 -You can also read