Cocaine and the critical care challenge - Review Article
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Review Article
Cocaine and the critical care challenge
Christina M. Shanti, MD; Charles E. Lucas, MD, FCCM
Objective: Cocaine, which first made its appearance >1,000 the brain, heart, lung, kidneys, gastrointestinal tract, muscula-
yrs ago, is now widely used throughout the world. The physiologic ture, and other organs. These harmful effects are additive to
responses to cocaine may cause severe pathologic effects. This preexisting organ dysfunction.
review highlights the many critical care challenges resulting from Intervention: Recognition of associated cocaine injury alerts
these effects. the physician that organ dysfunction is more likely to occur and
Design: Historical vignettes, epidemiologic factors, modes of to be more severe. Such anticipation helps plan for therapy in the
preparation and delivery, and the physiologic and pharmacologic critical care setting.
effects of these agents are presented. Results and Conclusions: Cocaine use is an expanding health
Setting: Cocaine causes intense vasoconstriction, which po- hazard, despite intense governmental efforts to contain its dis-
tentially causes damage to all organ systems. Examples of these tribution and use. Recognition of the signs and symptoms of
toxicities are presented. cocaine toxicity help anticipate the subsequent organ dysfunction
Patients: The adverse multisystem responses to cocaine ex- and implement earlier organ system support. (Crit Care Med 2003;
posure produce organ failure, which challenges diagnostic accu- 31:1851–1859)
racy and therapeutic intervention. Organ system failure involves KEY WORDS: cocaine; critical care; organ failure
C ocaine has become a major gious ceremonies, the sovereign Inca, algesia of the tongue and, subsequently,
confounder in the diagnosis and occasionally soldiers (2). The coca its use in relieving laryngeal pain became
and treatment of surgical leaves were also given by the Inca as a popular in England and America (2).
emergencies. This complex reward or token of appreciation (1). Coca During the 1880s Freud experimented
drug made its first appearance about leaf storehouses were built along the with cocaine and used it to treat opiate
1200 yrs ago in the northern Andes of roads to supply messengers who carried addiction (1, 2, 4, 5). Several of his arti-
Peru and Bolivia. Figures depicted on ce- messages at a rate of 150 miles a day (2). cles describe its powerful effects and ad-
ramic pottery show that coca leaves were The word cocada is a measure of the vocate its use for increasing physical ca-
harvested and chewed by the Indians (1– distance a man can walk without tiring pacity, treating digestive disorders and
3). Anthropologic studies reveal that co- under the influence of the coca leaf. cachexia, counteracting morphine and al-
caine-filled saliva of the chewed coca When Pizarro conquered the Incan Em- cohol withdrawal, treating asthma, and
leaves was used as a local anesthetic dur- pire in 1533, the Indian slaves working in stimulating sexual activity. The strong
ing trephining operations for traumatic Spanish silver mines chewed the coca leaf euphoriant properties of cocaine contrib-
intracranial hematomas (1). The Incas to fight fatigue and hunger (1, 3). The uted to Freud’s transient addiction. Inter-
founded their capital at Cuzco, Peru, in Spanish capitalized on this practice by estingly, Freud’s experimentation with
1021 AD, and their empire flourished (2). enforcing a 5% tax on the coca crop. The cocaine preceded his work in psychoanal-
They believed in a supreme being repre- church received its share of the tax ysis and hypnosis. This period of cocaine
sented by the sun, worshipped that which money and supported this practice (2). use was eliminated from his autobiogra-
gave life, including the coca plant, named The Spaniard Nicolas Monardes wrote the phy (1). Concomitantly, Freud’s friend
their first queen “Mama Cuca,” and first scientific article on coca in 1565 (1, Carl Koller, a Viennese ophthalmologist,
placed the coca leaf on the royal emblem 2, 4). Later, in 1580, he brought coca conducted animal and clinical experi-
(1, 2). Consumption of the “divine” coca
leaves to Europe (1, 2). Coca use in Eu- ments that corroborated his theory that
leaf was reserved for priests during reli-
rope flourished during the next 300 yrs, cocaine can produce anesthesia in the
and many publications appeared (1, 4). In cornea and conjunctiva, thus introducing
1854, the United States sent its first in- cocaine as a local anesthetic for ophthal-
From the Department of Surgery, The Detroit Med-
vestigational expedition to South Amer- mologic procedures (1–3, 6).
ical Center/Wayne State University School of Medicine,
Detroit, MI. ica. Pizzi, a laboratory director at LaPaz The North American medical experi-
Supported, in part, by an Interstitial Fluid Fund, in Bolivia, extracted the alkaloid (2). In ences with cocaine date to Halstead who
account 4-44966. 1857, Gaedicke extracted a sublimate of performed the first nerve block using in-
Address requests for reprints to: Charles E. Lucas,
small crystals he named erythroxyline (1, jectable cocaine; by 1886, he was battling
MD, Department of Surgery, Wayne State University,
4201 St. Antoine, Room 2V, Detroit, MI 48201. E-mail: 2). In 1860, Niemann isolated the alkaloid his own addiction to cocaine, which re-
clucas@med.wayne.edu from the coca leaves and named it co- portedly reached 2 g/day (1, 3, 6). George
Copyright © 2003 by Lippincott Williams & Wilkins caine (1, 2, 4). In 1862, Schroff and De- Crile in 1897 used direct nerve infiltra-
DOI: 10.1097/01.CCM.0000063258.68159.71 marle observed that cocaine produced an- tion of cocaine in amputation. Cushing
Crit Care Med 2003 Vol. 31, No. 6 1851performed the first herniorrhaphy using (1, 6). The past generation has seen a new main producing countries (1, 3, 8). Co-
cocaine-induced nerve block. By 1898 co- upsurge in the popularity and use of co- caine in the United States has tradition-
caine became widely used by several phy- caine partly due to the widespread avail- ally come mostly from Columbia and
sicians to induce spinal anesthesia (1). ability of inexpensive crack cocaine (1, 7). Peru, although more and more is coming
Sir Arthur Conan Doyle described his from Asia (8). The coca bush may grow to
own addiction through Sherlock Holmes EPIDEMIOLOGY 8 feet with leaves twice the size of a
who, from 1888 until 1891, was tireless thumbnail. Cocaine can be produced
with cocaine his weapon. Holmes became Cocaine abuse and dependence is epi- within 18 months of planting and
increasingly paranoid and withdrawn, demic in the United States. More than 50 throughout a 40-yr lifespan. The leaves
and he disappeared at Reichenbach Falls million Americans have used cocaine, are harvested in the months of March,
in 1891 (1, 4). When he reappeared in and ⬎6 million Americans of all ages use June, and November. They are placed in
1894 a pipe had replaced the cocaine ad- it on a regular basis. The national preva- gasoline drums with kerosene and other
diction, and his health was restored (4). lence of cocaine use is highest among 18- solvents. The mixture is allowed to soak,
The Age of the Cocainized Nostrum to 25-yr olds but is becoming quite pop- then the fluid is drawn off, and the leaves
began in the 1890s and ended in 1914 (1). ular in the teenage group. The reported are removed. The remaining thick paste
Pemberton, a Georgia pharmacist, com- use is 3% of 12- to 17-yr olds including is placed in containers and sold to “labo-
pounded the Coca-Cola syrup in 1886. about 1% who use it daily (8). In New ratory agents.” The laboratories refine
This was a combination of the coca leaf York City between 1990 and 1992, 26.7% the paste into the cocaine powder (1).
cocaine extract and the African kola nut of fatal injury victims had cocaine metab- Coca leaves yield approximately 0.65% to
caffeine extract. Pemberton sold 25 gal- olites in their urine or blood. More than 1.2% of their weight in cocaine (1, 3).
lons of his syrup for $50 and used 90% of 30% of deaths after cocaine use were the Cocaine, or benzoylmethylecgonine, is
his profits for advertisement (5). Candler result of drug intoxication; 65% involved treated with hydrochloric acid to form
bought Coca-Cola and introduced the soft traumatic injuries from homicide, sui- the cocaine hydrochloride salt, which is
drink in 1892 as a tonic for the elderly cide, traffic accidents, and falls. Death freely soluble in water and can be injected
people who were easily tired. Cocaine was after cocaine use is one of the five leading intravenously or absorbed through the
sold in cigarettes, cigars, inhalants, coca causes of death in the 15- to 44-yr-old age nasal mucosa (1, 8). Freebase and crack
liquors, crystals, solution form, and wine group (9). More than 20% of patients cocaine are prepared from the same co-
(1, 5). Cocaine was promoted for the with orthopedic injuries in an inner city caine alkaloid form using two different
treatment of opiate and alcohol addiction, environment test positive for cocaine. techniques (8).
runny nose, sore throat, headaches, fatigue, This is often associated with more severe Freebase. Cocaine hydrochloride is
hay fever, high blood pressure, nervous dis- injuries requiring a longer length of stay dissolved in water, and ammonia is added
orders, and even tuberculosis (5). (10). About 20% of blunt trauma patients as a base. The cocaine base is then dis-
Soon, nonmedical cocaine use and and 57% of penetrating trauma patients solved in ether and is extracted by evap-
abuse increased. By 1902, Crother re- test positive for cocaine (11). In a study of orating the ether at low temperature. The
ported that only 5% of the cocaine sold in 42,981 patients admitted to R. Adams cocaine freebase can then be smoked,
New York and other metropolitan areas Cowley Shock Trauma Center in Mary- mixed with tobacco, or inhaled by heat-
was used for medicine and dentistry (1). land between July 1984 and December ing it in special pipes. Occasionally,
Medical experts issued notes of caution 1998, there was a 262% increase in co- traces of the highly volatile ether remain
on cocaine use, and the public critical caine use in all victims of violence and a after the extraction process, and this may
attitude toward cocaine, in 1903, caused 161% increase in victims of nonviolent ignite, causing ether burns particularly of
the manufacturer to voluntarily remove injuries (12). the face and trachea (8).
cocaine from the Coca-Cola drink (5). The cocaine supply industry is grow- Crack Cocaine. Cocaine hydrochloride
The Coca-Cola company today still ex- ing. In Columbia, the coca fields have is dissolved in water, then mixed with
tracts cocaine from imported leaves but expanded from 100,000 acres in 1994 to baking soda. The mixture is heated, and
turns it over to the government for med- 250,000 acres in 1998. According to the cocaine base precipitates into a soft
ical use. Processed leaves are still used as United Nations figures, coca production mass that dries into a hard “rock.” Crack
a flavoring agent (3). has doubled since 1985, and the drug cocaine may be smoked using a glass or
In 1913, President Taft pronounced prices are falling (13). The war against regular pipe or by mixing it with tobacco
cocaine to be “public enemy #1,” and, in drugs has become increasingly more or marijuana. The name crack comes
1914, Congress passed the Harrison “Nar- costly during the past two decades. The from the “popping” sound the cocaine
cotics” Tax Act, which required persons federal government drug budget has crystals make when smoked. Crack is in-
authorized to handle and manufacture grown from $1.5 billion in 1981 to $14 expensive and readily available; it is cur-
drugs to keep a record of all “narcotics” billion in 1995, and the epidemic contin- rently the most popular form being used
(including cocaine) in their possession ues to grow (8, 13). by most cocaine addicts (8).
(1, 6, 7). This mislabeled cocaine as a Cocaine is also known as Snow, Flake,
narcotic and drove it underground (1). COCAINE PREPARATION Her, Girl, Lady, Blow, She, Jam, Happy
Nationwide, educational efforts were Trails, Rock, Nose-candy, The Star Span-
launched, and by the 1950s, recreational From Leaf to Powder. Cocaine is an gled Powder, Dama Blanca, The gift of the
use was minimal, whereas its use in med- alkaloid of the Erythroxylin coca bush, a Sun God, Heaven Leaf, The Rich Man’s
ical practice particularly as a topical an- shrub grown in the Andes mountains in Drug, Speedball Coke, Gold Dust, Ber-
esthetic, decongestant, and vasoconstric- western South America with Peru, Co- nice, and The Pimp’s Drug (1, 8). A
tor for intranasal procedures continued lumbia, Ecuador, and Bolivia being the “speedball” is a combination of cocaine
1852 Crit Care Med 2003 Vol. 31, No. 6and heroin taken intravenously, presum- tion potential and can slow the conduc- TOXICOLOGICAL SCREENING
ably doubling the “rush” (1, 3). Patients tion rate of the action potential; this may
on methadone often turn to cocaine for a cause cardiac dysrhythmias and sudden Screening for cocaine and its metabo-
kick because its euphoriant effects are death (8, 14). In the mesolimbic and me- lites can be performed on many biological
not altered by methadone (3). socortical areas of the brain, cocaine fluids and tissues including urine, serum,
blocks the dopamine uptake pump and saliva, gastric aspirates, breast milk,
impairs dopamine reuptake into the pre- meconium, and even hair (24 –26). In the
PHARMACOLOGY AND
synaptic neurons, which results in dopa- acute setting, urine testing is widely used
PHARMACOKINETICS and is least expensive. Two methods are
mine accumulation in the synaptic cleft
Cocaine is benzoylmethylecgonine, an and sustained stimulation of dopaminer- generally employed. The first is an immu-
ester of benzoic acid and the nitrogen- gic receptors; this produces intense eu- noassay qualitative method for cocaine’s
containing base ecgonine; ecgonine is a phoria with increased alertness and self- most common metabolite, benzoylecgo-
tropine derivative and is the parent com- confidence (8, 14, 15). Concomitant nine. Depending on the concentration
pound of atropine and scopolamine. Co- suppression of the activity of the pontine cutoff set by the lab, this test can be 94%
caine is the only naturally occurring local nucleus and the locus ceruleus sup- to 100% specific. The lower the concen-
anesthetic (1). Because it is absorbed presses feelings of fear and panic (8, 14). tration cutoff (lowest is 150 ng/mL), the
through any mucous membrane, cocaine The craving for cocaine comes from de- higher the sensitivity and specificity. The
can be inhaled, snorted, or injected intra- pletion of dopaminergic stores in the pre- immunoassay test can be confirmed if
venously or intramuscularly (14). The synaptic neurons after repetitive use (15). desired by a quantitative gas chromatog-
half-life is 30 –90 mins. Smoked crack This causes an increase in the number of raphy-mass spectrometry method. This is
cocaine is absorbed through the pulmo- the presynaptic dopaminergic receptors, substantially more expensive($200.00 vs.
nary vasculature and reaches the cerebral which require larger and larger doses of $0.10) and is done only when specifically
circulation in 6 – 8 secs, producing in- cocaine to produce the same euphoric requested. In general, urine testing will
tense euphoria. Intravenous cocaine effect. This tachyphilactic phenomenon remain positive up to 6 –14 days, but the
takes about 12–16 secs to reach the brain. within the central nervous system is only results of both tests, however, depend on
Snorted cocaine, on the other hand, re- partially seen in the cardiovascular sys- the amount of cocaine used, the time it
quires 3–5 mins to reach the brain. In- tem, resulting in the catastrophic cardio- was used last, and the patient’s renal
tranasal cocaine causes local vasocon- vascular events often seen during a co- function. Test results should, therefore,
striction, thus limiting quick absorption; caine binge (8). Cocaine also blocks be interpreted while taking the above into
its plasma concentration peaks at 60 presynaptic serotonin binding sites and consideration (27–29).
mins and persists for up to 6 hrs. This inhibits serotonin reuptake and removal.
explains why snorted cocaine yields the The consequent serotonin accumulation PATHOPHYSIOLOGY
most prolonged euphoria (8). in the brain causes intense stimulation
The highest organ concentrations of and may precipitate seizures. Intense Cocaine exposure produces a myriad
cocaine appear in the brain, spleen, kid- central nervous system stimulation is of signs and symptoms, which obscure
ney, and lungs. About 80% to 90% of also achieved by direct cocaine binding to the classic response to injury and hem-
cocaine is metabolized to a) ecgonine sigma and muscarinic (M1 and possibly orrhagic shock. Acute cocaine exposure
methyl esters by rapid enzymatic hydro- M2) receptors (14). In high concentra- in high doses may be associated with hy-
lysis by plasma and liver esterases; b) tions, cocaine can act as an anticholin- perthermia, hypertension, tachycardia,
benzoylecgonine by spontaneous nonen- ergic drug through muscarinic receptor mydriasis, seizures, stupor, and respira-
zymatic hydrolysis; and c) norcocaine by blockade, resulting in decreased gastric tory and cardiac depression. Death can
liver N-demethylation. Between 1% and motility and subsequent ulceration sec- occur within 2–3 mins, and attention
5% remains unaltered and is excreted in ondary to prolonged acid exposure (8, should be paid to securing the airway,
the urine 3 to 6 hrs after use. Cocaine 15). assuring breathing, and close cardiac
metabolites can be detected in the urine In the lungs, cocaine impairs alveolar monitoring. Beta blockade may be
for 6 to 14 days after administration. macrophage function and cytokine produc- needed to control the acute sympathomi-
When taken in proximity to ethanol in- tion, which may result in local immuno- metic effects, whereas barbiturates are
gestion, cocaine is transesterified by a suppression and infectious complications generally used for management of con-
liver esterase to ethylcocaine, which po- (16). It also activates polymorphonuclear vulsions. Benzodiazepines can be used for
tentiates cocaine’s systemic toxicity (8, cells, resulting in a burst of acute inflam- anxiety as well as the treatment of hyper-
14). matory activity that may contribute to fur- tension (14). The treatment of these sys-
Cocaine blocks the reuptake of cat- ther lung injury (17). Cocaine also in- temic effects of acute cocaine exposure is
echolamines by the presynaptic sympa- creases platelet activation and aggregation, often complicated by more life-threaten-
thetic nerve terminals, resulting in accu- decreases protein C and antithrombin III ing organ-specific toxicities.
mulation of catecholamines in the levels, and increases plasminogen activator Central Nervous System Complica-
synaptic clefts and increasing cell recep- inhibitor activity. This induces a prothrom- tions. Perhaps the most devastating cen-
tor stimulation. Cocaine exerts its local botic effect in both small and large blood tral nervous system complication of co-
anesthetic effects by blocking fast sodium vessels (18 –20). Animal studies show that caine is a stroke. The stroke can be
channels in neuronal cells and impairing cocaine, in a dose-dependent fashion, af- ischemic secondary to cocaine-related va-
conduction of nerve impulses (14). In the fects the heat regulation center in the hy- sospasm, or cerebral artery thrombosis
cardiac myocyte, it decreases the rate of pothalamus and causes significant alter- or, rarely, cerebral vasculitis (30 –33). A
depolarization and amplitude of the ac- ations in the core temperature (21–23). stroke can also be hemorrhagic second-
Crit Care Med 2003 Vol. 31, No. 6 1853ary to a cocaine-induced hypertensive cri- hemorrhage (37). The frequency of pul- farction is seen less commonly because of
sis resulting in ruptured berry aneurysms monary infarction is not known. These the dual blood supply, but occasionally
or arteriovenous malformations (34, 35). conditions present a special threat to the the severe vascular spasm and arterial
A patient with severe injury and hypovo- cocaine user and may compound the re- endothelial injury with cocaine binging
lemia due to hemorrhage may exhibit a spiratory compromise due to injury or may result in platelet aggregation and
normal mean arterial pressure due to sepsis. Both upper and lower respiratory pulmonary infarction (8, 42).
pathologic vasoconstriction; this combi- tract complications are common. Habit- Cocaine’s direct endothelial toxicity
nation promotes added cerebral insult, ual snorters can present with epistaxis, causes increased permeability and non-
which may not be fully appreciated by the nasal septal perforations, and oropharyn- cardiogenic pulmonary edema (37, 42).
resuscitation team. Cocaine can also pre- geal ulcers due to vasoconstriction and Cocaine can also cause markedly in-
cipitate generalized tonic and clonic con- consequent ischemic necrosis (38). Pre- creased vascular resistance and acute left
vulsions and focal seizures. These are septal cellulitis, palatal necrosis, and os- ventricular failure, which results in car-
usually secondary to intense central ner- teolytic sinusitis have also been reported diogenic pulmonary edema (8). These
vous system stimulation either directly (39 – 41). Inhalation of hot cocaine vapors pulmonary changes appear to be additive
by cocaine on the sigma and muscarinic and spontaneous ignition of residual to those seen with hemorrhagic shock
receptors or indirectly by the increase in ether in freebase cocaine cause thermal and sepsis. Patients with moderate in-
serotonin central nervous system levels. burns of the face and upper airway, lead- sults may undergo successful treatment
Patients who are seizure prone have a ing to both acute inflammation of the only to succumb to progressive cardio-
lower seizure threshold with cocaine ex- tongue, epiglottis, vocal cords, and tra- pulmonary dysfunction. Chronic cocaine
posure (36). Seizures can also result from chea and result in subsequent chronic use may result in pulmonary artery hy-
the acute hyperthermia due to cocaine- scarring. As a direct airway irritant, co- pertension and hypertrophy leading to
induced increased muscular activity and caine damages bronchial epithelial cells, cor pulmonale, a complication that is in-
intense vasoconstriction, which impairs exposes and stimulates vagal receptors, dependent of the dose, frequency, or
heat dissipation (8). Cocaine-induced sei- and causes severe bronchospasm, thus route of cocaine administration (45, 46).
zures may complicate the initial resusci- exacerbating asthma (42– 44). Patients Pneumomediastinum, pneumoperi-
tation of an injured patient and may com- present with wheezing, hoarseness, cardium, and pneumothorax can occur in
promise the establishment of an airway coughing, carbonaceous sputum, and cocaine smokers who take deep pro-
and institution of intravenous catheters. singed nasal hairs (37, 38, 42). Expecto- longed inspirations followed by a Valsalva
Repetitive small doses of cocaine cause ration of black sputum results from the maneuver to increase absorption and in-
subthreshold stimulation of the limbic inhalation of the carbonaceous residue tensify central nervous system stimula-
system and ultimately precipitate a sei- from butane- or alcohol-soaked cotton tion and euphoria. Absorption of cocaine
zure; a phenomenon known as kindling sponges used to ignite the cocaine (42). is also enhanced by positive-pressure ven-
(36). Cocaine also acts as an antigen and tilation applied through direct mouth-to-
Cocaine-related accumulation of do- induces immunoglobulin-E production. mouth contact with another person.
pamine in the basal ganglia can cause a This reaction occurs on the surface of These maneuvers cause an acute eleva-
variety of movement disorders, namely mast cells after reexposure to cocaine and tion in airway pressure, which predis-
Tourette’s syndrome, tardive dyskinesia, causes the release of histamine, seroto- poses to alveolar rupture. Free air dis-
choreoathetosis, akathisia, and dystonic nin, and eosinophil chemotactic factor, sects into the mediastinum, neck,
reactions. In fact, cocaine users with cho- which causes direct lung injury (8). Co- pericardium, and pleura (11, 37, 38, 47).
rea and akathisia are known as “crack caine also acts as a hapten and, combined A “Hamman crunch” can be heard upon
dancers” (8). Manifestations of these be- with albumin or globulin, induces hyper- auscultation of the precordium during
haviors after operative treatment of an sensitivity pneumonitis (also known as systole (11, 47). Substernal chest pain is
emergency surgical problem may be con- crack lung), which is characterized by often present (11, 28). These entities may
fused with therapeutic drug reactions, fever, dyspnea, wheezing, and productive not always require tube thoracostomy be-
electrolyte abnormalities, psychological cough associated with diffuse interstitial cause they resolve spontaneously (37, 38,
aberrations, or even unusual manifesta- and alveolar infiltrates. Less commonly, 42). Treatment is supportive during the
tions of sepsis. Recently, a 53-yr-old co- cocaine causes bronchiolitis obliterans subsequent period of observation (38,
caine-using woman presented 3 days after (42). Pulmonary granulomas and pneu- 47). Rarely does the air dissect centrally
a 20% total body scald burn with confu- moconiosis-like reactions may be occa- in both the arterial and venous systems.
sion and sepsis. She developed excessive sionally found in cocaine users due to Venous air may pass through the left
urine output, which was attributed to the inhalation of talc, cellulose, or silica, heart and cause diffuse embolization and
inappropriate polyuria of sepsis, when, in which are often mixed with cocaine (38). organ failure. Symptoms may include
fact, the patient had suffered from a co- Regardless of route of administration, temporary visual disturbances, confusion
caine-induced stroke 3 yrs earlier that led cocaine causes both pulmonary and bron- or convulsions from cerebral air emboli-
to diabetes insipidus. Her confusion was chial arterial constriction and ischemia zation, renal insufficiency, and myocar-
not due to sepsis, as originally thought, leading to interstitial and alveolar hem- dial infarction from coronary artery air
but was a result of her cocaine-induced orrhage (37, 38). Inhaled impurities can embolization (11).
stroke. cause injury directly to the alveolar epi- Cardiac Complications. A wide range
Pulmonary Complications. Pulmo- thelium and pulmonary basement mem- of cardiac complications result from both
nary complications secondary to cocaine brane. Up to 25% of cocaine smokers acute and chronic cocaine use. Acute
use occur in 25% of users and extend present with hemoptysis secondary to myocardial infarction may occur in pa-
from simple asthma to fatal pulmonary pulmonary hemorrhage. Pulmonary in- tients with normal or diseased coronary
1854 Crit Care Med 2003 Vol. 31, No. 6arteries, and both Q-wave and non-Q- of norepinephrine or myocardial stun- unconscious secondary to intoxication of
wave changes may be seen on the elec- ning secondary to coronary vasospasm, traumatic brain injury.
trocardiogram (8). The pathophysiology and transient cessation of blood flow. The Cocaine-induced mesenteric arterial
of myocardial infarction is multifactorial. cardiac dilation is reversible if circulating vasoconstriction results in decreased in-
Cocaine increases the heart rate, blood catecholamine levels are promptly nor- testinal blood flow, petechial hemor-
pressure, and systemic vascular resis- malized. Chronic cocaine use, however, rhages, bowel edema, mucosal ulcer-
tance by blocking the reuptake of norepi- results in persistently high concentra- ation, necrosis, and perforation (59, 60).
nephrine in the sympathetic nerve termi- tions of catecholamines, which causes The patient will have constant pain in the
nals throughout the cardiovascular myocytolysis and fibrosis and subsequent mid abdomen associated with moderate
system. Beta- and alpha-adrenergic re- chronic dilated cardiomyopathy (48, 49, tenderness, low-grade fever, and leukocy-
ceptor stimulation increases calcium 51). tosis (55). The high occurrence of co-
concentration in the cardiac myocyte, Given the wide range of potentially caine use at the time of blunt abdominal
which causes increased calcium uptake fatal cardiac complications and the prev- trauma compounds the clinical assess-
by the troponin-actin-myosin contractile alence of cocaine use among young ment. The ischemic insult from cocaine
complex. The increase in heart rate and trauma patients, an unexplained cardiac is focal so that the full thickness necrosis
blood pressure as well as cardiac contrac- arrest in an injured or septic hospitalized may be pinpoint, small, and contained by
tility increase cardiac oxygen demand, patient should prompt a drug screen. adjacent viscera (Fig. 1). Thus, explor-
which exceeds the oxygen supply pro- Street drugs are available to postopera- atory laparotomy for suspected bowel
vided by coronary arteries in vasospasm. tive patients through friends and “busi- rupture leads to the diagnosis of focal
Infarction can also result from focal cor- ness” colleagues. Two factors make the full-thickness ischemia, which would
onary artery or diffuse spasm in patients risk of in-hospital illicit drug usage espe- likely have responded to bowel rest and
with coronary atherosclerosis. Patients cially dangerous. First, the friend selects antimicrobials (Fig. 2) (55).
with coronary artery disease have im- the “best” preparation, which is undi- Cocaine-induced acute and subacute
paired release of nitric oxide and prosta- luted. Second, the cardiopulmonary re- ischemic colitis is less common but still
cyclin from the endothelial cells and, serve of the postoperative patient is re- challenging. The endoscopically visual-
consequently, impaired coronary endo- duced. This promotes a cardiac ized lesions are usually segmental and
thelial-mediated vasodilatation. This ex- catastrophe when the patient snorts or include pseudopolyps, ulcers, and focal
acerbates the vasoconstrictive effects of smokes his so-called normal dose. After mucosal hemorrhage, typically confined
cocaine. Chronic cocaine use also accel- resuscitative efforts have failed, a post- to the hindgut in contrast to the classic
erates coronary atherosclerotic disease as mortem drug screen will identify the real form of diffuse ischemic colitis (61). This
seen at autopsy in up to 40% of young culprit and deter subsequent malpractice observation rules out hemorrhagic shock
cocaine users who die of acute myocar- litigation directed toward some lethal and as the precipitating insult. Expectant
dial infarction. Cocaine can also cause cryptic treatment error (52–54). therapy is recommended. When celiot-
direct endothelial injury, which causes Gastrointestinal Complications. The omy is performed for suspected peritoni-
platelet aggregation, thromboxane pro- most common and serious gastrointesti- tis due to hollow viscus rupture, the co-
duction, and coronary artery thrombosis nal complication of cocaine use is acute lon perforation due to cocaine ingestion
as yet another mechanism for myocardial ischemia secondary to intense arterial va- should be excised. Microscopic studies
infarction (48 –50). Cocaine can cause soconstriction through cocaine-induced will confirm the focal nature of the isch-
acute myocarditis, which may be con- catecholamine stimulation of alpha- emic necrosis and perforation (Fig. 3).
fused with myocardial infarction (48, 49). adrenergic receptors in the gastric and Cocaine-induced splenic infarction
Therefore, a hypovolemic or septic pa- mesenteric vessels (55). Gastrointestinal and hemorrhage has also been reported.
tient with cocaine intoxication can ischemia may result in gastroduodenal The infarction results from intense vaso-
present with significant cardiac demand ulceration and perforation usually within spasm; hemorrhage ensues after the va-
and a low-flow-state condition, which can 3 days of cocaine use (8, 55–57). In con- sospasm resolves. Splenic hemorrhage
result in death. trast to peptic ulcer disease, where ulcer- may also occur from arteriolar rupture
The cocaine-induced cardiac arrhyth- ation and perforation present more com- from cocaine-induced hypertension (62).
mias, namely ventricular tachycardia and monly in the duodenal bulb in the 48- to Patients may present with vague and con-
fibrillation, lead to sudden death. This is 65-yr age group, cocaine-induced foregut stant left upper quadrant pain, which is
secondary to increased circulating nor- ulceration and perforation present in more severe than that associated with a
epinephrine and myocardial intracellular younger patients and often occur in the traumatic splenic hematoma. The radio-
calcium. Cocaine can also block fast so- prepyloric region, the pyloric canal, or graphic finding may mimic a traumatic
dium channels, which impairs propaga- the greater curvature of the stomach (8). hematoma. Frank hemorrhage may ne-
tion of an electric impulse and results in Cocaine’s anticholinergic actions pro- cessitate celiotomy expecting to find
conduction block and reentrant arrhyth- duce gastric hypomotility, delayed gastric blunt splenic trauma. The finding of focal
mias. emptying, and prolonged exposure to rupture of the splenic surface without
Cocaine induces ventricular hypertro- gastric acid, thus contributing to ulcer large rents leads the surgeon to suspect a
phy and dilation and subsequent depres- formation. Cocaine also acts directly on cocaine-induced rupture.
sion of left ventricular contractility and the medullary centers that regulate gas- Cocaine-related gastrointestinal com-
relaxation in up to 50% of chronic co- tric motility and vasomotor activity (58). plications are sometimes seen in “body
caine users. This is associated with di- Delayed gastric emptying results in in- packers” or “mules,” who smuggle co-
lated cardiomyopathy from hypertension, creased risk of pulmonary aspiration, par- caine intracorporeally. Body packers
direct toxic effects of high concentrations ticularly in a patient who is sedate or swallow multiple packets of cocaine along
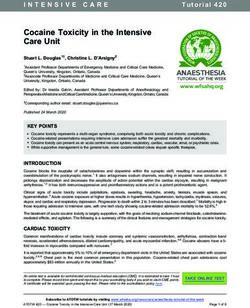
Crit Care Med 2003 Vol. 31, No. 6 1855Figure 4. Aortogram of a patient who had a high-
speed motor vehicle crash while on cocaine
shows bilateral renal artery clots and aortic
thrombosis. He developed renal tubular necrosis
after emergent thrombectomies. From Webber J,
Kline RA, Lucas CE: Aortic thrombosis associated
with cocaine use: Report of two cases. Ann Vasc
Surg 1999; 13:302–304.
Figure 1. Resected small bowel showing pinpoint necrosis at a site of cocaine-induced focal perforation
(arrow), which was walled off by adjacent bowel. Preoperation diagnosis was blunt rupture of bowel
after assault.
sults in focal segmental glomerulosclero-
sis (8).
Renal failure also occurs in about 30%
of patients with cocaine-induced trau-
matic or nontraumatic rhabdomyolysis.
Cocaine induces vasoconstriction of in-
tramuscular arteries, which results in
muscular ischemia, myofibrillar degener-
ation, and acute rhabdomyolysis (67, 68).
Rhabdomyolysis can also result from co-
caine-induced seizures with coma and
compression of a major muscle group
(68). The large amount of free myoglobin
Figure 3. Photomicrograph of perforated sigmoid
colon after a motor vehicle crash shows mucosal
aggravates the renal vasoconstrictive in-
necrosis (long arrow) and submucosal inflamma- sult and causes renal tubular obstruction
tion with thrombosed submucosal blood vessel and decreased glomerular filtration re-
(short arrow). Preoperative diagnosis was blunt sulting in acute renal failure. Patients
rupture of colon (hematoxylin and eosin, ⫻150) present with muscle pain and tenderness,
hyperkalemia, hyperphosphatemia, and
hyperuricemia. Serum creatinine is in-
body packers can be managed with ca- creased, and the extent of rhabdomyolysis
thartics and observation. Surgical inter- is reflected by the high levels of plasma
Figure 2. Photomicrograph shows focal mucosal vention is recommended if the packets creatinine kinase, which may exceed
necrosis (arrow) and underlying submucosal in- fail to clear after 3– 4 days of medical 100,000 untis/L. Tissue thromboplastin
flammation and fibrosis (hematoxylin and eosin, management (63). may be released into the circulation and
⫻40). Renal Complications. Cocaine induces precipitate disseminated intravascular
direct and indirect renal complications. coagulation, which is usually fatal (67).
The direct complications include acute These renal complications can be amelio-
with a constipating agent. Once through renal infarction resulting from renal ar- rated by generous hydration to optimize
customs, they use laxatives or enemas to terial vasospasm and thrombosis caused renal blood flow.
retrieve the packets in the stool. Each by an imbalance between thromboxane Vascular Complications. Cocaine in-
packet contains 3–7 g of cocaine, a fatal and prostacyclin synthesis in the dam- duces small and large vessel occlusion by
dose if a packet ruptures and the cocaine aged renal artery endothelial cells (Fig. 4) both vasospasm and thrombosis with or
is absorbed. The ingested cocaine packets (64, 65). Cocaine-induced renal artery ar- without endothelial cell injury. The re-
may also cause a mechanical bowel ob- teriosclerosis is another mechanism for sult may be focal necrosis or widespread
struction. Once ruptured, the surviving renal infarction and subsequent renal ischemia and infarction depending on the
patient may experience all of the compli- failure (66). Cocaine induces macrophage diameter of the occluded vessel. Chronic
cations of cocaine toxicity, including gi- interleukin-6 production and subsequent cocaine use causes an increase in adven-
ant gastric ulceration. Asymptomatic mesangial cell proliferation, which re- titial mast cells and atherosclerosis of the
1856 Crit Care Med 2003 Vol. 31, No. 6vessels, which predisposes to end-organ mined by the end-organ effects. Mesen- precipitates hemorrhage. Thirty-five per-
ischemia in young patients (69). teric artery occlusion without necrosis, cent of documented cocaine-exposed fe-
Arterial thrombosis is secondary to renal artery occlusion without renal tuses have ultrasonographic evidence of
the cocaine-induced decrease in protein shutdown, and aortic thrombosis without central nervous system cavities, ventric-
C and antithrombin III levels, increase in distal ischemia (Fig. 4) can be treated by ular enlargement, infarction, subarach-
plasminogen activator inhibitor activity, anticoagulation and careful monitoring noid hemorrhage, intraventricular hem-
and increase in platelet activation and in a critical care setting. When end-organ orrhage, or subependymal hemorrhage
aggregation (18, 19, 20). Thrombosis of failure or tissue necrosis is threatened, (77). Cocaine also causes direct intense
large vessels including the aorta has been emergency thrombectomy is needed (70). stimulation of the central nervous system
reported and typically presents within 12 Aortic dissection secondary to cocaine by catecholamines or infarction, through
hrs of cocaine exposure (Fig. 4) (8). When may also occur. The dissection begins cocaine-induced fetal hypertension,
a patient presents with long bone frac- with an intimal tear secondary to a com- which precipitates seizures in the neona-
tures obtained under the influence of co- bination of repeated lateral motion of the tal period (78). Thirty percent of neonates
caine, the clinical picture may be confus- aorta near the beating heart and the he- exposed to cocaine in utero experience
ing. Cocaine-induced rhabdomyolysis of modynamic shear forces of the blood- withdrawal manifested by seizure, leth-
the leg muscles after intramedullary rod- stream enhanced by cocaine-induced hy- argy, feeding problems, hyperactive re-
ding of the ipsilateral femur may be mis- pertension. A subintimal hematoma flexes, vomiting, and diarrhea. Cocaine
taken for direct blunt injury of the leg. forms and propagates as a result of sus- also induces ventricular tachycardia and
The cocaine-induced muscle injury is tained hypertension; this may be a coronary artery spasm with myocardial
more likely to cause a more severe eleva- chronic process. If untreated, the dissec- ischemia in the neonate (8). On follow-
tion of tissue pressure compared with di- tion is likely to rupture (71, 72). The up, cocaine-exposed neonates demon-
rect external trauma. When a patient has clinical syndrome of excruciating sudden strate neurobehavioral deficits and long-
both external injury and cocaine-induced chest pain that is “tearing” or “ripping” term cognitive and developmental delays
injury, the decision regarding fasciotomy may be confused with blunt aortic disrup- (79). These myriad of maternal and fetal
should be based on sequential measure- tion after severe thoracic injury. The goal events create havoc when a woman pre-
ments of tissue pressure. The clinical co- of treatment is control of the hyperten- sents with an acute surgical emergency
nundrum is even more complex when the sion, which becomes easier as the cocaine in the third trimester of pregnancy under
effects of cocaine-induced large-vessel oc- level decreases. Hypotension is an omi- the influence of cocaine. Routine drug
clusion are added (Fig. 5). Thrombec- nous sign and suggests acute aortic re- screens will alert the trauma surgeon and
tomy followed by anticoagulation in this gurgitation with proximal dissection and the obstetrician of the potential for fetal
setting may be limb saving (70). cardiac failure, pericardial tamponade, or distress or sudden expulsion of a poten-
When named intraabdominal arteries myocardial infarction (72). tially viable fetus.
become occluded, the mechanism of ac- Maternal-Fetal and Neonatal Compli- Psychiatric Complications. A comor-
tion is thought to be stasis in the vaso- cations. Das and Laddu (73) reported that bid psychiatric disorder is present in 60%
vasorum leading to intimal injury and 11% of pregnant women are substance to 70% of cocaine users. These abnormal-
platelet aggregation. Treatment is deter- abusers, with cocaine being the favorite ities include mood disorders, bipolar
drug. Cocaine causes direct and indirect manifestation, attention deficit, panic at-
insult to the growing fetus. Cocaine tacks, paranoid ideation, and a behavior
crosses the placenta by simple diffusion pattern that may be conducive to violence
and accumulates in the fetal plasma in and homicidal intent (11). Forty percent
higher than expected concentrations sec- of cocaine and opiate users are likely to
ondary to rapid diffusion, decreased ma- be injured and, when injured, are more
ternal and fetal cholinesterases, which likely to suffer from posttraumatic stress.
metabolize cocaine, and increased norco- Incarceration and expulsion from school
caine synthesis by the pregnant patient are common features of cocaine users.
(14, 74). At the maternal level, cocaine is Cocaine-associated delirium is now better
known to cause spontaneous abortions, recognized. Agitated delirium accounts
abruptio placenta, placenta previa, and for 10% of cocaine deaths. This is seen in
stillbirths (75, 76). Cocaine induces spon- patients with modest cocaine blood levels
taneous abortion by increasing maternal but high levels of benzylecgonine, the
plasma norepinephrine levels, which principal cocaine metabolite. Treatment,
cause uterine contractions through al- when patients survive long enough to
pha- and beta-adrenergic receptor stimu- reach the hospital, is supportive (80 – 83).
lation, constriction of placental vessels, Recognition of cocaine-induced mental
and decrease of fetal blood flow (76). Fe- aberrations is problematic in patients
tal hypoxia leads to intrauterine growth with traumatic brain injury or stroke.
retardation and developmental abnormal- The coexistence of alcohol exposure fur-
Figure 5. Arteriogram showing occlusion of the ities of the brain, heart, great vessels, and ther impairs accurate diagnosis. Psychi-
right profunda femoris artery in a patient with a gastrointestinal and urogenital tracts. Fe- atric evaluation may be necessary for the
right femur fracture after a motor vehicle crash. tal hypoxia also impairs fetal central ner- management of acute mental aberrations
Subsequent rhabdomyolysis led to acute renal vous system autoregulation, which in- and long-term follow-up in drug treat-
failure. creases cerebral blood flow and ment centers.
Crit Care Med 2003 Vol. 31, No. 6 1857cocaine parallel those effects, which are rophage function and cytokine production.
R
seen in the systemic inflammatory re- Am J Respir Crit Care Med 1997; 156:
ecognition of the sponse. Early identification of cocaine in- 1606 –1613
toxication will also identify patients in 17. Baldwin GC, Buckley DM, Roth MD, et al:
signs and symp- Acute activation of circulating polymorpho-
whom treatment with beta blockade, sed-
nuclear neutrophils following in vivo admin-
toms of cocaine atives, or anticonvulsants might be ben- istration of cocaine. Chest 1997; 111:
eficial. 698 –705
toxicity help anticipate the Although reliable data on the effects of 18. Heesch CM, Negus BH, Steiner M, et al:
cocaine on healthcare cost is not avail- Effects of in vivo cocaine administration on
subsequent organ dysfunc- able, the authors believe that the organ human platelet aggregation. Am J Cardiol
tion and implement earlier function changes, which are made worse 1996; 78:237–239
by the presence of cocaine, lead to in- 19. Chokshi SK, Miller G, Rongione A, et al:
organ system support. creased need for critical care beds and a Cocaine and cardiovascular diseases: The
prolonged length of stay. leading age. Cardiology 1989; III:1– 6
20. Moliterno DJ, Lange RA, Gerard RD, et al:
Influence of intranasal cocaine on plasma
REFERENCES constituents associated with endogenous
CONCLUSION thrombosis and thrombolysis. Am J Med
1. Gay GR, Inaba DS, Sheppard CW, et al: Co- 1994; 96:492– 496
Cocaine exposure in trauma patients caine: History, epidemiology, human phar- 21. Fahim I, Ismail M, Osman OH: Hypothermic
and critically ill patients complicates re- macology, and treatment. Clin Toxicol 1975; effect of cocaine in rats. West Afr J Pharma-
suscitation and treatment. A myriad of 8:149 –178 col Drug Res 1975; 2:48 –56
multiple organ toxicities, in the authors’ 2. Christenson EM: Coca, divine plant of the 22. Wicchman BE, Spratto GR: Body tempera-
experience, aggravate the detrimental ef- Incas. Anaesthesia 1946; 2:4 –12 ture response to cocaine and diazepam in
fects of hemorrhagic shock and sepsis, 3. Cohen S: Cocaine. JAMA 1975; 231:74 –75 morphine-treated rats. Pharmacology 1982;
4. Musto DF: A study in cocaine. JAMA 1968; 25:308 –319
leading to higher mortality rate. Recog-
204:125–130 23. Long SF, Davis WM, Waters IW: Additive
nition of these multiple organ sequelae of
5. Schoenberg BS: Coke’s the one: The centen- hypothermic effects of cocaine and nicardi-
cocaine is essential for the treating phy- pine in guinea-pigs. Gen Pharmacol 1994;
nial of the “ideal brain tonic” that became a
sician to provide optimal care and avoid symbol of America. South Med J 1988; 81: 25:1585–1590
otherwise unforeseen complications. 69 –74 24. Maurer HH: Liquid chromatography-mass
Identification of cocaine use can only be 6. Bailey BJ: Looking back at a century of co- spectrometry in forensic and clinical toxicol-
provided by an aggressive approach by caine use and abuse. Laryngoscope 1996; ogy. J Chromatogr B Biomed Sci Appl 1998;
the physician team. This approach should 106:681– 683 713:3–25
include routine questioning of patients 7. Jonnes J: The rise of the modern addict. Am J 25. Kintz P, Samyn N: Use of alternative speci-
about substance utilization and routine Public Health 1995; 85:1157–1162 mens: Drugs of abuse in saliva and doping
toxicology screen at the time of admis- 8. Boghdadi MS, Henning RJ: Cocaine: Patho- agents in hair. Ther Drug Monit 2002; 24:
physiology and clinical toxicology. Heart 239 –246
sion to identify which patients may be at
Lung 1997; 26:466 – 481 26. Dickson PH, Lind A, Studts P, et al: The
risk for these sequelae. A repeat toxicol- routine analysis of breast milk for drugs of
9. Marzuk PM, Tardiff K, Leon AC, et al: Fatal
ogy screen may be utilized in patients injuries after cocaine use as a leading cause abuse in a clinical toxicology laboratory.
who have unusual detrimental effects to of death among young adults in New York J Forensic Sci 1994; 39:207–214
treatment at a time when recovery should city. N Engl J Med 1995; 332:1753–1757 27. Moeller MR, Steinmeyer S, Kraemer T: De-
be clear. Sudden death in the patient who 10. Levy RS, Hebert CK, Munn BG, et al: Drug termination of drugs of abuse in blood.
is improving and is almost ready for dis- and alcohol use in orthopedic trauma pa- J Chromatogr B Biomed Sci Appl 1998; 713:
charge should be suspected of being re- tients: A prospective study. J Orthop Trauma 91–109
lated to the ingestion of cocaine typically 1996; 10:21–27 28. Linder MW, Bosse GM, Henderson MT, et al:
brought in by patient friends. The early 11. Lucas CE, Ledgerwood AM, Kline RA. Alco- Detection of cocaine metabolite in serum
hol and drugs. In: Trauma. Mattox KL, Feli- and urine: Frequency and correlation with
identification of cocaine intoxication
ciano DV, Moore EE (Eds). New York: NY, medical diagnosis. Clin Chim Acta 2000; 295:
should lead the physician to increase the 179 –185
McGraw-Hill, 2000, pp 1059 –1074
level of monitoring for detrimental organ 12. Soderstrom CA, Tandon M, Dischinger PC, et 29. Maurer HH: Systematic toxicological analy-
sequelae, which may be implemented in al. Epidemic increases in cocaine and opiate sis of drugs and their metabolites by gas
an intensive care environment. Earlier use by trauma center patients: Documenta- chromatography-mass spectrometry. J Chro-
identification of organ changes then tion with a large clinical toxicology database. matogr 1992; 580:3– 41
helps facilitate therapy. Consequently, J Trauma 2001;51:557–564. 30. Qureshi AI, Akbar MS, Czander E, et al:
the pragmatic role of early toxicological 13. Tran M: Drugs war is ‘futile exercise.’ Guard- Crack cocaine use and stroke in young pa-
screening clearly affects treatment deci- ian Weekly June 21, 1998, pp 5 tients. Neurology 1997; 48:341–345
sion and will likely lead to improved pa- 14. Hollister LE: Drugs of abuse. In: Basic and 31. Kaufman MJ, Levin JM, Ross MH, et al: Co-
Clinical Pharmacology. Katzung BG (Ed). caine-induced cerebral vasoconstriction de-
tient outcome.
Norwalk, CT, Appleton & Lange, 1992, pp tected in humans with magnetic resonance
Once cocaine intoxication is identi-
437– 449 angiography. JAMA 1998; 279:376 –380
fied, it may be difficult to determine 15. Leshner AI: Molecular mechanisms of co- 32. Gradon JD, Wityk R: Diagnosis of probable
which are the detrimental effects of the caine addiction. N Engl J Med 1996; 335: cocaine-induced cerebral vasculitis by mag-
cocaine as opposed to the organ effects of 128 –129 netic resonance angiography. South Med J
hemorrhagic shock and/or sepsis because 16. Baldwin GC, Tashkin DP, Buckley DM, et al: 1995; 88:1264 –1266
many of the multiple organ effects of Marijuana and cocaine impair alveolar mac- 33. Merkel PA, Koroshetz WJ, Irizarry MC, et al:
1858 Crit Care Med 2003 Vol. 31, No. 6Cocaine-associated cerebral vasculitis. Se- 51. Pitts WR, Vongpatanasin W, Cigarroa JE, et 69. Kolodgie FD, Virmani R, Cornhill F, et al:
min Arthritis Rheum 1995; 25:172–183 al: Effects of the intracoronary infusion of Increase in atherosclerosis and adventitial
34. Aggrawal SK, Williams V, Levine SR, et al: cocaine on left ventricular systolic and dia- mast cells in cocaine abusers: An alternative
Cocaine-associated intracranial hemorrhage: stolic function in humans. Circulation 1998; mechanism of cocaine-associated coronary
Absence of vasculitis in 14 cases. Neurology 97:1270 –1273 vasospasm and thrombosis. J Am Coll Car-
1996; 46:1741–1743 52. Shen WK, Edwards WD, Hammill SC, et al: diol 1991; 17:1553–1560
35. Nolte KB, Brass LM, Fletterick CF: Intracra- Sudden unexpected nontraumatic death in 70. Webber J, Kline RA, Lucas CE: Aortic throm-
nial hemorrhage associated with cocaine 54 young adults: A 30-year population-based bosis associated with cocaine use: Report of
abuse: A prospective autopsy study. Neurol- study. Am J Cardiol 1995; 76:148 –152 two cases. Ann Vasc Surg 1999; 13:302–304
ogy 1996; 46:1291–1296 53. Krome RL, Ledgerwood A, Lucas CE: The 71. Rashid J, Eisenberg MJ, Topol EJ: Cocaine-
36. Dhuna A, Pascual-Leone A, Langendorf F, et hazards of drug addiction on a trauma ward. induced aortic dissection. Am Heart J 1996;
al: Epileptogenic properties of cocaine in hu- Mich Med 1971; 70:603– 605 132:1301–1304
mans. Neurotoxicology. 1991; 12:621– 626. 54. Weicht GT, Bernards CM: Remote cocaine 72. Chang RA, Rossi NF: Intermittent cocaine
37. Cruz R, Davis M, O’Neil H, et al: Pulmonary use as a likely cause of cardiogenic shock use associated with recurrent dissection of
manifestations of inhaled street drugs. Heart after penetrating trauma. Anesthesiology the thoracic and abdominal aorta. Chest
Lung 1998; 27:297–305 1996; 85:933–935 1995; 106:1758 –1762
38. Albertson TE, Walby WF, Derlet RW: Stimu- 55. Herrine SK, Park PK, Wechsler RJ: Acute 73. Das G, Laddu A: Cocaine: Friend or foe? Part
lant-induced pulmonary toxicity. Chest 1995; mesenteric ischemia following intranasal co- I. Int J Clin Pharmacol Ther 1993; 31:
108:1140 –1149 caine use. Dig Dis Sci 1998; 43:586 –589 449 – 455
39. Sousa O, Rowley S: Otorhinolaryngologic 56. Sharma R, Organ CH, Hirvela ER, et al: Clin- 74. Chasnoff IJ, Lewis DE, Griffith DR, et al:
symptoms caused by the intranasal abuse of ical observation of the temporal association Cocaine and pregnancy: Clinical and toxico-
cocaine: Report of a case. Rev Med Panama between crack cocaine and duodenal ulcer logical implications for the neonate. Clin
1994; 19:55– 60 perforation. Am J Surg 1997; 174:629 – 633 Chem 1989; 35:1276 –1278
40. Perper JA, Van Thiel DH: Respiratory com- 57. Lin C, Gabram SG, Roskam SA, et al: Perfo- 75. Macones GA, Sehdev HM, Parry S, et al: The
plications of cocaine abuse. Recent Dev Al- rated peptic ulcer and cocaine use. Contemp association between maternal cocaine use
cohol 1992; 10:363–377 Surg 1999; 54:109 –112 and placenta previa. Am J Obstet Gynecol
41. Underdahl JP, Chiou AG: Preseptal cellulitis 58. Abramson DL, Gertler JP, Lewis T, et al: 1997; 177:1097–1100
and orbital wall destruction secondary to na- Crack-related perforated gastropyloric ulcer. 76. Hurd WW, Betz AL, Dombrowski MP, et al:
sal cocaine abuse. Am J Ophthalmol 1998; J Clin Gastroenterol 1991; 13:17–19 Cocaine augments contractility of the preg-
125:266 –268 59. Mizrahi S, Laor D, Stamler B: Intestinal isch- nant human uterus by both adrenergic and
42. Haim DY, Lippmann ML, Goldberg SK, et al: emia induced by cocaine abuse. Arch Surg nonadrenergic mechanisms. Am J Obstet Gy-
The pulmonary complications of crack co- 1988; 123:394 necol 1998; 178:1077–1081
caine. Chest 1996; 107:233–240 60. Nalbandian H, Sheth N, Dietrich R, et al: 77. Dixon SD, Bejar R: Echoencephalographic
43. Averbach M, Casey KK, Frank E: Near-fatal Intestinal ischemia caused by cocaine inges- findings in neonates associated with mater-
status asthmaticus induced by nasal insuffla- tion: Report of two cases. Surgery 1985; 97: nal cocaine and methamphetamine use: In-
tion of cocaine. South Med J 1996; 89: 374 –376 cidence and clinical correlated. J Pediatr
340 –341 61. Niazi M, Kondru A, Levy J, et al: Spectrum of 1989; 115:770 –778
44. Tashkin DP, Kleerup EC, Koyal SN, et al: ischemic colitis in cocaine users. Dig Dis Sci 78. Singer LT, Yamashita TS, Hawkins S, et al:
Acute effects of inhaled and IV cocaine on 1997; 42:1537–1541 Increased incidence of intraventricular hem-
airway dynamics. Chest 1996; 110:904 –910 62. Homler HJ: Nontraumatic splenic hematoma orrhage and developmental delay in cocaine-
45. Kleerup EC, Wong M, Marques-Magallanes related to cocaine abuse. West J Med 1995; exposed, very low birth weight infants. J Pe-
JA, et al: Acute effects of intravenous cocaine 163:160 –161 diatr 1994; 24:765–771
on pulmonary artery pressure and cardiac 63. Miller JS, Hendren SK, Liscum KR: Giant 79. Singer LT, Arendt R, Minnes S, et al: Cogni-
index in habitual crack smokers. Chest 1997; gastric ulcer in a body packer. J Trauma tive and motor outcomes of cocaine-exposed
111:30 –35 1998; 45:617– 619 infants. JAMA 2002; 287:1952–1960
46. Yakel DL, Eisenberg MJ: Pulmonary artery 64. Kramer RK, Turner RC: Renal infarction as- 80. Morrow CE, Bandstra ES, Anthony JC, et al:
hypertension in chronic intravenous cocaine sociated with cocaine use and latent protein Influence of prenatal cocaine exposure on
users. Am Heart J 1995; 130:398 –399 C deficiency. South Med J 1993; 86: full-term infant neurobehavioral function-
47. Sullivan TR, Pierson DJ: Pneumomediasti- 1436 –1438 ing. Neurotoxicol Teratol 2001; 23:533–544
num after freebase cocaine use. AJR Am J 65. Heng MC, Haberfeld G: Thrombotic phenom- 81. Wetli CV, Mash D, Karch SB: Cocaine-
Roentgenol 1997; 168:84 ena associated with intravenous cocaine. associated agitated delirium and the neuro-
48. Mouhaffel AH, Madu EC, Satmary WA, et al: J Am Acad Dermatol 1987; 16:462– 468 leptic malignant syndrome. Am J Emerg Med
Cardiovascular complications of cocaine. 66. Fogo A, Superdock R, Atkinson JB: Severe 1996; 14:425– 428
Chest 1995; 107:1426 –1434 arteriosclerosis in the kidney of a cocaine 82. Mirchandani HG, Rorke LB, Sekula-Perlman
49. Thadani PV: NIDA conference report on car- addict. Am J Kidney Dis 1992; 20:513–515 A, et al: Cocaine-induced agitated delirium,
diopulmonary complications of “crack” co- 67. Roth D, Alarcon FJ, Fernandez J, et al: Acute forceful struggle, and minor head injury.
caine use. Chest 1996; 110:1072–1076 rhabdomyolysis associated with cocaine in- Am J Forensic Med Pathol 1994; 15:95–99
50. Pitts WR, Lange RA, Cigarroa JE, et al: Co- toxication. N Engl J Med 1988; 319:673– 677 83. Ruttenber AJ, Lawler-Heavner J, Yin M, et al:
caine-induced myocardial ischemia and in- 68. Singhal PC, Rubin B, Peters A, et al: Rhab- Fatal excited delirium following cocaine use:
farction: Pathophysiology, recognition, and domyolysis and acute renal failure associated Epidemiologic findings provide new evidence
management. Prog Cardiovasc Dis 1997; 40: with cocaine abuse. Clin Toxicol 1990; 28: for mechanisms of cocaine toxicity. J Foren-
65–76 321–330 sic Sci 1997; 42:25–31
Crit Care Med 2003 Vol. 31, No. 6 1859You can also read