Current Research into the Diagnosis and Treatment of Canine Degenerative Myelopathy
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Current Research into the Diagnosis and
Treatment of Canine Degenerative
Myelopathy
Submitted for The College of Animal Physiotherapy Diploma in Animal
Physiotherapy
Student identification number: 100513 (Juliet Emery)
31st October 2018
Contents
Acknowledgements .................................................................................................................... 3
Introduction ................................................................................................................................ 4
History, Signalment and Epidemiology ..................................................................................... 5
Causes......................................................................................................................................... 6
Clinical Signs and Symptoms .................................................................................................... 7
Pathophysiology ......................................................................................................................... 9
Diagnosis .................................................................................................................................. 10
Biomarker Study .................................................................................................................. 11
Diffusion Tensor Imaging Study .......................................................................................... 12
Treatment ................................................................................................................................. 14
Physiotherapy ....................................................................................................................... 14
Therapeutic Exercises ...................................................................................................... 15
Treatment Modalities ....................................................................................................... 17
Alternative Therapies ........................................................................................................... 21
Hydrotherapy.................................................................................................................... 21
Acupuncture ..................................................................................................................... 22
Nutrition and Diet................................................................................................................. 23
Comfort Aids ........................................................................................................................ 25
Boots/Socks ...................................................................................................................... 25
Bedding ............................................................................................................................ 26
Movement Aids .................................................................................................................... 27
Assistive Harnesses and Slings ........................................................................................ 27
Wheelchairs and carts....................................................................................................... 28
Home Modifications ............................................................................................................. 29
Indoor Traction ................................................................................................................. 29
Ramps ............................................................................................................................... 29
Supportive Care .................................................................................................................... 29
Case Study ................................................................................................................................ 31
Conclusion................................................................................................................................ 32
Bibliography ............................................................................................................................. 33
References ................................................................................................................................ 34
Appendix 1 ............................................................................................................................... 37
2
Acknowledgements
I would like to thank Fred and Sherry, the tutors and the support staff at The College of Animal
Physiotherapy for their knowledge, patience and positive support during my years of study for
the Postgraduate Diploma in Animal Physiotherapy.
Thanks also go to Peter A. Jenkins, Director of Education and Technology at Spectravet
Therapeutic Lasers, and Chip Godine, Owner/Veterinarian at Ruckersville Animal Hospital,
Virginia USA for their advice regarding therapeutic laser treatment protocols for canine
degenerative myelopathy.
Heather Halton, who I met on my first practical day, has become a valued friend and has never
faltered in her support and encouragement throughout the duration of my studies.
Xanthe Randall has been Dixie’s hydrotherapist for the last 10 years. She is also a wonderful
friend who has encouraged me endlessly, regularly boosted my confidence, looked after Dixie
when I was away on practical days and proof-read all my assignments.
I would like to thank my wonderful parents for their unfailing support in everything I do and
for being proud of even my smallest achievements.
And last, but not least, to my beloved Dixie. You are the brightest light in my life, my sanity
and my inspiration. I am thankful for you every day. This is for you.
3
Introduction
On 25th May 2018 my 12-year-old Golden Retriever, Dixie, was given a presumptive diagnosis
of Degenerative Myelopathy. The news was utterly devastating and I had so many questions
which no one seemed to be able to answer. I decided I wanted to understand everything about
the disease that was slowly going to take her dignity away from her, and her life away from me.
I wanted to know what was happening inside her body and what effect that was going to have
on her physically and mentally. I wanted to find the most recent knowledge from scientific
studies and clinical trials that were aiming to find a cure, a definitive diagnosis and an effective
treatment. Mostly, I wanted to know what I could do to make both our lives easier and happier.
I wasn’t prepared to sit back and let it happen.
Dixie is the reason I wanted to train as a physiotherapist, so I wanted to use the skills she
inspired me to acquire, in order to keep her with me as long as possible. The topic of my final
dissertation was staring me in the face: Current Research into the Diagnosis and Treatment of
Canine Degenerative Myelopathy.
4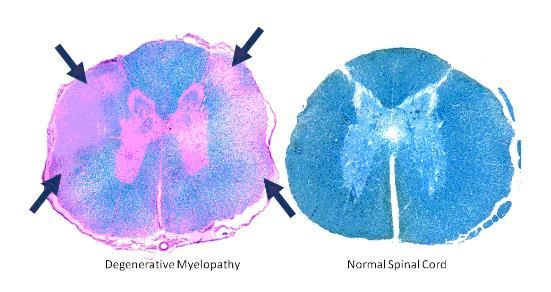
History, Signalment and Epidemiology
Canine Degenerative Myelopathy (DM) was originally described in 1973 as a specific
degenerative neurological disease of the spinal cord affecting dogs, specifically German
Shepherds, presenting with progressive general proprioceptive ataxia and upper motor neuron
(UMN) spastic paresis of the pelvic limbs (Averill, 1973). In 1975, Griffiths and Duncan
published papers describing cases with similar clinical signs but with additional
histopathological features of nerve root involvement. They named the condition chronic
degenerative radiculomelopathy (CDRM). In their case studies, breeds other than German
Shepherds were represented. Further studies have shown that over 43 breeds have been found
to be affected by DM with an overall disease prevalence of 0.19%. In addition to German
Shepherds, Rhodesian Ridgebacks, Pembroke and Cardigan Welsh Corgis, Boxers and
Chesapeake Bay Retrievers seem to be over-represented, although this is not an exhaustive list
(Zink and Van Dyke, 2013).
DM is an adult onset disease, with clinical signs rarely presenting before 8 years of age and
there is no gender predilection (Coates, 2010). The clinical spectrum of the disease has been
broadened beyond the UMN in the spinal cord, as dogs progressing to later stages of the disease
were found to eventually develop lower motor neuron (LMN) paraparesis which leads to the
involvement of the thoracic limbs and the brainstem. There is currently no cure for DM and it
is ultimately fatal. The average survival time from presumptive diagnosis is 6 – 12 months as
many owners elect for euthanasia when their dogs can no longer support their own weight (Zink
and Van Dyke, 2013).
Most rehabilitation practitioners will encounter dogs with DM during the course of their careers.
The disease itself is not painful, but there may be compensatory issues due to altered
biomechanics and overused tissues which may become painful. As the disease affects older
dogs, there are likely to be arthritic changes in joints, so this will present challenges to the
treatment of the primary disease whilst also maintaining comfort for the dog. The dog may
become mentally distressed as the disease progresses due to an inability to carry out normal
maintenance behaviours such as scratching, comfort shifting of the body, urinating and
defecating. Pressure sores and ulcers, and urine scalding may occur secondary to hindlimb
paralysis and must be dealt with by advanced nursing care by the owner. Quality of life for the
dog and the owner must always be a primary consideration.
5
Causes
The cause of DM is still unknown. Research conducted during the 1980s and early 1990s by
Roger Clemmons, Professor of Neurology at the University of Florida, lead him to suspect DM
of being an autoimmune disease. Evidence from recent research would seem to support the
claim that this is an inflammatory autoimmune caused by the dogs own immune systems
attacking the spinal cord. This process creates an accumulation of inflammatory cells and it is
these inflammatory cells over time which result in the degeneration of the myelin sheath leading
to progressive axonal nerve tissue damage and excitotoxicity. If degeneration is very severe,
deficits in the spinal cord lead to an abnormal increase in astrocytes (astrogliosis), causing
sclerotic lesions to form (Marsden, 2015). The damage eventually disrupts nerve signals
resulting in the loss of voluntary and involuntary motor control. Lesions are first noted in the
spinal cord segment T3 to L3, which are supplied by smaller arteries, therefore making it more
susceptible to ischemia and oxidative stress (Pfafman, 2017).
In non-DM affected dogs, an enzyme called super oxide dismutase (SOD) is abundantly present
in the cytoplasm of the central nervous system (CNS) where it scavenges the oxygen free
radicals produced during periods of oxidative stress before they can damage nerve cells. In DM
affected dogs, there is a mutation in this enzyme which results in abnormal folding of the protein
rendering it ineffective. Toxic by-products then accumulate in the axons of the nerve cells
causing destruction of the myelin and increasing the number of reactive astrocytes which causes
scarring and disruption to axonal regeneration, and thus affects the homeostasis of nerve signal
transmission (Coates, 2010).
Since DM appears to have a genetic predisposition, given the disease has a delayed onset, only
affecting dogs approximately 8 years or older, something must precipitate the accumulation of
defective SOD-1 enzymes. Could the inflammation be secondary to mechanical trauma or from
an orthopaedic lesion adjacent to the spinal cord? Could it be associated with other concurrent
conditions such as disc disease? Could this be why the disease always starts in the same region
of the spine? In the dog, the ratio between the spinal cord and the vertebral foramen increases
in the thoracic spinal column, which could imply a greater potential risk for micro-trauma and
cord impingement (Marsden, 2015). These questions are yet to be answered.
6
Clinical Signs and Symptoms
Symptoms of DM can be divided into two distinct phases depending on whether it is just the
Upper Motor Neuron (Early disease) which is affected, or whether the disease has progressed
to include both the Upper and Lower Motor Neurons (Late disease) (See Table 1). Symptoms
start gradually but often owners will seek veterinary assistance during the early phase of the
disease when there is a noticeable deficit to the functioning of the pelvic limbs. Affected dogs
will present with a swaying, or staggering spastic/long-strided hind limb gait, often
accompanied by scuffing and dragging of the rear limbs. The two middle toenails may show
signs of abnormal wear. Initially, this tends to be worse on one side but will eventually progress
to both hind limbs (Millis and Levine, 2014). The dog may have difficulty rising from a down
position, walking, running and jumping. The tail may become limp, and owners may notice
their dogs knuckling over onto the dorsal aspect of their hind paws where sores may have
developed. They will likely fail a dorsiflexion neurological test performed by the vet where
they are unable to correct a postural challenge due to loss of conscious proprioception (Figure
1). Full pelvic paralysis usually occurs within 6 – 12 months of diagnosis.
Figure 1: Knuckling onto dorsal aspect of the hind paw
As the disease progresses to affect the Lower Motor Neuron, the dog will likely show signs of
ataxia in the forelimbs, which, as with the hind legs, if allowed to progress, will eventually also
become completely paralysed. There will be widespread muscle atrophy due to disuse as well
as denervation. When all 4 legs are affected, the animal will be considered tetraplegic and will
be non-ambulatory. There will be associated urinary and/or faecal incontinence of varying
degrees which may cause urine scalding. The dog will be totally reliant on the owner for
comfort shifting and may develop bed sores and skin ulcers (Zink and Van Dyke, 2013).
Brainstem involvement may leave the dog with inability to bark, swallow and cough, also
known as dysphagia (Millis and Levine, 2015).
7
Table 1: Classification scheme for disease stages of degenerative myelopathy.
Stage of
Neurological Signs Symptoms
Disease
Upper Motor Neuron (UMN) affected
1 Asymmetric, general Rear limb weakness and muscle loss,
proprioceptive ataxia and decreased co-ordination, loss of balance,
spastic paresis in pelvic difficulty with positional changes, climb
limbs. Loss of conscious stairs, jump into the car or onto furniture.
proprioception.
2 Non-ambulatory Limp tail, crossing of hindlimbs under the
paraparesis, paraplegia. body (“drunken gait”), rear leg drag.
Pelvic limb muscle atrophy Unusual toe nail wear. May progress to
+/- urinary/faecal dragging themselves with the front limbs
incontinence. due to loss of mobility in the rear. Faecal
and/or urinary incontinence may occur. Bark
may be hoarse. Urinary tract infections may
occur, pressure sores may develop. Anxiety
increases. Twitching of rear limbs as
misfiring of nerves occur.
Lower Motor Neuron (LMN) affected
3 Flaccid paraplegia, thoracic Weakness advances through the core
limb paresis. Severe pelvic muscles and then affects the front limbs.
limb muscle atrophy. Muscle mass loss to the shoulders. Dog will
Urinary/faecal incontinence. eventually be unable to stand or walk, and
may also be unable to remain in sternal
recumbency without assistance. Pressure
sores, systemic infections, urinary tract
infections due to urine retention.
4 Flaccid tetraplegia. Severe Disease progresses to the brain stem and the
generalised muscle atrophy. cranial nerves which may affect vital organs
Urinary/faecal incontinence. such as the diaphragm and intercostals –
Dysphagia, dysphonia, asphyxiation may occur. May lead to
respiratory difficulty. multisystem failure including kidney, lung
and heart. Euthanasia should be considered
prior to this stage if the animal is distressed.
8
Pathophysiology
Histopathological studies of spinal sections of dogs that have died of DM, have shown notable
degenerative changes in the white matter, including nerve fibre loss of ascending sensory and
descending motor pathways as a result of axonal degeneration and secondary demyelination
(See Figures 2 and 3). The area’s most severely affected include the mid- to caudal thoracic
spinal cord segments (T3 – L3) (Coates and Wininger, 2010). There is an associated
proliferation of reactive astrocytes which leads to the formation of sclerotic lesions and scar
tissue formation in the myelin sheath of all spinal cord funiculi (axon bundles) but this is
consistently more severe in the dorsal horn of the spinal cord at the mid- to lower thoracic
region (Zink and Van Dyke, 2013). The scar tissue inhibits axon regeneration.
The degeneration of the spinal cord tissue is caused by the action of excessive amounts of
damaging reactive oxygen species (ROS) molecules leading to a chronic inflammatory state.
Neuronal cell body degeneration is rarely noted in the ventral horn.
Figure 2: Section of spinal cord from a
dog that died of DM (left) compared to a
section from the spinal cord of a normal
dog (right). Axonal degeneration in the
white matter is seen as a loss of the blue
colour at the edges of the cord (arrows).
Image from: https://www.holisticpetcentre.com/rehab-medical-conditions/degenerative-myelopathy-pets-dogs-
cats/
Figure 3: Spinal cord histopathology
A – thoracic cord cross-section from
DM-affected 13 yo Pembroke Welsh
Corgi
B - Unaffected 13 yo Labrador
retriever. (Awano, 2008).
Image from: http://www.pnas.org/content/pnas/106/8/2794.full.pdf
9
Originally, neurologists compared DM in dogs to Multiple Sclerosis in humans as this too is an
autoimmune disease where parts of the nervous system are recognised as foreign leading to
progressive deterioration of the spinal cord and ultimately results in paralysis. Latterly, genetic
studies have shown that DM is more closely related to the rarer disease familial amyotrophic
lateral sclerosis (ALS) due to the presence of SOD-1 mutations (Awano et al., 2009). Human
ALS, also known as Lou Gehrig’s disease, has an almost identical clinical presentation as an
adult onset fatal paralytic neurodegenerative disease with both upper and lower motor neuron
involvement.
In 2009, Awano et al., sequenced the SOD1 gene in normal and DM affected dogs which
revealed a G to A nucleotide transition, resulting in an E40K missense mutation (Zink and Van
Dyke, 2013). In 2011, Wininger et al., discovered another point mutation in the SOD1 gene; an
A to T nucleotide transition specific to Bernese Mountain Dogs (Kobatake et al., 2017). The
mutation alters the tertiary structure of the SOD protein causing a conformational change,
altering its three-dimensional shape and therefore inhibiting its biological function. The
mutation renders the superoxide dismutase enzyme ineffective at scavenging oxygen free
radicals leading to an accumulation of ROS which results in a chronic state of inflammation.
Additionally, the substrate of the enzyme may be altered leading to the accumulation of toxic
by-products in the axons of the nerve cells in the white matter of the spinal cord thereby causing
degeneration and demyelination as detailed above. This progressive disruption of nerve fibres
that transmit movement commands from the brain to the limbs and then the sensory feedback
from the limbs to the brain, results in the classic symptoms seen in DM and ALS. (Marsden,
2015).
Diagnosis
True diagnosis can only be determined post-mortem by histology of a cross section of the spinal
cord. Currently, DM can only be diagnosed in living animals by elimination of other similarly
presenting diseases based on a lack of clinically relevant compressive myelopathy (Coates and
Wininger, 2010). Other diseases that may mimic the signs and symptoms of DM, include
intervertebral disc disease (IVDD), myelitis, degenerative lumbosacral stenosis, spinal cord
neoplasia (tumour), hip dysplasia and certain parasitic diseases which also cause inflammation
of the spinal cord (Millis and Levine, 2014). These other causes of hind limb weakness must
10be excluded before reaching a presumptive diagnosis of DM, but this can be difficult as some
of them may be concurrent.
A number of investigative procedures can be used to exclude other diseases which have a
similar presentation. Advanced imaging procedures such as electromyography, myelography,
nerve conduction studies, computed tomography (CT) scans and magnetic resonance imaging
(MRI) may be used alone or in combination to rule out other diseases or injury. Disc protrusions
may be present, not necessarily because of IVDD, but as a result of weakness and stresses in
the spine during DM disease progression, and this may confound diagnosis. Conversely, the
position of the dog during the process of imaging can sometimes hide disc protrusions and lead
to a false positive. X-Rays of the chest and thoracolumbar regions of the spine can be used to
screen for primary or metastatic cancerous tumours in close proximity to the spinal cord which
may contribute to the symptoms.
Cerebrospinal fluid (CSF) samples may be collected from a spinal tap and analysed for evidence
of inflammation. Parasitic infections can be diagnosed from CSF panels, however elevated
levels of protein segments in the absence of any parasites may be indicative of DM (Goran,
2010). Blood and urine samples to assess red blood cell cell count, serum chemistry panel,
thyroid panel and urinalysis can indicate other causes of hind limb weakness, but results will
be unremarkable in a dog with DM.
As mentioned previously, genome wide association analysis reveals a SOD-1 mutation in
canine degenerative myelopathy that resembles amyotrophic lateral sclerosis in humans (Coates
et al., 2009). A DNA test for the SOD-1 mutation was developed at the University of Missouri-
Columbia which can identify dogs as either normal (N/N), a carrier of the disease (SOD-1/N),
or those at high risk of developing the disease (SOD-1/SOD-1). About 60% of dogs with two
mutated copies of the gene will go on to develop the disease, whilst the remaining 40% will
not. This means there are other factors at play, in addition to the SOD-1 mutation, that leads to
the clinical development of DM in dogs (Zeng et al., 2014).
Biomarker Study
Recent studies into diagnosing DM have centred around the identification of a biomarker
specific to DM in order to aid early intervention and facilitate appropriate patient management.
In 2017, Toedebusch et al. produced a paper identifying phosphorylated neurofilament heavy
11(pNF-H) as a possible fluid biomarker for canine DM. The protein pNF-H is an abundant
structural protein of myelinated motor axons and can be detected in disease states where axonal
injury is indicated. Increasing levels of this protein in blood serum and cerebrospinal fluid
(CSF) have been shown to have a high correlation with disease progression in human patients
with ALS.
They showed that the biomarker pNF-H was increased in the CSF samples of DM-affected dogs
at all disease stages compared to age-matched control groups, but was not increased in blood
serum. There was no significant difference in the concentration of pNF-H at each of the
different stages of disease progression, therefore levels do not correlate with increasing axonal
degeneration and cannot be used as a measure of axonal damage (Figure 4). Finally, the control
group of ‘mimic’ diseases showed no difference between CSF pNF-H concentrations in DM
dogs versus those with other primary axonal diseases. However, it is still a promising
antemortem diagnostic tool for DM and further study is required (Toedebusch et al., 2017).
Figure 4: pNF-H is increased in CSF of DM-
affected dogs compared with control dogs at all
disease stages (Toedebusch et al., 2017)
Diffusion Tensor Imaging Study
Non-invasive imaging is essential in the management of spinal cord injury. Although
veterinarians regularly use conventional clinical magnetic resonance imaging (MRI) to rule out
‘mimic’ diseases in suspected cases of degenerative myelopathy, the spinal cord lesions
themselves are undetectable and therefore limit the ability to diagnose and monitor the disease
(Hendrix et al., 2015). Diffusion Tensor Imaging (DTI) is an alternative MRI technique that
measures the size and direction of the diffusion of water molecules through various tissues
(Vedantam et al., 2014). In nerve fibres the cell membrane and myelin sheath provide a
12biological barrier to perpendicular diffusion of water molecules instead directing them along
the axon bundles longitudinal axis, therefore DTI can be used to visualise white matter tracts
and can infer the orientation of surrounding axonal fibres (Hendrix et al., 2015).
Quantitative measurements relating to DTI within the spinal cord can provide an assessment of
neural damage in various spinal cord pathologies with a high level of correlation to histological
and functional observations (Figure 5). More data is required, and scanning protocols and
imaging processing need to be further refined and standardised, however, this is a promising
scanning technique for diagnosis and monitoring of patients with spinal cord disease.
(Vedantam et al., 2014)
Figure 5: A human patient with severe myelopathy.
Panel C - conventional MRI was suggestive of only mild
myelopathy. Panel D – DTI shows almost complete loss of fibres at
C5/6 correlating with the patient’s clinical presentation (Hendrix et
al., 2015).
Studies of people with ALS have shown that DTI is able to detect the microscopic changes in
the spinal cord caused by this condition. In August 2017, Dr. Philippa Johnson, an American
Veterinary Surgeon at Cornell University, started a comparative clinical trial with the aim of
determining if DTI is able to detect the spinal cord lesions caused by degenerative myelopathy.
She recruited two groups of dogs: 1) Dogs with a positive SOD-1 test for degenerative
myelopathy that are showing clinical signs consistent with degenerative myelopathy and 2)
Dogs with a normal neurological examination that are over the age of 8 years.
This project aims to determine if this technique is able to identify the spinal cord lesions caused
by DM by comparing imaging results from a group of dogs with the condition with a normal
group. Dr. Johnson hypothesises that DTI can detect white matter lesions, and the extent of the
lesions correlates to the neurological status in DM dogs at the time of imaging. DTI has the
potential to become a non-invasive and reliable imaging method for the diagnosis and
monitoring of degenerative myelopathy. In addition, the ability to track lesion load and location
over time would be a valuable tool to assess response to treatment trials currently being
13undertaken with SOD1 mutant mice aiming to terminate neurological deterioration (Johnson,
2017). Results are pending as the data collection process for the study was due to be concluded
August 2018.
Treatment
Physiotherapy
Managing the symptoms of DM includes ensuring the nervous system is constantly stimulated
to keep the nerve impulses firing. This should prolong the length mobility of the dog. The best-
known treatment to achieve this aim, based on the outcome of a number of case studies, is for
the animal to undergo physiotherapy.
In 2006, Kathmann et al. produced survival data from a study of 22 DM affected dogs that
received varying degrees of physiotherapy. There were three treatment groups in the study:
1. Intensive physiotherapy group (n=9).
• 5 – 20 minutes active gait exercise, 3-5x/day AND
• Massage or Passive ROM, 3x/day OR
• Hydrotherapy daily
2. Moderate physiotherapy group (n=6)
• 5 – 20 minutes active gait exercise, max. 3x/day AND
• Massage 1x/week OR
• Hydrotherapy 1 x/week
3. No physiotherapy group (n=7)
Active exercises were modified depending on the dog’s neurological status, with slings or other
supports used as necessary. The results showed that the dogs in the intensive physiotherapy
group had longer mean survival times (225 days) compared to those on the moderate treatment
plan (130 days) and those on the no treatment plan (55 days) (Kathmann et al., 2006).
Although the study by Kathmann et al., 2006 would imply that physiotherapy has a beneficial
effect on prolonging the survival time of dogs with a presumptive diagnosis of DM, it did not
consider the disease stage or UMN/LMN signs. It also had other limitations such as lack of
randomisation, definitive diagnosis, small group size and owner bias. However, it does warrant
further investigation into the efficacy of disease stage appropriate therapeutic exercises, whilst
14being mindful of not over-exerting these dogs who tire very easily. Over-exertion in many
situations can be counter-productive (Zink and Van Dyke, 2013).
It is clear that physiotherapy has a vital role in the treatment of DM in order to maintain
functional movement in the animal and delay the progression of the disease. Given the poor
prognosis, physiotherapy can also improve the psychological impact on the dog and owner
alike, enhancing the quality of life for the patient and giving the owner a sense of actively
delaying the loss of mobility. Owner support is vital as the dog will become more and more
reliant on them and anxiety may increase as the disease stages progress. Functionally, the aims
of physiotherapy would include:
• Maintaining muscle mass and nerve stimulation
• Maintaining mobility, movement, postural strength and gait patterns
• Prevent tightening of soft tissues such as tendons, muscles and ligaments
• Enhance balance and co-ordination
• Prevent injury that might occur as a result of existing issues
Therapeutic Exercises
One of the known mental and physical stressors for dogs with DM is over-exertion, therefore a
therapeutic exercise program should always begin slowly and at low level and then be modified
regularly by constantly assessing progress and mental state. Ideally, the exercise program
should start while the dogs are still ambulatory, but this is not always possible due to the
difficult nature of diagnosis.
Active exercises should include a variety of core strengthening techniques which will improve
quality of life by targeting trunk musculature (thoracic limb and pelvic stabilisers, vertebral
column stabilising muscles, abdominals) and improving overall movement efficiency. As the
disease progresses, strong core muscles will also aid respiratory movements. Some exercises to
improve core strength include:
• Figure-of-eight around cones.
• Weight shifting (balance pads, wobble cushions) – all 4 legs up
• Rhythmic stabilisations (360°)
• Stepping over Cavaletti rails
15• Sit-stand-sit positional changes
• Stair climbing, incline work
Active and Passive Range of Motion (ROM) exercises will stretch muscle groups in the limbs
in a functional movement pattern therefore aiding efficiency of gait. Spinal flexors and shoulder
flexors will be affected and will restrict movement. Encouraging the stretching of the soft
tissues by focussing on hip extension, spinal extension and shoulder extension will greatly
improve prospects and delay the loss of mobility. It will also help break down ligamentous
calcification that promotes spondylosis and rigidity in the spine. Exercises to improve ROM
include:
• Stepping over Cavaletti rails
• Stair climbing, incline work
• Give-a-paw, extend elbow
• Bowing (elbows extended), forelimb raised, hind limb raised,
• Luring with a treat side-to-side and down between front legs.
Balance and proprioception will be negatively affected by the degeneration of the nerve
impulses, therefore exercises which include increasing the length of time the dog can hold a
standing balance will be beneficial. Offering support by use of a body harness to extend the
amount of time will also encourage improved balance. Encouraging proprioceptive stimulation
can be achieved with light touching, wraps, or gentle tapping of the muscles which will increase
sensory input to the limbs. Exercises to improve balance and proprioception include:
• Stepping over Cavaletti rails
• Weight shifting on balance pads/wobble cushions - forelimbs elevated
• Walking on different surfaces/textures (stones, sand, grass, water etc.)
• Drop-sticks/Obstacle Course
• Lateral stepping
Strengthening and endurance exercises should be modified according to the dog’s baseline
ability. Functional analysis includes ability to walk and efficiency of transitions between
positions.
16Massage will aid circulation, helping to remove toxic inflammatory mediators, which can build
up in the muscles, and therefore will assist maintenance of muscle tone. The increased
circulation will also improve production of white blood cells which will boost the immune
system and decrease cortisol levels reducing stress levels and relaxing the dog.
Treatment Modalities
A physiotherapist will have access to a selection of treatment modalities which can complement
a therapeutic exercise program and benefit the functional aims of treatment. As previously
mentioned, although the degeneration of nerve impulses is not painful in itself, it is
presumptuous to say that some dogs with DM do not suffer pain. Ageing dogs are likely to have
other disease processes which may be painful and exacerbated by lack of co-ordination. There
will also be compensatory effects and concurrent diseases, which may cause some level of pain.
A physiotherapist will be able to identify these areas through massage and palpation techniques.
• Electrotherapy
Electrotherapy involves passing low to medium levels of electrical current through the body in
order to reverse atrophy, improve muscle function and reduce pain signals. At the cellular level,
electrotherapy causes local nerve cell excitation and changes cell membrane permeability which
will stimulate protein synthesis, osteosynthesis and fibroblast formation (Millis, 2017). At the
tissue level, increasing muscular strength by stimulating skeletal muscles can be achieved with
the use of a Neuromuscular Electrical Stimulation (NMES) machine. The device can be used
to stimulate muscle contraction and hence improve muscle bulk and strength by emitting
electrical impulses and stimulating the local motor nerve without the involvement of the central
nervous system (CNS). This device can therefore help reduce the rate of muscle atrophy as a
result of the dog’s inability to actively move their own body. Through the stimulated movement,
the muscle contractions will also result in improved joint mobility as well as circulatory and
lymphatic drainage. Care must be taken to provide an almost imperceptible contraction strength
at the outset, and increase it slowly only when the animal is comfortable and aware of the
procedure so as not to cause any anxiety.
17• Therapeutic Laser Therapy
Photobiomodulation (PMB) is the use of therapeutic lasers in medical treatment, and is intended
to describe the modulation of cellular processes in the body as a result of the application of light
therapy. Class 3 therapeutic lasers emit low power (10mW – 500mW) radiation via photons of
light with wavelengths in the red to near infrared region of the spectrum (660nm – 905nm)
without emitting any heat (non-thermal mechanism). These wavelengths are able to penetrate
the skin to different depths and therefore affect various soft and hard tissue types (Cotler et al.,
2015). These energised cells then have further downstream tissue effects such as pain
modulation, increased local microcirculation for tissue healing and regeneration, stimulation of
the immune system and reduction of the inflammatory process. Depending on the chosen
parameters, PBM can have stimulatory or inhibitory effect on biochemical processes (Downing,
2017).
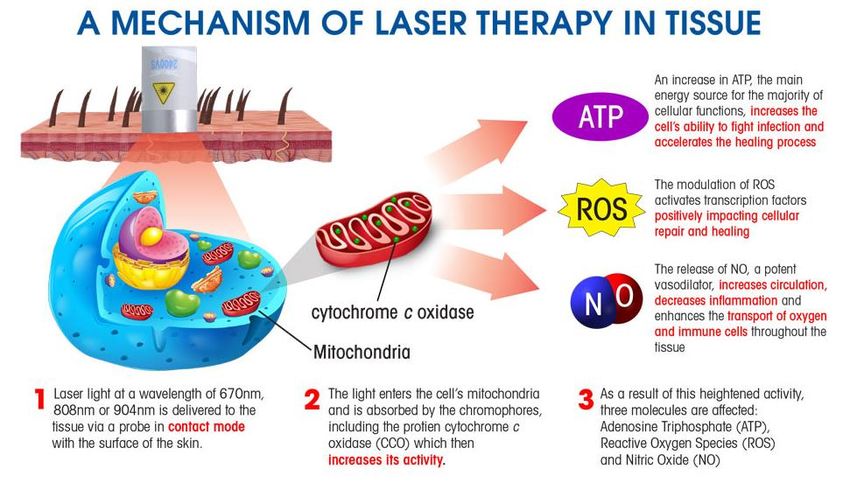
Biochemical processes are powered by mitochondria, which are the “energy centres” of the cell.
They convert nutrients and oxygen, via a series of chemical reactions, into molecules of energy
(ATP) by a process known as oxidative phosphorylation, or cellular respiration. One of the key
elements of this process, an enzyme called cytochrome c oxidase (CCO), is also a chromophore
and can be activated by photons of light. CCO is the primary photo receptor for red and near
infrared wavelengths of light (Cotler et al., 2015).
In stressed or ischaemic tissues, the level of nitric oxide (NO) increases and can inhibit cellular
respiration by binding to CCO. Unregulated NO production can cause cell death through
oxidative stress, disrupted energy metabolism and DNA damage. This leads to an increase in
the production of reactive oxygen species (ROS) which leads to inflammation. The absorption
of the red and near infrared light photons by CCO, causes NO to dissociate and allows oxygen
back into the electron transport chain, thereby increasing the cellular production of ATP and
reducing ROS. (Hamblin, 2016) (See Figure 6)
18Figure 6: https://eriksenchiropracticlaser.com/storage/app/media/laser_diagram.jpg
Myelin-rich white matter in the nervous system is one of the most sensitive tissues to oxidative
damage in the body – the exact pathology seen in dogs with DM. With these facts, the
application of laser therapy should have a positive effect on dogs with DM. PBM has been used
in a number of studies relating to surgical nerve repair, and it has been shown to support nerve
regeneration, re-innervation of denervated muscle, and functional recovery following
peripheral nerve injury (Anders et al., 2014). A study in 2013 by Anders et al., demonstrated
an increase in neurological activity and angiogenesis on day 14 following a surgically induced
nerve injury treated with a PBM protocol, compared to non-treated controls.
The benefits of PBM include reduction of pain and inflammation, potential nerve regeneration,
increased local circulation and increased axonal growth. This stimulation of neural pathways
should be beneficial for a dog with DM to improve their functional and ambulatory status, and
the reduction of pain and inflammation should ease concurrent and compensatory issues given
the goal to prolong and improve quality of life of the dog. Although there have been some
studies involving mechanical spinal cord damage, there are currently no clinical trials involving
the use of PBM in the treatment of neurodegenerative conditions in a dog, however, as DM is
a naturally occurring canine model of human ALS, anecdotal evidence may lead to funding a
study in the future.
19In August 2018, there was a presentation by Debbie Torraca at the IAVRPT (International
Association for Veterinary Rehabilitation and Physical Therapy) Rehab Summit where she
reported some benefit to the use of PBM in conjunction with a structured therapeutic exercise
protocol for 24 dogs. At the time of the report, 22 out of the 24 dogs had continued past 12
months, although some were in a cart. The PBM protocol used dosages of 20 – 30 Joules/cm2
“applied to anatomical localised region, and epaxial located in the region”, with most
anatomical regions being “T3 – L3 and L3 – S3”. However, there was no mention of the size
of area treated, the duration of treatment, or the total dose delivered during each treatment
session.
Leading manufacturers of Class 3 and Class 4 lasers are developing some speculative treatment
protocols for various diseases and conditions derived from clinical case reports.
• Spectravet Therapeutic Lasers: Dr. Chip Godine, a US veterinary surgeon and
specialist laser consultant for Spectravet, suggested that he has not seen any positive
benefits to the use of PBM thus far. His theory has been to treat the spinal cord from
mid thoracic area to L4 – L5 using the 810nm-multi-500mW (x4) probe, pulsed at 10Hz
for 80 seconds aimed at 45 degrees to the right and left intervertebral foramen. This
should provide a dose of ~ 3J/cm2 at a depth of 2.5 cm from the skin surface at a
frequency of 3x/week until a clinical effect is seen then can be reduced accordingly
(personal communication, 2018).
• Thor Lasers: A protocol designed by Thor laser systems uses their superficial 69 diode
LED cluster probe (660 and 850nm) giving a total power 1390mW and a dose of
44.6mW/cm. They suggest timings of 1 minute/area with a pulse rate of 2.5Hz. Treat
left and right Paraspinals from C4 – S3, the major muscle groups of hind legs and
pudenal nerve area (See Figure 7).
Figure 7: Green circle indicates
placement of probe. © Thor
20It is clear there is much work to be done with this treatment option regarding appropriate
treatment location on the body, treatment timings, probe power and accurately measuring the
depth of photon penetration into different tissue types. The treatment doses prescribed above
are in differing units so there needs to be a standardised international dose unit so the results of
case studies and clinical trials can be compared accurately.
Alternative Therapies
Treating DM can be improved by using a multi-modal approach involving a variety of
rehabilitation professionals including hydrotherapy, acupuncture and dietary amendments, in
conjunction with a regular physiotherapy regime. This will help delay the progression of the
disease by keeping the dog mobile for longer and reducing physiological and psychological
stresses.
Hydrotherapy
Hydrotherapy is an excellent form of rehabilitation for dogs with DM. The effects and physical
properties of water, such as density, hydrostatic pressure and buoyancy will benefit the physical
constraints of the condition supporting the weight of the animal and providing low joint impact
during movement to exercise weakened areas of the body. The hydrostatic pressure and
therapeutic temperature of the water stimulates metabolic and neuromuscular systems as well
as decreasing pain and oedema therefore allowing a greater range of joint and muscle motion.
Hydrotherapy is good for any stage of the disease and can be carried out in an underwater
treadmill or in a pool, depending on the stage of the disease. In the early stages of the disease,
while the dog is still able to support its own body weight, a treadmill can be used to encourage
appropriate gait movement. It is best to begin with standing exercises with the water at the level
of the greater trochanter (decreases weight bearing by 73%). Once the dog is comfortable with
standing, progression to slow walking will help maintain muscle strength and joint range of
motion.
Hydrotherapy also provides dogs with mental stimulation, and a sense of freedom and purpose.
The progression of DM can be very distressing for the dog as they are unable to move and
defend themselves, which in turn can make them anxious, depressed and bored. The freedom
21of moving in water where it is not physically possible on land is hugely beneficial for their
mental wellbeing. It has been reported in some cases that dogs have independently moved
paralysed legs in a hydrotherapy pool! Frequency of hydrotherapy sessions does not have to be
limited except by the fatigue level of the dog.
In conjunction with Hydrotherapy, Ozone Hydro-Massage Therapy in a canine spa has also
shown to be beneficial to dogs with DM. The Ozone has a strong anti-bacterial function and
can help alleviate itching, and other skin conditions which may be concurrent. The tiny and
powerful bubbles and their rhymical impact delivers a full body massage helping to stimulate
and activate body tissues. This relieves tension and fatigue and encourages the production of
red and white blood cells helping to clear inflammatory mediators from stressed muscles. It is
difficult to groom dogs with DM, so the spa has the added benefit of loosening grease and dirt
from the skin as well as loose hairs. Capillaries in the skin are dilated with the warmth of the
water, bringing nourishment to the surface of the skin therefore allowing it to breathe better and
enhancing healing of abrasions and bed sores.
Acupuncture
Acupuncture is one branch of Traditional Chinese Medicine (TCM) that has been used for
thousands of years for the treatment of pain and neurological issues. It has only been since the
1970s that this form of medicine has gained popularity in Western Culture, both clinically and
in research. Acupuncture treatment involves stimulating specific pressure points on the surface
of the body by inserting long, hair thin needles, resulting in a therapeutic or homeostatic effect.
The aim is to ‘realign’ Qi (energy) allowing it to flow harmoniously, which can be equated in
Western practice to stimulation of the parasympathetic and sympathetic components of the
autonomic nervous system. Modern studies have determined that acupuncture points are located
in areas of sensitive neuro-immune modulation, where there is a high density of immune
mediated mast cells, lymphatic vessels and an increased ratio of myelinated nerve fibres
(Roynard et al., 2017).
There are no specific studies using acupuncture in cases of degenerative myelopathy, but there
have been some small randomised trials involving other spinal cord myelopathies with positive
results. A study of acupuncture treatment in rats with spinal cord injuries showed a significantly
improved functional recovery compared to the placebo control groups (Figure 8). The affected
22group also had a significant reduction in the expression of inflammatory mediators, offering
increased neuroprotection and reducing neuronal cell death and axonal loss (Choi et al., 2010).
Figure 8: Representative footprints obtained from each group of rats with spinal cord
injury at 35 days after SCI. The control group of rats dragged their hind limbs. The
group receiving acupuncture showed advanced functional recovery (Choi et al., 2010).
Nutrition and Diet
In the 1990s a treatment protocol for DM was formulated by a veterinary neurologist Roger
Clemmons, and is known as The Clemmons Protocol. It was formulated around a diet designed
to counter immune-mediated damage as well as a structured and regular exercise program. The
diet centred around unprocessed food with supplements which included sustained use of anti-
oxidants, fibrinolytics and prednisone as and when required. The latter two aimed to limit
inflammation of the cord itself (Marsden, 2015). An independent study testing the supplement
regime in the absence of the diet and physiotherapy showed no improvement in the survival
time of dogs with DM (Pfafman, 2017).
Diet should focus on feeding unprocessed foods as they are naturally higher in anti-oxidants
and will limit oxidative stress in the spinal cord, control acute and chronic inflammation and
help regulate the immune system. Starchy food, as is found in most dog kibble feed, increases
insulin levels and can promote inflammatory cytokine production. This reduces the
bioavailability of nitric oxide (NO) which is a key molecule involved in the resolution of
inflammation. Ongoing inflammation promotes oxidative stress which exacerbates and
accelerates the disease (Pfafman, 2017).
Polyunsaturated fatty acids are one of the most effective anti-inflammatories which should be
included in the diet as they are not produced by the body. The most important is Omega-3 and
it can be found in fish oils. Other antioxidants beneficial to DM affected dogs include vitamin
23C, vitamin E, vitamin A, carotenoids, selenium, coenzyme Q10 and taurine. Most of these can
be found in fresh fruit and vegetables (Mayer, 2018).
There are some plant extracts which have been shown to protect the spinal cord from
inflammation, these include:
o Bupleurum which helps to moderate white blood cell movement into the
interstitial space of the spinal cord and reduces production of key inflammatory
cytokines.
o Curcumin (found in Turmeric) which inhibits the production of inflammatory
cytokines in the spinal cord and inhibits destruction of damaged tissues and
gliosis (a pathological process in the CNS).
o Milk Thistle which is also a powerful antioxidant and inhibits gliosis (Marsden,
2015.
A canine nutritionist will be able to design a bespoke diet based on the requirement for a low
glycaemic index, high levels of anti-oxidants, and foods with effective anti-inflammatory
properties. With frequent consultation, they will also be able to modify the diet to account for
the diminishing energy requirements of the dog as it starts to lose active mobility and therefore
moderating their weight. This would be an additional benefit to avoid physical and
physiological stress.
Physiotherapy is the most successful and proactive treatment currently available to improve the
quality of life for dogs with DM. Not only is it important for the physical and psychological
welfare of the dog, but also a valuable source of information and support for the owner. A
physiotherapist will be able to advise on alternative treatments to accompany physiotherapy in
a multi-practitioner approach to managing the condition. Although a generalised treatment plan
for physiotherapy and alternative therapies can be devised (See Appendix 1), all dogs are
different and will respond differently to intervention. It is important to modify the plan for each
individual dog as the disease advances, therefore frequent assessment of progress is necessary.
Physiological and psychological stress are accompanied by a decline in neurological function
and one of the major stressors for the dog is a stressed owner (Torraca, 2018). The disease has
a mental and physical impact on owners as they come to terms with the prognosis and managing
a progressively incapacitated dog. A physiotherapist can provide emotional support as well as
24information and advice on home exercises, comfort aids, assistive devices and home
modifications which will positively impact the welfare of the dog in between treatment sessions.
Comfort Aids
Boots/Socks
Boots and Socks can be used to protect the dog’s paws from abrasions, open sores and wearing
down their nails when they knuckle and drag their hind limbs. There are many varieties of dog
boots available and the correct type will depend on the weight and size of the dog as well as the
stage of the disease. Ruffwear™ Dog Walking Boots and RoyalCare™ Protective dog boots
are both good quality, waterproof and sturdy (Figure 9). It is important to bear in mind that DM
dogs already struggle with hind limb strength and proprioception and so heavy-duty hiking
boots, although durable and good for protection, may not be appropriate for some dogs as they
may be too cumbersome and will throw them off balance causing them to trip.
Figure 9:
Left: https://www.ruffwear.co.uk/dog-gear/dog-boots
Right: https://www.amazon.co.uk/Royalcare-Protective-Boots-Waterproof-Medium/dp/B0776VLQ8S
25A less cumbersome option is dog socks with grippy soles such as Grippers™ non-slip dog
socks. They are not as protective or durable and will be affected by weather conditions, but the
dog will be less likely to trip while wearing them. Human baby socks with grippy dots for extra
traction could be used as an alternative. PAWZ dog boots are rated well (Figure 10). Although
they look like deflated balloons, they are lightweight, durable and waterproof. They are not
breathable however, so are suitable for outdoors, and then can be swapped for a more breathable
material whilst the dog is indoors. It is important to note that they should be removed overnight
so the dog’s paws and skin can breathe sleeping.
Figure 10:
Left: https://www.dogquality.co.uk/products/grippers
Right: https://www.pawzdogboots.com/
Bedding
A supportive orthopaedic dog bed can alleviate bed sores. If the bed is too soft, it may be
difficult for the dog to get up from it. In addition, because the dog may have lost proprioception,
they may feel unsafe getting on the bed if it is too deep and too soft. A removable washable
cover is beneficial when the dog has become incontinent so it can be cleaned with ease. If the
bed does not have a removable cover, an incontinence sheet or puppy pad can be used and then
covered with blankets. Be cautious of some memory foam beds that compress too easily as this
will unbalance the dog, and they will be less likely to use it. Also consider temperature
regulation as some memory foam mattresses can retain heat and are not breathable. A paraplegic
dog will not be able to alter their recumbent position by themselves, so the owner must be aware
of discomfort. There are many brands of Orthopaedic bed and it is not always possible to try
26out pet beds before you buy them. The Pet Fusion Ultimate Pet bed and Lounger has received
good reviews.
https://www.amazon.co.uk/PetFusion-Memory-Medium-Large-91x71cmx23cm/dp/B00TQ47CPW
Movement Aids
Assistive Harnesses and Slings
As the symptoms of DM progress, the dog may require assistance walking, going up and down
stairs, getting in and out of the car and even during toileting. This can be quite a physical
challenge for owners with larger breeds. A support harness will enable the dog to remain
mobile, and give them a greater level of perceived independence. The Help ‘Em Up™ Harness
is probably the best known. It is made with high quality materials and with lifting handles over
the front and rear limbs. Not all dogs tolerate the straps around the hind limbs and hips, and
prefer just a thoracic support harness. The GingerLead® Dog Support and Rehabilitation
Harness is a good alternative (Figure 11). There is good sizing advice available by the retailers
of both these harnesses, but additionally, a physiotherapist should be able to help adjust it to fit
comfortably.
Figure 11:
Right: Help ‘Em Up Harness https://www.orthopets.co.uk/mobility-solutions/help-emup/
Left: GingerLead® Harness http://www.gingerlead.com/
A sling is now available to assist dorsiflexion of the hind feet. It prevents paw knuckling by
supporting the two centre digits via an adjustable elastic cord attached to a strap in the hock. It
is not suitable for prolonged use, or where the dog has delicate or sensitive interdigital skin.
27Another version is available as a Ruffwear boot conversion (Figure 12) so the sling can lift the
paw without directly contacting the skin.
Figure 12: https://www.orthopets.co.uk/mobility-solutions/sciatic-sling/
Wheelchairs and carts
Wheelchairs can be used during the initial stages of the disease when the degeneration only
affects the hind quarters (See Figure 13). They can be expensive and are not always tolerated
by the dog, but for some they bring a new lease of life as the dog enjoys independent locomotion
again. Care must be taken for them to fit correctly, but most reputable suppliers will build a
bespoke wheelchair for each individual dog. Carts can be used at any stage of the disease; as a
respite from fatigue during a walk in the early stages, or just to get the dog out and about for
extended periods of time when they are paraplegic. They are also expensive, but with some
imagination, cheaper options can be found - some owners retrofit a garden trolley!
Figure 13:
Left: Hercules Stroller
https://www.petsownus.co.uk/collections/3-wheelers-dog-strollers-dog-pram/products/hercules-heavy-duty-dog-
buggy-stroller-incl-rain-cover
Right: Eddies Wheels: https://eddieswheels.com/
28Home Modifications
Indoor Traction
To prevent slips and falls the use of rubber backed mats or non-slip rug netting will give the
dog more traction on slippery floors and stairs. Adhesive anti-slip tape or anti-slip discs are also
available and is an effective solution to provide more grip and enable more stability in the dog’s
movement.
Ramps
Ramps are invaluable when the dog is too large to lift in and out of the car or up and down steps
in the garden. Owners can easily construct a sturdy ramp that will remain permanently in one
position, such as in the garden. Portable ramps for getting in and out of a car are available in
lightweight folding and telescoping configurations.
The provision of any ramp should consider the following recommendations:
• Wide walking surface to make an unstable dog feel more confident to use them.
• Good traction on the surface so the dog doesn’t slip. Reduced proprioception is already
a problem so no slats.
• No bounce – should be built solid so they do not bounce. Uncoordinated dogs will find
a bouncy ramp frightening and will probably refuse to use it.
• Low gradient – should be as long as possible long so the angle of ascent is not too steep.
Always use a harness to guide the dog up and down any ramp.
Supportive Care
Dogs progressing to the second stage of the disease and beyond will be paraplegic and most
likely incontinent. The owner must take on a carer’s role providing support, company and
nursing care. Skin damage can occur as a result of pressure sores and urine scalding, but
frequently turning the dog from one side to the other and providing them with incontinence
pants (Figure 14) can minimise these problems. If skin damage does occur, the owner will need
to provide nursing care to keep the wound clean as it heals – phototherapy devices to aid skin
healing can be rented from a physiotherapist.
29You can also read