Dentalook Ontario Protocols - COVID PHASE 1 - OPENENING POLICIES AND PROCEDURES CREATED BY DENTALOOK OPERATIONS TEAM
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
JUNE 1 2020 Dentalook Ontario Protocols COVID PHASE 1 – OPENENING POLICIES AND PROCEDURES CREATED BY DENTALOOK OPERATIONS TEAM 1|Page June 1, 2020 CONFIDENTIAL FOR INTERNAL USE ONLY
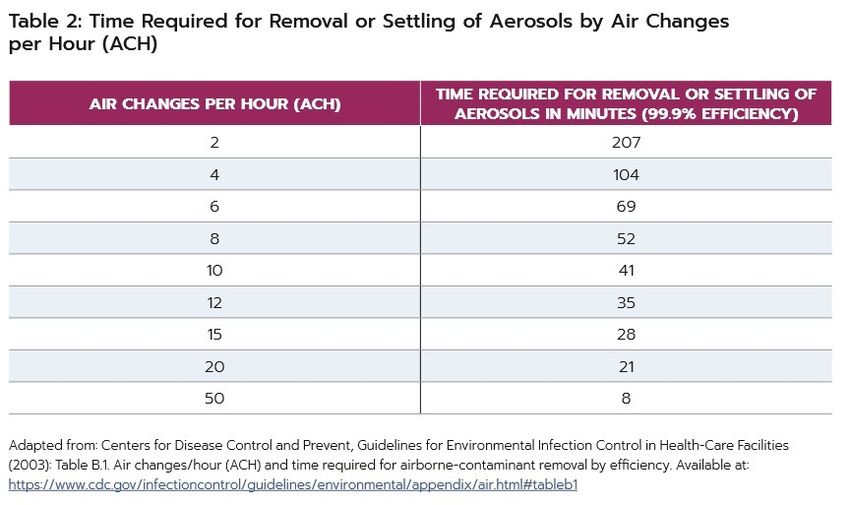
Table of Contents 1.0 INTRODUCTION ...................................................................................................................................... 4 2.0 COMMUNICATING WITH PATIENTS....................................................................................................... 5 2.1 Social Media Updates............................................................................................................................. 5 2.2 Recall Max Updates ............................................................................................................................ 5 2.3 Voicemail Updates ............................................................................................................................. 6 2.4 Booking and Confirming Appointments ............................................................................................ 6 2.4.1 EMAIL PRIOR TO APPOINTMENT ................................................................................................ 6 3.0 ENTERING & EXITING THE OFFICE .......................................................................................................... 7 3.1 Entering the Office ............................................................................................................................. 7 3.2 Exiting the Office .......................................................................................................................... 8 3.3 Clinical Notes ................................................................................................................................ 8 3.4 Temperature & Blood Oxygen Level Guide ....................................................................................... 8 4.0 PROTOCOL FOR TEAM MEMBER............................................................................................................ 9 4.1 Orientation: ........................................................................................................................................ 9 4.2 Attire to and From Work .................................................................................................................... 9 5.0 PROTOCOL FOR FACILITY ..................................................................................................................... 10 5.1 General Start up procedural check list ............................................................................................ 10 6.0 PROTOCOL FOR CLINICAL PROCEDURES .............................................................................................. 11 6.1 Pre-Procedural Rinse ........................................................................................................................ 11 6.2 Non-Aerosol Generating Procedures ............................................................................................... 11 The RCDSO (non-COVID) and CDHO allows for all the use of instruments and tools, including: ........... 11 6.3 Aerosol Generating Procedures ....................................................................................................... 12 6.3.1 RCDSO Aerosol Generating Procedures ................................................................................... 12 6.3.2 CDHO Aerosol Generating Procedures ..................................................................................... 13 7.0 PROTOCOL FOR PERSONAL PROTECTIVE EQUIPMENT ....................................................................... 14 7.1 Steps for Donning PPE ................................................................................................................ 14 7.2 Steps for Doffing PPE........................................................................................................................ 15 8.0 Cleaning the Operatory ........................................................................................................................ 15 8.1 Non Aresol Generating Operatory ................................................................................................... 15 8.2 Aerosol Generating Operatory – CDHO and RCDSO COVID positive.............................................. 15 9.0 Reporting Process................................................................................................................................. 16 2|Page June 1, 2020 CONFIDENTIAL FOR INTERNAL USE ONLY

10.0 Training and Education ...................................................................................................................... 17 11.0 CONCLUSION ...................................................................................................................................... 17 Appendix A: Office Equipment Checklist Appendix B: COVID-19 – What We Know So Far About… Routes of Transmission What We Know So Far Appendix C: HEALTH AND SAFETY GUIDANCE DURING COVID-19 FOR DENTAL OFFICES 3|Page June 1, 2020 CONFIDENTIAL FOR INTERNAL USE ONLY
1.0 INTRODUCTION Our office has revised our exiting protocols and procedure to ensure the safety of our team, patients, and communities. We have always delivered care with the highest level of infection control protocols. The following updated protocol were developed by combining the strict directives of: • Royal College of Dental Surgeons of Ontario • Ontario Ministry of Health • College of Dental Hygienist of Ontario Dentistry remains a safe and important aspect of healthcare. As future phases of Open Ontario evolve, our guidelines will adapt. Please ensure you are referencing the most recently dated document as you review this file. Should you have any questions or concerns, please address them with your manager. We value your input, insight, and feedback. Sincerely, Your Dentalook Operations Team 4|Page June 1, 2020 CONFIDENTIAL FOR INTERNAL USE ONLY
2.0 COMMUNICATING WITH PATIENTS Patients are likely now aware that visiting the dentist will require additional steps and procedures. However, we need to ensure that we fully inform our patients about the new processes in place. Thus, all patients must be called prior to their appointment in order to inform them of the mandatory protocols. 2.1 Social Media Updates TASK The regional manager will assign the office manager to post on their Facebook / Instagram page the following message. If you are unable to do so, please reach out to Marketing to do this for you. Social Media Announcement: We have exciting news! We will be reopening ! We received the green light to accommodate all dental services in our clinic. However, we are working to prioritize our emergency and urgent patients' needs. If you are experiencing pain or discomfort, please reach out, and we will work to see you as quickly as possible. Otherwise, we’ll be in touch to rebook or confirm upcoming appointments. We can’t wait to see your smile! 2.2 Recall Max Updates TASK The regional manager will assign the office manager to send a message to ALL patients via Recall Max. (please edit before you send) Recall Max Message: To our valued patients and families, We have exciting news! We are now able to accommodate all dental services in our clinics. However, we are working to prioritize our emergency and urgent patients' needs. If you are experiencing pain or discomfort, please reach out, and we will work to see you as quickly as possible. If you have an upcoming appointment, we will be in touch soon to confirm. If your appointment was canceled due to the COVID-19 closure, we will contact you to arrange a visit. We look forward to seeing you and introducing you to our new normal. The health and safety of our patients and team members are always our priority. On your next visit, you'll see some additional changes that further enhance our commitment to your safety. 5|Page June 1, 2020 CONFIDENTIAL FOR INTERNAL USE ONLY
When we call to confirm your appointment, we'll take a moment to do a health screening. Encourage you to arrive at your appointment wearing a mask but can provide one for you if necessary. We are always here to answer your questions and address your concerns. We are all in this together! One thing is for sure - we certainly have missed seeing all the friendly faces in our office, and we look forward to seeing them again. Your ….. 2.3 Voicemail Updates TASK The Office Manager will need to update the message on the phones to the following: (edit response before recording) Office Voice Message Please update your voicemail message to include “We are now open and treating all ranges of dental needs. We are working on prioritizing our urgent and emergency patients needs. However, we are also re-booking and confirming upcoming appointments. Thank you for your patience during this time and we look forward to seeing you!”. 2.4 Booking and Confirming Appointments TASK When you call the patients to book them in for their appointment: -Please ask for their email address -Restate their appointment time -Ask them if they have had any cough, fever or health issues requiring hospitalization in last two weeks -Walk them through the steps -Let them know that we will be emailing them a checklist of what to expect with the new changes. 2.4.1 EMAIL PRIOR TO APPOINTMENT The following is what to share with patients via email ahead of their appointment. We are looking forward to your upcoming appointment with us. I would like to introduce you to our “new normal”. There have been additional measures put in place to enhance our measures. It is, and has always been, our priority to keep our patients and team members safe. Prior to coming for your appointment, we ask that you: • Please wear a mask to your appointment. If you do not have one, we will give you a mask • Call the office at xxx-xxx-xxxx when you arrive 6|Page June 1, 2020 CONFIDENTIAL FOR INTERNAL USE ONLY
• We will let you know when to enter the office • Please come alone into the office. If you require a ride to the office, we will need your driver to wait in the vehicle for you as we are limiting traffic in the office. • A team member will greet you at the office when you arrive, and you will sanitize your hands • The Ontario Ministry of health assessment form will be completed, and your temperature recorded • You will be asked to sign a consent form prior to your treatment • We will call you 48 hours and then 14 days after your treatment to ensure that you are healthy and well. At this time, we are NOT accepting cash, please be prepared to pay with your credit card or debit card Again, we look forward to seeing you and if you have any questions or concerns, you may reach us at xxx-xxx-xxxx (Dental Office Name) 3.0 ENTERING & EXITING THE OFFICE To follow social distancing rules and the various guidelines, we are required to limit the number of patients in the dental office at one time. Thus, new steps for visiting and leaving the office are in place. 3.1 Entering the Office • Patients and/or their Parent/Guardian must wear a mask or be provided with one. • Patients and/or their Parent/Guardian “Check-In” from their car upon arrival at the office, by calling the office phone number • The Patient and/or their Guardian/Parent will wait in the car until the office calls the patient into the office, or confirmed that they may enter • The patient (if a minor) will be escorted to the office door by the parent/guardian • Only the patient is allowed in the office • The Parent/Guardian will “Hand-Off” their minor child to the dental administrator/ concierge at the door • The temperature and blood oxygen levels of every patient will be taken before they come into the office • Proper Patient protection will be at the door for the patient to put on before entering the office • Patients are to use hand sanitizer when entering the office 70-90% hand sanitizer or soap and running water • Patient must be cleared by the Office Administrator/ concierge to enter the Dental Office. • A “concierge” from the office will escort the patient directly to the treatment area/chair (after hand sanitizer) 7|Page June 1, 2020 CONFIDENTIAL FOR INTERNAL USE ONLY
3.2 Exiting the Office • Upon completion of the dental service, the patient’s guardian/parent will be notified by phone to come to the front door. • The patient will use hand sanitizer when leaving the office (They use it twice; arrival and departure). • The patient will be “Handed-off” to their parent/Guardian who is outside by the door and NOT in the office • If a payment is required, the patient will be required to make the payment before leaving the office • If it is a minor payment can be made over the phone with credit card • Patients will discard mask in the garbage prior to leaving the office • 48 hours and 14 days following treatment, the patient will be contacted to screen for any new COVID-19 symptoms. Health status must be documented in the patient chart. • Should the patient indicate they are symptomatic, please follow the Reporting Process Protocol 3.3 Clinical Notes • Pre procedural rinse at the beginning of the appointment for 60 seconds and again after the appointment • High Volume suction is to be used throughout the appointment to reduce Aerosols 3.4 Temperature & Blood Oxygen Level Guide Temperature: • The average normal body temperature is generally accepted as 98.6°F (37°C). • Some studies have shown that the "normal" body temperature can have a wide range, from 97°F (36.1°C) to 99°F (37.2°C). • A temperature over 100.4°F (38°C) most often means you have a fever caused by an infection or illness. Blood Oxygen Saturation (Sp02): • Sp02 indicates the level of oxygen in a patient’s red blood cells. There is some evidence to show that asymptomatic COVID patients can have low levels of blood oxygen. Patients with COVID • By checking their Sp02, we are adding another layer of safety Normal Levels are between 95-100% Below Average levels are 91-95% Low/Warning levels are under 90% ADVISE YOUR PATIENT CONSULT THEIR DOCTOR 8|Page June 1, 2020 CONFIDENTIAL FOR INTERNAL USE ONLY
4.0 PROTOCOL FOR TEAM MEMBER We’ve all missed working together, however, to ensure social distancing, we must: • Please ensure that there is no gathering • Lunch breaks will be staggered • As best possible, we must maintain social distancing • Enhance general office housekeeping, including cleaning and disinfection of high-touch surfaces i.e., door handles, debit terminal after each patient will take place 4.1 Orientation: • Each office/clinical team member must be orientated and read and sign off on the new protocol • Each clinical team member must watch the Donning and Doffing Video – note our office may have a slight variation on the video, depending on the set up in place. • Each office/clinical team member must conduct their own self-assessment for COVID-19, prior to attending the dental practice for work. • Each office/clinical team member must take their temperature and record it on the log sheet when they arrive 4.2 Attire to and From Work • Each clinical team member must change into scrubs at the dental office. We cannot leave the office in scrubs. Even though we are wearing additional PPE, we must maintain baseline practices. Consider wearing short sleeve scrubs, since it can get warm with a gown on top. • Safely store your garments in a plastic bag, so you can wash when you return home • Each clinical team member must change their shoes when arriving and leaving the office • Follow appropriate steps for putting on and removing PPE. • After you dispose your PPE, wash your hands with antibacterial soap and water for 60 seconds • The level of mandatory PPE will be related to the task they are performing. Please refer to the College Guidelines to understand what PPE is required for your role. • If extended use of PPE is in place, note that we are following the World Health Organization Protocols 9|Page June 1, 2020 CONFIDENTIAL FOR INTERNAL USE ONLY
5.0 PROTOCOL FOR FACILITY Remove all the contents in operatories in which an aerosol-generating procedure may be performed, including unnecessary equipment, supplies, plants and artwork. Remove all magazines and toys from waiting areas to prevent contamination. Reception waiting chairs must be wipeable. Hand washing signs need to be displayed within the washroom Putting on and removing PPE poster needs to be displayed in all operatories Each operatory requires a Garbage can with a lid needs and a Soiled Linen Can A garbage can must be place outside the operatory to discard other PPE Aerosol Generating Procedure signage should be placed at the entrance to the room Social Distancing Posters must be clearly visible to patients and staff Any remaining chairs in the waiting room must be spaced 6 feet apart Place a marking 6’ away from the front counter, in the unlikely event that two people are waiting to pay at the same the time As most of our practices only have one entrance, please ensure the timing of patients entering and exiting the practice does not conflict. 5.1 General Start up procedural check list The Equipment Start Up Process Checklist.docx is a general guide that you can follow to help start equipment up in your office. Please see Appendix A. It is highly recommended to schedule one of the Technical Service Representatives to visit your office to help ensure that all your equipment is operational, it is preferred to be done before opening day. 10 | P a g e June 1, 2020 CONFIDENTIAL FOR INTERNAL USE ONLY
6.0 PROTOCOL FOR CLINICAL PROCEDURES Currently the province has a multi-staged approach to return to practice. Dental Procedures Acceptable in Stage 1 At the height of community transmission, in-person dental care is restricted to emergency and urgent care only (RCDSO_definitions_dental_care.pdf) . In Stage 1, non-emergency and non-urgent care may only be provided remotely (i.e., via teledentistry). Dental Procedures Acceptable in Stage 2 As community transmission declines, dentists will be permitted to provide an expanded list of in-person services, with enhanced precautions. Note: as of June 1st, 2020, the RCDSO developed a separate pathway for patients who screen or are verified as COVID positive status. The CDHO does not permit dental hygiene treatments in COVID-19 positive patients at this time. Dental Procedures Acceptable in Stage 3 When community transmission has been significantly mitigated, dentists will enter the ‘new normal’ in which in-person care is provided with reduced precautions 6.1 Pre-Procedural Rinse • Each patient will have patients to rinse with 1% - 1.5% hydrogen peroxide or 1% providone- iodine for 60 seconds at the beginning and end of each appointment • The patient will spit the rinse back into the cup provided, which is then discarded • Over-the-counter peroxide is typically 2%, so it would need to be diluted. • Colgate Proxyl and Listerine Whitening mouth rinse, that are 1.5% and would not require dilution • Utilize what you may already have in office or can get through your dental suppliers. 6.2 Non-Aerosol Generating Procedures The RCDSO (non-COVID) and CDHO allows for all the use of instruments and tools, including: • High-speed and low-speed handpieces • Hand instruments • Air-water syringe, cotton roll or gauze or monojet RCDSO PPE REQUIREMENTS CDHO PPE REQUIREMENTS Surgical Mask – Level 2 or 3 Surgical Mask Level 1, 2 or 3 Gloves Gloves Eye Protection and/or Face Shield Eye Protection or Face Shield Isolation Gown 11 | P a g e June 1, 2020 CONFIDENTIAL FOR INTERNAL USE ONLY
6.3 Aerosol Generating Procedures The RCDSO and CDHO have outlined respective approaches for the management of aerosols in dental procedures. Dentalook is striving to maintain the highest level of safety precautions and upholding the respective guidelines. The following best practices algin to both guidelines: • AGP operatory rooms must have a Donning and Doffing Anteroom or Hallway Area • Doffing of gown and gloves may be done in operatory, while mask is doffed in the hall • If possible, use a rubber dam with high-volume suction to minimize aerosols and possible exposure to infectious agents • The following sign must be placed on the door should an AGMP take place 6.3.1 RCDSO Aerosol Generating Procedures RCDSO PPE REQUIREMENTS – COVID NEGATIVE RCDSO PPE REQUIREMENTS – COVID POSITIVE N95 Fit Tested or Surgical Mask – Level 2 or 3 N95 Mask fit tested Gloves Gloves Eye Protection or Face Shield Eye Protection AND Face Shield Protective Gown (Optional) Protective Gown Sealed Room with Closed Door Aerosol settle time – as calculated 12 | P a g e June 1, 2020 CONFIDENTIAL FOR INTERNAL USE ONLY
6.3.2 CDHO Aerosol Generating Procedures Dental hygienists and supporting staff are required to wear the following PPE during AGPs. RCDSO PPE REQUIREMENTS – COVID POSITIVE N95 Mask fit tested Gloves Eye Protection or Face Shield Protective Gown Sealed Room with Closed Door Aerosol settle time – as calculated Gowns must be changed after each procedure, either being laundered by commercial provider or disposed. N-95 masks must be disposed after each use. We are awaiting guidance on the use of silicone/re-useable masks that pass fit testing. 13 | P a g e June 1, 2020 CONFIDENTIAL FOR INTERNAL USE ONLY
7.0 PROTOCOL FOR PERSONAL PROTECTIVE EQUIPMENT Part of ensuring the effectiveness of the PPE provided is understanding the process of putting on (donning) and taking off (doffing) of the equipment. Task Please watch the donning and doffing video to be better understand the process. Donning Station – “Clean” Side Includes: Gowns, Masks, N95 Respirator, Level 2-3 masks, Goggles or Face Shields, Gloves, Alcohol Base Hand Rub (ABHR) Doffing Station – “Dirty” Side: Laundry Receptacle with Lid / Garbage Receptacle with Lid, Eye Protection Disinfection Receptacle with Lid. 7.1 Steps for Donning PPE PPE must be donned in the “Clean” Side before entering the AGP Operatory Room - do not go anywhere else once the PPE is donned. Outside the Room: 1) Perform hand hygiene 2) Put on gown 3) Put on mask, N-95 as per procedure and then Level 1-3 over top if required 4) Put on protective eye wear 5) Put on face shield 6) Hand hygiene 7) Put on gloves, ensure the cover cuffs Optional: cap or bonnet that can stays on for the day. COVID 19\rpap-recommeded-ppe-steps.pdf During AGP by the RDH team or dental team members treating COVID + patients: The operatory door shall remain closed during the procedure. Only the dentist, dental assistant and patient will be permitted in the operatory during treatment. The operatory door should only be opened once to discharge the patient and for clinical staff to exit. 14 | P a g e June 1, 2020 CONFIDENTIAL FOR INTERNAL USE ONLY
7.2 Steps for Doffing PPE PPE must be REMOVED in the AGP Operatory Room “Dirty Side” BEFORE you leave the room: 1) Remove the gloves 2) Perform hand hygiene 3) Remove the gown, and turn it inside out while removing it 4) Dispose of in the laundry basket or garbage if its disposable 5) Perform hand hygiene EXIT the room and close the door (You are now on the clean side) 1) Perform hand hygiene 2) Remove eye protection/ shield and place in appropriate place for cleaning 3) Remove Mask – disposing of Level 1-3, place N-95 in appropriate place for storage 4) Perform hand hygiene Refer to donning to doffing diagram chart 8.0 Cleaning the Operatory When a room can be cleaned and prepared for the next patient depends on what treatment was most recently preformed. 8.1 Non Aresol Generating Operatory The practitioner may clean the operatory during this time as outlined in the IPAC standard and Public Health guidelines. 8.2 Aerosol Generating Operatory – CDHO and RCDSO COVID positive As a best practice, Dentalook has calculated the air exchange time per hour for each operatories. The CDHO mandates that the room must sit afterwards to allow the aerosol to settle before it can be cleaned using normal IPAC Standards for Oral Health Care Facilities. This is also the case for the emergency treatment of COVID positive patients. Following a procedure, the following form MUST be completed and be visible to all: Follow Time Required for Removal or Settling of Aerosols by Air Changes per Hour (ACH) chart for specific settling time 15 | P a g e June 1, 2020 CONFIDENTIAL FOR INTERNAL USE ONLY
9.0 Reporting Process An essential of part of infection control is the pre- and post-procedural COVID-19 screening. The Ministry of Health Questionnaire is reviewed: 1) Over the phone at appointment confirmation 2) Prior to entry into the facility on the date of their appointment 3) 48 hours and 14 days following their procedure IF a patient reports symptoms indicative of COVID-19, it is our legal obligation to advise them to contact their Primary Care Provider or Telehealth Ontario at 1-866-797-0000. As providers, we must also contact our local Public Heath Authority to report the patient. Should the patient present as possibly symptomatic during in person pre-screening, the Concierge must immediately doff all PPE and sanitize the area. Note, pre-screening is not an Aerosol Generating Procedure, thus there is no need to wait the 180 minutes. 16 | P a g e June 1, 2020 CONFIDENTIAL FOR INTERNAL USE ONLY
10.0 Training and Education In addition to the Dentalook COVID-19 Guidance document, you are required to review and understand the following: 1) Ontario Public Health: COVID-19 – What We Know So Far About… Routes of Transmission What We Know So Far This document is attached in the PDF as Appendix B. 2) Public Service Health and Safety Association: HEALTH AND SAFETY GUIDANCE DURING COVID-19 FOR DENTAL OFFICES This document is attached in the PDF as Appendix C. Our Dentalook training process includes other elements not reflected in this manual: Dentalook videos Donning and Doffing Safe use of PPE RCDSO Guidelines CDH0 Guidelines IPAC Guidelines As healthcare providers, it is our obligation and ethical responsibility to ensure we abide by all guidelines and regulations. Regulatory compliance allows for a safe work environment and best possibly delivery of care to our patients. Please consult your Regional Manger to ensure that you have completed all modules. A sign off sheet is in each office and is maintained as essential record keeping during this pandemic. It is important to note that our training also extends to third party providers who visit Dentalook sites. For example, our cleaning and laundering service partners, will also have relevant training provided to them. 11.0 CONCLUSION This document represents the collective effort of the Dentalook Operations team for returning to clinical practice. This document will continue to evolve and reflect the changes that our various governing bodies release in due course. As always, we value your input, efforts, and contribution towards ensuring our patients have the best possible dental care available. 17 | P a g e June 1, 2020 CONFIDENTIAL FOR INTERNAL USE ONLY
2020 DENTALOOK EQUIPMENT CHECKLIST POST COVI D - 19 PATH TO RECOVERY TOOLS
DENTALOOK 4S FRAMEWORK About this Equipment Checklist Our dental practices house considerable amounts of equipment which are essential in the providing of oral health treatments. The extended closure of practices come with the risk of damage or maintenance requirements for our equipment. The Dentalook Operations Team is sharing some of the tools we used to ensure that our re-opening process was smooth and our equipment in working order to see patients. Our vendors have strongly recommended that dental practices schedule visits with their technical service representatives. The demand for their time will be high, thus we suggest being proactive in this manner. Regards, The Dentalook Operations Team DISCLAIMER This content is a representation of Dentalook’s best understanding of the current situation. It was built from provincial guidelines set forth by the Saskatchewan Health Authority, the College of Dental Surgeons of Saskatchewan, and the Saskatchewan Dental Hygienists Association. Your local guidelines may be different. Our goal is to share our thought process to practice safely and responsibly post-COVID. Dentalook is not liable for how your practice may implement provincially mandated requirements. 4S Framework© 2020 – DENTALOOK
DENTALOOK 4S FRAMEWORK EQUIPMENT CHECKLIST – PHASE 1 RE-OPENING Utility room / Mechanical room ☐First turn on water filter bypass (replace Filter if needed) ☐ Turn on Compressor, Ensure unit turns off after a few minutes then check air for leaks. ☐ Before turning on your vacuum pumps, clean or replace the solids collector/filter/screen. Turn on the vacuum system and check for any leaks. ☐ Amalgam Separator, check cartridge level and for any leaks. Filter must be replaced if required. ☐ Be sure to check on the utility room frequently while doing the start up to ensure all equipment remains leak free. The last thing you need is a flood to occur. ☐ Nitrous Oxide, check all connections are secure and turn on tanks and check for leaks. Sterilization Area ☐ Sterilizers, empty all water out of unit, if it was not done at shutdown please clean reservoir tank and refill. Wipe door seal and associated contact area with a wet cloth. At least run two empty cycles on all sterilizers. Perform a sterility confirmation test. ☐ Perform a spore test ☐ Instrument washers, reconnect the soap dispenser and run a standard cycle. And check for proper operation. ☐ Handpiece lubricator check fluid levels and test. ☐ Ultrasonic bath fill and test. ☐ Water distillers, Run unit as per usual. If cleaning was not done at shutdown please clean unit as per manufacturer instructions then you can operate the unit. 4S Framework© 2020 – DENTALOOK
DENTALOOK 4S FRAMEWORK ☐ Other water purification systems check for leaks and change filters as required. Operatories ☐We highly recommend you to perform water shock treatment and CFU testing to all water lines (Call your Service Department Rep for more detailed information and assistance). ☐Flush all Handpiece lines and syringes for at least 2 minutes. ☐Check all suction valves for correct operation, if not opening smoothly soak in hot water. ☐ Ensure there is no air or water leaks. ☐ General check of all items to ensure proper operation. Chair, Light, Scaler, Foot controls, etc. ☐ Turn on x-rays and do a test to confirm proper operation. ☐ Turn on all computers and connected products / equipment. ☐ Connect all sensors and test, if you are not familiar with this, please contact one of our Digital specialists in your area. Test sensor for image acquisition. Film Processors (Chemical) ☐Ensure that the chemicals were cleaned out of the film processor. ☐Preferably soak racks in warm water for at least 15 minutes to help remove any crystalized chemical and allow proper function the racks. Turn gears or rollers by hand to ensure racks are moving freely. ☐Assemble unit, put water into all tanks and run the unit (cleaning film where applicable) to ensure proper operation, if transports are turning smoothly, drain water and refill with Fixer and Developer chemistry. 4S Framework© 2020 – DENTALOOK
DENTALOOK 4S FRAMEWORK Scaler / Polisher Units ☐Flush for a minimum of 2 minutes on low power setting, prior to inserting tip. ☐Test units to ensure proper operation. ☐Prophy Jet-: Refill powder chamber with fresh and Dry Powder and test. Pan/ceph/CBCT x-ray room ☐Check functionality of Phosphor plate system if applicable. ☐Check power cables, power cycle to panoramic x-ray and power conditioners. ☐Test pan/ceph/cbct into digital imaging software. CAD CAM and milling units ☐Connect cad/cam system cables to computer and run a test scan on a model. ☐Replace water tank solutions and run in tests to flush the water lines on milling unit. ☐Check if water is properly spraying onto milling burrs in milling chamber. General ☐Ensure all necessary equipment is powered. ☐Check plaster trap in lab, run water and check for leaks. ☐Do a final check in the mechanical room for any leaks. 4S Framework© 2020 – DENTALOOK
SYNOPSIS 04/28/2020 COVID-19 – What We Know So Far About… Routes of Transmission Introduction “What We Know So Far” documents are intended to provide an overview of some of the published and unpublished reports related to emerging issues with respect to Coronavirus Disease 2019 (COVID-19). As this is a rapidly evolving situation, the information will only be current as of the date the document was written, with further updates as needed. Key Points COVID-19 is transmitted via droplets during close, unprotected contact. Airborne spread has not been documented for COVID-19, but aerosols may be generated during aerosol generating medical procedures which could theoretically lead to transmission through this route. There is no specific evidence documenting transmission through fomites. However, the virus has been detected on surfaces in the patient environment and this is a likely source of transmission based on experience with other coronaviruses. While the virus has been detected in the stool and the blood, the roles of fecal-oral and bloodborne transmission remain uncertain. There is no conclusive evidence of vertical transmission to date, but further studies are needed. Background The purpose of this document is to outline what is known about how COVID-19 is transmitted from person-to-person, based on a review of the scientific literature. The virus responsible for COVID-19 is genetically similar to other coronaviruses. In particular, it shares a high degree of genetic similarity (79% identity) (Lu R et al.), with the coronavirus (CoV) responsible for Severe Acute Respiratory Syndrome (SARS). Therefore, in instances of limited evidence for COVID-19, it is reasonable to extrapolate existing data from other coronaviruses, in particular SARS-CoV. Droplet and Contact Transmission Current evidence suggests that the mode of transmission of COVID-19 is through direct contact and respiratory droplets that have the potential to be propelled for varying distances (European Centre for Disease Prevention and Control (ECDCa), Imai et al., Schneider et al.). COVID-19 – What We Know So Far About…Routes of Transmission
The majority of cases have been linked to person-to-person transmission through close direct contact to someone with respiratory symptoms (Burke et al., Chan et al., ECDCa, Pung et al.) or close contact with a case in the incubation period who was later confirmed to have COVID-19 (Huang R et al., Tong et al., Yu P et al.). High viral loads have been identified in individuals who were asymptomatic or pre-symptomatic (Arons et al.); however, uncertainties remain regarding the role of asymptomatic transmission in driving outbreaks in the absence of major droplet- releasing symptoms (e.g. coughing, sneezing). A recent report by the World Health Organization (WHO) Joint Mission on Coronavirus Disease 2019 (COVID-19) in China, summarizes the experience with 75,465 cases and indicates that the route of transmission is droplet during close unprotected contact (WHO) Respiratory droplets have been shown to be propelled up to 2 meters (m) in most studies (ECDCa, Imai et al., Schneider et al.) studies and occasionally have been found on the floor up to 13 feet (ft) (or 4 m) away from the patient (Guo et al.). Conjunctiva Transmission through the ocular surface is considered a possible route of transmission for COVID-19 based on a recent case report and evidence of virus detection from the eye among cases with conjunctivitis. In a case report, the authors describe a healthcare worker who became infected with COVID-19 after visiting a patient wearing an N95 respirator, but no eye protection. The healthcare worker developed eye redness and then pneumonia (Lu C et al.). In one study of 30 confirmed COVID-19 cases with pneumonia, tear and conjunctival secretions were collected twice from each patient and tested using reverse transcription polymerase chain reaction (RT-PCR) assays. Only one patient had conjunctivitis with one of two samples yielding a positive RT-PCR result. The remaining 58 samples from all other patients were negative (Xia et al.). In a cross-sectional study of 72 laboratory-confirmed cases of COVID-19, two patients (2.8%) had conjunctivitis. Viral RNA fragments were identified in ocular discharges using a RT-PCR assay in one patient with conjunctivitis (Sun et al.). In another cross-sectional study, conjunctival RT-PCR assays were conducted on 14 confirmed cases and 16 suspect cases of COVID-19. All results were negative (Xu L et al.). Airborne Transmission There is currently no evidence that COVID-19 is transmitted through the airborne route. As more epidemiological data emerge on cases globally, information is becoming available that suggest that airborne transmission is not occurring: A recent report from the WHO China Joint Mission on COVID-19 summarizing 75,465 cases indicates that airborne spread has not been reported (WHO). This report states that the majority of COVID-19 transmission in China is occurring within families. Of all of the infection clusters investigated, 78-85% were within families, with a household secondary attack rate of 3-10%. The absence of significant clusters in other settings suggests that the mode of COVID-19 transmission is not airborne. An article describing the active follow-up of individuals exposed to first ten cases of COVID-19 in the United States describes secondary transmission only to close household contacts. In this COVID-19 – What We Know So Far About…Routes of Transmission 2
article, 445 persons who had contact with one of the cases were identified. Of these, 19 (4%) were household members, 104 (23%) were community members who spent at least 10 minutes in close proximity to the case, 100 (22%) were community members exposed in a healthcare setting and 222 (50%) were healthcare workers. Two persons who were household members of cases of COVID-19 tested positive, for a symptomatic secondary attack rate of 0.45% (2/445) among all contacts and a symptomatic secondary attack rate for all household contacts of 10.5% (2/19) (Burke et al.). The absence of transmission to contacts outside the household setting suggests that the mode of COVID-19 transmission is not airborne. Of note, five household members who were continuously exposed to a case did not become infected. Healthcare workers caring for COVID-19 patients in other jurisdictions, including British Columbia, have not acquired COVID-19 while using Droplet and Contact Precautions recommended in the province (Weeks). The lack of transmission to passengers seated nearby cases who have travelled on airplanes, does not support an airborne transmission route of COVID-19 (Schwartz et al.). Studies have inconsistently detected virus in air sampling: In two studies conducting air sampling around confirmed cases, COVID-19 was not detected (Cheng et al., Ong et al.). One study detected SARS-CoV-2 by PCR in 35% (14/40) air samples in the ICU and 12.5% (2/16) air samples on the general ward where patients with COVID-19 are managed. The majority of these air samples were within 2 m of the patients, with 1/8 samples positive at 4 m away (Guo et al.). An investigation of a COVID-19 outbreak in a restaurant in Guangzhou, China determined that the air conditioning ventilation likely contributed to droplet transmission. Infections were documented in three families after sitting in close proximity (< 1 m) for more than 1 hour. None of the other staff or diners were infected, suggesting airborne transmission was unlikely (Lu J et al.). Airborne Transmission during AGMPs While airborne transmission has not been documented under routine circumstances (i.e. in community settings and in routine patient care) it may be possible for it to occur when an aerosol-generating medical procedure (AGMP) is performed. This is supported by the recent report from WHO, which states that airborne transmission could theoretically occur during an aerosol-generating medical procedure, although there were no documented occurrences in the report (WHO). Studies have documented the aerosol stability of SARS-CoV-2 In the study by van Doremalen et al., aerosols were created experimentally (three-jet nebulizer and Goldberg drum) and found to survive up to three hours on surfaces, supporting that aerosols may be generated under certain circumstances (i.e. AGMPs). Case series of exposures to COVID-19 patients during AGMPs have not demonstrated transmission to HCWs using droplet/contact precautions (Ng et al., Wong et al.). During the SARS outbreak in 2003, infections disproportionately occurred among healthcare workers, with those involved in aerosol-generating procedures and manipulation of the airway (i.e. at the time of intubation) at greatest risk (Booth CM et al.). An investigation into a nosocomial outbreak of SARS in Toronto concluded that the epidemiological links described in their investigation support the theory that SARS is transmitted primarily through respiratory droplets and direct contact, but noted that transmission occurred during high risk procedures COVID-19 – What We Know So Far About…Routes of Transmission 3
(i.e. intubation) when only a surgical mask was utilized, in the absence of protective eyewear (Varia et al.). More information on what is currently known about COVID-19 and the risks to healthcare workers can be found in the WWKSF document on the Risks to Health Care Workers. Fomite Transmission There is currently no data on the ability of COVID-19 to survive or be transmitted through surfaces. However, there is indirect evidence to support that this is a possible source of transmission: Studies have documented the presence of virus on surfaces in the environment of patients who have tested positive for COVID-19 (Ong et al., van Doremalen et al.). Other coronaviruses have been observed to remain viable for days to weeks on environmental surfaces. Survival is enhanced at low temperatures (i.e., 4°C vs. 20°C) (ECDCb, Kampf et al.). The relative importance of indirect contact transmission (i.e. droplets spreading from a patient to an environmental surface to another individual) for the coronaviruses responsible for SARS and Middle East Respiratory Syndrome (MERS) is also uncertain (Otter et al.). Two field studies have evaluated SARS-CoV surface contamination: In a study involving hospitals in Bangkok, Thailand, Taipei, and Taiwan, 24/63 (38%) of surfaces (patient rooms, nursing stations, emergency department, and public spaces) had viral RNA detected by PCR. However all were culture negative (i.e. viable virus could not be grown from the samples) raising uncertainty of the viability of the detected virus and its ability to cause human infection (Dowell et al.). During the 2003 SARS outbreak in Toronto, 85 swabs were taken from 19 patient rooms in Toronto hospitals. A total of 3 (3.5%) were positive (bed table, TV remote, fridge handle in nursing station), however none were culture positive, raising similar questions about the risk for human infection (Booth TF et al.). Fecal-oral Transmission While the virus has been detected in the stool, the roles of fecal-oral transmission remains uncertain. As part of early investigations of the outbreak, the virus responsible for COVID-19 has been detected and isolated in the intestinal tissues of animals challenged with the virus (WHO). Tissues in the oral cavity express angiotensin-converting enzyme 2 (ACE2) receptors that are believed to be used by COVID-19 to enter cells (Xu H et al.). ACE2 receptors have also been documented in the cytoplasm of gastrointestinal epithelial cells (Xiao et al.). It has been reported that a small proportion of patients experience diarrhea and vomiting during COVID-19 infection (Chen N et al., Guan et al., Wang D et al.), with case reports of gastrointestinal symptoms in the absence of respiratory symptoms (Hosoda et al., Song et al.). COVID-19 RNA has been detected in stool in various studies, with prolonged shedding for up to 4-5 weeks in moderate cases and pediatric cases (Chen L et al., Tang et al., Wu et al., Xu Y et al.). Live virus has reportedly been cultured from stool, in some cases (Wang W et al., WHO, Pan et al., Zhang et al.). A case report found SARS-CoV-2 RNA detection and intracellular staining of viral nucleocapsid protein in gastric, duodenal, and rectal epithelia demonstrating that SARS-CoV-2 infects these gastrointestinal glandular epithelial cells (Xiao et al.). COVID-19 – What We Know So Far About…Routes of Transmission 4
The WHO-China Joint Mission Document notes that viral RNA has been detected in feces in up to 30% of patients from day 5 following onset of symptoms and in some cases has been detected for up to 4-5 weeks (WHO). More information on fecal-oral transmission can be found in the What We Know So Far (WWKSF) document on fecal-oral transmission. Bloodborne Transmission While the virus has been detected in the blood, the role of bloodborne transmission remains uncertain. Several studies have reported detection of COVID-19 RNA, in either plasma or serum (Chan et al., Huang C et al., Wang W et al.). More information on bloodborne transmission can be found in the WWKSF document on bloodborne transmission. Vertical Transmission To date, there has been no conclusive evidence of vertical transmission of COVID-19 from mother to child. Although several case reports suggest that it may be possible, the reported case series to date suggest that it is not a common occurrence. The following studies have shown no evidence of vertical transmission: Khan et al. reported no vertical transmission after three pregnant women with COVID-19 delivered naturally; children had normal birth weights, lengths, and Apgar scores. Zhu et al. reported no vertical transmission after 9 pregnant women with COVID-19 delivered; findings were confirmed with throat swabs taken at one to nine days after birth and there was no evidence of vertical transmission. Fan et al. reported no vertical transmission after two pregnant women with COVID-19 delivered and both infants were in good health. Chen R et al. reported no vertical transmission after 17 pregnant women with COVID-19 delivered via Caesarean section. Three births were premature, but newborns were over 2500 g and children were discharged in good health following brief observation in the NICU. Lack of infection was confirmed with nasal swabs performed one day after birth and again on the day before discharge. Chen H et al. reported no vertical transmission after 9 pregnant women with COVID-19 pneumonia delivered via Caesarean section. SARS-CoV-2 could not be detected in amniotic fluid, cord blood, breast milk, or from neonatal throat swabs. Liu et al. reported no vertical transmission after 10 pregnant women with COVID-19 delivered via Caesarean section. There was no clinical or serologic evidence suggestive of vertical transmission. Yu N et al. reported unlikely vertical transmission after 3 pregnant women with COVID-19 delivered via Caesarean section. One of the newborns contracted the virus 36 hours after birth. SARS-CoV-2 was not detected in the placenta or cord blood in this patient. Yang et al. reported no vertical transmission after a pregnant woman with COVID-19 delivered via Caesarean section. An oropharyngeal swab, obtained immediately after birth, indicated the newborn was negative. During the next 2 days, the infant’s oropharyngeal COVID-19 – What We Know So Far About…Routes of Transmission 5
swab, blood, feces, and urine samples remained negative for SARS-CoV-2 throughout testing at 7 different time points. The following studies provide some evidence that vertical transmission of COVID-19 may occur, but do not provide conclusive evidence. The interpretation of antibody testing for SARs-CoV-2 is an evolving area and concerns around possible cross-reactivity and specificity need to be considered. Zeng L et al. reported possible vertical transmission in 3 of 33 neonates who were born to mothers with confirmed COVID-19 pneumonia. They report that because ‘strict infection control and prevention procedures were implemented during the delivery’ it is likely that the source of infection was maternal, but details of these practices are not provided. Neonates were diagnosed based on swab results done on Day 2 of life. Zeng H et al. reported possible vertical transmission in 2 of 6 neonates who were born to mothers with COVID-19 pneumonia at Zhongnan Hospital of Wuhan University and delivered via Caesarean section. All mothers wore masks, and all medical staff wore protective suits and double masks. The infants were isolated from their mothers immediately after delivery. Neonatal throat swabs and blood samples collected at birth all had negative RT-PCR test results. All 6 infants had antibodies detected in their serum, 2 infants had IgG and IgM concentrations higher than the normal level (
References 1. Alzamora MC, Paredes T, Caceres D, Webb CM, Valdez LM, La Rosa M. Severe COVID-19 during pregnancy and possible vertical transmission. Am J Perinatal. 2020 Apr 18 [Epub ahead of print] Available from: https://doi.org/10.1055/s-0040-1710050 2. Arons MM, Hatfield KM, Reddy SC, Kimball A, James A, Jacobs JR, et al. Presymptomatic SARS- CoV-2 infections and transmission in a skilled nursing facility. N Eng J Med. 2020 Apr 24 [Epub ahead of print]. Available from: https://doi.org/10.1056/NEJMoa2008457 3. Booth CM, Matukas LM, Tomlinson GA, Rachlis AR, Rose DB, Dwosh HA, et al. Clinical features and short-term outcomes of 144 patients with SARS in the Greater Toronto Area. JAMA. 2003;289(21):2801-9. Available from: https://doi.org/10.1001/jama.289.21.JOC30885 4. Booth TF, Kournikakis B, Bastien N, Ho J, Kobasa D, Stadnyk L, et al. Detection of airborne severe acute respiratory syndrome (SARS) coronavirus and environmental contamination in SARS outbreak units. J Infect Dis. 2005;191(9):1472-7. Available from: https://doi.org/10.1086/429634 5. Burke RM, Midgley CM, Dratch A, Fenstersheib M, Haupt T, Holshue M, et al. Active monitoring of persons exposed to patients with confirmed COVID-19 — United States, January–February 2020. MMWR Morb Mortal Wkly Rep. 2020;69(9):245-6. Available from: http://dx.doi.org/10.15585/mmwr.mm6909e1 6. Chan JFW, Yuan S, Kok KH, To KK, Chu H, Yang J, et al. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: a study of a family cluster. Lancet. 2020;395(10223):514-23. Available from: https://doi.org/10.1016/S0140-6736(20)30154-9 7. Chen H, Guo J, Wang C, Luo F, Yu X, Zhang W, et al. Clinical characteristics and intrauterine vertical transmission potential of COVID-19 infection in nine pregnant women: a retrospective review of medical records. Lancet. 2020;395(10226):809-15. Available from: https://doi.org/10.1016/S0140-6736(20)30360-3 8. Chen L, Lou J, Bai Y, Wang M. COVID-19 disease with positive fecal and negative pharyngeal and sputum viral tests. Am J Gastroenterol. 2020 Mar 20 [Epub ahead of print]. Available from: https:/dx.doi.org/10.14309/ajg.0000000000000610 9. Chen N, Zhou M, Dong X, Qu J, Gong F, Han Y, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. 2020;395(10223):507-13. Available from: https://doi.org/10.1016/S0140-6736(20)30211-7 10. Chen R, Zhang Y, Huang L, Cheng BH, Xia ZY, Meng QT. Safety and efficacy of different anesthetic regimens for parturients with COVID-19 undergoing Cesarean delivery: a case series of 17 patients. Can J Anaesth. 2020 Mar 16 [Epub ahead of print]. Available from: https://doi.org/10.1007/s12630-020-01630-7 11. Cheng V, Wong S-C, Chen J, Yip C, Chuang V, Tsang O, et al. Escalating infection control response to the rapidly evolving epidemiology of the coronavirus disease 2019 (COVID-19) due COVID-19 – What We Know So Far About…Routes of Transmission 7
to SARS-CoV-2 in Hong Kong. Infect Control Hosp Epidemiol. 2020 Mar 5 [Epub ahead of print]. Available from: http://doi.org/10.1017/ice.2020.58 12. Dong L, Tian J, He S, Zhu C, Wang J, Liu C, et al. Possible vertical transmission of SARS-CoV-2 from an infected mother to her newborn. JAMA. 2020 Mar 26 [Epub ahead of print]. Available from: https://doi.org/10.1001/jama.2020.4621 13. Dowell SF, Simmerman JM, Erdman DD, Wu JS, Chaovavanich A, Javadi M, et al. Severe acute respiratory syndrome coronavirus on hospital surfaces. Clin Infect Dis. 2004;39(5):652-7. Available from: https://doi.org/10.1086/422652 14. European Centre for Disease Prevention and Control (ECDCa). Risk assessment: outbreak of acute respiratory syndrome associated with a novel coronavirus, China: first local transmission in the EU/EEA – third update [Internet]. Stockholm: ECDC; 2020 [cited 2020 Feb 12]. Available from: https://www.ecdc.europa.eu/en/publications-data/risk-assessment-outbreak-acute- respiratory-syndrome-associated-novel-1 15. European Centre for Disease Prevention and Control (ECDCb). Factsheet about Middle East respiratory syndrome coronavirus (MERS-CoV) [Internet]. Stockholm: ECDC; n.d. [cited 2020 Jan 27]. Available from: https://www.ecdc.europa.eu/en/middle-east-respiratory-syndrome- coronavirus/factsheet 16. Fan C, Lei D, Fang C, Li C, Wang M, Liu Y, et al. Perinatal transmission of COVID-19 associated SARS-CoV-2: should we worry? Clin Infect Dis. 2020 Mar 17 [Epub ahead of print]. Available from: https://doi.org/10.1093/cid/ciaa226 17. Guan W, Ni Z, Hu Y, Liang W, Ou C, He J, et al. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med. 2020 Feb 28 [Epub ahead of print]. Available from: https://doi.org/10.1056/NEJMoa2002032 18. Guo ZD, Wang ZY, Zhang SF, Li X, Li L, Li C, et al. Aerosol and surface distribution of severe acute respiratory syndrome coronavirus 2 in hospital wards, Wuhan, China, 2020. Emerg Infect Dis. 2020;26(7). Available from: https://doi.org/10.3201/eid2607.200885 19. Hosoda T, Sakamoto M, Shimizu H, Okabe N. SARS-CoV-2 enterocolitis with persisting to excrete the virus for about two weeks after recovering from diarrhea: a case report. Infect Control Hosp Epidemiol. 2020 Mar 19 [Epub ahead of print]. Available from: https://doi.org/10.1017/ice.2020.87 20. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395(10223):497-506. Available from: https://doi.org/10.1016/S0140-6736(20)30183-5 21. Huang R, Xia J, Chen Y, Shan C, Wu C. A family cluster of SARS-CoV-2 infection involving 11 patients in Nanjing, China. Lancet Infect Dis. 2020 Feb 28 [Epub ahead of print]. Available from: https://doi.org/10.1016/S1473-3099(20)30147-X 22. Imai N, Cori A, Dorigatti L, Baguelin M, Donnelly CA, Riley S, et al. Report 3: Transmissibility of 2019-nCoV [Internet]. London: Imperial College London; 2020 [cited 2020 Apr 22]. Available from: https://www.imperial.ac.uk/media/imperial-college/medicine/mrc-gida/2020-01-25- COVID19-Report-3.pdf COVID-19 – What We Know So Far About…Routes of Transmission 8
23. Kampf G, Todt D, Pfaender S, Steinmann E. Persistence of coronaviruses on inanimate surfaces and their inactivation with biocidal agents. J Hosp Infect. 2020;104(3):246-51. Available from: https://doi.org/10.1016/j.jhin.2020.01.022 24. Khan S, Peng L, Siddique R, Nabi G, Undefined N, Xue M, et al. Impact of COVID-19 infection on pregnancy outcomes and the risk of maternal-to-neonatal intrapartum transmission of COVID- 19 during natural birth. Infect Control Hospital Epidemiol. 2020 Mar 19 [Epub ahead of print]. Available from: https://doi.org/10.1017/ice.2020.84 25. Liu Y, Chen H, Tang K, Guo Y. Clinical manifestations and outcome of SARS-CoV-2 infection during pregnancy. J Infect. 2020 Mar 4 [Epub ahead of print]. Available from: https://doi.org/10.1016/j.jinf.2020.02.028 26. Lu C, Liu X, Jia Z. 2019-nCoV transmission through the ocular surface must not be ignored. Lancet. 2020;395(10224):e39. Available from: https://doi.org/10.1016/S0140-6736(20)30313-5 27. Lu J, Gu J, Li K, Xu C, Su W, Lai Z, et al. COVID-19 outbreak associated with air conditioning in restaurant, Guangzhou, China, 2020. Emerg Infect Dis. 2020;26(7). Available from: https://doi.org/10.3201/eid2607.200764 28. Lu R, Zhao X, Li J, Niu P, Yang B, Wu H, et al. Genomic characterisation and epidemiology of 2019 novel coronavirus: implications for virus origins and receptor binding. Lancet. 2020;395(10224):565-74. Available from: https://doi.org/10.1016/S0140-6736(20)30251-8 29. Ng K, Poon BH, Kiat Puar TH, Shan Quah JL, Loh WJ, Wong YJ, et al. COVID-19 and the risk to health care workers: a case report. Ann Intern Med. 2020 Mar 16 [Epub ahead of print]. Available from: https://doi.org/10.7326/L20-0175 30. Ong SW, Tan YK, Chia PY, Lee TH, Ng OT, Wong MS, et al. Air, surface environmental, and personal protective equipment contamination by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) from a symptomatic patient. JAMA. 2020 Mar 4 [Epub ahead of print]. Available from: https://doi.org/10.1001/jama.2020.3227 31. Otter JA, Donskey C, Yezli S, Douthwaite S, Goldenberg SD, Weber DJ. Transmission of SARS and MERS coronaviruses and influenza virus in healthcare settings: the possible role of dry surface contamination. J Hosp Infect. 2016;92(3):235-50. Available from: https://doi.org/10.1016/j.jhin.2015.08.027 32. Pan Y, Zhang D, Yang P, Poon LLM, Wang Q. Viral load of SARS-CoV-2 in clinical samples. Lancet Infect Dis. 2020;20(4):411-12. Available from: https://doi.org/10.1016/S1473-3099(20)30113-4 33. Pung R, Chiew CJ, Young BE, Chin S, Chen MIC, Clapham HE, et al. Investigation of three clusters of COVID-19 in Singapore: implications for surveillance and response measures. Lancet. 2020;395(10229):1039-46. Available from: https://doi.org/10.1016/S0140-6736(20)30528-6 34. Schneider E, Bermingham A, Pebody R, Watson JM. SARS, MERS, and other coronavirus infections. In: Heymann DL, editor. Control of communicable diseases manual. 20th ed. Washington, DC: American Public Health Association; 2016. COVID-19 – What We Know So Far About…Routes of Transmission 9
You can also read