NATIONAL ALCOHOL AND OTHER DRUG WORKFORCE DEVELOPMENT STRATEGY 2015-2018 - A SUB-STRATEGY OF THE NATIONAL DRUG STRATEGY 2010-15
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Intergovernmental Committee on Drugs National Alcohol and other Drug Workforce Development Strategy 2015–2018 A Sub-strategy of the National Drug Strategy 2010–15
Contents
Executive Summary iv Part 2: The Strategy 13
Part 1: The Context 1 Goals 13
Background 1 Outcome area 1: Understand the specialist AOD
prevention and treatment workforce 13
The impact of alcohol and other drug
problems in Australia 2 Outcome area 2: Create a sustainable specialist
AOD prevention and treatment workforce by
What is workforce development? 2
addressing recruitment and retention issues 14
Why have an Alcohol and other Drug
Outcome area 3: Match roles with
Workforce Development Strategy? 3
capabilities 17
Key principles underpinning the development
Outcome area 4: Enhance capacity to cater
of the AOD Workforce Development Strategy 4
for older AOD clients as well as those with
Who is the AOD workforce? 6 co-and multiple morbidities and other
Future challenges 8 complex needs 18
Outcome area 5: Improve child and family
sensitive practice 20
Outcome area 6: Improve consumer
participation in AOD service provision,
policy and planning 21
Outcome area 7: Increase the capacity of the
workforce to respond appropriately to AOD issues
among Aboriginal and Torres Strait
Islander peoples 23
Outcome area 8: Increase the capacity of the
workforce to respond appropriately to AOD issues
among culturally and linguistically diverse (CALD)
groups 25
Outcome area 9: Increase the capacity of the
workforce to respond appropriately to AOD issues
among lesbian, gay, bisexual, transgender and
intersex individuals 26
Outcome area 10: Enhance the capacity
of generalist health, community, welfare and
support services workers to prevent and
reduce AOD harm 27
Outcome area 11: Continue to develop the
criminal justice workforce to prevent
and reduce AOD harm 29
Outcome area 12: Promote the ability of the
education sector to prevent and reduce
AOD harm 31
NATIONAL AOD WFD STRATEGY 2015-2020 iiReferences 32 Appendix: Links to other Strategies 34 Glossary of Terms 40 Acknowledgements 42 iii NATIONAL AOD WFD STRATEGY 2015-2020
Executive Summary
This Strategy has been developed to support The Strategy’s 12 key Outcome Areas are to:
the National Drug Strategy at the request of
the Intergovernmental Committee on Drugs 1. Understand the specialist AOD prevention and
in recognition of the need for a national focus treatment workforce
on workforce development activities for the
2. Create a sustainable specialist AOD prevention
alcohol and other drug (AOD) workforce. The
and treatment workforce by addressing
Strategy development process was guided
recruitment and retention issues
by a Project Working Group appointed by the
Intergovernmental Committee on Drugs. It 3. Match roles with capabilities
followed an extensive consultation process
involving forums held in each jurisdiction, a written 4. Enhance capacity to cater for older AOD
submission process and key informant interviews. clients as well as those with co-and multiple
morbidities and other complex needs
The AOD workforce includes workers whose
5. Improve child and family sensitive practice
primary role involves reducing AOD-related harm
as well as those whose primary work focus is on 6. Improve consumer participation in AOD
other issues but, nevertheless, play an important service provision, policy and planning
role in reducing AOD harm. Consequently, this
document addresses the needs of workers from 7. Increase the capacity of the workforce to
the health, welfare, criminal justice and education respond appropriately to AOD issues among
sectors. These could be workers acting in paid or Aboriginal and Torres Strait Islander peoples
unpaid capacities. 8. Increase the capacity of the workforce to
respond appropriately to AOD issues
This document is a national policy framework
among culturally and linguistically diverse
that is complemented, supported and integrated
(CALD) groups
with a range of other existing national, state/
territory, government and non-government 9. Increase the capacity of the workforce to
strategies, plans and initiatives. The Strategy respond appropriately to AOD issues among
identifies key strategic action areas to enhance lesbian, gay, bisexual, transgender and
the capacities of Australia’s AOD workforce. intersex individuals
It is intended to be a strategic, rather than
operational, document. The Strategy will link with 10. Enhance the capacity of generalist health,
other work already underway and be used to community, welfare and support services
inform future activity. workers to prevent and reduce AOD harm
11. Continue to develop the criminal justice
The goals of the Strategy are:
workforce to prevent and reduce AOD harm
• To enhance the capacity of the Australian
12. Promote the ability of the education sector to
AOD workforce to prevent and minimise
prevent and reduce AOD harm
alcohol and other drug-related harm across
the domains of supply, demand and harm Responsibility for implementing the actions
reduction activities. outlined in the Strategy is shared by all
governments, recognising that jurisdictions face
• To create a sustainable Australian AOD
different challenges and will undertake actions in
workforce that is capable of meeting future
line with their own priorities, timing and resources.
challenges, innovation and reform.
NATIONAL AOD WFD STRATEGY 2015-2020 ivPART 1: The Context
Background The NDS addresses alcohol, tobacco, illegal
drugs, pharmaceuticals and other substances.
Alcohol and other drug (AOD)-related harm The approach of harm minimisation has guided
represents a significant social and economic the NDS since its inception in 1985. This
burden to the Australian community. encompasses the three pillars of:
Consequently, preventing and minimising this
• Demand reduction:
harm is an important national priority which
requires commitment from all levels of government »» preventing the uptake and/or delaying
and a range of sectors and agencies. The National the onset of use of alcohol, tobacco and
Alcohol and other Drug Workforce Development other drugs;
Strategy (NADWFDS) was developed at the »» reducing the misuse of alcohol and the
request of the Intergovernmental Committee use of tobacco and other drugs in the
on Drugs in recognition of the need to enhance community; and
the capacity of the diverse workforce involved in
preventing and responding to AOD-related harm. »» supporting people to recover from
dependence and reintegrate with the
The multi-level and intersectoral nature of community.
Australia’s approaches to preventing and
• Supply reduction:
minimising AOD-related harm is reflected in its
national framework for action on alcohol and »» preventing, stopping, disrupting or
other drugs, the National Drug Strategy 2010- otherwise reducing the production and
2015 (NDS) (Ministerial Council on Drug Strategy, supply of illegal drugs; and
[MCDS] 2011). The NDS provides an overarching »» controlling, managing and/or regulating
policy context for the NADWFDS. The Mission of the availability of legal drugs.
the NDS is:
• Harm reduction:
To build safe and healthy communities by
»» reducing the adverse health, social and
minimising alcohol, tobacco and other drug-
economic consequences of the use of
related health, social and economic harms
alcohol and other drugs.
among individuals, families and communities
(MCDS, 2011). These three pillars are underpinned by strong
commitments to supportive approaches which:
• build workforce capacity;
• promote evidence-based and evidence-
informed practice, innovation and evaluation;
• encourage performance measurement to
enhance quality; and
• build partnerships across sectors.
NATIONAL AOD WFD STRATEGY 2015-2020 1The impact of alcohol and other Tobacco smoking is one of the top risk factors for
chronic disease, including many types of cancer,
drug problems in Australia respiratory disease and heart disease. Likewise,
illegal drugs can not only have dangerous health
Alcohol and other drug-related harm places a high
impacts, but are a significant contributor to crime.
burden on the Australian community. The cost of
Unsafe injecting drug use is also a major driver of
harmful alcohol, tobacco and other drug use in
blood-borne virus infections such as hepatitis C
2004–05 was estimated at $56.1 billion, of which:
and HIV/AIDS.
• Tobacco accounted for 56%;
In light of these substantial costs, it is important
• Alcohol accounted for 27.3%; and that Australia has a workforce with the capability
to prevent and reduce this harm.
• Illegal drugs accounted for 14.6%
(Collins & Lapsley, 2008).
In 2004-05 in Australia, there were: What is workforce
development?
• 3,494 deaths attributable to alcohol;
Workforce development (WFD) in the AOD field
• 15,050 deaths attributable to tobacco; and
aims to build the capacity of organisations and
• 872 deaths attributable to illicit and other individuals to prevent and respond to AOD-
drugs (Collins & Lapsley, 2008). related problems and to promote evidence-
based practice. It goes beyond the provision of
Alcohol and other drug-related harm does not education and training to include issues such as
only accrue to those using these substances. In recruitment and retention, workforce planning,
2005 an estimated: professional and career development and worker
wellbeing. As such, WFD can be defined as:
• 367 people died and almost 14,000 people
were hospitalised because of another’s alcohol …a multi-faceted approach which addresses the
consumption; range of factors impacting on the ability of the
workforce to function with maximum effectiveness
• 77 deaths stemmed from alcohol-related in responding to alcohol and other drug-related
violence attributable to another’s alcohol problems. Workforce development should have a
consumption systems focus. Unlike traditional approaches, this
• 277 people aged 15 years and over died as a is broad and comprehensive, targeting individual,
result of another’s drinking and driving; and organisational and structural factors, rather than
just addressing education and training of individual
• 70,000 Australians were victims of alcohol- mainstream workers (Roche, 2002a).
related assault, of whom 24,000 were victims
of alcohol-related domestic violence (Laslett et This broad definition of WFD mandates a focus
al., 2010). on a wide range of individual, organisational,
structural and systematic factors that impact on
In addition, an estimated 20,000 children across the ability of the workforce to effectively prevent
Australia were victims of substantiated alcohol- and respond to AOD issues. Without addressing
related child abuse or neglect in 2006/07 (Laslett these underpinning and contextual factors,
et al., 2010). Other alcohol-related harms include the ultimate aim of increasing the workforce’s
road and other accidents, domestic and public effectiveness is unlikely to be achieved
violence, crime, chronic disease, birth defects and (Roche & Pidd, 2010).
disability, family breakdown and broader social
dysfunction.
2 NATIONAL AOD WFD STRATEGY 2015-2020Why have an Alcohol and other that develops the capacity of the workforce to
effectively respond to current and emerging AOD
Drug Workforce Development issues. A number of jurisdictions in Australia have
Strategy? considered and/or developed AOD Workforce
Development Strategies. There is not, however, a
Practices aimed at preventing and responding nationally consistent approach to addressing the
to AOD harm need to continuously evolve in challenges facing the AOD workforce.
response to changes in societal needs and
advances in knowledge. In recent decades, shifts A WFD strategy can also help to:
have occurred in patterns of consumption and
• Identify the workforce implications of the
the types of substances consumed. Advances
current strategic and operational environment;
in knowledge have also led to changes in clinical
practice and prevention strategies. These include: • Enhance the professionalisation of the
workforce;
• Shifting patterns of use, particularly poly-drug
use; • Meet current needs and prepare for the future;
• New psychoactive substances; • Raise the profile of strategic workforce
planning within organisations and influence
• An expanded range of pharmacotherapies change from the top down;
and other treatment options;
• Integrate workforce planning with future
• Greater awareness of co-existing mental directions for organisations and sectors;
health disorders and multiple morbidities
(especially in the context of an ageing • Assess the current state of the workforce;
population); • Facilitate the seamless movement of AOD
• Greater awareness of foetal alcohol spectrum workers within and across jurisdictions as a
disorder, child protection and family sensitive result of more standardised qualifications;
practice issues; • Create, drive and implement workforce
• Problematic use across a widened age planning;
spectrum;
• Improve performance;
• Greater emphasis on cost efficiency,
professional practice efficacy, improved • Enhance service quality and outcomes;
outcomes and intersectoral collaboration;
• Enhance career development options; and
• A better understanding of effective preventive
measures; and
• Optimise implementation of evidenced based
• Greater recognition of the wide variety of practice.
workers involved in reducing AOD-related
harm. Another aim of the Strategy development process
is to achieve general agreement about the future
Factors such as these increase the demand directions of workforce development in the AOD
to prevent and respond to AOD problems. As field, which will shape practice in this area and
a result, there is growing recognition of the be reflected in service tendering processes and
need for a workforce development approach funding agreements.
NATIONAL AOD WFD STRATEGY 2015-2020 3Key principles underpinning 4. While recognising that a broad range of
workers have a role in reducing AOD harm the
the development of the AOD primary focal point of the Strategy is on the
Workforce Development workforce development needs of specialist
AOD workers.
Strategy
The development of the NADWFDS has been The scope of the Strategy includes a wide
predicated on a number of principles. Specifically: range of workers with a role in reducing AOD-
related harm. Nevertheless, having a highly
1. The Strategy should reflect the National Drug skilled specialist prevention and treatment
Strategy’s overarching approach of harm workforce is fundamental to positively
minimisation and address its three pillars of influencing the activities of generalist workers
supply reduction, demand reduction and harm (i.e. those whose primary role is not reducing
reduction. AOD related harm). From this perspective, the
role of the specialist workforce is not only to
Australia’s National Drug Strategy adopts a provide specialist services, but also to support
balanced approach to reducing AOD harm non-specialists.
involving the three pillars of supply, demand
5. The reduction of AOD harm in Australia will be
and harm reduction. It is therefore important
optimised by having a workforce engaged in
that the NADWFDS reflects the National Drug
evidence-based practice.
Strategy’s balanced approach to reducing
AOD-related harm.
The evidence base concerning effective
2. The Strategy should have a systems focus practice in preventing and responding to AOD
which addresses the range of factors harm continues to grow. The Strategy should
impacting on the ability of the workforce to therefore promote strategies to enhance the
prevent and reduce alcohol and other drug- uptake of these evidence-based practices.
related problems.
6. Workforce planning and development
in the AOD field should be built on a
Using a systems approach will enable the
comprehensive understanding of the national
Strategy to move beyond a simple focus on
workforce including demographics, roles and
education and training to include the wide
qualifications as well as modelling of future
range of factors which impact on workforce
demand.
effectiveness.
3. The Strategy should be developed following Considerable work has been undertaken in
an extensive consultation process. workforce development as well as workforce
planning activities and it is important to
The Strategy was developed following build on this and increase our knowledge
consultation involving: and understanding of the specialist AOD
workforce.
• Forums held in each state and territory;
7. The key driver of the AOD Workforce
• A written submission process; and Development Strategy is enhancing the quality
of AOD service provision.
• Key informant interviews.
Having a skilled, professional and adaptable
AOD workforce is essential to enhancing the
quality of AOD services in Australia.
4 NATIONAL AOD WFD STRATEGY 2015-20208. The Strategy should recognise the diversity, and demand for workers; the emergence of new
acknowledge the contribution of the totality of substances of concern; the need to link with
the workforce with a role in reducing AOD harm other agencies and sectors to meet the needs
regardless of roles, professional qualifications, of clients with complex needs; and changes
or whether paid or unpaid. in funding arrangements. In addition, future
prevention and intervention efforts are likely to
A broad range of workers have a role in involve greater attention directed towards the
reducing AOD harm in Australia. These include social determinants of AOD problems. The
workers from the health, welfare and criminal Strategy should aim to provide a foundation
justice sectors. The AOD sector itself is also for the AOD workforce to meet these
diverse, with workers from many different challenges.
backgrounds. For example, those with
professional training in a range of disciplines, 11. In recognition of the often complex needs of
those with vocational or on-the-job training, individuals experiencing AOD-related harm
and those with lived experience of recovery and their families, the Strategy should foster
from AOD dependence. Each group has enhanced cooperation between sectors and
unique needs that warrant attention in the agencies.
Strategy.
Alcohol and other drug treatment services
9. The Strategy should provide a framework for cannot effectively meet all the needs of clients
national AOD workforce development while with multiple morbidities. For this reason,
recognising jurisdictional differences and agencies will require new ways of working that
facilitating innovation. cater for these complex needs.
Alcohol and other drug workforce 12. The Strategy should focus on building
development efforts in Australia cannot be capacity in specific areas of need.
undertaken without cognisance of the sector’s
history. There are already many effective Alcohol and other drug related harm
jurisdictionally-based initiatives in place, upon differentially impacts groups of Australians.
which the Strategy can build. In addition there Some groups, such as Aboriginal and Torres
are historical variations between jurisdictions Strait Islander peoples, lower socio-economic
and complex differences in funding groups and children living in families in which
arrangements which can impact the provision AOD-related harm is occurring, experience
of AOD services in different jurisdictions greater levels of harm. The Strategy should
(Chalmers, Ritter, & Berends, 2013). All these therefore focus on these areas of need.
factors were be taken into consideration in the 13. Reducing AOD harm among Aboriginal and
Strategy’s development. The Strategy should Torres Strait Islander peoples is dependent
also not be so restrictive as to stifle innovation on recognising that Aboriginal and Torres
in approaches to preventing and reducing Strait Islander culture is a source of strength,
AOD harm. resilience, happiness, identity and confidence.
10. The Strategy should reflect a range of future
trends and challenges likely to impact on the The promotion and protection of culture
AOD workforce into the future. is critical to progressing improvements in
Aboriginal and Torres Strait Islander health and
It is evident that a range of issues will impact is inextricably linked to health and wellbeing. In
on the AOD workforce into the future. These order to reduce AOD harm among Aboriginal
include: an ageing population; an ageing and Torres Strait Islander peoples, the
AOD workforce in the context of increasing Australian AOD workforce must be responsive
NATIONAL AOD WFD STRATEGY 2015-2020 5to cultural differences and the impacts of government, not-for-profit (non-government) and
racism (conscious and unconscious) and a lack private sectors. Specialist AOD workers are the
of cultural safety1 on Aboriginal and Torres Strait primary focus of the NADWFDS.
Islander peoples. Aboriginal and Torres Strait
Islanders are also more likely to access, and Generalist workers are employed in the
will experience better outcomes from, services mainstream workforce and have non-AOD-related
that are respectful and culturally safe (Australian core roles, but nonetheless can prevent and
Indigenous Doctor’s Association, 2013). minimise AOD harm. Examples include:
• The criminal justice workforce, including the
Who is the AOD workforce? court system, police2, Aboriginal and Torres
Strait Islander law enforcement and community
The NDS recognises that an appropriately skilled
liaison officers and correctional officers;
and qualified workforce is critical to preventing
and responding to AOD-related harm. The NDS • Emergency medical services, paramedics and
also highlights that a broad range of workers are emergency department personnel;
involved in preventing and minimising AOD harm.
However, there is currently limited information • The mental health workforce;
concerning the characteristics of the AOD • The broader health and medical workforce
workforce in Australia. A primary goal of the including general practitioners, other primary
Strategy is to gain a better understanding of the healthcare workers and hospital workers;
extent and nature of the AOD workforce.
• Community, welfare and support services
The AOD workforce is commonly considered in including those working with culturally and
terms of two main components, specialists and linguistically diverse communities, in child
generalists. protection, in disability support services, and
in the homelessness, unemployment, income
Specialist AOD workers are those whose core support and youth sectors;
role involves preventing and responding to AOD
harm. They include AOD workers, nurses, social • Pharmacists and the pharmacy workforce;
workers, doctors, peer workers, needle and
• The aged care sector; and
syringe program workers, prevention workers,
addiction medicine specialists and specialist • The education sector.
psychologists and psychiatrists. These workers
As is evident, there is a diverse range of workers
may be employed in AOD specialist organisations
involved in preventing and responding to AOD
or in AOD programs within non-specialist
harm in Australia across the supply, demand and
organisations (Roche & Pidd, 2010). They may
harm reduction domains. It is important that the
have specialised degrees or little or no formal
Strategy addresses this diversity and focusses
training (Libretto, Weil, Nemes, Copeland Linder,
attention on the developmental needs of each
& Johansson, 2004), and can be employed in the
group. The levels of prevention and response
activities can be categorised into four tiers.
1
Cultural safety refers to the accumulation and application Generalist and specialist workers have roles
of knowledge of Aboriginal and Torres Strait Islander values, across these tiers (see Figure 1.).
principles and norms. Aboriginal and Torres Strait Islander
AOD workers are more likely to stay and thrive in learning
and working environments that consistently demonstrate
cultural safety. Aboriginal and Torres Strait Islander AOD
professionals’ experiences of a lack of cultural safety, racism 2
It is important to note that some police have highly specialised
and discrimination significantly detract from their mental health AOD functions. This includes those involved in drug investigations,
and wellbeing and negatively impact on their job satisfaction the policing of licensed premises and in AOD-related aspects of
(Australian Indigenous Doctor’s Association, 2013). road safety (such as random AOD screening and testing).
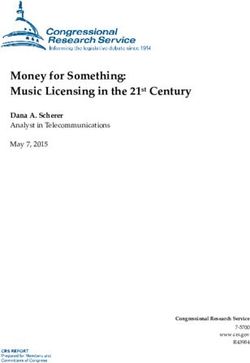
6 NATIONAL AOD WFD STRATEGY 2015-2020Whole of population focus, prevention, social
Tier 1 determinants, education, law enforcement,
community services
Tier 2 Primary healthcare, community services, information
services, NSP’s peer support, self help groups
Tier 3 Specialist assessment and referral, corrections,
case management, relapse prevention, community
pharmacotherapy, counselling
Tier
4 Services for people with complex needs,specialist
withdrawal management, residential rehab
Figure 1: Tiers of activity involving different services/workers.
Based on these tiers it is possible to identify the ways in which different occupational groups make their
contributions to preventing and reducing AOD-related harm (see Figure 2).13
Education
Emergency
and Welfare workers
Police
Corrections
Pharmacy workers
Mental Health
Specialist AOD, Clinical and Prevention Workers
Tier 1: Whole of population focus,
services
medical
prevention, social determinants, education,
Generalist health
law enforcement, community services.
Tier 2: Primary healthcare, community
services, information services, NSPs, peer
support, self-help groups.
Tier 3: Specialist assessment and referral,
corrections, case management, relapse prevention,
community pharmacotherapy, counselling.
Tier 4: Services for people with complex needs,
specialist withdrawal management, residential
rehab.
Figure 2: Tiers of activity in which different occupational groups make their contribution to
reducing AOD-related harm.
3
Figures 1 and 2 are intended to be indicative, rather than definitive, as services may have different roles in different tiers at different
times.
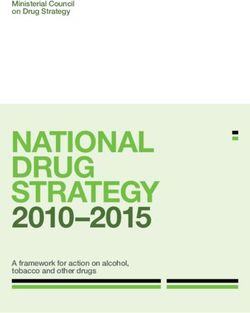
NATIONAL AOD WFD STRATEGY 2015-2020 7Tier 4: Inpatient Detox,
Residential rehab
Tier 1: Whole of population
Client
Tier 3: Specialist assessment,
case management
Tier 2: Primary Health Care, Community
Services Needle and syringe programs,
peer support
Figure 3: Wrap-around services, particularly for clients with complex needs.
It is important to note that individuals may receive non-communicable diseases (World Health
services from multiple providers working within or Organization, 2011), along with ageing, fertility and
across multiple tiers at the one time (see Figure mortality trends. If, as predicted, baby boomers
3). Indeed this ‘wrap around’ approach can be an have greater rates of lifetime alcohol and drug use
important part of service provision for individuals than previous generations, this will lead to more
with complex needs. older people experiencing AOD harm in the future
(Hunter, Lubman, & Barratt, 2011). This trend will
Future challenges require a better understanding of the physiological
and psychological impact of drug use in ageing
The development of the Strategy occurred in the populations (Colliver, Compton, Gfroerer, &
context of a range of challenges which will be Condon, 2006). The ageing population also
facing the AOD workforce into the future. These means that programs will be required to prevent
challenges and their implications are explored in harmful AOD use among older Australians.
more detail below.
The ageing of the population has particular
The ageing population significance for Aboriginal and Torres Strait
Australia’s population, like that of most developed Islander Australians who have a shorter than
countries, is ageing as a result of sustained low average life expectancy. Many chronic illnesses
fertility and increasing life expectancy (Australian (including those stemming from harmful AOD use)
Bureau of Statistics, 2011). This has major that are often evident among older Australians
implications for the NADWFDS. are common in middle age among Aboriginal
and Torres Strait Islander peoples. Therefore,
Health and welfare professionals and workforces services focussed on meeting the needs of older
(including those focussing on reducing AOD Australians experiencing AOD harm also need to
harm) need to be better equipped to deal target middle aged Aboriginal and Torres Strait
with a dramatic increase in the incidence of Islander people.
8 NATIONAL AOD WFD STRATEGY 2015-2020Different substances and patterns of use Smart drugs are a further issue on the horizon.
These are prescription drugs used to treat
The landscape of available psychoactive
conditions such as attention deficit hyperactivity
substances is rapidly changing. In Europe
disorder, narcolepsy and Alzheimer’s disease.
new psychoactive substances are reported to
When used by healthy people they may improve
authorities at a rate of approximately one per
cognitive functions (Partridge, Bell, Lucke, Yeates,
week (European Monitoring Centre for Drugs and
& Hall, 2011). The harmful use of these powerful
Drug Addiction, 2012). These trends are highly
medicines could significantly impact on AOD
likely to impact Australia because the Internet
treatment services in the future.
has increased the flow of information about these
drugs, and provides a means through which they New paradigms and treatments
can be purchased (European Monitoring Centre
for Drugs and Drug Addiction, 2012). This is In the future, approaches to preventing and
likely to present particular difficulties for treating responding to AOD problems are likely to arise
individuals who experience acute and chronic from a much broader foundation. Dealing with
harms stemming from the use of these drugs, the end results of problematic substance use will
because the nature of the substance they have always be important, and there will always be a
taken can be unclear to both the client and the role for specialist treatment services. However,
treating clinician (Arnold, 2013). future responses will be shaped by drivers that
extend this orientation, including increased
Furthermore, over the past decade there emphasis on the prevention and treatment
have been significant changes in the profile of implications of:
substances for which Australians are seeking
treatment. Since 2001-02, among publically • Social determinants of health (e.g. early life
funded AOD treatment episodes in which the experiences, work, unemployment, social
client was seeking help for their own problems: exclusion) which will feature more prominently
in our understanding of causal factors as
• Alcohol problems increased from 37 to 47%; well as response strategies to ameliorate
and problems;
• Heroin problems halved from 18% to 9% • Integrated models of care (mental health,
(Australian Institute of Health and Welfare, aged care, child and family, Aboriginal and
2012). Torres Strait Islanders, prisoners, non-English
Prescription drugs such as smart drugs, opioids, speaking) will become more prominent as
antipsychotic medicines and sedative hypnotics pressure and expectations grow for more
as well as performance and image enhancing coordinated and holistic care;
drugs have the potential to displace the demand • Complex health and comprehensive
for illicit drugs. This will require quite different community services models; no longer will
responses from AOD treatment and prevention narrow and simplistic models be adequate
services, and has important implications for the (Roche, 2013); and
development of the AOD workforce (Roche,
2013). In the past twenty years, for example, • Technology-based approaches to treatment
there has been a dramatic increase in the (Cunningham, Kypri, & McCambridge, 2011).
prescribing of pharmaceutical opioids in Australia The development of a Quality Framework for
and correspondingly increasing harms (Royal Australian Government funded drug and alcohol
Australasian College of Physicians, 2009). treatment services, funded by the Australian
Government Department of Health, is also likely to
NATIONAL AOD WFD STRATEGY 2015-2020 9influence future directions and standards in AOD disadvantage, and needs to be understood in the
service provision in Australia. The project aims to context of a history of dispossession, denial of
develop a quality framework for alcohol and other culture, and conflict (Gleadle et al., 2010).
drugs treatment services that:
Aboriginal and Torres Strait Islander AOD
• Complements other models/frameworks that workers play an important role in preventing and
services currently comply with; responding to AOD-related harm among this
population, and are critically important in the
• Is adaptable, flexible and suitable for a range context of the NADWFDS. Nevertheless they
of service types and settings, including cannot bear total responsibility for addressing
Indigenous-specific services; AOD-related harm among Aboriginal and Torres
Strait Islander peoples. Aboriginal and Torres
• Considers clients with comorbidity and the
Strait Islanders seeking treatment for their AOD
need to build and/or maintain capacity of
problems may not have the option of accessing
services to appropriately manage these
an AOD service established to cater for their
clients;
needs. Even in Aboriginal and Torres Strait
• Considers all funding sources for services Islander-specific services, not all AOD workers
including client/patient contributions; are Indigenous. Consequently, these clients are
highly likely to have contact with non-Aboriginal
• Clearly describes the expected quality and Torres Strait Islander service providers. From
standards for each service type; this perspective, it is critically important that all
• Has clear guidelines, policies and procedures AOD workers, regardless of their own Indigenous
to support the achievement and maintenance status, are capable of preventing and responding
of these quality standards; to AOD harm among Aboriginal and Torres
Strait Islander Australians in a culturally safe and
• Allows incorporation of accreditation models sensitive manner.
that services currently have in place or may
have in place in the future; and Aboriginal and Torres Strait Islander AOD workers
are usually employed in comparatively low status,
• Considers related aspects such as lower paid positions such as Health Workers or
accreditation and minimum qualifications. community workers (Gleadle et al., 2010). Against
a background of disadvantage and complex AOD
Additionally, the project will aim to provide
use, these AOD workers face unique stressors
a detailed draft implementation plan for the
including:
framework, with recommendations drawn from
the project and other information that informs use
• Heavy work demands and a lack of clearly
and future development needs.
defined roles and boundaries reflecting high
The needs of Aboriginal and community need and a shortfall of Aboriginal
Torres Strait Islander Australians and Torres Strait Islander AOD workers;
Aboriginal and Torres Strait Islander Australians • Dual forms of stigmatisation stemming from
have higher rates of tobacco and other drug use attitudes to AOD work and racism;
compared to the non-Indigenous population.
• Difficulties translating mainstream work
Alcohol and other drug use by Aboriginal and
practices to meet the specific needs of
Torres Strait Islander Australians contributes
Aboriginal and Torres Strait Islander clients;
to compromised physical and psychosocial
health status and ongoing socio-economic • Challenges of isolation when working in
remote areas;
10 NATIONAL AOD WFD STRATEGY 2015-2020• Dealing with clients with complex Increased emphasis on service outcomes
comorbidities and health and social issues;
Future service funding is likely to be increasingly
and
linked to agencies’ ability to deliver demonstrable
• Lack of cultural understanding and support outcomes for clients and the broader community.
from non-Indigenous health workers (Roche, Outcomes in relation to prevention and treatment
Nicholas, Trifonoff, & Steenson, 2013). and recovery are as yet undefined. The
implications of a movement towards outcomes-
These challenges mean that Aboriginal and
based funding extend beyond changes in service
Torres Strait Islander AOD workers have distinct
provision. Such a movement will also mean that
workforce development needs, and that WFD
the AOD sector will need to be more familiar with
strategies are required that can be implemented
the collection, interpretation and presentation of
in a culturally safe manner.
data in order to ensure continued funding. It will
Responding to multiple morbidities also be important to ensure that outcomes focus
on the characteristics and clients of individual
Individuals experiencing AOD harm are at risk services, so as not to disadvantage programs
of a range of comorbid conditions including which cater for clients with more entrenched
infectious and non-communicable diseases problems.
(Australian Government Preventative Task Force,
2009). Mental illnesses are a particularly prevalent Increasing consumer input into their own
comorbidity among AOD clients. treatment and care
The appropriate management of long-term Consumer input into service provision is an
multi-morbid disorders is a key challenge for important part of providing person-centred
health systems internationally. It is increasingly care. The challenge for the AOD sector is to
apparent that multi-morbidities are the norm for turn widespread acceptance of the principle
people with chronic health problems, particularly of service user participation into processes
the most socio-economically disadvantaged. and resourcing that make it both feasible and
Co-and multiple morbidities have important effective. As well as involvement in service
implications for the training and structure of the planning, clients should have:
AOD workforce. Strategies such as co-location, • Improved knowledge and confidence to make
multi-disciplinary health professionals and teams, choices about their treatment and awareness
inter-professional education and cross sectoral of how to self-manage after formal treatment;
workforce development will increasingly be
required. • High levels of active involvement in their
treatment including planning, setting goals and
This issue will become a growing challenge decision making; and
for AOD service provision in the future. AOD
services will need to develop ways of meeting • A comprehensive assessment and care
the multi-morbidity needs of their clients through plan that is oriented towards their goals
a combination of enhanced generalist in-house and designed with them according to their
service provision and enhanced linkages with choices, preferences and changing needs
other service providers. This ‘no wrong door’ (Department of Health Victoria, 2012).
approach means that regardless of where clients
with complex needs present they can obtain the
services they require.
NATIONAL AOD WFD STRATEGY 2015-2020 11Child and family sensitive Differences between government
policy and practice and non-government sectors
The AOD, family and child welfare sectors In some jurisdictions there are significant
have increasingly recognised the relationship differences in workforce profiles between
between AOD problems, child and adolescent government and non-government organisations
development, and child wellbeing and protection. (NGOs) (Roche & Pidd, 2010). Some of these
Child and family sensitive policy and practice differences are due to alternative service delivery
involves raising awareness of the impact of models, different funding levels and different client
substance use problems upon families, addressing groups. As a result, workforce development
the needs of families (Addaction, 2009), and issues may be different for NGO and government
seeing the family-rather than an individual adult workforces. This, in turn, has workforce
or child-as the unit of intervention. It includes development implications (Duraisingam, Pidd,
identifying and addressing the needs of adult Roche, & O’Connor, 2006). In several jurisdictions
clients as parents, as well as the needs of their there are also significant disparities between
children, as part of prevention, treatment and salaries and conditions offered by NGO agencies
intervention processes, in order to ensure that as and public sector agencies. Staff employed by
parents they are supported and child wellbeing NGO agencies are generally paid considerably
and safety is maintained (Battams & Roche, 2010). less due to funding arrangements and differences
in awards (Roche & Pidd, 2010). This can lead
Workforce-related challenges to a workforce drain from the NGO to the public
The AOD workforce faces a number of future sector, with the NGO sector bearing a significant
challenges which impact on the development of burden for recruiting and training new entrants to
NADWFDS. the AOD workforce.
Ageing workforce
As a result of an ageing population, demand for
workers in health care and social assistance in
Australia will outstrip all other sectors over the next
few years (Community Services & Health Industry
Skills Council, 2013) which will increase pressure
on AOD services to attract and retain suitable
staff. This will be particularly relevant for medical
practitioners and nurses (Australian Bureau of
Statistics, 2003). As older workers retire, the
human services workforce is likely to be negatively
impacted by a loss of highly skilled workers. This
means that the AOD sector will continue to age
and will have to compete with other sectors for
staff in an increasingly difficult human resource
environment. Furthermore, the demand for
workers will not be confined to Australia. As the
human services workforce becomes increasingly
globalised, AOD agencies will be required to
compete with other countries for staff.
12 NATIONAL AOD WFD STRATEGY 2015-2020Part 2: The Strategy
The Strategy addresses a broad range of factors Some jurisdictions have undertaken surveys
designed to improve the quality and functioning of their AOD workforces, but these are often
of the AOD sector and systems responses. It confined to either government or non-government
contains a series of suggested actions which sectors. In addition, they also do not always
jurisdictions may take to implement the goals of include data on individuals employed in prevention
the Strategy. Jurisdictions already have a range of roles, peer workers or needle and syringe
measures in place and face different challenges. workers. Differing criteria and terminology also
It is therefore anticipated that jurisdictions will mean that findings may not be comparable
undertake actions in line with their own priorities, between jurisdictions.
timing and resources.
There is a need to continue to work across
jurisdictions to strengthen the knowledge
Goals: base required for workforce development
and planning. This includes issues such as
To enhance the capacity of the Australian AOD employee demographics, qualifications, roles
workforce to prevent and minimise alcohol and and employment intentions. Data is also needed
other drug-related harm across the domains of about specialist workers within non-specialist
supply, demand and harm reduction activities. organisations.
To create a sustainable Australian AOD workforce Once obtained, this information could be linked
that is capable of meeting future challenges, of to the results of work currently being undertaken
innovation and reform. to estimate AOD treatment demand such as the
Drug and Alcohol Clinical Care & Prevention (DA-
CCP) project. The DA-CCP project aims to:
Outcome areas
Outcome area 1: Understand the specialist • Build the first national population-based model
AOD prevention and treatment workforce for AOD service planning by estimating the
need and demand for services;
Considerable work has already been undertaken
in workforce development and planning, and • Use clinical evidence and expert consensus
it is important to build on this and increase our to specify the care packages required by
knowledge and understanding of the specialist individuals and groups;
AOD workforce. To be able to conduct effective
• Calculate the resources needed to provide
workforce development and planning, information
these care packages; and
on three issues is required:
• Provide an AOD service planning tool
• The existing workforce and their
for jurisdictions. (e.g. Ritter, Chalmers, &
characteristics;
Sunderland, 2013).
• The demand for the workforce; and
• Entries to and exits from the workforce (Health
Workforce Australia, 2013).
NATIONAL AOD WFD STRATEGY 2015-2020 13Actions could include: Outcome area 2: Create a sustainable
• Developing a nationally agreed taxonomy specialist AOD prevention and treatment
of specialist AOD prevention and treatment workforce by addressing recruitment and
roles as a basis for systematic workforce retention issues
enhancement and workforce development. The demand for workers in the health and
welfare sectors is projected to increase
• Undertaking a national census of workers
substantially (Community Services & Health
employed in specialist AOD prevention and
Industry Skills Council, 2013). Consequently, the
treatment roles, including those working in
AOD sector will be competing for workers with
non-specialist organisations. The census
other Australian health and welfare agencies.
should utilise the nationally agreed data
Globalisation of the health and welfare workforce
definitions, and be supplemented with other
will also result in international competition for
sources of data such as that provided by
staff. The recruitment and retention of specialist
Health Workforce Australia, the Australian
staff in the AOD sector is therefore a critical
Bureau of Statistics and peak bodies. As
issue. While there are significant gaps in our
well as basic demographic/occupational
understanding of the characteristics of the AOD
data, the census should collect information
specialist workforce, it is understood that:
on issues such as employment intentions,
Indigenous status, ethnicity and language • The majority are female;
skills. This information could be collated to
create a comprehensive picture of the current • The majority are aged 45 years or older; and
workforce. • Approximately one third are employed part
time (Roche & Pidd, 2010).
• Using this workforce data along with
projections of treatment demand to enhance Recruitment and retention strategies should be
workforce planning and identify workforce based on consideration of these demographic
needs. characteristics and refined as more detailed
information becomes available. Effective
• Encouraging all jurisdictions to consistently strategies are particularly important in rural and
adopt the workforce census data definitions remote areas and for medical and nursing staff.
in all future workforce development surveys
and analyses to enable ongoing workforce
monitoring and mapping.
Actions could include:
Key Performance Indicators could include: Improving recruitment into specialist AOD roles
• Nationally consistent terminology to describe by:
the roles of the specialist AOD prevention and
treatment workforce. • Developing and implementing measures to
reduce the stigma associated with working
• Comprehensive knowledge of the extent and within the AOD sector;
nature of the specialist AOD prevention and
• Investigating the value of registration or
treatment workforce.
credentialing for the AOD sector to enhance
its professionalism and desirability;
14 NATIONAL AOD WFD STRATEGY 2015-2020• Promoting the AOD sector as a career of • Exploring alternative pathways through which
choice for suitable individuals via marketing medical graduates can become Fellows of the
to universities and vocational education Chapter of Addiction Medicine which do not
institutions (particularly in schools of medicine, require basic physician training, or fellowship
psychology, public health/policy, nursing; of other colleges; and
occupational therapy and social work);
• Examining current supervisory arrangements
• Increasing opportunities for placements for trainees enrolled in the Royal Australian
in AOD settings during vocational, and New Zealand College of Psychiatrists
undergraduate and post graduate education; Certificate in Addiction Psychiatry to determine
the viability of broadening the range of
• Better defining career pathways for workers in
potential supervisors.
prevention roles;
Improving specialist workforce retention by
• Develop clear articulation pathways (within enhancing the availability of:
and between vocational education and training
(VET) and higher education systems) to ensure • Flexible working arrangements (part time work,
that workers have access to qualifications that position sharing, time-in-lieu and working from
enable career progression within the AOD home);
field. This will include the mapping of entry
• Flexible access to education and training
points for workers from associated fields;
opportunities including enhanced use of on-
• Enhancing early exposure to drug and alcohol line learning and other technologies;
nursing as a career path among nursing
• Parental leave;
students and graduates;
• Comprehensive orientation programs to
• Expanding the number of AOD nurse
support transition into the sector;
practitioner positions available and developing
a structured career pathway for progression • Mentoring and clinical supervision programs;
into nurse practitioner positions;
• Meaningful career pathways which do not
• Enhancing early exposure to addiction medicine necessarily require clinicians to move into
as a career path among medical students management roles in order to gain promotion;
and junior medical officers by increasing
opportunities for placements/rotations through • Strategies to facilitate re-entry of former
addiction medicine specialty areas; specialist AOD workers;
• Increasing AOD teaching in undergraduate • Roles for experienced workers which focus
clinical and public health/policy tertiary on expanding their skills into more clinically
courses; complex areas or mentoring and transferring
their skills;
• Establishing a critical mass of addiction
medical specialists to enable vertical • Management and leadership development
integration of teaching involving medical programs focussing on responding to the
students, interns/junior medical officers, needs and expectations of the workforce;
registrars and consultants;
NATIONAL AOD WFD STRATEGY 2015-2020 15• Pay increments related to competency/ • Percentage of agencies providing specialist
qualification acquisition as appropriate; AOD prevention and treatment services that
report they are able to attract and retain
• Opportunities for service linked scholarships
requisite staff.
and education cost payments;
• Appropriate turnover rates in specialist AOD
• Employment exit interviews/surveys to better
prevention and treatment services.
understand the reasons for leaving the AOD
sector; • Percentage of specialist AOD prevention
and treatment staff receiving mentoring and
• Portability of long service and sick leave
support.
entitlements as workers move between
agencies; • Career paths defined and expanded for AOD
workers.
• Enhanced job security via longer-term
employment contracts/permanent positions; • Career satisfaction enhanced and stress and
burnout rates minimised among specialist
• Succession planning for staff and
AOD prevention and treatment staff.
management;
• Measures to assist existing staff to embrace
new technologies and new philosophies;
• Medicare Benefits Schedule items for
professional attendances provided by
addiction medicine specialists to ensure that
services provided by these specialists attract
equivalent remuneration to similar medical
specialties;
• Medicare Benefits Schedule items for
professional services provided by AOD nurse
practitioners;
• Appropriate medical officer career structures
in the public and private sectors which
combine teaching, clinical research and public
health roles to make the addiction medicine
speciality more attractive; and
• Mechanisms to showcase the achievements
of the sector.
Key Performance Indicators could include:
• Number of long-term filled positions in
agencies providing specialist AOD prevention
and treatment services.
• Level of available mentoring, clinical
supervision and appraisal programs.
16 NATIONAL AOD WFD STRATEGY 2015-2020Outcome area 3: Match roles with Actions could include:
capabilities • Formulating a workforce development
The AOD field involves a diverse range of roles, matrix which includes the capabilities
requiring differing levels of knowledge and skills. required to fulfil all roles in the specialist
To-date these roles have not been differentiated AOD field and defines pathways to achieve
and fully and uniformly described on a national these capabilities.
basis (see Outcome Area 1-nationally agreed • Ensuring that capabilities which are pivotal
taxonomy of specialist AOD roles), nor have the to the future of the AOD sector are included
sets of capabilities required to undertake them in the workforce development matrix.
been explicitly identified. These include capabilities concerning
client-centred service provision, program
The establishment of a workforce development
evaluation, inter-professional practice,
matrix involving the major roles in the specialist
responding to multiple morbidities,
AOD field, and pathways to achieve them, would
responding to the needs of older people,
help to address this shortcoming. For some
leadership skills, child and family sensitive
members of the AOD workforce, the required
practice and responding to special needs
capabilities could be aligned with the attainment
groups, such as those outlined in Outcome
of specified competencies in the vocational
Area 7.
education and training sector. Others would
require capabilities that could be attained via • Ensuring that workforce capabilities evolve
tertiary study, inservice training, recognition of to reflect emerging research evidence
prior learning, assessment of clinical skills by (such as drug trends and intervention
supervisors, or completion of a professional effectiveness).
development program (such as that provided by
the Chapter of Addiction Medicine). A credentialing • Exploring options for the formation of
program (such as that provided by the Drug and national workforce development programs
Alcohol Nurses of Australasia), represents a way of and resources (including web-based
measuring the attainment of these capabilities. approaches).
• Ensuring that mentoring, clinical supervision
It will be important to ensure that these
and appraisal programs support the
capabilities are set at comparable levels with
attainment of identified capabilities.
other fields. If they are set at levels which are
higher than comparative fields this could reduce
Key Performance Indicators could include:
the attractiveness of AOD work. In addition, it
is important that the identified capabilities are • Capability requirements and the pathways
not regarded as employment pre-requisites. to achieve these are clearly identified for all
Opportunities must be provided for new entrants major roles in the specialist AOD field.
and existing staff to acquire the required capability • Level of articulation between different types
levels during their employment. In addition, it will and levels of competencies required to
be important not to disadvantage workers who work in the AOD field.
wish to remain in their current roles for which
identified capabilities did not previously exist. • Evidence of capabilities being reviewed and
updated based on emerging research.
NATIONAL AOD WFD STRATEGY 2015-2020 17You can also read