Developmental anatomy of the heart: a tale of mice and man1
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Physiol Genomics 15: 165–176, 2003;
review 10.1152/physiolgenomics.00033.2003.
Developmental anatomy of the heart: a tale of mice and man1
Andy Wessels and David Sedmera
Department of Cell Biology and Anatomy, Cardiovascular Developmental Biology Center,
Medical University of South Carolina, Charleston, South Carolina 29425
Submitted 12 March 2003; accepted in final form 26 August 2003
Wessels, Andy, and David Sedmera. Developmental anatomy of
the heart: a tale of mice and man. Physiol Genomics 15: 165–176, 2003;
10.1152/physiolgenomics.00033.2003.—Because of the increasing avail-
ability of tools for genetic manipulation, the mouse has become the most
popular animal model for studying normal and abnormal cardiac devel-
opment. However, despite the enormous advances in mouse genetics,
which have led to the production of numerous mutants with cardiac
abnormalities resembling those seen in human congenital heart disease,
relatively little comparative work has been published to demonstrate the
similarities and differences in the developmental cardiac anatomy in
both species. In this review we discuss some aspects of the comparative
anatomy, with emphasis on the atrial anatomy, the valvuloseptal com-
plex, and ventricular myocardial development. From the data presented
it can be concluded that, apart from the obvious differences in size, the
mouse and human heart are anatomically remarkably similar through-
out development. The partitioning of the cardiac chambers (septation)
follows the same sequence of events, while also the maturation of the
cardiac valves and myocardium is quite similar in both species. The
major anatomical differences are seen in the venous pole of the heart. We
conclude that, taking note of the few anatomical “variations,” the use of
the mouse as a model system for the human heart is warranted. Thus the
analysis of mouse mutants with impaired septation will provide valuable
information on cellular mechanisms involved in valvuloseptal morpho-
genesis (a process often disrupted in congenital heart disease), while the
study of embryonic lethal mouse mutants that present with lack of
compaction of ventricular trabeculae will ultimately provide clues on the
etiology of this abnormality in humans.
mouse; human; cardiac development; embryo
A FAST-INCREASING NUMBER of genetically modified mouse dimensions and properties of the full-grown hearts.
models with structural and functional abnormalities in The human heart weighs about 250–300 g and beats,
the cardiovascular system undoubtedly will contribute on average, 60–70 times per minute. In contrast, the
to an improved understanding of molecular and mor- mouse heart weighs only about 0.2 g, and has a heart-
phological mechanisms that regulate human heart de- beat of around 500–600 times per minute. Apart from
velopment in health and disease. It becomes more and their size, the most pronounced difference in external
more obvious, however, that for proper extrapolation of features between the adult mouse and human heart is
findings in the murine model systems it is crucial to found in their overall shape. The most important factor
have detailed knowledge of the specific anatomical/ determining this shape is the anatomical context of the
morphological details of developing and adult heart in adult heart within in thoracic cavity. In human, the
mice and humans (2, 33, 35). heart “rests” on the diaphragm. This is reflected in its
Before discussing some of the specific anatomical more pyramidal shape and a flat dorsal (or inferior)
features in both species, it is important to consider the surface. In comparison, the mouse heart, which in the
four-legged mouse does not rest on the diaphragm and
has more room to move freely within the pericardial
Article published online before print. See web site for date of cavity, has a more ellipsoidal (“rugby ball” shape).
publication (http://physiolgenomics.physiology.org).
Address for reprint requests and other correspondence: A. Wes-
Another difference in external features is that in the
sels, Dept. of Cell Biology and Anatomy, Medical Univ. of South human heart the atria are very prominent structures,
Carolina, 173 Ashley Ave., Basic Science Bldg., Rm. 648, PO Box whereas in the mouse heart the atrial chambers and
250508, Charleston, SC 29425 (E-mail: wesselsa@musc.edu). their appendages are relatively small.
1
This review article was based on work originally presented at the
“NHLBI Symposium on Phenotyping: Mouse Cardiovascular Func-
Developmentally, it is interesting to note that the
tion and Development” held at the Natcher Conference Center, NIH, gestational window during which the heart develops is
Bethesda, MD, on October 10–11, 2002. quite different in the mouse and human. In the human
1094-8341/03 $5.00 Copyright © 2003 the American Physiological Society 165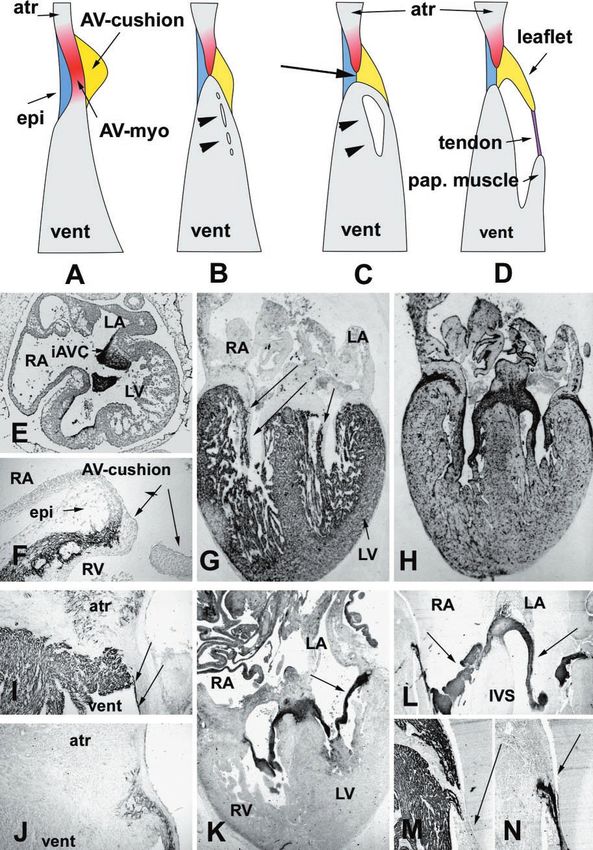
166 REVIEW: ANATOMY OF MOUSE AND HUMAN HEART
it takes about 2 mo (from conception) for the heart to MATERIAL AND METHODS
complete septation, followed by another 7 mo to further Most of the images of human and murine specimens used
mature until the baby is born and the pulmonary in the illustrations of this review were generated in the
circulation kicks in. In the mouse, however, it takes context of studies published previously (26, 27, 31, 37, 38,
only 2 wk from the time of conception for cardiac 40–43). Some of the scanning electron microscope (SEM)
septation to complete. After that, the mouse fetus has images are from the collection of late Tomas Pexieder. De-
less than 1 wk of prenatal life before birth. Without tails regarding tissue collection, preparation, histology, im-
going into any detail, it suffices to say that some of the munohistochemical staining procedures, characterization
developmental events that in the human are more or and properties of antibodies, and the preparation of SEM
samples can be found in papers mentioned above and in the
less completed at birth are still in progress in the remainder of the text. As most of the photographs in the
neonatal mouse. There are several publications in lit- respective histological and SEM collections did not contain
erature in which the comparative developmental scale bars, we could unfortunately not provide scale bars for
stages in mouse and human are listed (28, 39). These the figures in this paper.
tables are helpful when studying developmental
events. It is important to realize, however, that the THE ANATOMY OF THE POSTNATAL HEART IN MOUSE
staging protocol used to determine the developmental AND HUMAN
stage of mouse embryos is not always the same. For
instance, when using the “vaginal plug” method, most The basic anatomical features of the postnatal heart
investigators will mark the morning on which a sperm in the human and mouse are very similar (Fig. 1). Thus
plug is observed as embryonic day 0.5 (ED0.5 ; Ref. 34). in both species the heart has four chambers; two atria,
Others, however, will consider this ED1.0. This obvi- separated by an interatrial septum (IAS), and two
ously can lead to confusion, and more importantly, ventricles, separated by an interventricular septum
misinterpretation of data. Thus, when describing and (IVS). In addition, located between the IAS and IVS
comparing developmental events, it is very important there is a small “septal segment,” which, as a result of
to be very explicit about the staging process when the offset of the atrioventricular (AV) valves, is known
presenting developmental data. Moreover, when work- as the atrioventricular septum (AVS), as it is basically
ing with tissues generated by others (previously col- situated in between the subaortic outlet segment of the
left ventricle from the right atrium. In the human, this
lected materials, existing collections, collaborations)
AVS is a thin fibrous structure, known as the membra-
where the exact staging protocol that has been followed
nous septum. In the mouse this structure is relatively
is not known, it is equally important to point that out
thick and mostly muscular, partly as a result of de-
when reporting on data based on these tissues. As more
layed delamination of the septal leaflet of the tricuspid
and more clinical imaging techniques are now being
valve (35), and partly as a result of myocardialization
adapted for use in studies on mouse models [e.g., MRI, of the mesenchymal tissues (13). In the junction situ-
ultrasound (10)], it is imperative to keep the issues ated between the atria and ventricles, i.e., the AV
mentioned above in mind. Thus, although the murine junction (AVJ), we find two AV valves. The arrange-
and human heart are anatomically very similar, it is ment of the AV valves in mouse and human is compa-
crucial to be very careful when extrapolating informa- rable (35). In the left AVJ we find a mitral valve, which
tion obtained by studying the mouse into the human has two distinct leaflets (a bicuspid valve), whereas in
context. the right AVJ a tricuspid valve is located, which has
In this review we will first discuss some of the ana- three distinct leaflets. In the human heart the valves
tomical characteristics of the human and murine car- are at their “tips” in continuity with very pronounced
diovascular system. It will be demonstrated that these papillary muscles via relatively long and numerous
characteristics do not differ significantly. In the re- tendinous chords (chordae tendineae; Fig. 1A). In the
mainder of the review we will, therefore, focus on the mouse these chordae are far less prominent (Fig. 2, A
general development of the cardiovascular system in and C). The inner lining of the ventricles is character-
both species by providing some insight in the mecha- ized by the presence of numerous myocardial protru-
nisms that lead to the formation of the functional, fully sions better known as trabeculae (trabeculae carneae).
septated, four-chambered heart. As cardiac develop- In the human, but not so in the mouse, there is a
ment is a very complex process, and it is beyond the pronounced difference in the morphology of the trabec-
scope of this review to discuss all the aspects that ulae in the right vs. the left ventricle (35). In the left
relate to this event, we will limit ourselves to the ventricle of the human heart, the trabeculae are rela-
discussion of two topics that relate to congenital mal- tively thin, whereas the trabeculae in the right ventri-
formations frequently seen in humans. First, as many cle have been described as being coarse. In addition to
of the congenital heart defects found in the newborn the trabeculation and the chordae tendineae, we can,
human heart include abnormalities of the valvulosep- within the apical cavity of the ventricles in both spe-
tal complex, we will discuss some of the developmental cies, also discriminate thin, cordlike, structures that
events that lead to proper valvuloseptal morphogene- resemble the tendinous chords attached to the papil-
sis. We will also, albeit less extensively, describe some lary muscle. Because of their tendonlike appearance, in
of the events that are involved in myocardial differen- older anatomy textbooks (e.g., Told-Hochstetter,
tiation and maturation. Anatomischer Atlas, 1948) these structures are often
Physiol Genomics • VOL 15 • www.physiolgenomics.org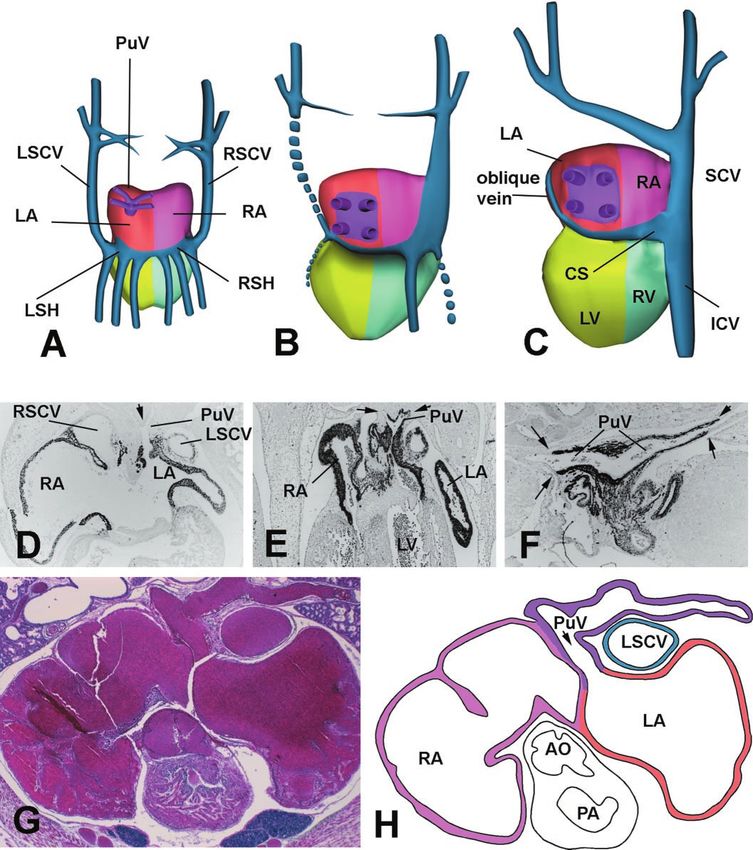
REVIEW: ANATOMY OF MOUSE AND HUMAN HEART 167
Fig. 1. Anatomy of the postnatal human
heart. A: a postnatal human heart in 4-cham-
ber view (from Ref. 1, with permission). B:
histological section of a 5-wk old neonatal
heart, sectioned in the same orientation, is
shown. The section was immunohistochemi-
cally stained for the presence of atrial myosin
heavy chain (aMHC) as described in Ref. 40.
In addition to the expression of aMHC in the
atria, expression of this MHC isoform is also
observed in the left and right bundle
branches of the atrioventricular conduction
system (arrows). Note the orientation and
thickness of the interventricular septum
(IVS) in relation to the left and right ventric-
ular free wall. Ao, aorta; AVS, atrioventricu-
lar septum; IAS, interatrial septum; LA, left
atrium; LBB, left bundle branch; LV, left
ventricle; RA, right atrium; RBB, right bun-
dle branch; RV, right ventricle.
described as trabeculae tendineae. However, despite of human and murine embryo, the left and right superior
this resemblance, these thin structures are not really caval veins (LSCV and RSCV) initially drain into the
tendons, but are actually extensions of the subendocar- sinus venosus. The sinus venosus itself opens via the
dial ventricular network of the cardiac conduction sys- sinoatrial foramen into the right atrium (36, 37). As
tem, and are therefore nowadays generally referred to development progresses, in the human heart the left
as “false tendons” (Fig. 2D). As they consist almost caval vein regresses and the remaining proximal por-
exclusively of Purkinje cells (i.e., specialized myocytes tion (with part of the left sinus horn) becomes the
of the conduction system) within a fibrous sheet, they coronary sinus, the remnant of the LSCV becoming the
can be used to obtain enriched preparations of conduc- so-called ligament of Marshall and oblique vein (Fig. 3,
tion system related genes (20) or to perform physiolog- A–C). In the mouse, however, the LSCV does not re-
ical experiments (9). A slight morphological difference gress and persists into postnatal life (Fig. 3H). In the
in the overall ventricular anatomy between mouse and human, persistent LSCV is considered a congenital
human is found in the relative size and shape of the malformation (incidence ⬍1:100) frequently associated
muscular ventricular septum and the position of the with other congenital malformations. It is likely that
aortic outlet in relation to the IVS (cf. Figs. 1 and 2). In these differences in development of the venous tribu-
the human heart the muscular IVS is a massive struc- taries into the atrial chambers are the underlying
ture, its thickness approaching or exceeding that of the reasons for the relatively small size of the atrial com-
left ventricular free wall (Fig. 1, A and B). The human ponents in the murine heart.
muscular IVS has a very broad base just below the AV
valve attachments. In the mouse, the IVS is not quite Valvuloseptal Development
as massive and compact (Fig. 2, A and B), and at the
base it gradually tapers toward the AV septum. The The first step in cardiac development in the verte-
difference in the angle of the aortic outlet relative to brate heart involves the formation of two bilateral
the axis of the IVS is another remarkable feature (cf. heart fields of precardiac mesoderm. These heart fields
Fig. 1B and Fig. 2A). The most prominent anatomical are situated on opposite sides of the embryonic midline
variations between the cardiovascular systems in (6, 24) and contain endocardial as well as myocardial
mouse and human are probably those found in the precursor cells. As the embryo develops, the heart
venous components of the atria (Fig. 3). All of these fields fuse, resulting in the formation of a primary
variations reflect the species-specific differences in de- heart tube. This tubular heart consists of a myocardial
velopment of the venous tributaries connecting to the outer mantle with an endocardial inner lining. Be-
inferior atrial wall. Thus, whereas in the human heart tween these two concentric epithelial cell layers, an
the left atrium receives four pulmonary veins (37), in acellular matrix is found which is generally referred to
the mouse heart, the pulmonary veins join in a pulmo- as the cardiac jelly (Fig. 4A). During cardiac looping,
nary confluence behind the left atrium (Fig. 3, G and the cardiac jelly basically disappears from the future
H), which in turn empties via a single foramen into the major chambers of the heart (i.e., atria and ventricles),
dorsal wall of the left atrium (13, 36). Another anatom- whereas in the junction between the atria and ventri-
ical difference in the atrial anatomy relates to the cles, the atrioventricular junction (AVJ), as well as in
venous drainage into the right atrium. During the the developing outflow tract (OFT), the cardiac jelly
early stages of cardiac morphogenesis, in both the starts to accumulate. This results in the formation of
Physiol Genomics • VOL 15 • www.physiolgenomics.org168 REVIEW: ANATOMY OF MOUSE AND HUMAN HEART
Fig. 2. Scanning electron micrographs
(SEM) of the postnatal mouse heart. A
and B: SEM images of the posterior (A)
and anterior (B) half of an adult mouse
heart. C: an enlargement of the boxed
area in A, showing the relatively small
leaflets of the murine mitral valve (cf.
Fig. 1A). D: an enlargement of the
boxed area in B and demonstrates
some of the false tendons in the apical
portion of the right ventricle. See leg-
end to Fig. 1 for definitions of abbrevi-
ations.
Fig. 3. Development of the venous pole of the heart. A–C: a schematic representation of the development of the
venous pole in human heart (modified from Fig. 7-10 in Human Embryology, William J. Larsen, Churchill
Livingstone, 1993). D–F: immunohistochemically stained section of human embryos stained for ␣-MHC at,
respectively, 5.5 (D), 7 (E), and 8 wk (F) of development. G: a histological section of a nonperfused neonatal mouse
heart. H: is a schematic representation of G (color coding according to A–C). A: in early development (⬃4–5 wk)
the left and right horns of the sinus venosus communicate with the developing (unseptated) atrium. The left sinus
horn (LSH) receives blood from several vessels including the left superior caval vein (LSCV), and the right sinus
horn (RSH) is connected to the right superior caval vein (RSCV). As development progresses, the LSCV regresses
(see B), resulting in the formation of the oblique vein (see C), with the remnant of the LSH becoming the coronary
sinus (CS) emptying into the right atrium (RA; see C). The cartoon also illustrates how during human cardiac
development the confluence of the pulmonary veins (PuV; see A) becomes incorporated into the left atrium (see B
and C). D: at 5.5 wk of development the pulmonary veins connect to the LA through a single communication (note
that the walls of the pulmonary veins are not myocardial at this point). At 7 wk the walls of the confluence of the
pulmonary veins are becoming myocardial (E). The process of incorporation is nearly completed at 8 wk; the walls
of the pulmonary veins are now myocardialized up to the pericardial reflection (arrows). The images in G and H
demonstrate that in the mouse the pulmonary confluence does not become incorporated into the LA. Instead, the
pulmonary veins drain into the LA via a single channel (arrow). G and H also illustrate that, unlike in the human,
persisting LSCV is a normal anatomical situation in the postnatal mouse. ICV, inferior caval vein; PA, pulmonary
artery; SCV, superior caval vein. See legends of previous figures for other abbreviations.
Physiol Genomics • VOL 15 • www.physiolgenomics.orgREVIEW: ANATOMY OF MOUSE AND HUMAN HEART 169
the endocardial cushion tissues in the AVJ (see Figs. 4, their epithelial context, transform, thereby assuming a
E–H, for examples in the mouse and Figs. 6, E and F mesenchymal phenotype, and start to migrate into the
for an example in the human) and OFT. An important extracellular matrix of the cushions (Fig. 4B). This
developmental event in the subsequent maturation of process, which is, at least partly, regulated by growth
these cushions is the endocardial epithelial-to-mesen- factors that are produced in the underlying myocar-
chymal transformation (EMT; see Ref. 19). During this dium (for a review, see Ref. 7), results in the mesen-
EMT, a subset of the endocardial cells delaminate from chymalization of the cushions. The endocardial cushion
Physiol Genomics • VOL 15 • www.physiolgenomics.org170 REVIEW: ANATOMY OF MOUSE AND HUMAN HEART
tissues are extremely important for cardiac morpho- cushions starts to develop in the lateral aspects of the
genesis. They are the major “building blocks” of, and AVJ. These cushions are generally referred to as the
provide the “glue” for, virtually all of the septal struc- lateral cushions (Fig. 4, C and F). Interestingly, al-
tures in the heart (38). Dysmorphogenesis of the endo- though the lateral cushions are very important for
cardial cushions and/or failure of proper fusion are valvuloseptal morphogenesis, as they contribute to the
generally thought to play a major role in the etiology of formation of anterosuperior leaflet of the tricuspid
congenital heart disease in humans, for instance, in valve (17) and the mural leaflet of the mitral valve, the
the setting of common AV defects. Gross abnormalities mechanisms that are responsible for inducing their
in formation of endocardial cushion tissue is observed development and differentiation have thus far been
in a variety of genetically modified mouse models such very poorly studied.
as the neurofibromin-1 (16), hyaluronan synthase-2 Fate of the AV cushions. After fusion, the (major) AV
(Has2) (4), and RXR-␣ knockout mice (8) and is usually cushion-derived tissue basically forms a large mesen-
associated with fetal lethality. The spectrum of cushion chymal “bridge” spanning from the posterior wall of the
abnormalities is very broad. In some genetically al- AV canal to the anterior wall of the heart (37). Postero-
tered mice, hardly any cushion tissue is formed, inferiorly, this mesenchymal component is in continu-
whereas others develop hypercellularized and/or en- ity with the dorsal mesenchymal protrusion/dorsal me-
larged cushions. In many cases this appears to be a socardium and the mesenchymal cap (also endocardial
result of perturbed endocardial-to-mesenchymal trans- cushion material) that covers the leading edge of the
formation leading to either too many (16) or too few forming primary interatrial septum (pIAS) septum (de-
(14) endocardially derived cells in the cushions tissues. scribed in detail in Ref. 37). This mesenchymal cap is
Although, in general, mice with cushion abnormalities anterosuperiorly also in continuity with the remnant of
manifest defects in both the AV as well as the OFT the superior AVC cushion. The pIAS at this point has
region, sometimes this is not the case and only the OFT not closed the communication between left and right
cushions are affected (NFAT-C and SOX-4; Ref. 44). As atrium yet, and as a result the mesenchymal bridge
indicated above, endocardial cushions develop in the spans the primary atrial foramen (interatrial commu-
AVJs as well as in the OFT. There are many similari- nication) between the dorsal and ventral aspects of the
ties in the fate of endocardial cushions in AVJ and fused cushions. As development progresses, the mes-
OFT. The cushion tissues in the AVJ contribute to the enchymal cap on the primary septum and the fused
formation of AV septal structures and AV valves, and cushions merge completely, thereby closing this pri-
the cushion tissues in the OFT take part in septation of mary foramen. The remodeling of this mesenchymal
the OFT and in the formation of the semilunar valves “crux of the heart,” which at this point basically con-
of aorta and pulmonary artery (see, e.g., Ref. 23). In the sists of the fused major AV cushions and the mesen-
next section we will discuss some of the aspects of AV chymal cap of the pIAS and which is situated between
development in a little more detail. the muscular IVS and the IAS (Fig. 5A), eventually
The AV junction. As briefly outlined above, the en- leads to the formation of the membranous AV septum,
docardial jelly in the AVJ forms the base material for the septal leaflet of the tricuspid valve (17), and the
the AV cushions (21, 38). Initially only two endocardial aortic leaflet of the mitral valve (Fig. 5B). Although the
cushions develop which face each other on opposing endocardial cushion tissues are important in the for-
sides of the common AV canal. These cushions, which mation of the valves, AV valve morphogenesis also
we will refer to as the “major” AV cushions, are known involves a number of myocardial remodeling steps (Fig.
as the inferior (also known as posteroinferior or dorsal) 6). Below, we have summarized (and simplified) the
AV cushion and the superior (also known as ventral or steps that are involved in the formation of the valves. It
anterosuperior) AV cushion (Fig. 4, B and E). The is important to realize that not all the leaflets of the AV
major AV cushions are the most prominent endocardial valves develop exactly the same (see Refs. 17 and 21).
cushion tissues in the heart, and, as development pro- However, in the context of this paper it suffices to
ceeds, the leading edges of the cushions fuse (Fig. 4, C, describe the general principle, focusing on the fate of
F, and G), thereby separating the common AV canal the lateral cushions. First, it is important to determine
into a left and right AV orifice (Fig. 4, C, D, and F). At the relationship between the cushions and the adjacent
this point, another set of, relatively small, endocardial tissues. The cushions have an upper (atrial) boundary
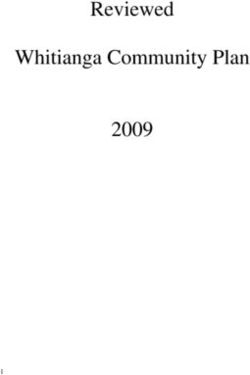
Fig. 4. Development of the atrioventricular cushions in the mouse. A–D: schematic of the development of the AV
cushions in the mouse/human heart. A: the tubular heart stage. The outer myocardial layer and the inner
endocardial cell layer sandwich the cardiac jelly (CJ). B: the stage in which the cardiac jelly has given rise to the
formation of the major AV cushions. The cells within the subendocardial space indicate that endocardial-to-
mesenchymal transformation has been initiated. C: the mesenchymalized major cushions are fusing, while at the
lateral aspects of the AV canal the lateral AV cushions have formed. In D, the fusion has been completed, and a
wedge of mesenchyme separates the left from the right AV orifice. The specimen shown in E is representative for
the cartoon in B, F shows a specimen that correlates to C, while H demonstrates the fused mesenchymal tissues
as depicted in D. G: a higher magnification of the boxed area in F, showing the fusion of the endocardial layers of
the two major AV cushions. “cap,” mesenchymal cap on leading edge of IAS; endo, endocardium; epi, epicardium;
iAVC, inferior AV cushion; llAVC, left lateral AV cushion; OFT, outflow tract; sAVC, superior AV cushion; myo,
myocardium; rlAVC, right lateral AV cushion. See legends of previous figures for other abbreviations.
Physiol Genomics • VOL 15 • www.physiolgenomics.orgREVIEW: ANATOMY OF MOUSE AND HUMAN HEART 171 Physiol Genomics • VOL 15 • www.physiolgenomics.org
172 REVIEW: ANATOMY OF MOUSE AND HUMAN HEART
Fig. 5. Contributions of the major atrioventricular cush-
ions to valvuloseptal morphogenesis in the human heart.
These panels show two serial sections of a human heart at
⬃6 wk of development stained for the presence of atrial
MHC (A) and ventricular MHC (B) as described before
(42). A: this is how the mesenchymal tissues of the two
major cushions and the mesenchymal cap on the IAS have
fused to form the mesenchymal “crux” of the heart. B: this
indicates how the structures indicated in A contribute to
valvuloseptal morphogenesis in the AV junction (AVJ).
epi, epicardially derived mesenchyme. See legends of pre-
vious figures for other abbreviations.
and a lower (ventricular) boundary. The bulk of the (for a detailed description of this process see Refs. 18,
cushion tissue is plastered against the AV junctional 38, and 41). There is only one place where this separa-
and ventricular myocardium (Fig. 6, A, E, and F). The tion does not take place, and that is where the special-
first myocardial remodeling event leads to the inter- ized myocardium of the AV conduction axis (AV node
ruption of the continuity between atrial and myocar- and proximal His bundle) develops (38). These compo-
dial ventricular myocardium (Fig. 6, B and C) and is a nents of the AV conduction system (AVCS) relay the
result of the fusion between cushion-derived tissues cardiac impulse from atria to ventricles. The second
and epicardially derived mesenchyme (38). Specifi- myocardial remodeling event that plays an important
cally, this process takes place at the lower end of the role in the formation of the freely moveable leaflets of
AV canal myocardium resulting in the incorporation of the AV valves is myocardial delamination (17, 21).
most of the AV canal myocardium into the lower rim of During this process the lower part of the AV cushions,
the atrial chambers (Fig. 6C). This process establishes with associated myocardial layer (Fig. 6, B, C, G, and
the functional separation, and electrical insulation, H), separates from adjacent ventricular myocardium
between atrial and ventricular working myocardium by a hitherto undetermined process. This results in the
Fig. 6. Atrioventricular valve development in the embryonic human heart. A–D: schematic representations of AV
valves in the developing human heart. E–N: a series of immunohistochemically stained sections of representative
stages in this process. Sections shown in E, J, K, L, and N were stained with the “cushion-tissue antigen” antibody
249-9G9 (anti-CTA; Ref. 38), the sections in F, G, and I were stained with anti-ventricular MHC (43), the section
in H (sister section to G) with anti-mesenchymal cell antigen (anti-MCA; Ref. 38), and the section in M (sister
section to N) was stained with an antibody that recognizes the atrial as well as the ventricular isoform of MHC (38).
The sections shown in E and F are from a heart at ⬃5 wk of development (38). G and H: sister sections from a
9-wk-old heart. I–K: sister sections from a heart at 12–13 wk of development. L–N: sister sections from a heart at
17 wk of development. The panels demonstrate (represented schematically in A–D) how during development the
leaflets of the valves delaminate and detach from the myocardial wall. Initially, the leaflets contain a considerable
amount of myocardium at their ventricular aspect (best seen in G), but as development progresses this myocardium
gradually disappears (cf. G, I, and M). AV myo, atrioventricular myocardium. See legends of previous figures for
other abbreviations.
Physiol Genomics • VOL 15 • www.physiolgenomics.orgREVIEW: ANATOMY OF MOUSE AND HUMAN HEART 173 Physiol Genomics • VOL 15 • www.physiolgenomics.org
174 REVIEW: ANATOMY OF MOUSE AND HUMAN HEART
Fig. 7. Development of the compact
ventricular myocardium in mouse de-
velopment in health and disease. Com-
paction of the ventricular trabeculae
adds to proportion and thickness of the
compact myocardium. In the human,
this takes place between 12 wk (A) and
18 wk (B). Sagittally dissected parietal
halves of left ventricles are shown.
Scale bars 100 m. (Images are from
the Pexieder collection: B first pub-
lished in Ref. 26, and A appeared in
Ref. 31). Compaction occurs in the
mouse between ED13 and 14, resulting
in well-formed multilayered compact
layer by ED14.5 in the wild-type ani-
mal (black arrows in C and white ar-
row in E). This process is perturbed in
several knockouts, such RXR-␣ (black
arrows in D and white arrow in F),
resulting in “thin compact myocardium
syndrome” and embryonic lethality.
formation of “immature” or “prevalvar” bilayered leaf- surgical left atrial ligation (25). This procedure leads to
lets, with the inferior (or “ventricular”) layer consisting the formation of a (albeit dysmorphic) fibrous leaflet,
of myocardium and the superior (“atrial”) layer being reminiscent of the situation in mouse and human.
cushion derived (Fig. 6, C and G). Toward the ventric- In-depth studies of the molecular mechanisms involved
ular apex, these leaflets are attached to the ventricular in the molecular regulation of this myocardialization
walls and/or IVS through the developing papillary process might provide important clues regarding val-
muscles (Fig. 6, G and H). The myocardium gradually vuloseptal morphogenesis in general, as myocardial-to-
disappears from the developing leaflets between 10 fibrous and fibrous-to-myocardial “transformations”
and 17 wk of development (Fig. 6, I–N). Interestingly, are common steps in normal and perturbed cardiovas-
in the right AVJ of the chick heart, the initial develop- cular development in the chick, mouse, and human
ment of the lateral AV leaflet resembles that of the heart (13, 29, 30).
mouse and human. However, instead of the regression
of muscular tissue, leading to the formation of a fibrous Myocardial Compaction
leaflet, the mesenchymal tissue gets replaced by myo-
cardium, resulting in the formation of the characteris- Ventricular trabeculation starts to develop in the
tic muscular flap valve in the right AVJ of the chick. apical region of the ventricles soon after looping in both
Immunohistochemical studies indicate that the mech- mouse and human. The trabeculation serves primarily
anism that is responsible for this process is myocardi- as a means to increase myocardial oxygenation in ab-
alization, i.e., the ingrowth of existing myocardium sence of coronary circulation. At its peak prior to com-
into flanking mesenchymal tissues. Experimental pletion of ventricular septation, the trabeculae can
studies have revealed that this myocardialization pro- form as much as 80% of the myocardial mass in the
cess in the avian right AV valve can be disturbed by embryonic human heart (3) and provide most of the
Physiol Genomics • VOL 15 • www.physiolgenomics.orgREVIEW: ANATOMY OF MOUSE AND HUMAN HEART 175
ventricular wall thickness between ED11 and ED16 in disease. We conclude that mouse molecular genetics
the mouse. Concomitant with ventricular septation, combined with detailed morphological assessment of
the trabeculae start to compact at their base adjacent generated cardiac malformations in the genetically
to the outer compact myocardium, adding substan- modified mouse models will lead to important break-
tially to its thickness (reviewed in Ref. 26). This pro- throughs in the identification of a series of (candidate)
cess is fairly rapid (in mouse, between ED13 and ED14, genes, and the elucidation of pathways, involved in the
in human between 10 and 12 wk; Ref. 26), coinciding etiology of human congenital heart disease.
with establishment of the coronary circulation. From
ED16 in the mouse and the 4th mo of gestation in ACKNOWLEDGMENTS
human, the compact layer forms most of the ventricu-
We thank Dr. Tom Trusk for preparing the informative cartoons
lar myocardium, although its structural complexity in Figs. 3 and 4, and we thank Dr. Steve Kubalak for providing the
continues to develop (12). Noncompaction of the myo- illustrations of the RXR-␣ knockout mouse (Fig. 7).
cardium presents serious functional consequences for
the heart. Several mouse null mutants present with a GRANTS
complete lack of compaction [e.g., RXR-␣ knockout A. Wessels and D. Sedmera are financially supported by National
mouse (8); see Fig. 7], which results in lethality around Institutes of Health Grants PO1-HL-52813 (to A. Wessels), P20-RR-
ED14 (reviewed in Ref. 26), emphasizing the impor- 16434 (to D. Sedmera), and PO1-HD-39946 (to A. Wessels and D.
tance of the compact myocardium for force generation Sedmera).
in later fetal stages. In humans, ventricular noncom-
REFERENCES
paction is usually localized. Although it can occur in
isolation, it was found in association with heart failure 1. Anderson RH and Becker AE. Cardiac Anatomy: An Inte-
and sudden cardiac death (32). Even if only a relatively grated Text and Colour Atlas. London: Gower, 1980.
2. Anderson RH, Webb S, and Brown NA. The mouse with
small proportion of ventricular wall is affected, ventric- trisomy 16 as a model of human hearts with common atrioven-
ular dynamics is perturbed (11). This condition can tricular junction. Cardiovasc Res 39: 155–164, 1998.
now be diagnosed by ultrasound and is classified as a 3. Blausen BE, Johannes RS, and Hutchins GM. Computer-
distinct cardiomyopathy. There is a growing body of based reconstructions of the cardiac ventricles of human em-
bryos. Am J Cardiovasc Pathol 3: 37–43, 1990.
evidence that the epicardium and the epicardially de- 4. Camenisch TD, Spicer AP, Brehm-Gibson T, Biesterfeldt
rived cells play a crucial role in the development of the J, Augustine ML, Calabro A Jr, Kubalak S, Klewer SE, and
compact layer of the ventricular myocardial walls. Not McDonald JA. Disruption of hyaluronan synthase-2 abrogates
only is the “thin-myocardium syndrome” observed in normal cardiac morphogenesis and hyaluronan-mediated trans-
formation of epithelium to mesenchyme. J Clin Invest 106: 349–
several mouse models with perturbed epicardial devel- 360, 2000.
opment [e.g., ␣4-integrin (45) and VCAM-1 (15) knock- 5. Chen TH, Chang TC, Kang JO, Choudhary B, Makita T,
out mice], recent experimental studies in which epicar- Tran CM, Burch JB, Eid H, and Sucov HM. Epicardial
dial development was perturbed in avian embryos also induction of fetal cardiomyocyte proliferation via a retinoic acid-
demonstrated inhibition of ventricular compaction inducible trophic factor. Dev Biol 250: 198–207, 2002.
6. De Haan RL. Morphogenesis of the Vertebrate Heart. New York:
(22). The mechanism(s) that are responsible for the Holt, Rinehart and Winston, 1965.
regulation of ventricular myocardial differentiation, 7. Eisenberg L and Markwald R. Molecular regulation of atrio-
growth, and compaction are at present poorly under- ventricular valvuloseptal morphogenesis. Circ Res 77: 1–6, 1995.
stood, but it is to be expected that further analysis of 8. Gruber P, Kubalak S, Pexieder T, Sucov H, Evans R, and
Chien K. RXR alpha deficiency confers genetic susceptibility for
mutant mice with “thin compact myocardium,” such as aortic sac, conotruncal, atrioventricular cushion, and ventricular
the RXR-␣ knockout mouse (5, 14), can provide clues on muscle defects in mice. J Clin Invest 98: 1332–1343, 1996.
the cascade of genetically regulated events that lead to 9. Han W, Wang Z, and Nattel S. Slow delayed rectifier current
trabecular compaction and hence molecular etiology of and repolarization in canine cardiac Purkinje cells. Am J Physiol
this condition in humans. Heart Circ Physiol 280: H1075–H1080, 2001.
10. Huang GY, Cooper ES, Waldo K, Kirby ML, Gilula NB, and
Lo CW. Gap junction-mediated cell-cell communication modu-
CONCLUSIONS lates mouse neural. J Cell Biol 143: 1725–1734, 1998.
11. Jenni R, Oechslin E, Schneider J, Jost CA, and Kaufmann
In this review we have demonstrated that, given the PA. Echocardiographic and patho-anatomical characteristics of
considerable differences in cardiac size and heart rate, isolated left ventricular non-compaction: a step towards classifi-
cation as a distinct cardiomyopathy. Heart 86: 666–671, 2001.
the cardiac anatomy in mouse and human is, with the 12. Jouk PS, Usson Y, Michalowicz G, and Grossi L. Three-
exception of some small variations (mainly in the ve- dimensional cartography of the pattern of the myofibres in the
nous pole), remarkably similar. We have also shown second trimester fetal human heart. Anat Embryol (Berl) 202:
that, at least within the context of the topics discussed, 103–118, 2000.
the developmental events that lead to the formation of 13. Kruithof BPT, Van den Hoff MJB, Wessels A, and Moor-
man AFM. Cardiac muscle cell formation after development of
the four-chambered heart are also very comparable. the linear heart tube. Dev Dyn 227: 1–13, 2003.
Consequently, the mouse can serve as a good model 14. Kubalak SW, Hutson DR, Scott KK, and Shannon RA.
with which to study the human heart. The genetic Elevated transforming growth factor beta2 enhances apoptosis
modification of the murine genome is resulting in a and contributes to abnormal outflow tract and aortic sac devel-
opment in retinoic X receptor alpha knockout embryos. Develop-
growing numbers of mouse models presenting with ment 129: 733–746, 2002.
cardiac malformations that are very reminiscent of the 15. Kwee L, Baldwin HS, Shen HM, Stewart CL, Buck C, Buck
heart anomalies seen in patients with congenital heart CA, and Labow MA. Defective development of the embryonic
Physiol Genomics • VOL 15 • www.physiolgenomics.org176 REVIEW: ANATOMY OF MOUSE AND HUMAN HEART
and extraembryonic circulatory systems in vascular cell adhe- 32. Waller BF, Smith ER, Blackbourne BD, Arce FP, Sarkar
sion molecule (VCAM-1) deficient mice. Development 121: 489– NN, and Roberts WC. Congenital hypoplasia of portions of both
503, 1995. right and left ventricular myocardial walls. Clinical and nec-
16. Lakkis ML and Epstein JA. Neurofibromin modulation of ras ropsy observations in two patients with parchment heart syn-
activity is required for normal endocardial-mesenchymal trans- drome. Am J Cardiol 46: 885–891, 1980.
formation in the developing heart. Dev Biol 125: 4359–4367, 33. Waller BR, McQuinn T, Phelps AL, Markwald RR, Lo CW,
1998. Thompson RP, and Wessels A. Conotruncal anomalies in the
17. Lamers WH, Viragh S, Wessels A, Moorman AF, and trisomy 16 mouse: an immunohistochemical analysis with em-
Anderson RH. Formation of the tricuspid valve in the human phasis on the involvement of the neural crest. Anat Rec 260:
heart. Circulation 91: 111–121, 1995. 279–293, 2000.
18. Lamers WH, Wessels A, Verbeek FJ, Moorman AF, Viragh 34. Waller RB III and Wessels A. Cardiac morphogenesis and
S, Wenink AC, Gittenberger-de Groot AC, and Anderson dysmorphogenesis II. An immunohistochemical approach. In:
RH. New findings concerning ventricular septation in the hu- Developmental Biology Protocols, edited by Lo CW. Totowa, NJ:
man heart. Implications for maldevelopment. Circulation 86: Humana, 2000, p. 151–161.
1194–1205, 1992. 35. Webb S, Brown NA, and Anderson RH. The structure of the
19. Markwald RR, Fitzharris TP, and Manasek FJ. Structural mouse heart in late fetal stages. Anat Embryol (Berl) 194: 37–47,
development of endocardial cushions. Am J Anat 148: 85–119, 1996.
1977. 36. Webb S, Brown NA, Wessels A, and Anderson RH. Develop-
20. Oosthoek PW, Viragh S, Mayen AE, van Kempen MJ, Lam- ment of the murine pulmonary vein and its relationship to the
ers WH, and Moorman AF. Immunohistochemical delineation embryonic venous sinus. Anat Rec 250: 325–334, 1998.
of the conduction system. I. The sinoatrial node. Circ Res 73: 37. Wessels A, Anderson RH, Markwald RR, Webb S, Brown
473–481, 1993. NA, Viragh S, Moorman AF, and Lamers WH. Atrial devel-
21. Oosthoek PW, Wenink AC, Vrolijk BC, Wisse LJ, DeRuiter opment in the human heart: an immunohistochemical study
MC, Poelmann RE, and Gittenberger-de Groot AC. Devel- with emphasis on the role of mesenchymal tissues. Anat Rec 259:
opment of the atrioventricular valve tension apparatus in the 288–300, 2000.
human heart. Anat Embryol (Berl) 198: 317–329, 1998. 38. Wessels A, Markman MW, Vermeulen JL, Anderson RH,
22. Perez-Pomares JM, Phelps A, Sedmerova M, Carmona R, Moorman AF, and Lamers WH. The development of the atrio-
Gonzalez-Iriarte M, Munoz-Chapuli R, and Wessels A. Ex- ventricular junction in the human heart. Circ Res 78: 110–117,
perimental studies on the spatiotemporal expression of WT1 and 1996.
RALDH2 in the embryonic avian heart: a model for the regula- 39. Wessels A and Markwald R. Cardiac morphogenesis and dys-
tion of myocardial and valvuloseptal development by epicardi- morphogenesis. I. Normal development. Methods Mol Biol 136:
ally derived cells (EPDCs). Dev Biol 247: 307–326, 2002. 239–259, 2000.
23. Qayyum SR, Webb S, Anderson RH, Verbeek FJ, Brown 40. Wessels A, Mijnders TA, de Gier-de Vries C, Vermeulen
NA, and Richardson MK. Septation and valvar formation in JLM, Viragh S, Lamers WH, and Moorman AFM. Expres-
the outflow tract of the embryonic chick heart. Anat Rec 264: sion of myosin heavy chain in neonatal human hearts. Cardiol
273–283, 2001. Young 2: 318–334, 1992.
24. Redkar A, Montgomery M, and Litvin J. Fate map of early 41. Wessels A, Vermeulen JL, Verbeek FJ, Viragh S, Kalman
avian cardiac progenitor cells. Development 128: 2269–2279, F, Lamers WH, and Moorman AF. Spatial distribution of
2001. “tissue-specific” antigens in the developing human heart and
25. Sedmera D, Pexieder T, Rychterova V, Hu N, and Clark skeletal muscle. III. An immunohistochemical analysis of the
EB. Remodeling of chick embryonic ventricular myoarchitecture distribution of the neural tissue antigen G1N2 in the embryonic
under experimentally changed loading conditions. Anat Rec 254: heart; implications for the development of the atrioventricular
238–252, 1999. conduction system. Anat Rec 232: 97–111, 1992.
26. Sedmera D, Pexieder T, Vuillemin M, Thompson RP, and 42. Wessels A, Vermeulen JL, Viragh S, Kalman F, Lamers
Anderson RH. Developmental patterning of the myocardium. WH, and Moorman AF. Spatial distribution of “tissue-specific”
Anat Rec 258: 319–337, 2000. antigens in the developing human heart and skeletal muscle. II.
27. Seo JW, Kim EK, Brown NA, and Wessels A. Section directed An immunohistochemical analysis of myosin heavy chain iso-
cryosectioning of specimens for scanning electron microscopy: a form expression patterns in the embryonic heart. Anat Rec 229:
new method to study cardiac development. Microsc Res Tech 30: 355–368, 1991.
491–495, 1995. 43. Wessels A, Vermeulen JL, Viragh S, Kalman F, Morris GE,
28. Sissman NJ. Developmental landmarks in cardiac morphogen- Man NT, Lamers WH, and Moorman AF. Spatial distribution
esis: comparative chronology. Am J Cardiol 25: 141–148, 1970. of “tissue-specific” antigens in the developing human heart and
29. van den Hoff MJ, Kruithof BP, Moorman AF, Markwald skeletal muscle. I. An immunohistochemical analysis of creatine
RR, and Wessels A. Formation of myocardium after the initial kinase isoenzyme expression patterns. Anat Rec 228: 163–176,
development of the linear heart tube. Dev Biol 240: 61–76, 2001. 1990.
30. van den Hoff MJ, Moorman AF, Ruijter JM, Lamers WH, 44. Ya J, Schilham MW, de Boer PA, Moorman AF, Clevers H,
Bennington RW, Markwald RR, and Wessels A. Myocardi- and Lamers WH. Sox-4 deficiency syndrome in mice is an
alization of the cardiac outflow tract. Dev Biol 212: 477–490, animal model for common trunk. Circ Res 83: 986–994, 1998.
1999. 45. Yang JT, Rayburn H, and Hynes RO. Cell adhesion events
31. Varnava AM. Isolated left ventricular non-compaction: a dis- mediated by alpha 4 integrins are essential in placental and
tinct cardiomyopathy? Heart 86: 599–600, 2001. cardiac development. Development 121: 549–560, 1995.
Physiol Genomics • VOL 15 • www.physiolgenomics.orgYou can also read