Developmental Assessments in Preterm Children: A Meta-analysis - American ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Developmental Assessments in
Preterm Children: A Meta-analysis
Hilary S. Wong, MBChB, PhD,a Shalini Santhakumaran, MSc,b Frances M. Cowan, PhD,c
Neena Modi, MD,c Medicines for Neonates Investigator Group
CONTEXT: Developmental outcomes of very preterm (gestational age ≤32 weeks) or very low abstract
birth weight (The majority of outcome were tested sequentially. Applying weeks gestation or with VLBW, in studies of preterm births report the same diagnostic criteria, Roberts which at least 2 serial assessments, neurodevelopmental status at 18 or et al7 also found a reduction in consisting of a developmental 24 months postterm age (corrected the proportions of very preterm assessment between 1 and 3 years for prematurity). This practice (gestational age
TABLE 1 Review-Specific Signaling Questions and Standards for Appraisal of Study Quality
Domain Patient Selection Index Test (Early Developmental Reference Standard Flow and Timing
Assessment) (School-age Cognitive
Assessment)
Signaling questions (1) Was a consecutive or (1) Was an age-appropriate (1) Was an age-appropriate (1) Were all eligible
random sample of patients validated standardized validated assessment participants receiving
enrolled? assessment tool used? standardized assessment the same assessments?
tool used?
(2) Did the study avoid (2) Were the assessors blinded (2) Were all participants
inappropriate exclusion? to the results of the early included in the analysis?
developmental test?
High risk of bias Nonconsecutive or random Inappropriate test used for Inappropriate test used for If participants receive
sampling methods; population under study population under study different assessments
additional inclusion or if assessors were not or if drop-out rates
criterion based not on birth blinded to results of early >30%
weight or gestational age developmental test
High concerns regarding Subcohort of infants (eg, Nonuniversal tests (eg, only Nonuniversal tests (eg, only
applicability only intrauterine growth standardized in a specific standardized in a specific
restricted infants were population). Older versions population). Assessment
included) recruited. Infants of assessments validated in tools that may not be
born before 1990 because normative populations that may representative of current
they would differ from no longer be representative of populations (eg, published
target population in terms contemporaneous populations before 1990)
of neonatal care received (eg, published before 1990)
and severity/pattern of
diseases experienced
ages at developmental and cognitive version 2 (QUADAS-2) appraisal by early developmental assessments
assessments, and mean test scores). tool.8 The QUADAS-2 tool uses were calculated. Because of the
“signaling questions” to judge bias variation in impairment prevalence
For this review, mild-moderate
in 4 domains: patient selection, across studies, meta-analyses on
deficit was defined as developmental
index test, reference standard, PPV and NPV, which are dependent
or cognitive test scores between 1
and flow of participants through on prevalence rates, were not
and 2 SD below the standardized
the study and timing of the index performed. Separate pooling of
or control group means. Severe
test. The applicability of the study sensitivities and specificities from
deficit was defined as test scores
to the review question in the first the studies, which ignore the
>2 SD below the standardized or
3 domains was also assessed. In correlation between the 2 measures,
control group means. In studies
the context of this review, the could lead to an underestimation of
where a control group of children
index tests referred to the early the diagnostic accuracy.9 Instead,
born at full-term was recruited and
developmental assessments and a hierarchical summary receiver
assessed simultaneously, the mean
the reference standards were the operator characteristics (HSROC)
and SD of the control group were
school-age cognitive assessments. curve was used for meta-analysis.10
used as the references for defining
Table 1 lists the signaling questions The HSROC model accounts for both
the presence of deficit. Data on the
and the quality standards set for this within-study sampling variation and
number of “true-positive”, “false-
review. By appraising against the set between-study heterogeneity using
positive”, “false-negative,” and “true-
standards, each study was given a random effects. The output includes
negative” mild-moderate and severe
rating of “low,” “high,” or “unclear” for a summary operating point (pooled
cognitive deficits identified by early
risk of bias and concerns regarding values for sensitivity and specificity)
assessments were collated from each
applicability in each domain. with 95% confidence region. Meta-
study. Unpublished data were sought
regression was conducted by
from study authors through e-mail Statistical Analysis using bivariate models to test for
requests.
From each study, the estimated the possible association between
sensitivity, specificity, positive sensitivity and specificity and the
Quality Assessment
predictive values (PPV) and negative following study-level variables: mean
The quality of included studies predictive values (NPV), and the gestational age, mean birth weight,
was assessed using a checklist corresponding 95% confidence mean ages at assessments, time
adapted from the Quality of interval (CI) of identifying any and interval between assessments, and
Diagnostic Accuracy Studies, severe school-age cognitive deficits earliest year of birth of participants.
Downloaded from www.aappublications.org/news by guest on January 17, 2021
PEDIATRICS Volume 138, number 2, August 2016 3All analyses were performed by using
Stata statistical package, version 11.0
(Stata Corp, College Station, TX) and
SAS 9.3 (SAS Institute Inc, Cary, NC).
RESULTS
The electronic literature search
yielded 2844 unique citations; 2
additional studies were identified
through a manual search. The flow
of articles through the search and
selection process is depicted in the
PRISMA diagram in Fig 1. Fifty-four
studies met the eligibility criteria.
Data required for the review and
meta-analysis were extractable
directly from 6 articles. The
authors of 18 of the remaining
48 studies contributed unpublished
data. Therefore, 24 studies
(37 articles)4–7,12–44 were included in
this review, and their characteristics
are detailed in Supplemental Table
3. The characteristics of eligible
studies that were not included (year
of publication, countries where the
studies were conducted) were similar
to those included in the review. For
simplicity of referencing, studies that
are represented by >1 article will be
denoted by the first author and year
of publication of the earliest article in
tables and figures.
The study populations included
3133 children who were born at ≤32
weeks and/or had a birth weight
FIGURE 1there were 20 participants from the of the total population of infants in were examined at different time
study of Cohen17 that were born in the Bavarian region to categorize points within the 2 age ranges we
early 1970s. We have not excluded impairments. It should be noted studied, only the results from the
studies on the basis of the time that the study population in Smith assessment performed at the oldest
period the participants were born in et al34 was from low to middle age are presented. This gives a final
because it allowed for analysis of the socioeconomic groups, and the mean sample size of 3060 children for the
variability of diagnostic validity over test score achieved by the control meta-analysis.
time. Children with known genetic group was about 0.5 SD below the
There was significant heterogeneity
syndromes and congenital anomalies normative mean. Using the results
in the reported sensitivities and
were excluded from the studies. from the control group in this case
specificities among studies
Children with severe neurosensory could lead to an underestimation of
(P < .001 for both). The estimated
(including blindness and deafness) the prevalence of impairment in this
sensitivities of diagnosing any
and motor impairment were likely to study. If the test standardized norm
impairment ranged from 17.0% to
be underrepresented in the values were used, the prevalence of
90.5%. There appears to be a wider
cohort because 13 studies cognitive impairment diagnosed at
range and poorer precision (wider
(contributing to 55% of the final 8 years of age would increase from
Confidence Intervals [CI]) in the
sample) excluded children who were 24.0% to 36.0% for mild-moderate
estimated sensitivity than specificity
unable to complete the assessments impairment and from 6.0% to 6.6%
across studies. This may reflect the
as a result of their physical for severe impairment.
presence of heterogeneity or may
disabilities.5,12–15,17,19,21,29,33–35,37
Bias and Applicability of Included be due to estimates of sensitivity
The actual number of children
Studies being based on smaller samples
excluded from the analysis for this
than estimates of specificity. The
reason is unknown because not all The proportions of studies
HSROC curves providing the pooled
studies provided this information. considered to be at “low,” “high,”
measures are presented in Fig 4.
Study participants were assessed and “unclear” risk for bias and
The summary points corresponded
between the ages of 18 and 40 applicability concerns according
to a pooled sensitivity of 55.0%
months using the BSID in 13 studies, to the QUADAS-2 appraisal are
(95% CI, 45.7%–63.9%) and a
the Griffiths Mental Development displayed in Fig 2. The quality of an
pooled specificity of 84.1% (77.5%–
Scales in 6 studies, the Stanford-Binet individual study and the reasons for
89.1%) for the identification of
Intelligence Scale in 1 study, and the being considered at high risk for bias
any impairment. For the diagnosis
Brunet-Lezine Scale in 1 study. In 3 or of concern for applicability are
of severe impairment, the pooled
studies,16,23,29 >1 of these assessment detailed in Supplemental Table 4.
sensitivity was 39.2% (26.8%–
tools were used. School-age cognitive The loss in follow-up of >30%
53.3%) and pooled specificity was
assessments were conducted of the eligible birth cohort was a
95.1% (92.3%–97.0%). Because
between the ages of 5 and 18 years, main source of selection bias in the
the BSID-II was the most commonly
and 11 different tests were used. included studies. Although the overall
used developmental test, a post-hoc
risk of bias was low, the applicability
meta-analysis of the subgroup of 11
The proportion of children diagnosed of the results to our current
studies that only used this tool for
with developmental impairment (test population of preterm infants is
early developmental assessment
scores >1 SD below the standardized concerning. This is because many of
showed a pooled sensitivity of
or control group mean) varied widely the included studies were conducted
54.9% (39.5%–69.3%) for any
among studies, ranging from 6.0%14 >20 years ago; the characteristics
impairment and 43.6% (23.5%–
to 67.0%.6 The reported prevalence of the study populations would
66.0%) for severe impairment; the
of school-age cognitive deficit was be different now, and some of the
corresponding specificities were
between 5.0%17 and 67.4%26 for assessment tools used have been
84.3% (70.1%–92.5%) and 96.4%
mild-moderate (1–2 SD below mean) superseded by newer versions.
(90.0%–98.8%). These values are
and 0.0%17,18 and 37.8%26 for severe
Predictive Validity of Early similar to the results for the whole
impairment (>2 SD below mean). In 5
Developmental Assessment group.
studies,7,21,27,28,34 the categorization
of outcomes was based on the mean The sensitivities, specificities, and None of the study-level variables
and SD of the scores achieved by PPV and NPV of early assessment for examined (gestational age, birth
concurrently recruited term-born identifying any and severe cognitive weight, ages at assessments, time
controls. Wolke et al41 used cohort- deficit estimated from each study interval between assessments,
specific cut-off points derived from are presented in the forest plots in and year of birth) were associated
a normative sample representative Fig 3. In studies where participants with sensitivity or specificity
Downloaded from www.aappublications.org/news by guest on January 17, 2021
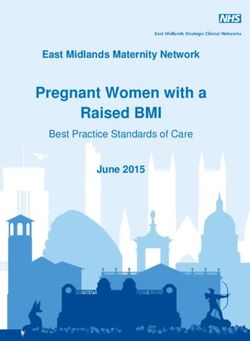
PEDIATRICS Volume 138, number 2, August 2016 5FIGURE 2
Proportions of studies with low, high, or unclear risk of bias and concerns regarding applicability. Bar charts are annotated with the number of studies
in each category.
FIGURE 3
Results of cross-tabulations and forest plots of the estimated sensitivities, specificities, and PPV and NPV of early developmental assessments in identifying
the presence of (A) any cognitive impairment and (B) severe cognitive impairment. Sensitivities, specificities, PPV, and NPV are expressed as proportions.
FN, false-negative, FP, false-positive, TN, true-negative; TP, true-positive.
Downloaded from www.aappublications.org/news by guest on January 17, 2021
6 WONG et aland therefore did not explain the
heterogeneity present between
studies (Table 2).
PPV estimates were most precise
(narrower CIs) in studies in which
the prevalence for any impairment
was >40%, and ranged from
63.0% to 80.6%. For impairment
prevalence >40%, PPV estimates
for the prediction of any cognitive
impairment were between
20.0% and 88.9%. In general,
the NPV of early developmental
assessments were high (range for
“any impairment,” 47.8%–95.5%),
particularly in predicting the
absence of severe impairment (NPV
range for “severe impairment,”
68.9%–100%).
Significance testing confirmed that
asymmetry was not present in the
funnel plot of the log DOR against the
inverse of the square root of the ESS
(Fig 5, P = .22), indicating the absence
of sample size–related effects in the
meta-analysis.
DISCUSSION
Through a systematic review of the
literature, we found a substantial
number of studies published in the
past 20 years that have reported
the early neurodevelopmental
outcomes and later school-age
cognitive abilities of children
born very preterm or with VLBW.
Although early assessments were
generally accurate in predicting
the absence of school-age cognitive
deficits (high NPV), the identification
and prediction of children who
would have cognitive difficulties
were weak. Meta-analysis of the
data suggested that almost half of
children who might experience
cognitive difficulties at school-age
were classified as having normal
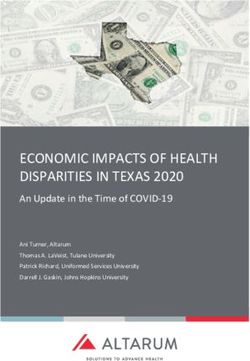
neurodevelopmental function at ages FIGURE 4
1 to 3 years. Even for cases of severe HSROC curves for the pooled sensitivity and specificity of early developmental assessment in
cognitive deficit, the accuracy in early identifying (A) any cognitive impairment and (B) severe cognitive impairment. Each marker displays
detection was low (meta-analytic the study estimates from 1 included study and is scaled according to the sample size of the study.
sensitivity of 39.2%).
Downloaded from www.aappublications.org/news by guest on January 17, 2021
PEDIATRICS Volume 138, number 2, August 2016 7TABLE 2 Association of Study-Level Variables With Estimated Sensitivity and Specificity
Study-Level Variable Sensitivity Specificity P for Joint Test
OR (95% CI) P OR (95% CI) P
Mean gestational age (per 1-wk increase) 0.84 (0.68–1.04) .11 1.29 (0.98–1.61) .04 .11
Mean birth weight (per 100-g increase) 0.86 (0.72–1.03) .09 1.21 (1.00–1.48) .05 .14
Mean age at early assessment (per 1-y 1.51 (0.77–2.98) .22 0.79 (0.36–1.72) .54 .35
increase)
Mean age at school-age assessment (per 0.98 (0.86–1.11) .73 1.01 (0.88–1.17) .86 .90
1-y increase)
Mean time between assessments (per 1-y 0.97 (0.86–1.10) .57 1.02 (0.89–1.17) .78 .82
increase)
Earliest year of birth (per 1-y increase) 0.99 (0.97–1.01) .291 0.99 (0.97–1.01) .23 .82
OR, odds ratio
in the review, and the funnel plot
symmetry confirmed no publication
bias by sample size. Hence, there is
no reason to presume that different
conclusions would be drawn. We
used available aggregated data and
were unable to verify data accuracy.
Although we had attempted to focus
the review on studies published since
1990, only 14 of the 24 included
studies recruited participants born
after 1990, and no participant was
born in the last 10 years. The past
couple of decades have seen an
overall reduction in the proportions
of survivors of very preterm birth
with adverse neurodevelopmental
outcomes at age 2 years,45–47 so we
can expect the characteristics of the
current preterm population to be
different than those from past eras.
FIGURE 5 Furthermore, the assessment tools
Funnel plot of the log DOR against the inverse of the square root of the effective sample size, with
pseudo 95% CIs. used in the included studies, although
validated and contemporary at the
This review sought to answer a wide. The use of a meta-analytic time of each study, have mostly
clinically relevant question that, approach increases the sample size been superseded by newer editions.
for individual cohort studies, and improves the precision of the For example, the BSID is now in its
pooled estimate. third edition.48 Recent studies have
would involve lengthy follow-up
suggested that children achieve
and significant resources. One of
However, we recognize weaknesses higher scores on the third edition of
the key strengths of the review is
in our study. It is possible that the the Bayley Scales compared with the
the systematic and comprehensive
included studies represent a biased second edition when concurrently
literature search that is highly tested with both versions.49,50
sample because a large number of
sensitive in capturing all available Therefore, caution should be
eligible studies were not included
data relevant to the research exercised when extrapolating from
because of nonresponse, refusal, or
question in different settings. the data was no longer accessible. results based on earlier versions
Because the sensitivity estimates However, the nonincluded studies of the assessment tools. Although
from individual studies were based share similar study characteristics psychometric property differences
on small numbers of participants (year of publication, countries where exist, all the assessment tools provide
with cognitive impairment, the the studies were conducted, inclusion comparative information of an
corresponding 95% CIs were very criteria, assessment tools) to those individual’s development in reference
Downloaded from www.aappublications.org/news by guest on January 17, 2021
8 WONG et alto age-appropriate normative data on and support or discharged from before the age of 1 year and nearly
the same scale. follow-up. Reassuringly, we found the half of the follow-up data were
false-positive rate for early diagnosis based on testing before school age.
We investigated the source of
of impairment to be low. It is likely The convergent validity of MDI
heterogeneity between studies using
that children with more severe scores and cognitive scores may
meta-regression. This method has a
impairments would be correctly reflect the short interval between
few drawbacks. The statistical power
identified at this stage. However, testing in this case. More crucially,
to detect associations between the
children with milder impairments, the statistical measures used in our
study estimates and the explanatory
who are harder to diagnose, may study (sensitivity and specificity)
variables is related to the magnitude
miss out on the potential advantages and the published meta-analysis
of the relationship between them,
of cognitive intervention programs. (correlation coefficient) evaluate
and is typically considered low
different test properties. Although
in meta-regression.51 This was Cognitive function in infancy is a poor
sensitivity and specificity assessed
compounded by the narrow range predictor of later IQ in the general
the stability of diagnosis defined as
of values available for each of population.54 This may reflect real
a dichotomous variable, correlation
the explanatory variables under changes in cognitive function during
coefficient measures the strength
evaluation. For example, the mean childhood, unveiling of deficits in
and direction of a linear relationship
gestational age of the included complex task performance that were
between 2 continuous variables. In
studies ranged from 25.9 to 33.1 nonessential in early childhood,
a hypothetical scenario where the
weeks. Hence, we cannot exclude or the increasing effect of social
1-year BSID MDI always fall 20 points
the possibility of a type II error. and environmental influences on
below the IQ measured at 10 years,
More importantly, meta-regression cognitive outcomes over time. Other
the measured correlation would be
is subjected to ecological fallacy explanations may be the impact
perfect, but the sensitivity would still
(or aggregation bias). Therefore, to of behavior and attention during
be poor.
identify factors reliably that influence testing at different ages as well as
the validity of early developmental the differences in the content and
assessments, it would be necessary to psychometric properties of early
CONCLUSIONS
use individual patient-level data. neurodevelopmental and later
cognitive assessment tools. It has Early neurodevelopmental
Early intervention programs,
been reported that IQ scores from assessment has high specificity and
initiated within the first 12 months
childhood to adulthood were more NPV, but low sensitivity in identifying
of postterm life, are known to
stable for very preterm/VLBW later school-age cognitive deficit. A
promote neurodevelopment among
than for term-born individuals, significant number of older children
preterm infants.52 We do not have
particularly among those with severe and adolescents born very preterm
the necessary information on
cognitive impairment.55 or VLBW experience difficulties in
whether study participants were
school and are a group that might
offered or received early intervention In 2013, a meta-analysis similar to
have benefitted from earlier support
to evaluate its effect. A Cochrane our study on the predictive value of
and intervention had their cognitive
review of 25 randomized controlled the BSID on later very preterm and/
deficits been recognized. We would
trials of early intervention programs or VLBW outcomes was published by
encourage future studies of the
reported that the cognitive benefit Luttikhuizen dos Santos et al.56 They
factors affecting the diagnostic
observed in infancy and at preschool reported a strong positive correlation
and predictive accuracy of early
age did not persist into school age.53 between BSID MDI in the first 3 years
neurodevelopmental assessments
However, most of these programs after birth and later cognitive scores
so as to identify follow-up schedules
terminate within the first year (pooled correlation coefficient: 0.61;
that have a maximal likelihood of
after birth, and little work has been 95% CI, 0.57–0.64) that accounted
detecting impairment.
done on cognitive rehabilitation for 37% of the variance in cognitive
or training programs that are functioning. There are several
sustained beyond toddlerhood. important methodological differences
ACKNOWLEDGMENTS
Neurodevelopmental assessment between this meta-analysis and
at 2 or 3 years of age is often used our study. Only studies using the Members of the Medicines for
as the endpoint for postdischarge BSID were included in the Dutch Neonates Investigator Group are Prof
follow-up of very preterm or VLBW meta-analysis and studies published Deborah Ashby (Imperial College
infants. Depending on the diagnosis before 1990 were not excluded. The London, United Kingdom), Prof Peter
at this stage, children are either meta-analysis incorporated early Brocklehurst (University College
referred for further intervention neurodevelopmental data obtained London, United Kingdom), Prof Kate
Downloaded from www.aappublications.org/news by guest on January 17, 2021
PEDIATRICS Volume 138, number 2, August 2016 9Costeloe (Queen Mary University (University Medical Centre, Utrecht, Hamburg, Germany), Prof Dieter
of London, United Kingdom), Prof Netherlands), Prof Ermellina Fedrizzi Wolke (University of Warwick,
Elizabeth Draper (University of (University of Padua, Italy), Prof United Kingdom), and Prof Lianne
Leicester, United Kingdom), Prof Vineta Fellman (Lund University, Woodward (Harvard Medical School,
Azeem Majeed (Imperial College Sweden), Prof Peter Gray (Mater Boston, MA).
London, United Kingdom), Prof Neena Mothers’ Hospital, Brisbane,
Modi (Imperial College London, Australia), Prof Howard Kilbride
United Kingdom) Prof Stavros (University of Missouri-Kansas City, ABBREVIATIONS
Petrou (University of Warwick, Kansas City, MO), Prof Neil Marlow
BSID: Bayley Scales of Infant
United Kingdom), Prof Alys Young (University College London, United
Development
(University of Manchester, United Kingdom), Prof Jennifer Pinto-
BSID-II: Bayley Scales of Infant
Kingdom), Mrs Jane Abbott and Ms Martin (University of Pennsylvania,
Development, second
Zoe Chivers (Bliss Charity, London, Philadelphia, PA), Prof Jon Skranes
edition
United Kingdom), and Mrs Jacquie (Norwegian University of Science &
CI: confidence interval
Kemp (London, United Kingdom). Technology, Trondheim, Norway),
DOR: diagnostic odds ratio
We thank the following investigators Prof Karen Smith (The University
ESS: effective sample size
who contributed unpublished and of Texas Medical Branch, Galveston,
HSROC: hierarchical summary
supplemental data for the review: Dr TX), Prof Mary Sullivan (University
receiver operator char-
Haim Bassan (Tel Aviv University, of Rhode Island, Kingston, RI),
acteristics
Israel), Prof Arend Bos (Beatrix Prof Paul Swank (The University
MDI: Mental Development Index
Children’s Hospital, Groningen, of Texas Health Science Center at
NPV: negative predictive value
Netherlands), Dr Marie-Laure Houston, Houston, TX ), Prof H.
PPV: positive predictive value
Charkaluk (Lille Catholic University, Gerry Taylor (Case Western Reserve
QUADAS-2: Quality of Diagnostic
Paris Descartes University, France), University, Cleveland, OH), Dr Viena
Accuracy Studies
Dr Sarale Cohen (retired), Prof Tommiska (Helsinki University
version 2
Olaf Dammann (Tufts University, Central Hospital, Finland), Dr Norbert
VLBW: very low birth weight
Boston, MA), Prof Linda de Vries Veelken (Asklepios Klinik Nord,
Accepted for publication May 24, 2016
Address correspondence to Neena Modi, MD, Section of Neonatal Medicine, Imperial College London, Chelsea & Westminster Hospital Campus, 369 Fulham Rd,
London SW9 1NH, United Kingdom. E-mail: n.modi@imperial.ac.uk
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2016 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose.
FUNDING: This paper represents independent research funded by the National Institute for Health Research (NIHR) under its Programme Grants for Applied
Research Programme (Reference RP-PG-0707-10010). The views expressed are those of the authors and not necessarily those of the National Health Service, the
NIHR, or the Department of Health.
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
REFERENCES
1. Marlow N. Neurocognitive outcome Group. Stability of cognitive outcome of Infant Development for cognitive
after very preterm birth. Arch from 2 to 5 years of age in very low function of extremely low birth weight
Dis Child Fetal Neonatal Ed. birth weight children. Pediatrics. children at school age. Pediatrics.
2004;89(3):F224–F228 2012;129(3):503–508 2005;116(2):333–341
2. Doyle LW, Anderson PJ. Adult outcome 5. Potharst ES, Houtzager BA, van 7. Roberts G, Anderson PJ, Doyle LW;
of extremely preterm infants. Sonderen L, et al. Prediction of Victorian Infant Collaborative Study
Pediatrics. 2010;126(2):342–351 cognitive abilities at the age of 5 Group. The stability of the diagnosis of
3. Aylward GP. Cognitive and years using developmental follow-up developmental disability between ages
neuropsychological outcomes: more assessments at the age of 2 and 3 2 and 8 in a geographic cohort of very
than IQ scores. Ment Retard Dev years in very preterm children. Dev preterm children born in 1997. Arch
Disabil Res Rev. 2002;8(4):234–240 Med Child Neurol. 2012;54(3):240–246 Dis Child. 2010;95(10):786–790
4. Munck P, Niemi P, Lapinleimu H, 6. Hack M, Taylor HG, Drotar D, et al. Poor 8. Whiting PF, Rutjes AW, Westwood ME,
Lehtonen L, Haataja L; PIPARI Study predictive validity of the Bayley Scales et al; QUADAS-2 Group. QUADAS-2: a
Downloaded from www.aappublications.org/news by guest on January 17, 2021
10 WONG et alrevised tool for the quality assessment 18. Fedrizzi E, Inverno M, Botteon G, care unit survivors with various
of diagnostic accuracy studies. Ann Anderloni A, Filippini G, Farinotti M. neonatal morbidities. Pediatrics.
Intern Med. 2011;155(8):529–536 The cognitive development of children 2000;106(6):1397–1405
born preterm and affected by spastic
9. Deeks JJ. Systematic reviews of 28. Orchinik LJ, Taylor HG, Espy KA,
diplegia. Brain Dev. 1993;15(6):428–432
evaluations of diagnostic and et al. Cognitive outcomes for
screening tests. In: Egger M, Davey 19. Gray PH, Burns YR, Mohay HA, extremely preterm/extremely
Smith G, Altman DG, eds. Systematic O’Callaghan MJ, Tudehope DI. low birth weight children in
reviews in health care: meta-analysis Neurodevelopmental outcome kindergarten. J Int Neuropsychol Soc.
in context, 2nd ed. London: BMJ; of preterm infants with 2011;17(6):1067–1079
2001:248–282 bronchopulmonary dysplasia.
29. Reuss ML, Paneth N, Pinto-Martin JA,
Arch Dis Child Fetal Neonatal Ed.
10. Rutter CM, Gatsonis CA. A Lorenz JM, Susser M. The relation of
1995;73(3):F128–F134
hierarchical regression approach transient hypothyroxinemia in preterm
to meta-analysis of diagnostic test 20. Gray PH, O’Callaghan MJ, Rogers infants to neurologic development
accuracy evaluations. Stat Med. YM. Psychoeducational outcome at two years of age. N Engl J Med.
2001;20(19):2865–2884 at school age of preterm 1996;334(13):821–827
infants with bronchopulmonary
11. Deeks JJ, Macaskill P, Irwig L. The 30. Pinto-Martin JA, Whitaker AH, Feldman
dysplasia. J Paediatr Child Health.
performance of tests of publication JF, Van Rossem R, Paneth N. Relation
2004;40(3):114–120
bias and other sample size effects of cranial ultrasound abnormalities
in systematic reviews of diagnostic 21. Gray D, Woodward LJ, Spencer C, in low-birthweight infants to motor
test accuracy was assessed. J Clin Inder TE, Austin NC. Health service or cognitive performance at ages 2,
Epidemiol. 2005;58(9):882–893 utilisation of a regional cohort of 6, and 9 years. Dev Med Child Neurol.
very preterm infants over the first 2 1999;41(12):826–833
12. Bassan H, Stolar O, Geva R, et al. years of life. J Paediatr Child Health.
31. Pinto-Martin J, Whitaker A, Feldman
Intrauterine growth-restricted 2006;42(6):377–383
J, et al. Special education services
neonates born at term or preterm:
22. Pritchard VE, Clark CA, Liberty K, and school performance in a regional
how different? Pediatr Neurol.
Champion PR, Wilson K, Woodward LJ. cohort of low-birthweight infants
2011;44(2):122–130
Early school-based learning difficulties at age nine [published correction
13. Bowen JR, Gibson FL, Leslie GI, Arnold in children born very preterm. Early appears in Paediatr Perinat Epidemiol.
JD, Ma PJ, Starte DR. Predictive Hum Dev. 2009;85(4):215–224 2004;18(6):467]. Paediatr Perinat
value of the Griffiths assessment in Epidemiol. 2004;18(2):120–129
23. Kilbride HW, Daily DK, Claflin K, Hall
extremely low birthweight infants. J
RT, Maulik D, Grundy HO. Improved 32. Lorenz JM, Whitaker AH, Feldman JF,
Paediatr Child Health. 1996;32(1):25–30
survival and neurodevelopmental et al. Indices of body and brain size
14. Bruggink JL, Van Braeckel KN, Bos outcome for infants less than 801 at birth and at the age of 2 years:
AF. The early motor repertoire of grams birthweight. Am J Perinatol. relations to cognitive outcome at
children born preterm is associated 1990;7(2):160–165 the age of 16 years in low birth
with intelligence at school age. weight infants. J Dev Behav Pediatr.
24. Kilbride HW, Daily DK. Survival and
Pediatrics. 2010;125(6). Available at: 2009;30(6):535–543
subsequent outcome to five years of
http://pediatrics.aappublications.org/ age for infants with birth weights less 33. Skranes J, Vik T, Nilsen G, Smevik
content/125/6/e1356. than 801 grams born from 1983 to O, Andersson HW, Brubakk AM. Can
15. Charkaluk ML, Truffert P, Marchand- 1989. J Perinatol. 1998;18(2):102–106 cerebral MRI at age 1 year predict
Martin L, et al; Epipage study group. motor and intellectual outcomes in
25. Marlow N, Wolke D, Bracewell MA,
Very preterm children free of disability very-low-birthweight children? Dev
Samara M; EPICure Study Group.
or delay at age 2: predictors of Med Child Neurol. 1998;40(4):256–262
Neurologic and developmental
schooling at age 8: a population-based disability at six years of age after 34. Smith KE, Landry SH, Swank PR. The
longitudinal study. Early Hum Dev. extremely preterm birth. N Engl J Med. role of early maternal responsiveness
2011;87(4):297–302 2005;352(1):9–19 in supporting school-aged cognitive
16. Claas MJ, de Vries LS, Bruinse HW, development for children who
26. Johnson S, Fawke J, Hennessy E,
et al. Neurodevelopmental outcome vary in birth status. Pediatrics.
et al. Neurodevelopmental disability
over time of preterm born children 2006;117(5):1608–1617
through 11 years of age in children
≤750 g at birth. Early Hum Dev. born before 26 weeks of gestation. 35. Tommiska V, Heinonen K, Kero P, et al.
2011;87(3):183–191 Pediatrics. 2009;124(2). Available at: A national two year follow up study
http://pediatrics.aappublications.org/ of extremely low birthweight infants
17. Cohen SE. Biosocial factors in early
content/124/2/e249. born in 1996-1997. Arch Dis Child Fetal
infancy as predictors of competence
Neonatal Ed. 2003;88(1):F29–F35
in adolescents who were born 27. McGrath MM, Sullivan MC, Lester
prematurely. J Dev Behav Pediatr. BM, Oh W. Longitudinal neurologic 36. Mikkola K, Ritari N, Tommiska V, et al.
1995;16(1):36–41 follow-up in neonatal intensive Neurodevelopmental outcome at
Downloaded from www.aappublications.org/news by guest on January 17, 2021
PEDIATRICS Volume 138, number 2, August 2016 115 years of age of a national cohort of 43. Wolke D, Schulz J, Meyer R. Longterm 50. Lowe JR, Erickson SJ, Schrader R,
extremely low birth weight infants who developmental outcome of very Duncan AF. Comparison of the Bayley
were born in 1996-1997. Pediatrics. prematurely born infants. Bavarian II Mental Developmental Index and
2005;116(6):1391–1400 longitudinal study. Monatsschrift the Bayley III Cognitive Scale: are
Kinderheilkunde. 2001;149(13):53–61 we measuring the same thing? Acta
37. Veelken N, Stollhoff K, Claussen paediatrica. 2012;101(2):e55–e58
M. Development of very low birth 44. Saigal S, den Ouden L, Wolke D, et al.
weight infants: a regional study School-age outcomes in children 51. Bossuyt P, Davenport C, Deeks J, Hyde
of 371 survivors. Eur J Pediatr. who were extremely low birth C, Leeflang M, Scholten R. Interpreting
1991;150(11):815–820 weight from four international results and drawing conclusions
population-based cohorts. Pediatrics. [Cochrane review]. In: Cochrane
38. Dammann O, Drescher J, Veelken 2003;112(4):943–950 Handbook for Systematic Reviews of
N. Maternal fever at birth and non- Diagnostic Test Accuracy. Version 0.9.
verbal intelligence at age 9 years in 45. Salt A, D’Amore A, Ahluwalia J, et al; Oxford, United Kingdom ; 2013
preterm infants. Dev Med Child Neurol. East Anglian Very Low Birthweight 52. Spittle A, Orton J, Anderson PJ, Boyd
2003;45(3):148–151 Project Group. Outcome at 2 years R, Doyle LW. Early developmental
for very low birthweight infants intervention programmes provided
39. Vermeulen GM, Bruinse HW, de Vries in a geographical population:
LS. Perinatal risk factors for adverse post hospital discharge to prevent
risk factors, cost, and impact of motor and cognitive impairment in
neurodevelopmental outcome congenital anomalies. Early Hum Dev.
after spontaneous preterm birth. preterm infants. Cochrane Database
2006;82(2):125–133 Syst Rev. 2015;11:CD005495
Eur J Obstet Gynecol Reprod Biol.
2001;99(2):207–212 46. Wilson-Costello D, Friedman H, Minich 53. Spittle A, Orton J, Anderson PJ, Boyd
N, et al. Improved neurodevelopmental R, Doyle LW. Early developmental
40. Rademaker KJ, Uiterwaal CS, outcomes for extremely low birth intervention programmes provided
Groenendaal F, et al. Neonatal weight infants in 2000-2002. Pediatrics. post hospital discharge to prevent
hydrocortisone treatment: 2007;119(1):37–45 motor and cognitive impairment in
neurodevelopmental outcome preterm infants. Cochrane Database
and MRI at school age in 47. Doyle LW, Roberts G, Anderson PJ; Syst Rev. 2015; (11):CD005495
preterm-born children. J Pediatr. Victorian Infant Collaborative Study
2007;150(4):351–357 Group. Changing long-term outcomes 54. Aylward GP. Prediction of function from
for infants 500-999 g birth weight in infancy to early childhood: implications
41. Wolke D, Meyer R. Cognitive status, Victoria, 1979-2005. Arch Dis Child Fetal for pediatric psychology. J Pediatr
language attainment, and prereading Neonatal Ed. 2011;96(6):F443–F447 Psychol. 2004;29(7):555–564
skills of 6-year-old very preterm 55. Breeman LD, Jaekel J, Baumann
children and their peers: the Bavarian 48. Bayley N. Technical manual for the N, Bartmann P, Wolke D. Preterm
Longitudinal Study. Dev Med Child Bayley Scales of Infant and Toddler Cognitive Function Into Adulthood.
Neurol. 1999;41(2):94–109 Development, 3rd ed. San Antonio, TX: Pediatrics. 2015;136(3):415–423
Psychological Corporation; 2006
42. Gutbrod T, Wolke D, Soehne B, Ohrt B, 56. Luttikhuizen dos Santos ES, de
Riegel K. Effects of gestation and birth 49. Moore T, Johnson S, Haider S, Kieviet JF, Königs M, van Elburg RM,
weight on the growth and development Hennessy E, Marlow N. Relationship Oosterlaan J. Predictive value of the
of very low birthweight small for between test scores using the second Bayley scales of infant development on
gestational age infants: a matched and third editions of the Bayley Scales development of very preterm/very low
group comparison. Arch Dis Child Fetal in extremely preterm children. birth weight children: a meta-analysis.
Neonatal Ed. 2000;82(3):F208–F214 J Pediatr. 2012;160(4):553–558 Early Hum Dev. 2013;89(7):487–496
Downloaded from www.aappublications.org/news by guest on January 17, 2021
12 WONG et alDevelopmental Assessments in Preterm Children: A Meta-analysis
Hilary S. Wong, Shalini Santhakumaran, Frances M. Cowan, Neena Modi and
Medicines for Neonates Investigator Group
Pediatrics originally published online July 28, 2016;
Updated Information & including high resolution figures, can be found at:
Services http://pediatrics.aappublications.org/content/early/2016/07/26/peds.2
016-0251
References This article cites 52 articles, 17 of which you can access for free at:
http://pediatrics.aappublications.org/content/early/2016/07/26/peds.2
016-0251#BIBL
Subspecialty Collections This article, along with others on similar topics, appears in the
following collection(s):
Developmental/Behavioral Pediatrics
http://www.aappublications.org/cgi/collection/development:behavior
al_issues_sub
Fetus/Newborn Infant
http://www.aappublications.org/cgi/collection/fetus:newborn_infant_
sub
Neonatology
http://www.aappublications.org/cgi/collection/neonatology_sub
Permissions & Licensing Information about reproducing this article in parts (figures, tables) or
in its entirety can be found online at:
http://www.aappublications.org/site/misc/Permissions.xhtml
Reprints Information about ordering reprints can be found online:
http://www.aappublications.org/site/misc/reprints.xhtml
Downloaded from www.aappublications.org/news by guest on January 17, 2021Developmental Assessments in Preterm Children: A Meta-analysis
Hilary S. Wong, Shalini Santhakumaran, Frances M. Cowan, Neena Modi and
Medicines for Neonates Investigator Group
Pediatrics originally published online July 28, 2016;
The online version of this article, along with updated information and services, is
located on the World Wide Web at:
http://pediatrics.aappublications.org/content/early/2016/07/26/peds.2016-0251
Data Supplement at:
http://pediatrics.aappublications.org/content/suppl/2016/07/20/peds.2016-0251.DCSupplemental
Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
has been published continuously since 1948. Pediatrics is owned, published, and trademarked by
the American Academy of Pediatrics, 345 Park Avenue, Itasca, Illinois, 60143. Copyright © 2016
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.
Downloaded from www.aappublications.org/news by guest on January 17, 2021You can also read