Diabetes Symptoms and Distress in ACCORD Trial Participants: Relationship to Baseline Clinical Variables
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
F e a t u r e A r t i c l e
Diabetes Symptoms and Distress in ACCORD Trial
Participants: Relationship to Baseline Clinical Variables
Mark D. Sullivan, MD, PhD, Gregory Evans, MA, Roger Anderson, PhD, Patrick O’Connor, MD, MPH,
Dennis W. Raisch, PhD, Debra L. Simmons, MD, MS, and K.M. Venkat Narayan, MD, MBA
T
ype 2 diabetes may lead to association of diabetes symptoms or at least two additional CVD risk
a variety of symptoms such and distress with patients’ overall factors (dyslipidemia, hyperten-
as excessive thirst, frequent health state as measured by a feeling sion, current status as a smoker,
urination, fatigue, and burning feet. thermometer. The feeling thermom- or obesity). Key exclusion criteria
These symptoms diminish quality of eter allows patients to rate their included frequent or recent serious
life, impair functional status, and current overall health between 100 hypoglycemia events, unwillingness
contribute to the psychological (perfect health) and 0 (death). to perform self-monitoring of blood
distress experienced by patients with glucose or inject insulin, a BMI
diabetes.1–4 However, there is no Study Methods > 45 kg/m2, a serum creatinine level
established metric for the severity of Study population > 1.5 mg/dl, or other serious illness.
diabetes symptoms and associated The rationale and design of the A total of 10,251 participants were
distress. Action to Control Cardiovascular Risk recruited and randomly assigned to
Many diabetes symptoms in Diabetes (ACCORD) trial and its either intensive glycemia-lowering
are linked through established health-related quality of life substudy with a target A1C < 6.0% or standard
pathophysiological mechanisms have been reported previously.8,9 glycemia management with a target
to inadequate short- or long-term Briefly, the ACCORD trial, spon- A1C of 7.0–7.9%.
glucose control or acute hypoglyce- sored by the National Heart, Lung, The study protocol was approved
mia. But studies to date suggest that and Blood Institute (NHLBI), was by the institutional review board or
the relationship between severity of conducted in 77 clinical centers across ethics committee at each center, as
diabetes symptoms and measures the United States and Canada. well as by an ethics review panel at
of glucose control such as A1C is We recruited participants with the NHLBI. All patients provided
weak.5–7 type 2 diabetes and an A1C ≥ 7.5% written informed consent.
A better understanding of factors and who either were 1) between the Of the 10,251 patients enrolled
that amplify or dampen diabetes- ages of 40 and 79 years and had in the trial, a randomly selected
related symptoms could lead to cardiovascular disease (CVD) or 2) subsample of 2,053 participants
improved approaches to maxi- between the ages of 55 and 79 years from each of the clinical centers
mize the quality of life of diabetes and had anatomical evidence of was enrolled in a substudy concern-
patients. The purpose of this study significant atherosclerosis, albumin- ing health-related quality of life
was to describe the relationship of uria, left-ventricular hypertrophy, (HRQL). The ACCORD HRQL
scores on the Diabetes Symptoms substudy was designed to assess
Distress Questionnaire to demo- In Brief three distinct outcomes: general
graphic and clinical variables for health, treatment satisfaction,
patients with type 2 diabetes. This Our study demonstrates strong and diabetes-related symptoms.
included an evaluation of the cross- associations of diabetes symptoms This report focuses on associa-
sectional association of diabetes and distress with female sex, higher tions between baseline symptoms
BMI, history of neuropathy, and
symptoms and distress with demo- and symptom distress, a feeling
current depressive symptoms.
graphic and clinical variables such thermometer used to rate patients’
Many diabetes-specific symptoms
as A1C, LDL cholesterol, blood general health state, and multiple
may be significantly shaped by
pressure, diabetes duration and demographic and clinical variables.
factors such as depression and
complications, and depression It includes all ACCORD study
obesity.
status. We also examined the subjects who were enrolled in the
Clinical Diabetes • Volume 30, Number 3, 2012 101F e a t u r e A r t i c l e
ACCORD HRQL substudy and who physical exam. Systolic and diastolic used to assess associations between
completed baseline data collection. blood pressure levels were deter- the four dependent variables and the
The ACCORD HRQL methods have mined using the average of three feeling thermometer. Results for the
been described previously.10 readings using an Omron device two methods were quite similar (all
(Omron Inc., Kyoto, Japan). coefficients agreed ± 0.05), and only
Key measures Depression was assessed using Pearson correlation coefficients are
We used the Diabetes Symptom the nine-item depression mea- presented here.
Distress Questionnaire developed sure from the Patient Health
by Anderson and Testa11 to assess 60 Questionnaire (PHQ-9). The PHQ-9 Ethical approval
individual symptoms of diabetes and is the self-report version of the The University of Washington
its treatment. This measure has been Primary Care Evaluation of Mental Institutional Review Board for
previously validated against physi- Disorders questionnaire, a well- the Protection of Human Subjects
cian report of patient symptoms.11 It validated psychiatric diagnostic approved this research, as did the
discriminates between patients with interview for use in primary care Institutional Review Boards of the
diabetes and those with hyperten- settings.14 In this analysis, we used other ACCORD clinical networks
sion12 and distinguishes between the PHQ-9 mean score and whether and the clinics where data were
patients with type 2 diabetes random- the score exceeded the threshold collected.
ized to glipizide or placebo.1 With suggesting major depression (a score
this questionnaire, subjects reported Study Results
≥ 10 on the PHQ-9). We also assessed
whether they had experienced a given patients’ history of depression and Baseline sample characteristics
symptom or feeling. If they had expe- use of antidepressant medications at Table 1 displays the characteristics
rienced it, then they were asked “How baseline. of the 1,950 study subjects who were
distressing was it?” according to this Finally, a feeling thermometer included in the ACCORD HRQL sub-
scale: 0 = not at all; 1 = somewhat; instrument15 was used to assess each study and provided complete baseline
2 = moderately; 3 = very much; and participant’s overall health percep- data. The study sample had a mean
4 = extremely. For each participant, tions.16 This instrument consists of a age of 62 years and was 60% male;
we calculated the total symptom single-item visual analog scale with 60% had post-secondary education,
count and the mean symptom distress which participants are asked to rate 80% lived with other adults, and 66%
(assigning participants not experienc- their current (today) health state were Caucasian. The mean duration
ing the symptom a distress score of from 0 (worst imaginable) to 100 of diabetes was just over 11 years. The
0). We also examined the relationship (best imaginable). mean baseline A1C was 8.3 ± 1%, with
between these and an overall rating 56% of the sample having an A1C of
of the patient’s health state using a Statistical analysis ≥ 8%.
feeling thermometer. We used both simple and multiple
Participant age, sex, ethnicity, linear regression analyses to assess Patient responses to Diabetes
educational level, social support relationships between demographic, Symptoms Distress Questionnaire
(living alone vs. living with oth- diabetes, and depression status and The 10 most commonly endorsed
ers), diabetes duration, history of the specified dependent variables. symptoms on the Diabetes Symptoms
eye disease, history of neuropathy, Separate models were fit for each Distress Questionnaire were: drowsy
and medication use were based on of the four dependent variables. or sleepy (59%), getting up often at
self-report. A central laboratory Multiple linear regression models night to urinate (57%), feeling over-
(with National Glycohemoglobin generally took this form: Diabetes weight (57%), tired or being weary
Standardization Program level I symptoms = demographics (step 1) (57%), being thirsty (50%), numbness
certification) analyzed blood for A1C + diabetes duration and A1C and of hands or feet (50%), having to
and lipid levels. Total cholesterol, complications (step 2) + depression urinate frequently (50%), drinking
HDL cholesterol, and fasting triglyc- (step 3) + glucose, blood pressure, a lot of fluids (50%), general weak-
eride concentrations were measured and lipid treatments (step 4). Given ness or fatigue (48%), and lethargy
enzymatically, and LDL cholesterol the large number of tests performed, or no energy to do things (44%).
was calculated using the Friedewald only those associations significant at These were generally also rated as
formula.13 BMI and Michigan the P < 0.001 level were considered the most distressing symptoms. The
Neuropathy Screening Instrument statistically significant. Pearson and most distressing symptom (range
(MNSI) scores were determined by Spearman rank correlations were 0–4) was feeling overweight (mean
102 Volume 30 Number 3, 2012• Clinical DiabetesF e a t u r e A r t i c l e
majority reporting multiple symp-
Table 1. Demographic and Clinical Characteristics of Study Subjects (n = 1,950)
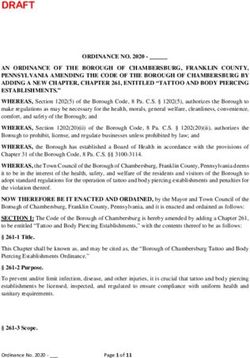
toms. The mean symptom count was
Characteristic Percentage or Mean (SD) 17.1. The median number of symp-
Mean age (years) 62.3 (6.7) toms was 15.0. Figure 2 displays the
distribution of symptom distress
Female (%) 39.8 in the study population. Symptom
Having post-secondary education (%) 59.8 distress was generally low, with 73%
reporting mean distress between 0
Living with other adults (%) 80.0 and 1 on the four-point scale. The
Caucasian (%) 65.9 overall mean for distress was 0.7, and
the median distress score was 0.6.
Mean duration of diabetes (years) 11.1 (7.9) Total symptom count was highly
Mean baseline A1C (%) 8.3 (1) correlated with mean symptom dis-
tress (Pearson r = 0.88, P < 0.0001).
Having baseline A1C ≥ 8% (%) 55.6 Symptom count (r = –0.35,
Reporting history of neuropathy (%) 27.5 P < 0.0001) and symptom dis-
tress (r = –0.36, P < 0.0001) were
Having foot amputation or MNSI score > 2 (%) 43.1
significantly and similarly correlated
Reporting history of eye disease (%) 29.7 with the overall health state rating
on the feeling thermometer.
Mean BMI (kg/m ) 2
32.4 (5.5)
Mean systolic blood pressure (mmHg) 136.3 (17.1) Univariate relationships between
symptoms, distress, and clinical
Mean diastolic blood pressure (mmHg) 74.4 (10.9) variables
Mean total cholesterol (mg/dl) 182.8 (41.1) Table 2 displays the univariate rela-
tionships between symptoms, distress,
Mean LDL cholesterol (mg/dl) 104.1 (33.8)
and clinical variables. Total symptom
Mean HDL cholesterol (mg/dl) 42.1 (11.6) count was significantly and negatively
associated with age. It was signifi-
Mean triglyceride level (mg/dl) 189.2 (140.2)
cantly and positively associated with
Reporting history of depression (%) 24.6 female sex, history of neuropathy,
Using antidepressant medications (%) 14.0 BMI, serum triglygeride level, history
of depression, use of antidepressants,
Mean PHQ-9 score 5.4 (5.1) mean PHQ-9 score, having a PHQ-9
Having PHQ-9 score ≥ 10 (%) 19.6 score ≥ 10, and use of insulin. Mean
symptom distress was significantly
Using oral hypoglycemic medications only (%) 56.9 and negatively associated with age
Using insulin (%) 35.9 and use of only oral hypoglycemic
medications. Mean symptom distress
Using thiazides (%) 26.8
was significantly and positively asso-
Using β-blockers (%) 30.4 ciated with female sex, baseline mean
A1C, having a baseline A1C ≥ 8%,
Using ACE inhibitors (%) 52.0
history of neuropathy, BMI, total
Using statins (%) 63.5 cholesterol, triglyceride level, history
of depression, use of antidepres-
distress score of 2.2). Eight symptoms reaction, pain in legs or calves when sants, mean PHQ-9 score, having a
tied for the second most distressing walking, gaining weight, and inability PHQ-9 ≥ 10, and use of insulin.
(mean distress score 1.8), including to sleep or insomnia.
numbness or tingling of hands or feet, Figure 1 displays the distribu- Multivariable models for symptom
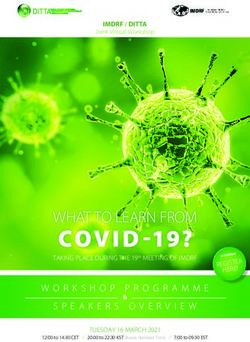
having to urinate frequently, lethargy tion of symptom counts in the study count, distress, and factors
or no energy to do things, foot cramps population. Less than 2% of subjects Multivariable models were derived in
or foot pain, high blood glucose reported no symptoms, with the vast a progressive manner, entering demo-
Clinical Diabetes • Volume 30, Number 3, 2012 103F e a t u r e A r t i c l e
associated with multiple factors when
these are considered individually,
including demographic and psycho-
logical variables and measures of
diabetes control and complications.
However, in multivariable models,
diabetes symptoms and distress are
significantly associated only with
sex, BMI, history of neuropathy,
and current depressive symptoms
(PHQ-9 score ≥ 10). These findings
suggest that efforts to reduce diabetes
symptoms should focus on strategies
to reduce neuropathy and depression.
We did not correct for any ongoing
depression treatment (medications or
psychotherapy) in our analyses.
Figure 1. Number of symptoms per participant. Previous research on diabetes
symptoms has shown a stronger
relationship between diabetes
symptom severity and the mental
component score of the Short Form-
36 Health Survey than the physical
component score.2 Other research
has suggested an important role for
depression in diabetes symptoms.
In a primary care sample of 4,168
patients with diabetes, Ludman et
al.6 found that patients with major
depression had more diabetes symp-
toms after adjusting for demographic
characteristics, objective measures
of diabetes severity, and medical
comorbidity. The overall number of
diabetes symptoms was related to the
number of depressive symptoms, and
Figure 2. Distribution of mean distress scores. depression was significantly related
to all of the 10 diabetes symptoms
graphic variables first, then diabetes primary outcomes: assessed. Previously, Ciechanowski
and cardiovascular risk variables, • Total symptom count was sig- et al.5 reported strong associa-
then depression variables, and then nificantly associated with female tions between diabetes symptoms
treatments for diabetes, blood pres- sex (β = 2.24), history of neuropathy and depression in a sample of 273
sure, and lipid control. These models (β = 3.71), and having a PHQ-9 diabetic patients recruited from a
are displayed in Table 3. score ≥ 10 (β = 11.13). specialty care setting.
Most predictor variables that • Symptom distress was significantly Depression in patients with
entered the multivariable models associated with history of neuropa- diabetes is likely both a cause and a
were significant at the P ≤ 0.001 thy (β = 0.10), BMI (β = 0.01), and consequence of diabetes symptoms,
level, and most remained signifi- PHQ-9 score ≥ 10 (β = 0.48). complications, and related health
cant in the more complete models. behaviors.17 Diabetes symptoms and
We therefore report only the final Discussion complications, smoking, and obesity
models including variables signifi- Diabetes symptom count and (BMI) have all been associated with
cant at P < 0.0001 for each of the two symptom-related distress appear to be an increased risk of depression in
104 Volume 30 Number 3, 2012• Clinical DiabetesF e a t u r e A r t i c l e
Table 2. Univariate Relationships With Symptom Outcomes
Characteristic Total Symptom Count Mean Distress
β SE P β SE P
Age (years) –0.169 0.038 < 0.0001 –0.007 0.001 < 0.0001
Sex (female vs. male) 3.817 0.512 < 0.0001 0.137 0.018 < 0.0001
Post-secondary education (yes vs. no) –0.118 0.519 0.821 –0.018 0.018 0.317
Living alone (yes vs. no) –1.00 0.636 0.114 –0.015 0.022 0.506
Caucasian (yes vs. no) 0.246 0.537 0.646 0.001 0.019 0.962
Duration of diabetes (years) 0.054 0.033 0.098 0.002 0.001 0.150
Baseline A1C (%) 0.557 0.243 0.022 0.037 0.009 < 0.0001
Baseline A1C ≥ 8% (yes vs. no) 1.590 0.511 0.002 0.079 0.018 < 0.0001
History of neuropathy (yes vs. no) 5.827 0.559 < 0.0001 0.195 0.020 < 0.0001
Foot amputation or MNSI score > 2 (yes vs. no) 1.596 0.513 0.002 0.051 0.018 0.005
History of eye disease (yes vs. no) 0.797 0.558 0.154 0.030 0.020 0.125
BMI (kg/m2) 0.387 0.045 < 0.0001 0.015 0.002 < 0.0001
Systolic blood pressure (mmHg) 0.000 0.015 0.989 0.000 0.001 0.892
Diastolic blood pressure (mmHg) 0.048 0.023 0.040 0.002 0.001 0.012
Total cholesterol (mg/dl) 0.021 0.006 0.001 0.001 0.000 < 0.0001
LDL cholesterol (mg/dl) 0.007 0.008 0.3669 0.000 0.000 0.154
HDL cholesterol (mg/dl) –0.004 0.022 0.8242 0.000 0.001 0.799
Triglyceride level (mg/dl) 0.008 0.002 < 0.0001 0.000 0.000 < 0.0001
History of depression (yes vs. no) 7.280 0.570 < 0.0001 0.268 0.020 < 0.0001
Using antidepressant medications (yes vs. no) 6.283 0.719 < 0.0001 0.258 0.025 < 0.0001
PHQ-9 score 1.311 0.040 < 0.0001 0.050 0.001 < 0.0001
PHQ-9 score ≥ 10 (yes vs. no) 13.357 0.566 < 0.0001 0.559 0.019 < 0.0001
Using oral hypoglycemics only (yes vs. no) –1.879 0.512 0.000 –0.086 0.018 < 0.0001
Using insulin (yes vs. no) 2.447 0.527 < 0.0001 0.111 0.018 < 0.0001
Using thiazides (yes vs. no) –0.238 0.574 0.678 –0.010 0.020 0.620
Using β-blockers (yes vs. no) 1.614 0.552 0.005 0.038 0.019 0.051
Using ACE inhibitors (yes vs. no) –0.743 0.509 0.145 –0.030 0.018 0.091
Using statins (yes vs. no) –0.229 0.529 0.666 –0.008 0.019 0.679
previous studies.18–21 This suggests ing and eating) exist in a mutually This pattern of reciprocal
that aversive symptoms (such as pain reinforcing pattern that exerts a interactions between symptom
from neuropathy), depression, and significant effect on patients’ overall severity, depression, and qual-
health behaviors associated with health state, as indicated by the feel- ity of life has been found in other
mood regulation (such as smok- ing thermometer findings. chronic diseases such as asthma22
Clinical Diabetes • Volume 30, Number 3, 2012 105F e a t u r e A r t i c l e
Table 3. Multivariable Relationships With Symptom Burden and Distress
Characteristic Total Symptom Count Mean Distress
β SE P β SE P
Age (years) –0.0223 0.0388 0.5658 –0.0003 0.0013 0.7909
Sex (female vs. male) 2.2421 0.5181 < 0.0001 0.0612 0.0169 0.0003
Post-secondary education (yes vs. no) 0.5286 0.4683 0.2591 0.0077 0.0153 0.6149
Living alone (yes vs. no) –0.0112 0.5607 0.9841 0.0211 0.0183 0.2479
Caucasian (yes vs. no) –0.5190 0.5092 0.3082 –0.0251 0.0166 0.1311
Duration of diabetes (years) 0.0168 0.0322 0.6021 –0.0003 0.0011 0.7396
Baseline A1C (%) 0.0060 0.2199 0.9784 0.0148 0.0072 0.0393
History of neuropathy (yes vs. no) 3.7069 0.5373 < 0.0001 0.1042 0.0175 < 0.0001
Foot amputation or MNSI score > 2 (yes vs. no) 0.8031 0.4757 0.0915 0.0219 0.0155 0.1572
History of eye disease (yes vs. no) –0.2710 0.5299 0.6091 –0.0050 0.0173 0.7726
BMI (kg/m2) 0.1395 0.0443 0.0017 0.0072 0.0014 < 0.0001
Systolic blood pressure (mmHg) 0.0110 0.0167 0.5093 0.0004 0.0005 0.478
Diastolic blood pressure (mmHg) 0.0067 0.0277 0.8091 0.0001 0.0009 0.892
Total cholesterol (mg/dl) 0.0031 0.0072 0.6701 0.0001 0.0002 0.7111
LDL cholesterol (mg/dl) 0.0077 0.0232 0.7415 0.0011 0.0008 0.163
Triglyceride level (mg/dl) 0.0038 0.0018 0.0328 0.0002 0.0001 0.0006
History of depression (yes vs. no) 2.1388 0.6303 0.0007 0.0517 0.0205 0.0118
Using antidepressant medications (yes vs. no) 0.6774 0.7454 0.3636 0.0488 0.0243 0.0446
PHQ-9 score ≥ 10 (yes vs. no) 11.1252 0.6105 < 0.0001 0.4804 0.0199 < 0.0001
Using oral hypoglycemic only (yes vs. no) 0.9480 0.9195 0.3026 0.0416 0.0300 0.1656
Using insulin (yes vs. no) 1.5094 0.9896 0.1274 0.0774 0.0322 0.0165
Using thiazides (yes vs. no) –0.3656 0.5111 0.4744 –0.0085 0.0167 0.6084
Using β-blockers (yes vs. no) 1.1790 0.5056 0.0198 0.0275 0.0165 0.0949
Using ACE inhibitors (yes vs. no) –0.9374 0.4524 0.0384 –0.0403 0.0147 0.0064
Using statins (yes vs. no) –0.1261 0.5001 0.801 0.0010 0.0163 0.951
and chronic kidney disease requiring Our analysis has some important waves of data will be necessary to
hemodialysis.23 Our study adds to limitations. First, the cross-sectional fully understand these complex
these other studies in supporting the study design precludes causal relationships.
idea that diabetes-specific symptoms inference. Longitudinal data Second, our sample is not rep-
are more significantly shaped by fac- are necessary to prove causality. resentative of the entire population
tors such as depression and obesity Because we posit reciprocal relation- of patients with type 2 diabetes.
than by severity and duration of ships between diabetes symptoms ACCORD participants had diabetes
diabetes per se. and their determinants, multiple for a mean of 10 years, were at high
106 Volume 30 Number 3, 2012• Clinical DiabetesF e a t u r e A r t i c l e
risk for cardiovascular events, and References diabetes. Postgrad Med J 64 (Suppl. 3):50–58,
discussion 90–52, 1988
were willing to undergo intensive 1
Testa MA, Simonson DC: Health
13
economic benefits and quality of life Friedewald WT, Levy RI, Fredrickson
treatment to control glucose, includ- during improved glycemic control in DS: Estimation of the concentration of
ing frequent clinic visits and the use patients with type 2 diabetes mellitus: a low-density lipoprotein cholesterol in
randomized, controlled, double-blind plasma, without use of the preparative
of insulin. trial. JAMA 280:1490–1496, 1998 ultracentrifuge. Clin Chem 18:499–502, 1972
Third, although we assessed 2
Gulliford MC, Mahabir D: 14
Spitzer RL, Kroenke K, Williams JB:
a broad range of factors for their Relationship of health-related quality of Validation and utility of a self-report version
life to symptom severity in diabetes of PRIME-MD: the PHQ primary care study.
associations with diabetes symp- mellitus: a study in Trinidad and Tobago. JAMA 282:1737–1744, 1999
toms, there are many other factors J Clin Epidemiol 52:773–780, 1999 15
EuroQol Group: EuroQol: a new facility
that could have been examined
3
Goddijn PP, Bilo HJ, Feskens EJ, for the measurement of health-related quality
Groeniert KH, van der Zee KI, Meyboom- of life. Health Policy 16:199–208, 1990
in metabolic (C-reactive protein), de Jong B: Longitudinal study on glycae- 16
Schunemann HJ, Griffith L, Jaeschke
physiological (nerve conduction mic control and quality of life in patients
with type 2 diabetes mellitus referred for R, Goldstein R, Stubbing D, Guyatt GH:
velocities), behavioral (exercise), and intensified control. Diabet Med 16:23–30, Evaluation of the minimal important
1999 difference for the feeling thermometer and
psychosocial (anxiety) domains that the St. George’s Respiratory Questionnaire
4
Currie CJ, Poole CD, Woehl A, Morgan in patients with chronic airflow obstruction.
may have affected the final multi- CL, Cawley S, Rousculp MD, Covington J Clin Epidemiol 56:1170–1176, 2003
variable models. MT, Peters JR: The health-related utility 17
Golden SH, Lazo M, Carnethon M,
and health-related quality of life of
In summary, our study demon- hospital-treated subjects with type 1 or Bertoni AG, Schreiner PJ, Diez Roux AV, Lee
HB, Lyketsos C: Examining a bidirectional
strates strong associations between type 2 diabetes with particular reference to
association between depressive symptoms
differing severity of peripheral neuropathy.
diabetes symptoms and distress and Diabetologia 49:2272–2280, 2006 and diabetes. JAMA 299:2751–2759, 2008
female sex, BMI, neuropathy, and 5
Ciechanowski PS, Katon WJ, Russo JE,
18
Katon W, von Korff M, Ciechanowski P,
Hirsch IB: The relationship of depressive Russo J, Lin E, Simon G, Ludman E, Walker
depression. These factors likely rein- E, Bush T, Young B: Behavioral and clinical
symptoms to symptom reporting, self-care
force each other, although precise and glucose control in diabetes. Gen Hosp factors associated with depression among
Psychiatry 25:246–252, 2003 individuals with diabetes. Diabetes Care
specification of these relationships 27:914–920, 2004
6
awaits longitudinal data. Ludman EJ, Katon W, Russo J, Von 19
Korff M, Simon G, Ciechanowski P, Lin Mier N, Bocanegra-Alonso A, Zhan
E, Bush T, Walker E, Young B: Depression D, Wang S, Stoltz SM, Acosta-Gonzalez RI,
Acknowledgments and diabetes symptom burden. Gen Hosp Zuniga MA: Clinical depressive symptoms
Psychiatry 26:430–436, 2004 and diabetes in a binational border
This work was supported by grants population. J Am Board Fam Med 21:223–
7
McKellar JD, Humphreys K, Piette JD: 233, 2008
from the NHLBI (N01-HC-95178, Depression increases diabetes symptoms by 20
N01-HC-95179, N01-HC-95180, complicating patients’ self-care adherence. Sacco WP, Wells KJ, Friedman
Diabetes Educ 30:485–492, 2004 A, Matthew R, Perez S, Vaughan CA:
N01-HC-95181, N01-HC-95182, 8
Adherence, body mass index, and
Buse JB, Bigger JT, Byington RP, depression in adults with type 2 diabetes: the
N01-HC-95183, N01-HC-95184, IAA- Cooper LS, Cushman WC, Friedewald WT, mediational role of diabetes symptoms and
Y1-HC-9035, and IAA-Y1-HC-1010); Genuth S, Gerstein HC, Ginsberg HN, self-efficacy. Health Psychol 26:693–700, 2007
Goff DC Jr, Grimm RH Jr, Margolis KL,
by other components of the National Probstfield JL, Simons-Morton DG, Sullivan
21
Sacco WP, Yanover T: Diabetes and
MD: Action to Control Cardiovascular Risk depression: the role of social support and
Institutes of Health, including the medical symptoms. J Behav Med 29:523–531,
in Diabetes (ACCORD) trial: design and
National Institute of Diabetes and methods. Am J Cardiol 99:21i–33i, 2007 2006
Digestive and Kidney Diseases, 9
Gerstein HC, Riddle MC, Kendall
22
Richardson LP, Lozano P, Russo J,
DM, Cohen RM, Goland R, Feinglos McCauley E, Bush T, Katon W: Asthma
the National Institute on Aging, MN, Kirk JK, Hamilton BP, Ismail-Beigi F, symptom burden: relationship to asthma
and the National Eye Institute; by Feeney P; ACCORD Study Group: Glycemia severity and anxiety and depression
treatment strategies in the Action to Control symptoms. Pediatrics 118:1042–1051, 2006
the Centers for Disease Control Cardiovascular Risk in Diabetes (ACCORD) 23
Weisbord SD, Fried LF, Arnold RM,
and Prevention; and by General trial. Am J Cardiol 99:34i–43i, 2007 Fine MJ, Levenson DJ, Peterson RA, Switzer
Clinical Research Centers. The 10
Sullivan MD, Anderson RT, Aron D, GE: Prevalence, severity, and importance of
Atkinson HH, Bastien A, Chen GJ, Feeney physical and emotional symptoms in chronic
following companies provided study P, Gafni A, Hwang W, Katz LA, Narayan KM, hemodialysis patients. J Am Soc Nephrol
medications, equipment, or sup- Nwachuku C, O’Connor PJ, Zhang P; ACCORD 16:2487–2494, 2005
Study Group: Health-related quality of life
plies: Abbott Laboratories, Amylin and cost-effectiveness components of the
Pharmaceuticals, AstraZeneca, Action to Control Cardiovascular Risk in
Diabetes (ACCORD) trial: rationale and Mark D. Sullivan, MD, PhD, is a
Bayer HealthCare, Closer design. Am J Cardiol 99:90i–102i, 2007 professor in the Department of
Healthcare, GlaxoSmithKline, King 11
Anderson R, Testa M: Symptom distress Psychiatry and Behavioral Sciences
Pharmaceuticals, Merck, Novartis, checklists as a component of quality of life
measurement. Drug Inf J 28:89–114, 1994 at the University of Washington in
Novo Nordisk, Omron Healthcare, 12
Testa MA, Simonson DC: Measuring
Seattle. Gregory Evans, MA, is an
Sanofi-Aventis, and Schering-Plough. quality of life in hypertensive patients with assistant professor in the Departments
Clinical Diabetes • Volume 30, Number 3, 2012 107F e a t u r e A r t i c l e of Biostatistical Sciences and O’Connor, MD, MPH, is assistant Albuquerque. Debra L. Simmons, Neurology at Wake Forest University medical director and a senior clinical MD, MS, is a professor at the School of Medicine in Winston-Salem, research investigator at HealthPartners University of Arkansas for Medical N.C. Roger Anderson, PhD, is a Research Foundation in Minneapolis, Sciences in Little Rock. K.M. Venkat professor in the Department of Health Minn. Dennis W. Raisch, PhD, is a Narayan, MD, MBA, is a professor at Sciences at Penn State College of professor at the College of Pharmacy the Rollins School of Public Health at Medicine in Hershey, Pa. Patrick of the University of New Mexico in Emory University in Atlanta, Ga. 108 Volume 30 Number 3, 2012• Clinical Diabetes
You can also read