Diagnostic Clues to Ectopic Pregnancy1
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Note: This copy is for your personal non-commercial use only. To order presentation-ready
copies for distribution to your colleagues or clients, contact us at www.rsna.org/rsnarights.
ABDOMINAL EMERGENCIES 1661
Diagnostic Clues to
Ectopic Pregnancy1
Edward P. Lin, MD • Shweta Bhatt, MD • Vikram S. Dogra, MD
Ectopic pregnancy accounts for approximately 2% of all pregnancies
TEACHING
POINTS
and is the most common cause of pregnancy-related mortality in the
See last page first trimester. Initial evaluation consists of hormonal assays and pelvic
ultrasonography (US). A history of pelvic pain along with an abnormal
β human chorionic gonadotropin level should trigger an evaluation for
an ectopic pregnancy. The fallopian tube is the most common loca-
tion for an ectopic pregnancy. An adnexal mass that is separate from
the ovary and the tubal ring sign are the most common findings of a
tubal pregnancy. Other types of ectopic pregnancy include interstitial,
cornual, ovarian, cervical, scar, intraabdominal, and heterotopic preg-
nancy. Interstitial pregnancy occurs when the gestational sac implants
in the myometrial segment of the fallopian tube. Cornual pregnancy
refers to the implantation of a blastocyst within the cornua of a bicor-
nuate or septate uterus. An ovarian pregnancy occurs when an ovum is
fertilized and is retained within the ovary. Cervical pregnancy results
from an implantation within the endocervical canal. In a scar pregnan-
cy, implantation takes place within the scar of a prior cesarean section.
In an intraabdominal pregnancy, implantation occurs within the intra-
peritoneal cavity. Heterotopic pregnancy occurs when an intrauterine
and an extrauterine pregnancy occur simultaneously. A spectrum of
intra- and extrauterine findings may be seen on US images. Although
many of the US findings are nonspecific by themselves, when several
of them are seen, the specificity of US in depicting an ectopic preg-
nancy substantially improves.
©
RSNA, 2008 • radiographics.rsnajnls.org
Abbreviation: hCG = human chorionic gonadotropin
RadioGraphics 2008; 28:1661–1671 • Published online 10.1148/rg.286085506 • Content Codes:
1
From the Department of Imaging Sciences, University of Rochester School of Medicine, 601 Elmwood Ave, Box 648, Rochester, NY 14642. Re-
ceived January 30, 2008; revision requested March 14 and received March 31; accepted April 14. All authors have no financial relationships to dis-
close. Address correspondence to V.S.D. (e-mail: Vikram_Dogra@URMC.Rochester.edu).
©
RSNA, 2008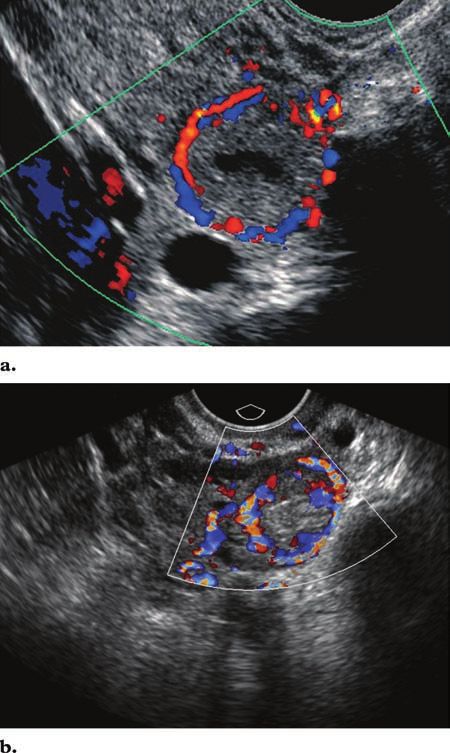
1662 October Special Issue 2008 RG ■ Volume 28 • Number 6
Introduction Table 1
Ectopic pregnancy occurs when a blastocyst ab- Risk Factors of Ectopic Pregnancy
normally implants outside the endometrium of
the uterus. The incidence of ectopic pregnancy Prior ectopic pregnancy
History of pelvic inflammatory disease
has increased from 0.37% of pregnancies in 1948 History of gynecologic surgery
to approximately 2% of pregnancies in 1992 (1). Infertility
Although mortality decreased by nearly 90% Use of intrauterine device
from 1979 to 1992, ectopic pregnancy remains History of placenta previa
Teaching the leading cause of death during the first trimes- Use of in vitro fertilization
Point ter of pregnancy, with a 9%–14% mortality rate Congenital uterine anomalies
(1,2). The main risk factors for ectopic pregnancy History of smoking
include a history of ectopic pregnancy, tubal sur- Endometriosis
Exposure to diethylstilbestrol
gery, and pelvic inflammatory disease. Other risk
factors are summarized in Table 1.
Early diagnosis and treatment of ectopic
pregnancy are essential in reducing maternal vilinear fashion early in pregnancy and continue
mortality and preserving future fertility. Most until they reach a plateau at approximately 9–11
patients who have an ectopic pregnancy present weeks (3). The plateau lasts for only a few days,
with a 5–9-week history of amenorrhea, mild pel- and thereafter β-hCG levels begin to decline at
vic pain, and vaginal spotting. These symptoms 20 weeks. The average doubling time of β-hCG
should trigger an evaluation for an ectopic preg- in a normal, viable intrauterine pregnancy is ap-
nancy (3,4). Up to 50% of patients who have an proximately 48 hours (range, 1.2–2.2 days) (4–7).
ectopic pregnancy are asymptomatic. Therefore, Because of the various impurities and con-
some authors have advocated routine documen- taminants that are found when determining hCG
tation of intrauterine pregnancies for all patients levels, standardized methods for measuring hCG
in their first trimester. Other clinicians limit first levels have been established by the International
trimester ultrasonography (US) to high-risk and Federation of Clinical Chemistry and the World
symptomatic patients. Health Organization (8). The third International
As an ectopic pregnancy enlarges, its risk for Standard (IS), or the first International Refer-
rupture increases. The severity of pelvic pain ence Preparation, is the most widely used stan-
does not necessarily correlate with the size of an dard and is the first IS to account for the alpha
ectopic pregnancy, and pain may even decrease and beta subunits of hCG (8). The hCG level at
or disappear following tubal rupture (4). Hypovo- which US can demonstrate an intrauterine ges-
lemic shock and shoulder pain secondary to dia- tational sac differs from one IS to another; the
phragmatic irritation are indirect signs of a rup- clinician should be aware of the IS used at his or
tured ectopic pregnancy. Any clinical suspicion her institution. Many earlier studies that inves-
for a ruptured ectopic pregnancy in a patient in tigated ectopic pregnancies were based on the
an unstable condition warrants emergent surgical second IS. The second IS can be converted to the
intervention (4). International Reference Preparation by multiply-
The initial evaluation of patients suspected ing by a factor of 1.8. From here on, this article
to have an ectopic pregnancy entails a quantita- will refer to the third IS when discussing β-hCG
tive measurement of serum human chorionic levels.
gonadotropin (hCG), with or without evaluation In ectopic pregnancies, serum hCG levels of-
of progesterone levels, and transvaginal US. The ten rise at a much slower rate. If β-hCG levels in-
hormonal assays, findings seen on US images, crease by less than 50% during a 48-hour period,
and diagnostic criteria that can improve specific- there is almost always a nonviable pregnancy
ity in diagnosing ectopic pregnancies are briefly associated, be it intra- or extrauterine (3). Eighty-
discussed in this article. five percent of viable intrauterine pregnancies
reflect an increase in β-hCG levels of 66% or
Laboratory Evaluation more during a 48-hour period (7). However, up
Human chorionic gonadotropin is a glycoprotein to 21% of ectopic pregnancies demonstrate a
hormone that contains both an alpha and a beta β-hCG doubling time identical to that of intra-
subunit. β-hCG levels begin to ascend in a cur- uterine pregnancies (9). Arriving at a β-hCG pla-
teau early in the pregnancy is highly suggestive of
an ectopic pregnancy.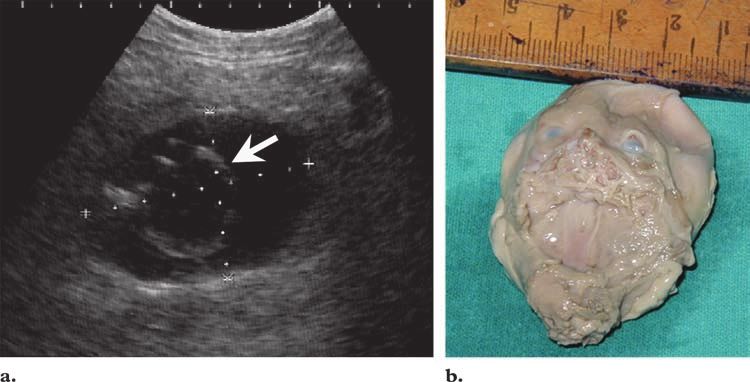
RG ■ Volume 28 • Number 6 Lin et al 1663
Figure 1. Diagram of the various locations of an ectopic pregnancy.
A normal serum progesterone level in viable within the endometrium and is surrounded by
pregnancies is typically more than 25 ng/mL. a hyperechoic ring. At approximately 5 weeks,
Ninety-nine percent of nonviable pregnancies the double decidual sac sign can be visualized.
have a progesterone level of less than 5 ng/mL The double decidual sac sign consists of two
(10,11). The combination of a low serum pro- concentric hyperechoic rings that surround an
gesterone level and an abnormal rise in serum anechoic gestational sac in a normal intrauterine
β-hCG is nearly diagnostic of a nonviable preg- pregnancy (13). The secondary yolk sac may be
nancy. However, progesterone levels often take identified at transvaginal US at approximately 5.5
several days to process. If a laboratory is unable weeks, when the gestational sac reaches 10 mm
to report a value within 24 hours, the test has (14,15). Embryonic cardiac activity should also
limited use. Because of the delay in measuring be visualized at transvaginal US at approximately
progesterone levels, clinical management often 5–6 weeks, when the gestational sac measures
relies on measuring β-hCG levels and on the pa- more than 18 mm or when the embryonic pole
tient’s clinical picture. measures 5 mm or more (16).
When neither an intrauterine pregnancy nor
US Evaluation specific findings of an ectopic pregnancy can be
When a patient presents with symptoms that documented in a patient with a subthreshold
suggest an ectopic pregnancy or when hormonal β-hCG level, the patient should be closely moni-
assays indicate an abnormal pregnancy, pelvic US tored with serial US examinations, and β-hCG
should be performed to determine the location levels should be continually tested until either an
of an intra- or extrauterine pregnancy. Transvagi- ectopic or an intrauterine pregnancy is identified
nal US is the preferred method of evaluation. (17).
Transvaginal US should be able to demonstrate When an abnormal pregnancy is suspected be-
a gestational sac when β-hCG levels are greater cause of hormonal assays, a spectrum of abnor-
than 2000 mIU/mL, which is the discriminatory malities can be detected at pelvic US (16). The Teaching
level of β-hCG (12). However, some institutions absence of an intrauterine gestational sac should Point
may use a higher threshold. Transabdominal US trigger a detailed search for an ectopic pregnancy.
can demonstrate an intrauterine pregnancy when In addition, up to 35% of ectopic pregnan-
β-hCG levels reach 6500 mIU/mL (4). cies may not display any adnexal abnormalities Teaching
The goal of first-trimester screening is to (12,14). Possible locations of ectopic pregnancy Point
document the presence of an intrauterine preg- are illustrated in Figure 1.
nancy, be it normal or abnormal. US is very
sensitive and specific in differentiating between US Findings by Location
normal and abnormal pregnancies in the first
trimester (13). In normal pregnancies, transvagi- Tubal Pregnancy
nal US can demonstrate an intradecidual sign Ninety-five percent of ectopic pregnancies are Teaching
approximately 4.5 weeks after the last menstrual tubal; they occur mostly in the ampulla (70%) Point
period (12). The intradecidual sign is a small
collection of fluid that is eccentrically located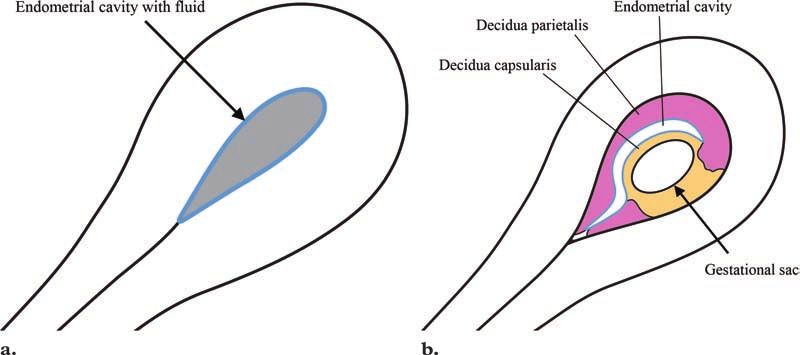
1664 October Special Issue 2008 RG ■ Volume 28 • Number 6
Figure 2. Transvaginal gray-
scale US image obtained with
M-mode scanning demon-
strates a left tubal ring with a
yolk sac and a live embryo (ar-
rowhead), which is suggested
by the presence of cardiac
activity. A live tubal pregnancy
was confirmed at surgery.
Figure 3. Transvaginal gray-scale US image of the
right adnexa reveals an extraovarian adnexal mass with
a hyperechoic tubal ring (arrow). A tubal pregnancy
was confirmed at surgery. OV = right ovary.
Figure 4. Tubal ring sign. Transvaginal US image of
the left adnexa reveals an extraovarian gestational sac Figure 5. Ring of fire sign. Transvaginal color Dop-
with a yolk sac (arrow). The yolk sac is surrounded by pler US images of a tubal pregnancy show peripheral
a thick echogenic ring (arrowhead). hypervascularity surrounding the extrauterine gesta-
tional sac (a) and a hemorrhagic ovarian cyst (b), a
finding that is a mimic of the ring of fire sign.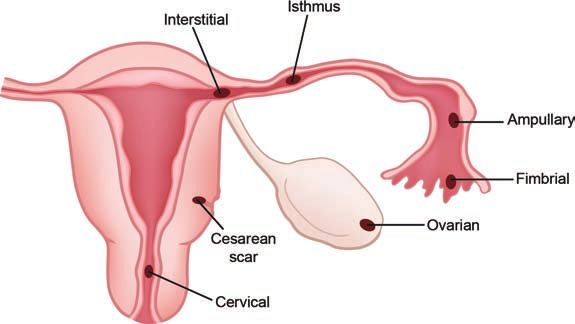
RG ■ Volume 28 • Number 6 Lin et al 1665
Figure 6. Pseudo–gestational sac.
Transvaginal gray-scale US image ob-
tained along the longitudinal axis shows
an intrauterine pseudo–gestational sac
(arrow); there is no yolk sac or fetal
pole. Free fluid is seen in the cul-de-sac
(*). The patient also had a tubal ectopic
pregnancy, which is shown in Figure 4.
Figure 7. Diagrams show a pseudo–gestational sac in an ectopic pregnancy (a) and a double
decidual sac sign in a normal intrauterine pregnancy (b).
or isthmus (12%) and are less common in the to describe the corpus luteum. Determining the
fimbria (11.1%) (18,19). An adnexal mass that location of this type of flow, whether it is within
is separate from the ovary is the most common the ovary or outside the ovary, is most important
finding of a tubal pregnancy and is seen on US to distinguish between an ectopic pregnancy and
images in up to 89%–100% of patients (20,21). a corpus luteum. However, the ring of fire sign is
An adnexal mass is more specific for an ectopic most helpful when no definite ectopic pregnancy
pregnancy when it contains a yolk sac or a living is seen on gray-scale images. Color Doppler im-
embryo (Fig 2) or when it moves independently ages of the adnexa may demonstrate the ring-
from the ovary (Fig 3) (22). However, an extra- of-fire flow in an otherwise nondescript adnexal
uterine mass may not be detected at transvaginal lesion and thereby may improve confidence in the
US in 15%–35% of patients with an ectopic preg- diagnosis of ectopic pregnancy.
nancy (12). Intrauterine findings of an ectopic pregnancy
The tubal ring sign is the second most com- include a “normal endometrium,” a pseudo–
mon sign of a tubal pregnancy. The tubal ring gestational sac, a trilaminar endometrium, and a
sign describes a hyperechoic ring surrounding thin-walled decidual cyst. A pseudo–gestational
an extrauterine gestational sac (Fig 4). A related sac represents a thick decidual reaction surround-
finding is the “ring of fire” sign, which is recog- ing intrauterine fluid (Fig 6). Ten percent of
nized by peripheral hypervascularity of the hy- patients with an ectopic pregnancy demonstrate
perechoic ring. The term ring of fire was used by a pseudo–gestational sac (25). The absence of
Pellerito et al (23) to describe the high-velocity, the double decidual sac sign helps distinguish a
low-impedance flow surrounding an ectopic ad- pseudo–gestational sac from a true viable ges-
nexal pregnancy. Peripheral hypervascularity is tational sac (Fig 7) (26). In addition, a pseudo–
a nonspecific finding of the ring of fire sign and gestational sac is located centrally within the en-
may also be seen surrounding a normal matur- dometrial canal, whereas a normal gestational sac
ing follicle or a corpus luteal cyst (Fig 5) (24).
Therefore, the ring of fire sign should not be used1666 October Special Issue 2008 RG ■ Volume 28 • Number 6
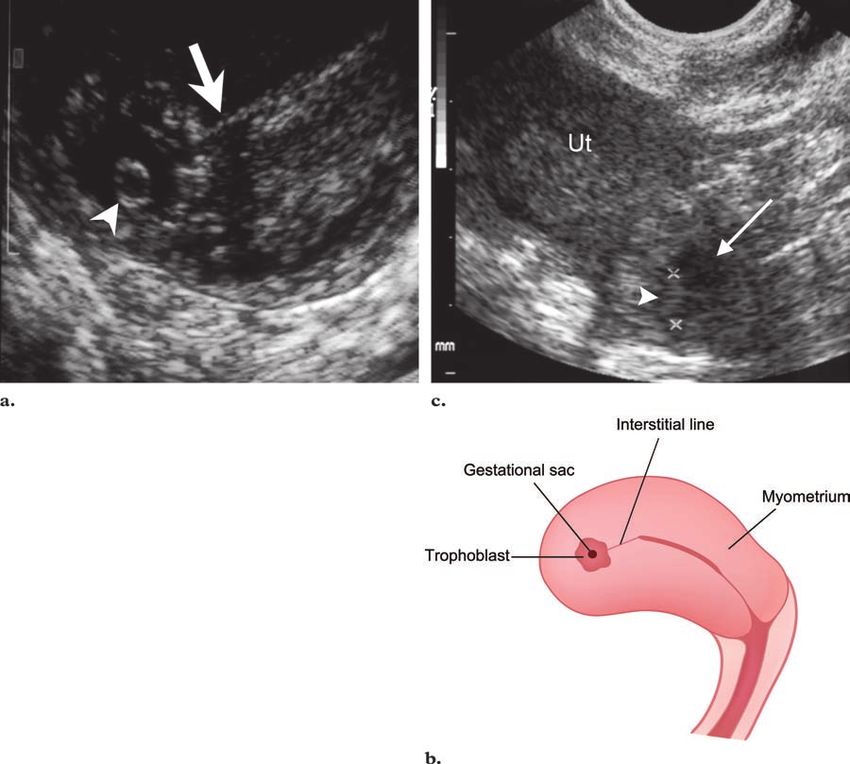
Figure 8. Interstitial pregnancy. (a) Transvaginal
US image obtained along an oblique axis shows
the yolk sac (arrowhead) within a gestational sac,
which is located in the interstitial portion of the fal-
lopian tube. The interstitial line sign (arrow) is also
seen. (b) Diagram of the interstitial pregnancy and
the interstitial line sign. (c) Transverse gray-scale
US image of the uterus in another patient shows a
gestational sac (arrow), which contains an embryo
(arrowhead), in the cornua/interstitial portion of the
fallopian tube. (Fig 8a reprinted, with permission,
from reference 25.)
is located eccentrically within the canal. A viable
gestational sac also exhibits low-resistance arte-
rial flow on color Doppler flow images.
A trilaminar endometrium is formed during
the late proliferative phase of the normal men- hemorrhage is a more specific finding, with an
strual cycle. It consists of an echogenic basal 86%–93% positive predictive value when β-hCG
layer and a hypoechoic inner functional layer fol- levels are abnormal (14,28). The presence of
lowed by a thin echogenic layer that represents echogenic fluid within the right posterior sub-
the interface with the endometrial lumen. When hepatic space (Morrison pouch) and within the
an abnormal pregnancy is suspected based on cul-de-sac should raise concern for a ruptured
laboratory results, the absence of a true gesta- ectopic pregnancy.
tional sac in the presence of a trilaminar endo-
metrium on US images is highly suggestive of an Interstitial Pregnancy
ectopic pregnancy (27). Interstitial pregnancies are uncommon, account-
Thin-walled decidual cysts are found at the ing for 2%–4% of all ectopic pregnancies (19).
junction of the endometrium and the myome- Risk factors for interstitial pregnancy include
trium and may be seen in both normal and ab- prior salpingectomy and in vitro fertilization. In-
normal pregnancies. The thin wall of the decidual terstitial pregnancies occur when the gestational
cyst differentiates it from a true gestational sac. sac implants in the intramyometrial segment of
Extrauterine findings of ectopic pregnancy in- the fallopian tube (29). Because of the increased
clude pelvic free fluid, hematosalpinx, and hemo- distensibility of this segment of the fallopian
peritoneum. Although the presence of pelvic free tube, interstitial pregnancies may be seen as late
fluid within the rectouterine space is nonspecific, as the 16th week of gestation (30). Rupture of an
it is a finding that may help confirm a suspected interstitial pregnancy can lead to life-threatening
ectopic pregnancy in lieu of other findings. Pelvic hemorrhage because of the proximity of the uter-
ine artery to the fallopian tube (30).RG ■ Volume 28 • Number 6 Lin et al 1667
of the intramural gestational sac” (Fig 8) (31).
This echogenic line most likely represents the in-
terstitial portion of the fallopian tube (31). In the
study by Ackerman et al (31), the interstitial line
sign was 80% sensitive and 98% specific for an
interstitial pregnancy.
Cornual Pregnancy
Although it is often used interchangeably with in-
terstitial pregnancy, cornual pregnancy specifically
refers to the implantation of a blastocyst within
the cornua of a bicornuate or septate uterus
(20,32). Cornual pregnancies are rare and ac-
count for less than 1% of all ectopic pregnancies
(33). Rupture of a cornual pregnancy also results
in catastrophic hemorrhage.
In a cornual pregnancy, the gestational sac is
Figure 9. Cervical pregnancy. Transvaginal US im- surrounded by a thin rim (1668 October Special Issue 2008 RG ■ Volume 28 • Number 6
Figure 11. Scar pregnancy in a
patient with a history of cesarean
section. Transvaginal gray-scale
US image of the uterus, obtained
with M-mode scanning along
the longitudinal axis, reveals a
gestational sac with a fetal pole
(arrowhead) in the anterior wall
of the uterus. There was no fetal
cardiac activity, a finding sugges-
tive of fetal demise.
Figure 12. Intraabdominal pregnancy in a patient who went to the hospital for an abor-
tion. The intraabdominal pregnancy was missed because US was not performed before
dilation and curettage. She presented with pain and fever secondary to pyometra 1 week
later. (a) Transabdominal US image reveals an extrauterine gestational sac with a fetal head
(arrow). Laparotomy was performed, and only the fetal head was found in a pocket of pus
in a retrocecal location. No other fetal parts were identified. (b) Photograph shows the sur-
gically removed extrauterine gestational sac with the fetal head. (Scale is in centimeters.)
(Reprinted, with permission, from reference 47.)
sac), this confirms that the gestational sac is not pregnancies may also rupture, which can result in
adherent to the cervix (excluding cervical preg- severe hemorrhage and hemodynamic collapse.
nancy), which indicates that an abortion is in In a scar pregnancy, a gestational sac may be
progress (43). visualized within the anterior wall of the inferior
aspect of the uterus (Fig 11) (46). Secondary to
Scar Pregnancy compression by the gestational sac, the myome-
Caesarean scar pregnancies are also rare and are trium may also be thinned anteriorly (46). Thin-
estimated to occur in less than 1% of all pregnan- ning of the myometrium may predispose a patient
cies (44). Implantation takes place within the to uterine rupture (21).
scar of a prior cesarean section, separate from the
endometrial cavity (44). Within the scar, the blas- Intraabdominal Pregnancy
tocyst is surrounded by myometrium and fibrous In an intraabdominal pregnancy, implantation
tissue (45). A suggested mechanism is that a tract occurs within the intraperitoneal cavity (Fig 12),
connects the endometrial canal and the uterine excluding tubal, ovarian, and intraligamentous lo-
myometrium; this tract facilitates implantation cations. This is a rare cause of ectopic pregnancy,
within the scar (45). Patients who have a scar but it is more common in patients who undergo
pregnancy may present with vaginal bleeding as assisted reproduction (48), and it may represent
early as 5–6 weeks and as late as 16 weeks. Scar 1.4% of ectopic pregnancies. Because of signifi-
cant hemorrhage, maternal mortality associated
with intraabdominal pregnancy is 7.7 times that
of other locations of ectopic pregnancy (49).RG ■ Volume 28 • Number 6 Lin et al 1669
Figure 13. Heterotopic pregnancy. Trans-
vaginal gray-scale US image demonstrates a
gestational sac within the uterus (arrow) and
an extrauterine gestational sac (arrowhead).
Table 2
US Findings of Ectopic Pregnancy by Location
Type of Pregnancy Findings on US Images
Tubal pregnancy Living extrauterine gestation, adnexal mass, tubal ring sign, ring of
fire sign, pelvic hemorrhage
Interstitial pregnancy* Eccentrically located gestational sac, gestational sac surrounded by a
thin myometrium (1000 mIU/mL; normal fallopian tubes; gesta-
tional sac, chorionic villi, or atypical cyst within the ovary; normal
β-hCG level after therapy
Cervical pregnancy‡ Trophoblastic flow surrounding the gestational sac within the cer-
vix, normal endometrial stripe, gestational sac within the cervix
with cardiac activity, hourglass-shaped uterus, cardiac activity
below the internal os
Cesarean scar pregnancy Gestational sac located within the lower anterior segment of the
uterus at the site of a prior cesarean section, thinning of myome-
trium anterior to the gestational sac
Abdominal pregnancy Absence of a normal intrauterine gestational sac, gestational sac locat-
ed within the intraperitoneal cavity, abdominal or pelvic hemorrhage
* Reference 37.
† References 48 and 49.
‡ Reference 40.
Heterotopic Pregnancy a known heterotopic pregnancy can potentially
Heterotopic pregnancy occurs when an intra- undergo US-guided ablation or laparoscopic
uterine and an extrauterine pregnancy occur si- removal of the extrauterine fetus to permit the
multaneously (Fig 13). Knowledge of heterotopic intrauterine pregnancy to continue normally. If a
pregnancy is becoming increasingly important patient undergoes an abortion of an intrauterine
as more women undergo assisted reproduction, pregnancy and continues to experience persistent
particularly ovulation induction. The prevalence adnexal pain with abnormal β-hCG levels, het-
of heterotopic pregnancy in women who undergo erotopic pregnancy should be suspected.
assisted reproduction has been reported to be Although many of the intra- and extrauterine
Teaching
1%–3% (50). Heterotopic pregnancy remains a findings are nonspecific when they are seen in
Point
diagnostic challenge and should be kept in mind isolation, the use of diagnostic criteria may im-
when a patient who has undergone assisted re- prove specificity when several findings are identi-
production presents with pelvic pain. US images fied in a patient suspected of having an ectopic
can demonstrate the presence of an intrauterine pregnancy (Table 2).
and an extrauterine pregnancy. Patients who have1670 October Special Issue 2008 RG ■ Volume 28 • Number 6
Conclusions 7. Eyvazzadeh AD, Levine D. Imaging of pelvic pain in
Although mortality has significantly decreased the first trimester of pregnancy. Radiol Clin North
Am 2006;44:863–877.
over the past two decades because of earlier 8. Birken S, Berger P, Bidart JM, et al. Preparation
detection and intervention, ectopic pregnancy and characterization of new WHO reference agents
remains the leading cause of death of women in for human chorionic gonadotropin and metabolites.
the first trimester of pregnancy. Work-up of a pa- Clin Chem 2003;49:144–154.
tient who presents with pelvic pain, amenorrhea, 9. Seeber BE, Barnhart KT. Suspected ectopic preg-
nancy. Obstet Gynecol 2006;107:399–413.
and vaginal spotting entails hormonal assays and 10. McCord ML, Muram D, Buster JE, Arheart KL,
pelvic US. When results of laboratory evaluation Stovall TG, Carson SA. Single serum progesterone
suggest an abnormal pregnancy, a detailed search as a screen for ectopic pregnancy: exchanging speci-
for an intra- or extrauterine pregnancy should be ficity and sensitivity to obtain optimal test perfor-
performed. mance. Fertil Steril 1996;66:513–532.
11. Dart R, Ramanujam P, Dart L. Progesterone as a
The most common location of an ectopic predictor of ectopic pregnancy when the ultrasound
pregnancy is the fallopian tube. US findings of is indeterminate. Am J Emerg Med 2002;20:575– 579.
ectopic pregnancy can be categorized by location 12. Levine D. Ectopic pregnancy. Radiology 2007;245:
(intra- or extrauterine). Although many of these 385–397.
findings are nonspecific when they are seen sin- 13. Morin L, Van den Hof MC. SOGC clinical prac-
tice guidelines: ultrasound evaluation of first tri-
gly, when several of them are seen, the specificity mester pregnancy complications. Int J Gynaecol
of US in depicting an ectopic pregnancy substan- Obstet 2006;93:77–81.
tially improves. Use of these diagnostic criteria, 14. Russell SA, Filly RA, Damato N. Sonographic
as was outlined previously, may therefore improve diagnosis of ectopic pregnancy with endovaginal
diagnostic accuracy when abnormal β-hCG or probes: what really has changed? J Ultrasound Med
1993;12:145–151.
progesterone levels suggest an ectopic pregnancy. 15. Nyberg DA, Hill LM. Normal early intrauterine
pregnancy: sonographic development and HCG
References correlation. In: Patterson AS, ed. Transvaginal ul-
1. Centers for Disease Control and Prevention (CDC). trasound. St Louis, Mo: Mosby, 1992; 64–85.
Ectopic pregnancy: United States, 1990–1992. 16. Paspulati RM, Bhatt S, Nour S. Sonographic evalu-
MMWR Morb Mortal Wkly Rep 1995;44:46–48. ation of first-trimester bleeding. Radiol Clin North
2. Lozeau AM, Potter B. Diagnosis and management Am 2004;42:297–314.
of ectopic pregnancy. Am Fam Physician 2005;72: 17. Banerjee S, Aslam N, Zosmer N, Woelfer B,
1707–1714. Jurkovic D. The expectant management of women
3. Lipscomb GH, Stovall TG, Ling FW. Nonsurgi- with early pregnancy of unknown location. Ultra-
cal treatment of ectopic pregnancy. N Engl J Med sound Obstet Gynecol 1999;14:231–236.
2000;343:1325–1329. 18. Bouyer J, Coste J, Fernandez H, Pouly JL, Job-Spira
4. Attar E. Endocrinology of ectopic pregnancy. Ob- N. Sites of ectopic pregnancy: a 10 year population-
stet Gynecol Clin North Am 2004;31:779–794. based study of 1800 cases. Hum Reprod 2002;17:
5. Daya S. Human chorionic gonadotropin increase 3224–3230.
in normal early pregnancy. Am J Obstet Gynecol 19. Webb EM, Green GE, Scoutt LM. Adnexal mass
1987;156:286–290. with pelvic pain. Radiol Clin North Am 2004;42:
6. Pittaway DE, Reish RL, Wentz AC. Doubling times 329–348.
of human chorionic gonadotropin increase in early 20. Dialani V, Levine D. Ectopic pregnancy: a review.
viable intrauterine pregnancies. Am J Obstet Gyne- Ultrasound Q 2004;20:105–117.
col 1985;152:299–302. 21. Atri M, Leduc C, Gillett P, et al. Role of endovagi-
nal sonography in the diagnosis and management
of ectopic pregnancy. RadioGraphics 1996;16:755–
774.RG ■ Volume 28 • Number 6 Lin et al 1671
22. Blaivas M, Lyon M. Reliability of adnexal mass transfer: a case report. Clin Exp Obstet Gynecol
mobility in distinguishing possible ectopic preg- 2001;28:100–101.
nancy from corpus luteum cysts. J Ultrasound Med 37. Herbertsson G, Magnusson SS, Benediktsdottir
2005;24:599–603. K. Ovarian pregnancy and IUCD use in a defined
23. Pellerito JS, Taylor KJ, Quedens-Case C, et al. Ec- complete population. Acta Obstet Gynecol Scand
topic pregnancy: evaluation with endovaginal color 1987;66:607–610.
flow imaging. Radiology 1992;183:407–411. 38. Spiegelberg O. Zur casuistic der ovarialschwanger-
24. Durfee SM, Frates MC. Sonographic spectrum of schaft. Arch Gynaekol 1878;13:73.
the corpus luteum in early pregnancy: gray-scale, 39. Sergent F, Mauger-Tinlot F, Gravier A, Verspyck
color, and pulsed Doppler appearance. J Clin Ul- E, Marpeau L. Ovarian pregnancies: reevaluation
trasound 1999;27:55–59. of diagnostic criteria [in French]. J Gynecol Obstet
25. Bhatt S, Ghazale H, Dogra VS. Sonographic evalu- Biol Reprod (Paris) 2002;31:741–746.
ation of ectopic pregnancy. Radiol Clin North Am 40. Vela G, Tulandi T. Cervical pregnancy: the impor-
2007;45:549–560. tance of early diagnosis and treatment. J Minim
26. Yeh HC, Rabinowitz JG. Amniotic sac development: Invasive Gynecol 2007;14:481–484.
ultrasound features of early pregnancy—the double 41. Hofmann HM, Urdl W, Höfler H, Hönigl W,
bleb sign. Radiology 1988;166:97–103. Tamussino K. Cervical pregnancy: case reports
27. Hammoud AO, Hammoud I, Bujold E, Gonik B, and current concepts in diagnosis and treatment.
Diamond MP, Johnson SC. The role of sonographic Arch Gynecol Obstet 1987;241:63–69.
endometrial patterns and endometrial thickness in 42. Kung FT, Lin H, Hsu TY, et al. Differential
the differential diagnosis of ectopic pregnancy. Am J diagnosis of suspected cervical pregnancy and
Obstet Gynecol 2005;192:1370–1375. conservative treatment with the combination of
28. Dogra V, Paspulati RM, Bhatt S. First trimester laparoscopy-assisted uterine artery ligation and
bleeding evaluation. Ultrasound Q 2005;21:69–85. hysteroscopic endocervical resection. Fertil Steril
29. de Boer CN, van Dongen PW, Willemsen WN, 2004;81:1642–1649.
Klapwijk CW. Ultrasound diagnosis of interstitial 43. Jurkovic D, Hacket E, Campbell S. Diagnosis and
pregnancy. Eur J Obstet Gynecol Reprod Biol treatment of early cervical pregnancy: a review and
1992;47:164–166. a report of two cases treated conservatively. Ultra-
30. Malinowski A, Bates SK. Semantics and pitfalls in sound Obstet Gynecol 1996;8:373–380.
the diagnosis of cornual/interstitial pregnancy. Fer- 44. Ash A, Smith A, Maxwell D. Caesarean scar preg-
til Steril 2006;86:1764.e11–e14. nancy. BJOG 2007;114:253–263.
31. Ackerman TE, Levi CS, Dashefsky SM, Holt SC, 45. Godin PA, Bassil S, Donnez J. An ectopic pregnancy
Lindsay DJ. Interstitial line: sonographic finding in developing in a previous caesarean section scar. Fer-
interstitial (cornual) ectopic pregnancy. Radiology til Steril 1997;67:398–400.
1993;189:83–87. 46. Li SP, Wang W, Tang XL, Wang Y. Cesarean scar
32. Lau S, Tulandi T. Conservative medical and surgi- pregnancy: a case report. Chin Med J (Engl) 2004;
cal management of interstitial ectopic pregnancy. 117:316–317.
Fertil Steril 1999;72:207–215. 47. Parekh VK, Bhatt S, Dogra VS. Abdominal preg-
33. Tulandi T, Saleh A. Surgical management of ectopic nancy: an unusual presentation. J Ultrasound Med
pregnancy. Clin Obstet Gynecol 1999;42:31–38. 2008;27:679–681.
34. Timor-Tritsch IE, Monteagudo A, Matera C, 48. Rojansky N, Schenker JG. Heterotopic pregnancy
Veit CR. Sonographic evolution of cornual preg- and assisted reproduction: an update. J Assist Re-
nancies treated without surgery. Obstet Gynecol prod Genet 1996;13:594–601.
1992;79:1044–1049. 49. Atrash HK, Friede A, Hogue CJ. Abdominal preg-
35. Hirose M, Nomura T, Wakuda K, Ishiguro T, nancy in the United States: frequency and mater-
Yoshida Y. Combined intrauterine and ovarian nal mortality. Obstet Gynecol 1987;69:333–337.
pregnancy: a case report. Asia Oceania J Obstet 50. Fernandez H, Gervaise A. Ectopic pregnancy after
Gynaecol 1994;20:25–29. infertility treatment: modern diagnosis and thera-
36. Melilli GA, Avantario C, Farnelli C, Papeo R, peutic strategy. Hum Reprod Update 2004;10:
Savona A. Combined intrauterine and ovarian 503–513.
pregnancy after in vitro fertilization and embryoRG Volume 28 • Volume 6 • October 2008 Lin et al Diagnostic Clues to Ectopic Pregnancy Edward P. Lin, MD, Shweta Bhatt, MD, and Vikram S. Dogra, MD RadioGraphics 2008; 28:1661–1671 • Published online 10.1148/rg.286085506 • Content Codes: Page 1662 Ectopic pregnancy remains the leading cause of death during the first trimester of pregnancy, with a 9%–14% mortality rate. Page 1663 The absence of an intrauterine gestational sac should trigger a detailed search for an ectopic pregnancy. Page 1663 In addition, up to 35% of ectopic pregnancies may not display any adnexal abnormalities. Page 1663 Ninety-five percent of ectopic pregnancies are tubal. Page 1669 Although many of the intra- and extrauterine findings are nonspecific when they are seen in isolation, the use of diagnostic criteria may improve specificity when several findings are identified in a patient suspected of having an ectopic pregnancy.
You can also read

















































