Edmonton Symptom Assessment System (ESAS-r) - Stratis ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
4/2/2021
Edmonton Symptom Assessment
System (ESAS-r)
Lyn Ceronsky DNP, GNP, FPCN
lceronsky@gmail.com
December 11, 2018
1
Objectives
• Explore the use of Edmonton Symptom
Assessment System (ESAS-r) tool in clinical
practice.
• Discuss strategies to assess patients'
symptoms to guide interventions.
2
2
14/2/2021
Thank you to our colleagues for permission to use
some of their slides
Dr. Cheryl Nekolaichuk1,2 and Dr. Sharon Watanabe1,3
1Divisionof Palliative Care Medicine, University of Alberta
2Palliative
Institute, Covenant Health
3Cross Cancer Institute, Edmonton, AB, Canada
Cheryl.Nekolaichuk@covenanthealth.ca
Sharon.Watanabe2@albertahealthservices.ca
3
3
Patient Story
• Esophageal cancer, 71 years, lives with spouse
• ESAS completed by patient at your visit,
screening shows 6 symptoms (pain, anxiety,
fatigue, anorexia, depression, and dyspnea)
• Caregiver feels overwhelmed and asks if more
can be done to improve symptoms
4
4
24/2/2021
Audience Discussion
• Are you using the ESAS now?
• What is working well?
• What are the challenges?
5
5
What Is ESAS?
• Self reporting tool of symptom intensity,
initially developed for advanced cancer
patients
• Symptoms were chosen based on experiences
of patients with advanced cancer
• Most patients (85%) agreed ESAS was easy to
do
Watanabe,S 2008
6
6
34/2/2021
Patient Reported Outcomes (PROs)
• ESAS is an example, gold standard, meets
quality standards for palliative care
• Pair with a comprehensive clinical assessment
that consider changes over time and impact
on function, mood
7
7
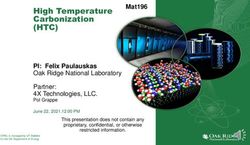
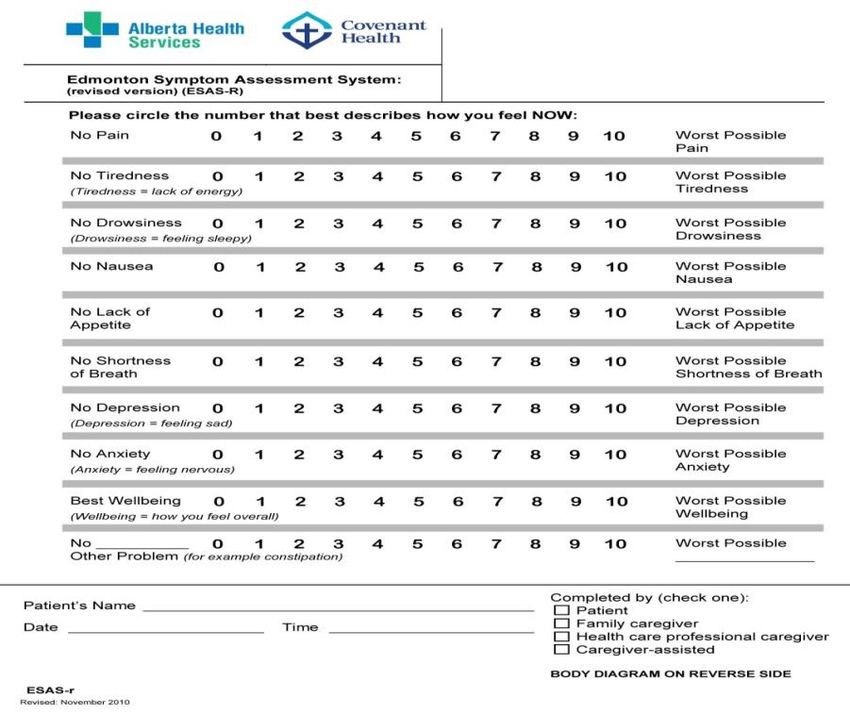
What is the Edmonton Symptom Assessment
System Revised (ESAS-r)?
• ESAS revised to improve ease of
understanding and completion
• Key changes
– Specifying “Now”
– Brief definitions
– Item order
– Example for “other
symptom”
– Improved readability
Watanabe SM et al. J Pain Symptom Manage 2011; 41:456-468.
8
8
44/2/2021
9
9
General Points About the ESAS-r
• Intended to capture patient’s perspective, but
sometimes necessary to capture caregiver’s
perspective
• Provides profile of symptom severity at a point
in time – repeated assessments help track
changes over time
• Only one part of a holistic clinical assessment
10
10
54/2/2021
Strengths of ESAS
• Strengths
– Pragmatic patient-centered symptom assessment
tool that is easy to administer, interpret, and
report
– The assessment of 10 symptoms at the same time
allows for symptom clusters to be identified
– Can be completed rapidly
– The responsiveness and minimal clinically
important differences have been identified
– Free of charge, multiple languages available
11
11
Limitations of ESAS
• One-dimensional scales that assess only
symptom intensity
• Different versions of ESAS are currently
used with different time anchors and
number of items,
• Few validation studies in non-cancer
populations
• Some items (e.g., well-being) are not well
defined
12
12
64/2/2021
How To Do the ESAS-r
• Patient to complete with guidance from health
care provider (HCP)
• Instruct patient to rate severity of each
symptom on 0-10 scale
– 0 = symptom not present
– 10 = worst possible severity
• Number should be circled on scale
• Instruct patient to rate severity “Now”
– Clinician may ask about other time points
13
13
Pain Assessment
• Remember needs of special populations
– Culture
– Age
– Mental status
– History of substance abuse
• Ask about multiple sites of pain
• Concept of total pain
• Hx and description (pqrst or OLDCART)
• Non verbal indicators
14
14
74/2/2021
Pain Anchors
• Worst pain you can imagine
• Not able to concentrate because of pain
• Horrible
• Brings you to tears
• Excruciating amount of pain, affects whole self
15
15
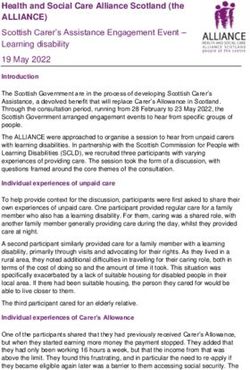
How to Do the ESAS-r
Please mark on these pictures where it is that you hurt:
• Use body diagram to mark
sites of pain
• Transfer numbers onto
ESAS-r graph
– Gives record of
symptom severity over
time
16
16
84/2/2021
Nausea Anchors
• Worst nausea you can imagine
• Even the thought of food…
• Can’t keep any food down
17
17
How to Do the ESAS-r
• Review definitions
– Tiredness: lack of energy
– Drowsiness: feeling sleepy
– Depression: feeling sad
– Anxiety: feeling nervous
– Wellbeing: how you feel overall
18
18
94/2/2021
Misinterpretation In Using the ESAS-r
• Confusion between drowsiness and tiredness
• Difficulty understanding “wellbeing”
• Not rating symptoms in the present moment:
“now”
• Reverse score for appetite and wellbeing
19
19
Addressing Common
Misinterpretations
• Confusion between drowsiness and tiredness
– Drowsiness = feeling sleepy
• Other words to use: “can’t keep eyes open” or “can’t
focus”
– Tiredness = lack of energy
• Other words to use: “fatigue” “low physical energy”
• Difficulty understanding “wellbeing”
– Other words to use: “How you feel overall, when
you think of everything you have told me about,
how do you feel?”
20
20
104/2/2021
Addressing Common
Misinterpretations
• Understanding the scale for appetite
– Zero = good appetite, not a problem
– Ten = really poor appetite, no interest in
eating
• Understanding the scale for wellbeing
– Zero = best wellbeing, feeling great
– Ten = low wellbeing, high distress in how
you feel
21
21
Who Should Do the ESAS-r?
• Patient: Provides ratings independently
• Caregiver Assistance: Patient cannot rate
symptoms independently but can provide
input with help (family, health care
professional)
• Caregiver Alone: Patient cannot or will not
participate; may indicate “unable to assess”
– ESAS-r administration guidelines includes objective
indicators 22
22
114/2/2021
Who Should Do the ESAS-r?
• Indicate method of
completion at bottom
of ESAS-r and graph
– Patient
– Family caregiver alone
– Health care professional
caregiver alone
– Caregiver Assisted
23
23
Patient Instructions
• Patients (and caregivers) appreciate
information on why it’s important to do this
– Reinforces validity of patient’s perspective
– Makes changes over time visible
– Guides further assessment → directs ways to help
• Complete at same time of day
24
24
124/2/2021
Clinical Pearls
• Pain: ask 3 ways: pain, discomfort, achiness
• Symptom intensity equal or > 7 = severe symptom
distress*
• For all symptoms:
– what is the impact on the patient’s quality of life?
– what does the symptom prevent the patient from doing?
• ESAS can be used for cancer distress screening
>7/10 physical and/or emotional→ increase
intensity of home visits
*Hui et al 2017
25
25
Ingredients for Success in Using ESAS
• Interdisciplinary commitment
• Ongoing communication to and education for
staff
• Regular audits to monitor use and action plans
• Excellent communication with patients and
families
26
26
134/2/2021
Clinical Applications
• Allows team members to “speak a common
language”
• Aids in discussions in team meetings & informal
discussions regarding ongoing patient management
• May assist with patient triage and referrals
• Assists with identification of team members to
involve:
– Referrals to other team member
– Distress screening at cancer facilities
27
27
Clinical Aspects
• What amount of change in scores is clinically
significant?
• What action should we take and when?
• How will we know the plan works?
28
28
144/2/2021
Personalized Symptom Goals
• Acknowledges differences in patient
perceptions of scores
– Example : pain score of “6”
• Change in one point may not be meaningful
• Ask: “Using 0-10 scale, what level would you
feel comfortable?”
29
29
Following Symptoms Over Time
• Document at baseline
• Symptoms fluctuate with disease progression
• Scores change as symptom management
becomes effective
30
30
154/2/2021
Clinical Implementation
• Amount and kind of resources available at
your site may determine how you use the
ESAS tool
• May be a way to help patients communicate
with their care providers
• May prompt additional assessment by current
team or referral to others
31
31
Example of Triaging Patient Visits
• ESAS was used to plan intensity of home
based palliative care visits
• Looked at patients with high, moderate, and
low sx burden
• Intensity of sx determined timing of initial visit
– High: seen within 3 days
– Moderate: 7 days
– Low: 10 days
32
32
164/2/2021
Putting It All Together
• Emily, age 84, has heart disease and COPD
• She tells you she has trouble staying awake
during the day and feels nervous
• She asks you how to mark these on the
symptom form
• What symptoms is she describing?
33
33
Putting It All Together
• Paul is a 56 year old with liver and kidney
disease, history of colon cancer
• He tells you that he is feeling “on top of the
world” after hearing good news at his recent
check up
• As you review his ESAS record, you notice that
he has marked “wellbeing” as a zero
• Does “zero” represent his wellbeing?
34
34
174/2/2021
Putting It All Together
• Carlos’s pain scores show a change from last
week.
• Previously he rated his pain as a 3
• This week he rates his pain as 7
• What is your next step?
35
35
Recommendations
From the Literature:
• Partner ESAS with clinical assessment
• Clarify items that are sometimes hard to
interpret: tiredness, drowsiness, depression,
anxiety, appetite, and wellbeing
• Emphasize timeframe of “now” (other
information about timing may be helpful for
your overall assessment)
• Consider presence of a health care
professional for the first patient use(s) of ESAS
36
36
184/2/2021
Role of Health Care Professional
• For patients, help them understand terms and
correct use of rating scale
• Health care professionals also appreciate
guidance in using terms appropriately
– Examples of how to ask questions
• Ongoing training: written materials, refreshers
37
37
Summary
• ESAS is a valid tool for assessing patients’
perceptions of symptoms
• Leads to additional assessment of symptoms
• Helps evaluate effectiveness of interventions
• Aids in communication among health care
team
38
38
194/2/2021
References
•Bruera E, Kuehn N, Miller MJ, Selmser P, Macmillan K. The Edmonton Symptom Assessment System (ESAS): a
simple method for the assessment of palliative care patients. J Palliat Care 1991; 7:6-9.
•Buttenschoen C, Stephan J, Watanabe, S, Nekolaichuk C. Health Care Providers’ Use and Knowledge of the
Edmonton Symptom Assessment System ( ESAS): is there a need to improve information and training? Support
Care Cancer 2014; 22:201-208.
•Hui D and Bruerra E. The Edmonton Symptom Assessment System 25 years Later: Past, Present and Future
Developments. J of Pain and Symptom Management. 2017; 53(3): 630-643.
•Hui D, Titus, A, Ho-Nguyen, V, Frederickson, D, Wray, C, Granville, T, Bruera E et al. Implementation of the
Edmonton Symptom Assessment System for Symptom Distress Screening at a Community Cancer Clinic: A Pilot
Program. The Oncologist 2017; 22:995-1001.
•Nekolaichuk C, Watanabe S, Beaumont C. The Edmonton Symptom Assessment System: a 15-year
retrospective review of validation studies (1991-2006). Palliat Med 2008; 22:111-122.
•Watanabe SM, Nekolaichuk C, Beaumont C, Mawani, A. The Edmonton symptom Assessment System-What do
patients think? Support Care Cancer 2009; 17: 675-683.
•Watanabe SM, Nekolaichuk C, Beaumont C, Johnson L, Myers J, Strasser F. A multi-centre comparison of two
numerical versions of the Edmonton Symptom Assessment System in palliative care patients. J Pain Symptom
Manage 2011; 41:456-468.
39
39
20You can also read