Fibroids and Endometriomas from the Perspective of REI - Paul C. Lin MD Seattle Reproductive Medicine
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Fibroids and Endometriomas
from the Perspective of REI
Paul C. Lin MD
Seattle Reproductive Medicine
DISCLOSURE
• I have nothing to disclose AKA I make no more money on
the side
Endometriosis and Fertility
Types of
patients with
endometriosis PAIN
WANT TO
CONCEIVE
DOES NOT DOES NOT
WANT WANT TO
CONCEIVE CONCEIVE
CURRENTLY EVER
Do I operate on infertility patients?
• NO
• Canadian 1997 RCT study
says maybe but not
practical, lot of unnecessary
surgeries (NNT 1:7)
• Italian study 1999 RCT
showed no difference
• Unless…..
When do I operate on pts trying to conceive?
• Symptoms
• have symptoms that affect QUALITY
OF LIFE (patient judgement)
• Endometrioma expected to or has
precluded adequate access to
maturing follicles during IVF
stimulation
• SOFT criteria: Ovarian reserve testing
i.e. AMH and AFC is assuring, Age < 40
Preop counseling key principles and expectations
• “I can not get it all”
• Approach it robotically (Why? better visualization with high def and
3D, wristing allows proper angles, “Firefly” technology MAY assist in
visualization when minimal amounts seen)
• Combination of resection/ablation/adhesiolysis (especially when the
tubes are involved)
Preop counseling key principles and expectations
• If pain is major goal and hysterectomy
with and without oophorectomy wants
to be done, refer back to general gyn
• Chromotubation always done
• Unless tubal status is known, i.e. hydro,
counsel about possible removal or
ligation of tubes (avoid a second surgery
to remove tubes)
• If endometrioma present, counsel about
potential decline in ovarian reserve
• Generate a postop plan for management
preoperatively, i.e. try to conceive with
a timeline or hormonal suppression if no
immediate plans to conceive
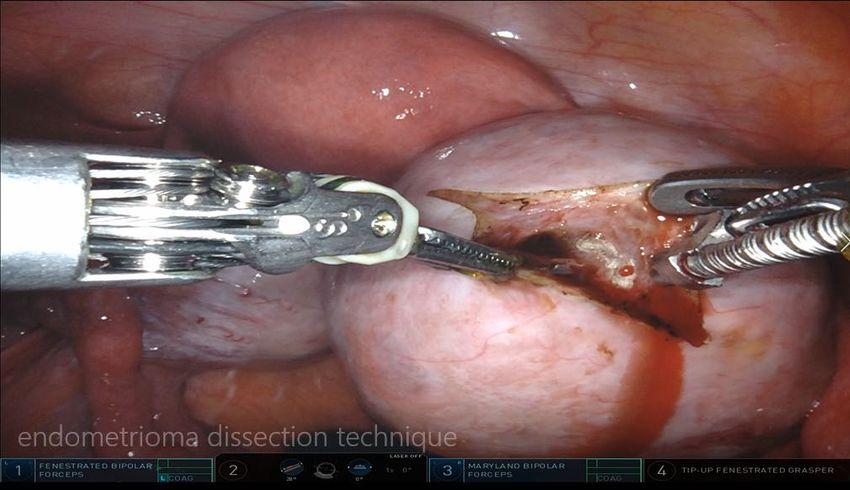
How do I operate?
• With the intention that this is the only surgery to be done
• Robot
• CO2 laser (minimal trauma) resection mostly but ablation also excellent
(better than coagulation with less defined borders)
• Unless having bowel symptoms, I do not do aggressive surgery on the
rectum
• Control bleeding with suture or anticoagulant therapy (no unipolar and
absolutely no bipolar energy on the ovary)
• Preoperatively counsel that tubes may need to be removed if significant(>10
mm in diameter) hydrosalpinges are present regardless of whether a HSG is
done or not.
Video
Adenomyosis
• Probably in ALL pts with endometriosis
• Diffuse or focal involvement
• When Focal, can be confused with a leiomyoma “Adenomyoma”
• Imaging (US: asymmetry, heterogeneity, cystic lesions, striations,
streaking, irregular junctional zone)
• Diagnosis: pathologic confirmation usually during a planned
“myomectomy”Adenomyosis treatment for fertility (in order of preference)
• Do nothing and proceed with getting pregnant in typical plan similar
to patient with endometriosis
• Pretreat with 3 months of GnRH agonist if failed ET or FET
• Surgery resection if above has not worked (rare)
• SurrogacyVideo of adenomyosis
Fibroids and Fertility
Types of patients with fibroids
• Trying to conceive
• Not trying to conceive
• location, location and locationSize does not matter…..if the location is not significant If no symptoms, no size criteria if endometrial cavity unaffected Very rare that a large fibroid will have no symptoms
When do I operate on fibroids when a patient is NOT trying to get
pregnant?
• Symptomatic
• Detailed history: menorrhagia, metrorrhagia, pressure symptoms,
how many times urination during the day?, urgency, nocturia,
constipation/obstipation, hemorrhoids
• Do they affect QOL?
• History taking often educational for patients: Patients don’t know
what they don’t know, need perspectiveWhen do I operate on fibroids when a patient is trying to get
pregnant?
• Symptomatic
• AGE is a factor
- 44 yo, open to third party egg donor
-43-44, most difficult to counsel (benefit of
surgery limited because prognosis of getting
pregnant is so low)
• Submucosal fibroids or fibroids with a submucosal component
• Multiple miscarriages documented (2 or more)When do I operate on fibroids when a patient is trying to get
pregnant with IVF?
• If intramural, Deviation of the endometrial cavity
• If two or more euploid embryos without
implantation and >3-4 cm
• If greater than 3-4 untested embryos without
implantation and >3-4 cmHow do I operate?
• Robot or conventional (prefer latter because of tactile feel)
• Conventional – absolutely necessary for intracorporeal tying
• Deep sutures with braided suture
• Intracorporeal interrupted for mid level closure
• Baseball stitch or running monofilament stitch
• Little to no electrical energy for coagulation (suturing, clipping or
vasopressin readministration)
• Harmonic (cut, coagulation) with limited “smoke”Preop counseling
• Risk of open overall < 1% up to 10 cm fibroid, increase to 10% if >10
cm
• MRI really helps in preop planning
• Won’t get them all, especially if 1 cm or less
• In bag morcellation v. open morcellationTo open or not?
• Ego should not be involved
• Decision is based on your own patient criteria (each of you will have
different criteria)
• Preop counsel everybody risk of open, never guarantee to patients
• Preop MRI very helpful in determining surgical approach (especially
very large and/or multiple fibroidsSubmucosal fibroid
• For fertility, always remove
• If > 3 cm, approach laparoscopic or counsel about two stage HSC
approach
• If > 50% involvement in myometrium, approach LSC
• IfJust because Mount Everest is there, doesn’t mean you have to
climb it……
• You don’t have to operate on everybody who
has a fibroid!
• Factors to consider:
Asymptomatic
Preop imaging suggests adenomyosis
Not TTC for a very long time
Age >42, unless their fertility plan includes third
party
Diminished ovarian reserve
SIV EMSCASE VIGNETTES
CASE #1 38 yo G1P0010 TTC 3 cm fibroid Hx of septum, attempted to resect cxed by uterine perforation
Video of LSC resection of a SM fibroid
Postoperative Management -Fibroids can distort the anatomy and make it difficult to deal with any intrauterine pathyology RECOMMEND: -post op uterine evaluation i.e. OH, SIS 3 months after -any type of intrauterine anatomy needs to be addressed postop after 3 months to allow the uterus to heal, whether it is a septum or other fibroids -need to do preop counseling that uterus needs to involute before endo cavity can be fully evaluated to be normal
Case #2 : Management of endometrioma For an infertility patient, should a large > 4 cm asymptomatic endometrioma be removed to improve chances for pregnancy ?
Usually not….but there are factors to consider
• HSG: I am assuming normal tubes, then no. If tubes dilated, will operate with goal to remove
one or both tubes for IVF (and resect any and all EMS).
• Ovarian reserve testing: AMH low, AFC low: proceed with IVF
• Size may matter: If during IVF, access to mature follicles is compromised or difficult, yes would
operate.
• If AMH normal >2, would consider if had symptom. No symptom, would leave alone and
attempt conservative therapy.
• If AMH 40, no.
•Case #3: Risk of Accreta • 39 year old with infertility and a negative work up other than multiple large fibroids including a transmural FIGO 2-5. I did an open multiple myomectomy removing about 15 fibroids and entered the cavity for the FIGO 2-5. I had her wait 3 months before attempting pregnancy. She was able to get pregnant but had an accreta and IUGR and ended up needing a premature delivery with a complicated post op recovery after her c-hyst. • How do you counsel patients risks after multiple myomectomies for accretas or other complications of pregnancy?
Preop counseling for Accreta/abnormal placentation
• ACCRETA and INTRAUTERINE ADHESIONS definitely needs to be talked about
• If Risk factors present such as devascularization/multiple scars created by a
myomectomy.
-Multiple fibroids
-“cobblestone” uterus
-Extensive reconstruction of the uterus
-Multiple myomectomy surgeries
-Smoking
-Myomectomy combined with multiple prior CS
• The actual risk is unknown but generally rare
• Prevention during surgery: only get the significant fibroids > 1 cm.Preop assessment for “cobblestone uterus”
• US of limited value (can’t see the ovaries,
can’t see the entire uterus)
• MRI is essential in the preop evaluation
• Trying to get pregnant – standard fertility
evaluation
• Defer HSG until myomectomy and normal
cavity is restored
• During surgery, chromotubation will be of
limited value for tubal assessment but
should be done to assessment proximity
or any violation of endometrial cavitySurgical approach for “cobblestone” uterus
• Open v. laparoscopic (as discussed before) to
remove as many but not all of the fibroids
• Staged approach
• 3 months recovery for uterine involution to
occur
• Unless MRI shows obvious SM fibroid, OH/SIS
• If SM fibroids present, proceed with HSC
myomectomyAfter 3 months…..Uterine evaluation
After 2nd surgery, HSC myomectomy….
Postop management of “cobblestone” uterus -ideally should be discussed preoperatively -Communication with her OB (?accreta, CS or not, etc.) -after the uterus involutes, office hysteroscopy or SIS 3 months afterwards -LIKELY HSC myomectomy may be needed to restore normal endometrial cavity anatomy -possible “mock” cycle either naturally or with ERT to see what their EML does (rare since surrogacy not an option at that point)
CASE #4: Large fibroid with endometrial cavity unaffected 41yo G1P0010. 2 prior failed IVF cycles with AMH 0.01 outside facility Uterine fibroids - 10cm, 6cm - not involving cavity with recent hysteroscopy Discussed as a group, recommended to move forward with egg donor. No symptoms OH showed small polyp and proceed forward with hsc polypectomy. Concurrent US showed 8 cm fibroid, posteriorly 1st donor cycle - no embryos for preservation 2nd fresh donor cycle - 12 MII, 7 2PN, 4 cryo embryos Had SAB with her first donor embryo FET. Did cytogenetics on POCs to help decided benefit of fibroid removal before future transfer and of course it came back inconclusive due to maternal contamination.
Posterior SS/pedunculated fibroid
Recommendation:
• Do not operate unless symptoms
• Would operate if 2 or more euploid FET / embryos from donor egg
or >3-4 untested embryos. (this case)
• The better the prognosis, the less embryos I would transfer before
moving forward with surgeryA good surgeon knows also when NOT to
operate…CASE #5: Age impact on myomectomy 43 yo G0 BMI 38 In 2001 had myomectomy done for menorrhagia, dysmenorrhea, symptoms got better 2011 and 2017, HSC myomectomy for worsening symptoms For one year of worsening menorrhagia and dysmenorrhea affecting QOL Wants to get pregnant but no partner, not interested in donor sperm Referred to me for surgery as recommended by her referring MD MRI done
Counseling
• Expected surgery, had to undo that recommendation
• Difficult discussion about her fertility prognosis
• Recommended ovarian reserve testing which she declined to assist in her
decision-making
• Ultimately recommended to her the following options:
1. If low prognosis with AFC and AMH or timeline uncertain or > 1 year or not
open to egg donor/sperm donor, consider definitive surgery, i.e hysterectomy
2. Hysteroscopic myomectomy and hormonal suppression to alleviate her current
symptoms while she figured out her family planning
3. If serious about getting pregnant, Sperm donor with IVF immediately after with
LBR 5% or less
4. Do nothing and proceed with TIC with overall prognosis of LBR 1-2% in her age
group
5. Did not even broach the topic of her weight…she was already mad/irritated
with me for NOT booking her for surgery immediatelyCASE #6: Fibroid actually adenomyosis 36 yo GO SIV EMS HSG outside showed Left mild hydro densely adhered to posterior uterus, right tube open Hx of LSC converted to open because of EMS severity Wants to get pregnant (timeline soon) On OCs with good control of her dysmenorrhea currently MRI showed 6 cm fibroid? (adenomyosis) Normal ovarian reserve AMH 1.7, FSH 7 and E2 < 20 Presented to me for possible myomectomy robotically and options Considering surrogacy
Counseling
• Discussion of my clinical suspicion she had
adenomyosis (had never heard of it) as a
subcategory of endometriosis
• Priority is getting pregnant since symptoms
controlled with OCs
• Given tubal status at minimum
compromised and SIV EMS, recommended
IVF with ET currently (requested HSG
images to assess “severity” of hydro – Left
with no hydro with dye going into probable
adenomyosis interpreted as a hydro, right
tube blocked) LESSON: See images
yourselfRecommendation:
• No immediate plans for surgical
intervention, IVF logistics and if
surrogacy being consider,
perform PGT-A
• If uses uterus, FET #1, if does not
work, FET #2 will do 3 months of
Lupron prior to FET
• Surrogate after two euploid
embryos do not workCASE #6: You don’t have to operate on every fibroid
36 yo GO
Not TTC but in the near future 2 years or so
IUD in place for symptoms
Started on Lupron for surgery to remove
fibroids by her referring provider
IUD currently effective for her symptoms but
wanted to change to different one
AMH 4.08
AFC could not be done due to large uterus,
US limited to assess fibroids
MRI orderedCounseling
• Options d/w patient
1. LSC to remove most but not all the fibroids,
allow 3 months for involution, HSC
myomectomy
2. HSC myomectomy only with IUD removal
3. No surgery, remove IUD and TTC
• Pt prefers the latter, least amount to do
• Recommended #2 and transition to OC’s
• Surgery went well. Normal cavity restored despite
all the other fibroids
• After surgery, proceed with rest of fertility workupCASE #7: BMI impact on Fibroid management 34 yo GO Not TTC but in the near future Seen for menorrhagia and pain IUD inserted, symptoms got better Referred to me for possible surgical intervention BMI 41, 5’3” and 230 lbs ?QOL – not bad with IUD, wants other options Checked labwork – slightly anemic, normal thyroid and prolactin In followup, talked about Lupron, combination hormonal suppression, surgery, elected to add in Ring Talked about risk of surgery, doing ok on IUD and Ring combination, continuing to lose weight TAKE HOME MESSAGE: unless symptoms intolerable, no rush to make the surgical situation optimal
BMI – if you can wait, wait
• Be patient
• As surgeon, operate and operate quickly “get it out mentality”
• BMI >40, needs to be 40 AND AGE >40 but IVF literature
(https://doi.org/10.1016/j.fertnstert.2014.03.012) suggesting that waiting 3 months in women
>40 had no impact on IVF outcomes
• Use it as a trial for patient to lose weight, refer to nutritionist.CASE #8: Endometriosis surgery after multiple IVF cycles
38 yo G4P1031
3 SAB
1 spontaneous full term pregnancy
Dysmenorrhea mild to moderate
AMH 0.8, AFC 7
IVF X2, 2 ET, 2 FET – no pregnancies
Interested in surgical interventionCASE #8: Endometriosis surgery after multiple IVF cycle failures
• Probably does not work and if it does, the impact is minimal with many needing to have surgery
to gain one extra pregnancy
• Medical therapy such as LTZ and Lupron could have benefit
• Women with EMS have a lower chance of implanting due to poor egg quality but not due to
endometrial environment
• Prospective studies looking Donor egg embryos showed not difference in pregnancy rate,
implantation rate, miscarriage rates in woman with endometriosis compared to controls
• SART data confirms very little difference in LBR in women with EMS compared to woman with
multiple factors related to fertility
• Surgery should be done for symptomatic reasons and not for fertility enhancement
• RECOMMENDATION:
-Lupron and letrozole may have some benefit for ART benefit. Side effect
profile may favor letrozole.
-No surgery recommended unless symptomaticSurgery done for symptoms
• Stage I EMS
• Path confirmed
• Both tubes open
• TTC on own for 6 months
• Doing another IVF cycle #3 without
letrozole and without Lupron
• Outcome unknownThank you!
You can also read

















































