IBS-D and Evaluation of Chronic Diarrhea - Amy Foxx-Orenstein, DO, MACP, FACP Professor of Medicine Division of Gastroenterology and Hepatology ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

4/22/2019
IBS-D and Evaluation of Chronic
Diarrhea
Amy Foxx-Orenstein, DO, MACP, FACP
Professor of Medicine
Division of Gastroenterology and Hepatology
Mayo Clinic
AOMA 97th Annual Convention
©2018 MFMER | slide-1
No Disclosures
©2018 MFMER | slide-2
1
4/22/2019
IBS-D Outline
• Evidence-based criteria to evaluate patients
with IBS symptoms
• Cost-effective evaluation and treatment
• Traditional and newer treatments for patients
with IBS-D
©2018 MFMER | slide-3
Representative Case
• 35 year old female with 8 years of abdominal
cramping, bloating and diarrhea on most days.
No bloody stools or nocturnal episodes. Has 3-4
loose stools daily with urgency, yet never had
an ‘accident’. LLQ cramping is relieved with
movements. Has hypothyroidism and anxiety,
on treatment. Weight is stable. No family history
of IBD or colon cancer/polyps.
• Does she have IBS?
• Are there other diagnosis to consider?
• What tests would you do to evaluate cause?
©2018 MFMER | slide-4
2
4/22/2019
What Else Could It Be?
Differential for diarrhea is broad and the history will
divulge many clues
• Infectious • SIBO
• Post-infectious • IBD
• Medication • Disaccharidase deficiency
• Bile acid • Food related
• Microscopic colitis • Villous adenoma
• Celiac • Toxins
• Caffeine
©2018 MFMER | slide-5
Rome IV Criteria for IBS
Recurrent abdominal Bristol Stool Form Scale
pain, on average, ≥1 day
per week in the last 3
months, associated with ≥
2 of the following:
• Related to defecation
• Change in frequency of
stool
• Change in form
(appearance) of stool
Criteria should be fulfilled
for the last 3 months with
symptom onset ≥ 6 months
before diagnosis IBS-D IBS-M
Lacy BE et al. Gastroenterology. 2016;150:1393-1407
©2018 MFMER | slide-6
3
4/22/2019
Limited testing
Diagnostic Testing for IBS-D and IBS-M
symptoms
IBS-D IBS-M
• CRP, fecal calprotectin • CRP, fecal calprotectin
• IgA ttG ± quantitative IgA • IgA ttG ± quantitative IgA
• Colonoscopy with random
biopsies and TI exam if
appropriate
• Consider EGD with small CRP = C-reactive protein
bowel biopsies ttg = tissue transglutaminase.
Chey WD, et al. JAMA. 2015;313:949
©2018 MFMER | slide-7
Limited testing
Prevalence of Structural Abnormalities
in IBS Patients Compared with Controls
IBS patients (n=466) Controls (n=451)
30
26.1
25
Patients, %
20
15
10 7.7
5
0.4 1.5
0 N/A
0
Adenomas IBD Microscopic colitis
Microscopic colitis more
common in IBS-D patients
aged ≥45 years
Chey WD et al. Am J Gastroenterol. 2010;105:859
©2018 MFMER | slide-8
4
4/22/2019
Proceed with testing
Alarm Features
• Onset of symptoms after age 50
• GI bleeding or iron-deficiency anemia
• Nocturnal diarrhea
• Unintended weight loss
• Family history of organic GI disease
(colorectal cancer, IBD, celiac)
©2018 MFMER | slide-9
Celiac is Common in IBS Patients with
Diarrhea
Prevalence of biopsy-proven celiac
disease in IBS-D vs controls
4.34 (1.78-10.58)
International meta-analysis
Ford et al. Archives Int Med. 2009;169:651
©2018 MFMER | slide-10
5
4/22/2019
IBS and Wheat
• Most IBS patients have
wheat sensitivity,
Not celiac disease!
Leonard MM et al. JAMA. 2017;318:647
Talley NJ. JAMA Intern Med. 2017;177:615
©2018 MFMER | slide-11
Breath Testing in IBS
• Tests for CHO
Carbohdrate maldigestion
load
and SIBO
H2 and/or
methane • Conditions
associated
with bloating
• Heterogeneity in test
performance,
Colonic preparation,
fermentation
indications, and
interpretation of
results
CHO = carbohydrate
SIBO = small intestinal bacterial overgrowth
Rezaie A et al. Am J Gastroenterol. 2017;112(775
©2018 MFMER | slide-12
6
4/22/2019
Food and IBS Symptoms
60% of patients report worsening of symptoms
after meals
IBS Patients Reporting Symptom Improvement
With Intervention
100 (N=1,242)
Patients, %
80 69
64
58 54
60
40
20
0
Small meals Avoiding fat Increasing Avoiding milk
fiber products
Simren M et al. Digestion. 2001;63:108
Halpert et al. Am J Gastroenterol. 2007; 102:1972
©2018 MFMER | slide-13
Food and IBS Symptoms: Restriction Diets
• FODMAPS are an important trigger of
meal-related symptoms in IBS
• Gluten-free diet found to be beneficial
in some patients with IBS-D
• Wheat contains fructans and other
proteins that may also cause
symptoms in IBS patients
• Food antigens may cause changes in the
intestinal mucosa of IBS patients
Shepherd SJ et al. Am J Gastroenterol. 2013;108:707;Biesiekierski JR et al. Gastroenterology.
2011;106:508;Vazquez-Roque MI et al. Gastroenterology. 2013;144:903;Chey WD, et al. JAMA. 2015;313:949
©2018 MFMER | slide-14
7
4/22/2019
Low FODMAP vs mNICE Diet:
Adequate Relief
“In the last week, have you had
adequate relief of your GI symptoms?”
P=0.3055
60
52
Adequate Relief, %
50
41
Patients with
40
30
20
10
N=45 N=38
0
mNICE Low FODMAP
Proportion of patients that answered “Yes” for ≥50% of weeks 3 and 4
mNICE, modified National Institute for Health and Care Excellence. Patients were instructed to
eat small frequent meals, avoid trigger foods, and avoid excess alcohol and caffeine
Eswaran SL, et al. Am J Gastroenterol. 2016;111:1824-1832.
©2018 MFMER | slide-15
mNICE vs FODMAP
Weekly Pain and Bloating Scores
Abdominal Pain Scores Bloating Scores
6 6
Average Daily Abdominal Pain
Average Daily Abdominal
Bloating Score (0-10)
5 5
○
Scores (0-10)
4 4 #
§
§ §
3 § 3 §
§
2 2
1 1
Baseline Week 1 Week 2 Week 3 Week 4 Baseline Week 1 Week 2 Week 3 Week 4
m-NICE Low FODMAP m-NICE Low FODMAP
mNICE, modified National Institute for Health and Care Excellence. Patients were instructed to
eat small frequent meals, avoid trigger foods, and avoid excess alcohol and caffeine
Eswaran SL, et al. Am J Gastroenterol. 2016;111:1824-1832.
©2018 MFMER | slide-16
8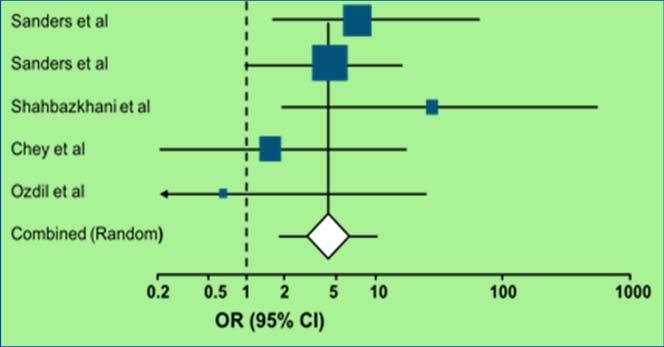
4/22/2019
Overview of IBS-D Therapies: MOA*
*MOA = Mechanisms of action
• Modulation of gut flora
• Antibiotics, Probiotics, gastric acidity, diet
• 5-HT3 antagonists
• Alosetron
• Antidepressants/antianxiety agents
• TCA’s, SSRI’s
• Opioid receptor modulators
• Loperamide, diphenoxylate, Eluxadoline
• Antispasmodics/Peppermint Oil
• Bile acid binding agents
• Colestid, Cholestyramine
©2018 MFMER | slide-17
Loperamide and Antispasmodics for IBS
Recommendation
2 Strong*
Clinical trials
Loperamide *FOR DIARRHEA
42 Quality of evidence
Patients treated Very Low
Recommendation
23 Weak
Antispasmodics Clinical trials
2,154 Quality of evidence
Patients treated Low
Ford AC, et al. Am J Gastroenterol. 2014;109:S2-S26
©2018 MFMER | slide-18
9
4/22/2019
Probiotics for IBS
23 2,575
Recommendation
Clinical trials Patients treated Weak
Recommendations regarding Quality of evidence
individual species, preparations, Low
or strains cannot be made
because of insufficient
and conflicting data
Ford AC, et al. Am J Gastroenterol. 2014;109:S2-S26
©2018 MFMER | slide-19
Alosetron for IBS-D
• Dose Recommendation
Alosetron is Strong
• .5-1 mg BID effective in
• Females females with
Quality of evidence
IBS-D
• Not first line treatment High
Rare Adverse Effects
Associated with Alosetron
Ischemic colitis
0.95 cases/1000 patient-years
Difficult constipation
0.36 cases/1000 patient-years
Ford AC, et al. Am J Gastroenterol. 2014;109:S2-S26
©2018 MFMER | slide-20
104/22/2019
Rifaximin for IBS-D
Adequate Relief of First and Second
Global* IBS Symptoms Retreatments
Urgency, bloating, pain, stool consistency
100 100
80 80
P=0.01
Patients, %
P=0.03 P4/22/2019
Antidepressent Agents in IBS-D
• Meta-analysis 16 RCT Antidepressant actions in IBS
TCA and SSRI reduced
Antidepressant
global pain and IBS action
symptoms
• SSRI’s may increase Visceral analgesia
intestinal transit
• SNRI’s have not been
adequately studied
Changes in motility
Smooth muscle
relaxation
Ford AC et al. Am J Gastroenterol. 2014;109:1350;Grover M, et al Gastroenterol Clin N Am. 2011;40:183;Chey
WD, et al. Gut Liver. 2011;5:253;Gorard DA, et al. Aliment Pharmacol Ther. 1994;8:159
©2018 MFMER | slide-23
Prescribing Antidepressants in IBS
Consider specific symptoms
TCA’s in IBS-D
SSRI for anxiety
Consider Side Effects
TCA’s → constipation
SSRI → diarrhea
Start LOW dose and titrate
8 weeks for full response
6-12 months treatment
Sobin WH et al. Am J Gastroenterol. 2017;112:693;Grover M et al. Gastroenterol Clin N Am. 2011;40:183;Dekel
R et al. Expert Opin Invest Drugs. 2013;22:329
©2018 MFMER | slide-24
124/22/2019
Eluxadoline for IBS-D
Mixed opioid receptor agonist (mu) and antagonist (delta)
Placebo BID Eluxadoline 75 mg BID Eluxadoline 100 mg BID
Weeks 1–12 Weeks 1–26
100 100
P4/22/2019
Prescribing Eluxadoline
• 100 mg BID with food
• 75 mg BID for patients
with hepatic impairment
Contraindications
1. Bile duct disorders
2. NO Gallbladder
3. History of pancreatitis
4. Severe constipation or liver disease
5. ETOH daily
©2018 MFMER | slide-27
Peppermint Oil for IBS
• Improved total IBS
symptom score, frequency
and intensity of symptoms
over 4 weeks (p4/22/2019
Psychological Therapy is Effective in
Many Patients With IBS
N=1278
• 20 studies
• Mindfulness, cognitive behavioral therapy, psychotherapy,
hypnosis
Psychological therapy Control therapy RR symptoms remain
(%) (%) (95% CI)
0.67
49.1 27.5
(0.57-0.79)
Patients often respond to psychological support,
including strong physician-patient relationship
Ford AC et al. BMJ. 2008;337:a2313.
Walter SA et al. Neurogastroenterol Motil 2013;25:741.
Halland M, Talley NJ. Nat Rev Gastroenterol Hepatol 2013;10:13.
©2018 MFMER | slide-29
Exercise Has a Positive Impact on IBS
Symptoms
(N=75)
Start 12 Weeks
• Randomized to physical
P = 0.001
activity* or maintain lifestyle
• Control group had 500
IBS Severity Score
significantly higher IBS
400
symptom scores than patients
in physical activity group 300
200
• Physical activity improved
IBS symptom scores (p=0.003) 100
Control group Physical activity
0 group
*Intervention: 20-60 minutes moderate to
vigorous exercise 3-5 times weekly
Johannesson E et al. Am J Gastroenterol. 2011;106:915-922.
©2018 MFMER | slide-30
154/22/2019
Summary IBS-D
• Diagnose using symptom-based criteria
• Check TTG, CRP
• Consider referral for endoscopy, breath tests
• Educate
• Primary role of diet in managing IBS
• Smaller meals, FODMAP, elimination
• Medications to achieve a goal: reduce pain and
diarrhea, improve quality of life
• Psychological therapy
• Exercise
©2018 MFMER | slide-31
The End
But there’s more…
©2018 MFMER | slide-32
164/22/2019
Evaluation and Management of
Chronic Diarrhea (not IBS)
©2018 MFMER | slide-33
Outline
• Stepwise approach to diagnosis and
management of chronic diarrhea
• Features of chronic diarrhea that warrant an
evaluation
• When and what tests are warranted
©2018 MFMER | slide-34
174/22/2019
Representative Case
• 53 y/o woman with diarrhea for 2 years. She has 4-6
watery stools daily, no formed stool. No blood, but she
has nocturnal stools, cramps and bloating. Medical
history of hypothyroidism and depression (treated).
Underwent a hysterectomy and radiation therapy for
cervical cancer 5 years ago.
• Does she have IBS?
• Are there historical clues in this case?
• What testing would you do?
©2018 MFMER | slide-35
Why is Diarrhea Important?
• Diarrhea is common
• You will see it!
• Affects 1-5% of the adult population
• $$ There can be considerable expense in the
work-up/management.
• Cost effective evaluation can be smart
• Differential can be broad
• Distinguishing alarm features is critical
©2018 MFMER | slide-36
184/22/2019
Step-Wise Approach to Diarrhea
• 1. Does the patient truly have diarrhea?
• 2. Is the diarrhea really chronic?
• 3. Can you categorize the diarrhea?
• 4. Are there historical clues to the diagnosis?
• 5. Is it diet or medication-induced?
• 6. Is there a factitious component?
Schiller LR, et al. CGH 2017;15:182
©2018 MFMER | slide-37
Step 1: Does the patient truly have
diarrhea?
• Fecal incontinence?
• Overflow from fecal impaction?
• Perception versus reality of volume /
frequency?
©2018 MFMER | slide-38
194/22/2019
Definition of diarrhea
• In past, based on volume and time:
• >200-250 g (or ml) per day
• >4 weeks
• Current way we diagnose:
• >3 unformed BM/day
• >25% loose or mushy stools
• Bristol stool scale 6 or 7
©2018 MFMER | slide-39
Step 2: Does the patient have acute or
chronic diarrhea?
• Acute = 2-4 weeks
• Chronic = >4 weeks
OR
©2018 MFMER | slide-40
204/22/2019
Step 3: Can you categorize the diarrhea?
• Watery
• Secretory versus osmotic
• Inflammatory
• Bloody stools, abdominal pain, fever, tenesmus
• Fatty
• greasy, oily, difficult to flush, floating stools, smelly
• Not specific!!!
• Large or small bowel intestine source
• Often differs in volume and frequency
©2018 MFMER | slide-41
Small bowel:
large volume, vitamin and
mineral deficiencies
Colon:
Smaller volume (not always),
frequent, bloody, tenesmus
with rectal involvement
©2018 MFMER | slide-42
214/22/2019
Tests Based on Characteristics
• Watery: Secretory versus Osmotic
• Osmotic gap = 290 mOsm/kg-2(stool Na+K)
• Gap < 50 Secretory
• Gap > 100 Osmotic
• Stool osmolality:
• Should be the same as serum e.g. 2(140+ 4)= 288
• Lower - urine or water contamination
• Higher - stool collection sitting around
©2018 MFMER | slide-43
Osmotic Secretory
Daily volume 1L
Effect of Fast Stops continues
Stool osmolality 290 290
Osmotic gap >1004/22/2019
Osmotic Secretory
Testing Dietary review Cultures
Strategy Malabsorption Structural
(breath tests, evaluation:
avoidance, small colon biopsies.
bowel biopsy) Neuroendocrine
Stool VIP, calcitonin,
magnesium gastrin
©2018 MFMER | slide-45
Tests based on characteristics
• Inflammatory:
• +CRP, fecal calprotectin or lactoferrin
• If positive, these are nonspecific
• Differential:
• infection, inflammation, ischemia,
radiation
• Often structural evaluation is needed
• colonoscopy and/or EGD with biopsies,
enterography
©2018 MFMER | slide-46
234/22/2019
Tests based on characteristics
• Fatty / Steatorrhea
• Symptoms: malodorous diarrhea, weight
loss, vitamin ADEK deficiencies
• Etiology: pancreatic, mucosal (e.g celiac,
Whipple’s disease)
• Tests:
• Qualitative fecal fat (Sudan stain) –’meh’!
• Fecal elastase ( pancreatic disease)
• Quantitative fecal fat (collection 24-72 hr)
normal < 7g/day or4/22/2019
Irritable bowel syndrome (IBS) ROME 4
• Recurrent abdominal pain on average at least 1
day/week in the last 3 months a/w 2 or more
features:
• Related to defecation
• Change in frequency of stool
• Change in form/consistency of stool
• Symptoms present at least 6 months
• In absence of alarm features manage
symptoms
Gastroenterology 2016:150:1393
©2018 MFMER | slide-49
Important in History/Exam
• If ALARM features are present, further workup
is needed:
• Bloody stool, weight loss, family history of
IBD or bowel cancer, new onset, older age,
immunosuppressed
• Keep in mind routine colorectal cancer
screening or surveillance based on age and risk
factors
©2018 MFMER | slide-50
254/22/2019
Step 5: Does the Patient Have Diet-
Induced Diarrhea?
• DIET
• Caffeine
• Soda, fruit/juice (fructose)
• Sweeteners (sucrose)
• Sugar free anything (xylitol)
• Dairy (lactose)
• Wheat (celiac, allergy, sensitivity)
• Syrups, elixirs (sorbitol)
©2018 MFMER | slide-51
Step 5: Does the Patient Have
Medication-Induced Diarrhea?
• >700 drugs implicated
• Makes up 7% of medication side effects!
Some to Remember:
NSAID Mg+
Metformin
Angiotensin receptor blockers (olmesatan)
Antibiotic
Herbal products
PPI
SSRIs Many chemotherapy agents
Rubio-Tapia A, et al. Mayo Clinic Proc 2012;87:732
Prieux-Klotz C, et al. Target Oncol 2017;12:301
©2018 MFMER | slide-52
264/22/2019
Step 6: Is there a factitious component?
• Stool osmolality not equal to 290 (diluted)
• Munchausen syndrome
• Melanosis coli
• Pigment from stimulant laxative use
• Benign/reversible
• Up to 15% undergoing diarrhea workup
©2018 MFMER | slide-53
Evaluation May Include:
Baseline Labs CBC, TTG, TSH, e-lytes,
CRP, vitamin levels
Stool Tests Calprotectin, lactoferrin, infectious panel,
parasites (Giardia), elastase, c diff, osmol
Endoscopy Colonoscopy with TI exam and biopsy,
EGD with SB biopy and aspirates
Imaging CT enterography, MRE
Quantitative Stool Tests 24-72 hour fat or bile acid collection
Very Individualized!
©2018 MFMER | slide-54
274/22/2019
Summary
• Many etiologies for diarrhea can be deciphered
from a careful history and examination
• A stepwise approach for diarrhea is cost-
effective and efficient.
• #1. Does the patient truly have diarrhea?
• #2. Is it chronic?
• #3. How is it characterized (watery, fatty, inflammatory)
• #4. Historical clues to the diagnosis? (travel, illness, medications)
• #5. Diet or medication induced?
• #6. Could it be factitious?
©2018 MFMER | slide-55
Thank you!
Foxx-Orenstein.amy@mayo.edu
©2018 MFMER | slide-56
28You can also read