COVID-19 Non-Invasive Mechanical Ventilation In The Treatment of
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Non-Invasive Mechanical
Ventilation In The Treatment of
COVID-19
Leonardo Seoane M.D, F.A.C.P
Chief Academic Officer, Senior System Vice President
Ochsner Health
Professor University of Queensland/Ochsner Clinical School
Associate Vice-Chancellor Academic Affairs
LSUHSC-Shreveport
Objectives • List evidence-based therapy for Hospitalized COVID- 19 patients • List lessons learned from the use of HFNC/NIVM in in the first wave of COVID-19 in the U.S. • Describe an evidence-based approach to the use of HFNC/NIMV in COVID-19
Ochsner Health: COVID-19 Census

Risk Factors for Severe Disease
• Demographics • Comorbid Conditions
• Age > 55 • Chronic lung disease
• Male – COPD, lung cancer,
moderate to severe
• Racial and ethnic asthma, IPF, CF
minority group
• Heart Disease
• Resident of long-term
• Obesity
care facilities
• Chronic liver of kidney
disease
• Immunocompromised
CHEST 2021
Current Treatments for COVID-19
Prevention
• social distancing
• masks Innate
• vaccines
Immune Adaptive
Antiviral Rx
• remdesivir Respons Immunity
Passive Tx (Ab)
– bamlan+etesevimab e
– casirivimab+imdevimab
– convalescent plasma
Anti-inflammatory Rx Viral
– Steroids
– Tocilizumab
Load
– Baricitinib
Other
– anticoagulation
Current COVID-19 Treatments
Evidence Based Therapies
Monoclonal Antibodies
Need to Treat 21 Patients to Avoid 1
Hospitalization
High Titer Convalescent Plasma
Need to Treat 7 Patients to Prevent 1
Occurrence of Severe Respiratory Disease
Dexamethasone
Need to Treat 8 Patients to Save 1 Life
Remdesivir
Improves Time to Recovery
Non-Invasive Ventilation
Prevents Need for Mechanical Ventilators
Anti-Inflammatories (Tocilizumab)
Data not compelling
Remdesivir ACTT-1 Outcomes
Median time to recovery:
– Remdesivir 10 days vs. placebo 15 days
– 1.29; 95% [CI], 1.12 to 1.49; P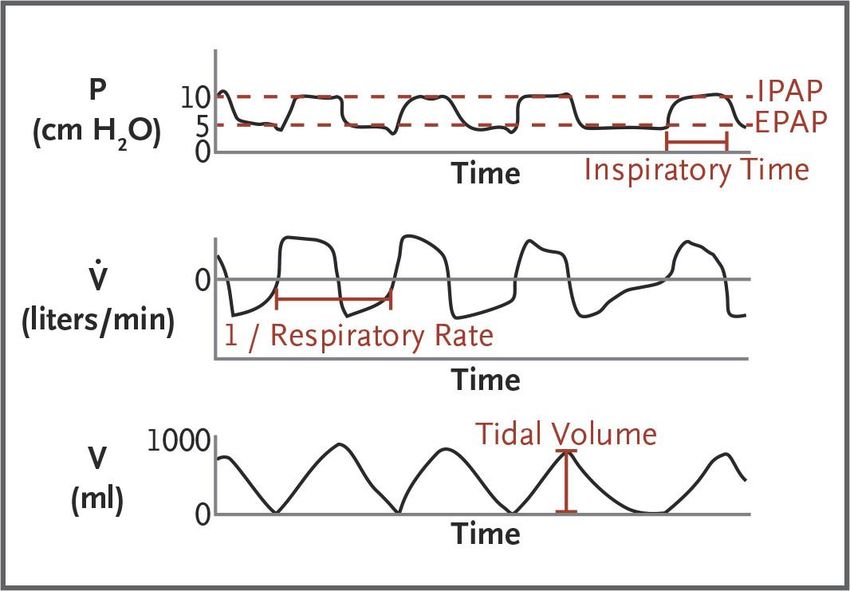
Recovery Trial Our results show that among hospitalized patients with Covid-19, the use of dexamethasone for up to 10 days resulted in lower 28-day mortality than usual care in patients who were receiving invasive mechanical ventilation at randomization (by 12.3 age-adjusted percentage points, a proportional reduction of approximately one third) and those who were receiving oxygen without invasive mechanical ventilation (by 4.2 age-adjusted percentage points, a proportional reduction of approximately one fifth). However, there was no evidence that dexamethasone provided any benefit among patients who were not receiving respiratory support at randomization, and the results were consistent with possible harm in this subgroup. Dexamethaasone 6mg IV/PO q 24 hours up to 10 days
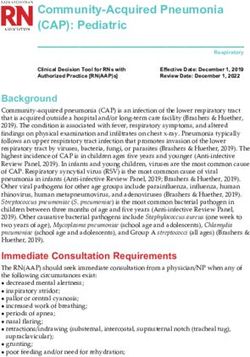
65 y/o female presents to ED complaining of fever, non- productive cough, severe muscle pain and SOB. She recently visited friends who now have tested positive for COVID-19. She did not get vaccinated because she “doesn’t want to be a Guinea Pig”. On exam she is breathing 30 times a minute using accessory muscles. Pulse oximetry reveals 90% Saturation on 50% Venturi mask. Chest Radiograph is below:
With regards to her hypoxemic respiratory failure what is the next best step? A. Place 100% Non-rebreather mask B. Start NIMV with Bipap and 100% FIO2 C. Start High Flow Oxygen through Nasal Cannula at 30 l/min and 100% FIO2 and trial of prone position D. Immediately intubate and place on Assist Control with 6-8 cc/kg TV and 100% FIO2
Normal Rat Lungs and Rat Lungs after Receiving High-Pressure
Mechanical Ventilation
Malhotra A. N Engl J Med 2007;357:1113-1120Biotrauma
TNF
IL-6
Granton JT, Slutsky AS, in Hall, Schmidt, Wood: Principles of Critical Care, 2005What is wrong with early
intubation in COVID-19
• Worsening acute lung injury due to ventilator
induced lung injury
• Requirement for heavy sedation
• Reliance on mechanical ventilators which
could be in limited supply in pandemic
• Intubation procedure may be high risk
exposure for health care team
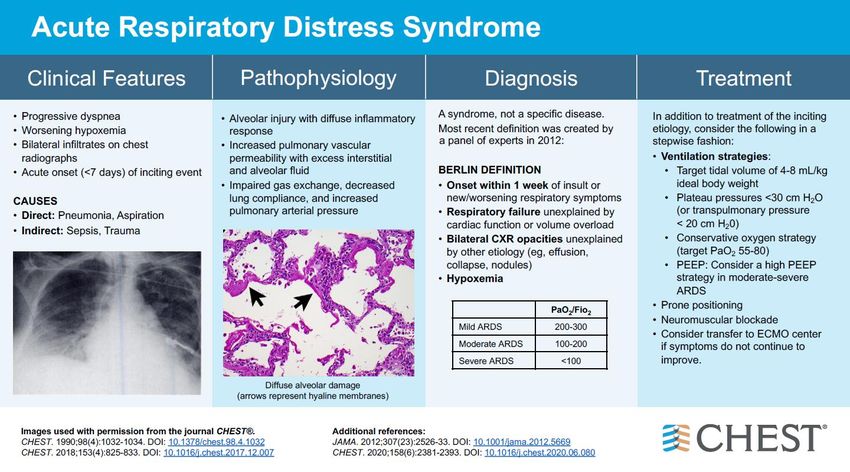
• Worst OutcomesOriginal Article
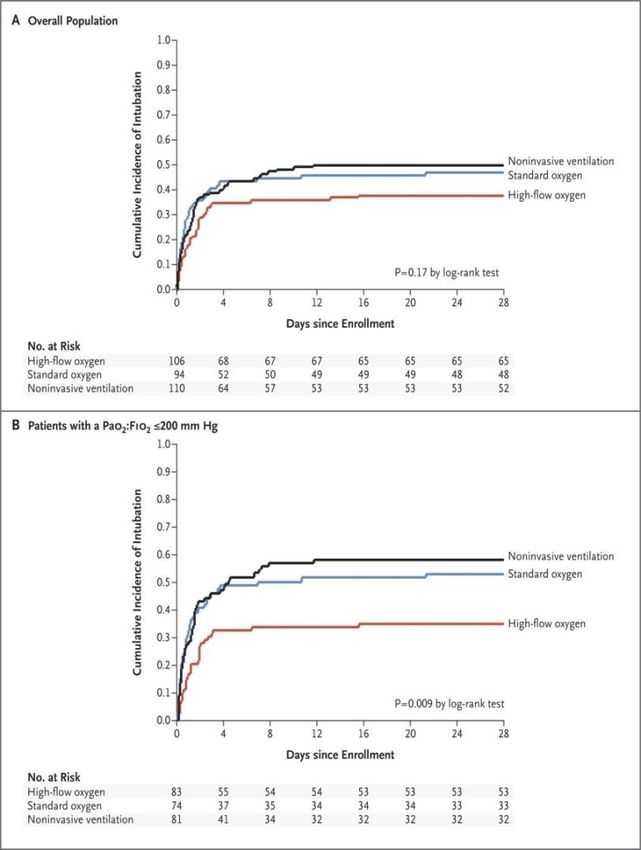
High-Flow Oxygen through Nasal Cannula in Acute
Hypoxemic Respiratory Failure
N Engl J Med 372(23):2185-2196 June 4, 2015
• Patients with acute hypoxemic respiratory failure were
assigned to standard oxygen therapy, high-flow
oxygen therapy, or noninvasive ventilation.
• The intubation rate did not differ significantly among
the groups, but 90-day mortality was lower in the high-
flow–oxygen group.N Engl J Med 372(23):2185-2196 June 4, 2015
High-Flow Oxygen through Nasal Cannula in Acute Hypoxemic
Respiratory Failure
N Engl J Med 372(23):2185-2196 June 4, 2015
Kaplan–Meier Plots Incidence of Intubation
Kaplan–Meier Plot of the Probability of SurvivalDoes HFNC Increase Bio-aerosol
Oxygen Device Flow rate in L/min Dispersion in cm
HFNC 60 17
30 13
10 7
Simple mask 10 10
Non-rebreather 25
Venturi mask .4 FiO2 6 40
Venturi mask .35 FiO2 6 27
Hui et Eur Respir J 2019; 53: 1802339.
Ip M et al Am J Infect Control 2007;35:684-689HFNC in COVID 19
Article Type of Study Number of Results
patients
Am J Resp Crit Retrospective Cohort 379 Decrease intubation
2020;202:1039-42 No difference in mortality
Heart & Lung Retrospective Cohort 43 Decrease intubations and 28-day
2021;50:425-29 mortality
Heart & Lung Case Series 8 Only 1 of 8 required intubation
2020;49:444-445
Eur J Clin Invest Retrospective Cohort 22 Improve gas exchange and ICU length
2021;51:e13435 of stay
Lancet 2020:395 Retrospective Cohort 41 Decreased intubation
BMC Pum Med Retrospective 105 62% avoided intubation ROX index >5.5
2020;20:324 observational study after 6 hours predicted success
Doi.org/10.1016/J.ajem. Observational trial 23 No difference in intubations or
2020.07.071 mortality
Health Sci Report 2021;4: Observational Trial 42 ROX index of 4.8 or greater associated
e287 with success, 52% avoided intubationOchsner’s Early Phase Response to
COVID-19 Respiratory Failure
• >90% vent rate in ICU
• Early Intubation and Mechanical Ventilation for COVID-
19 respiratory failure recommended by European
Respiratory Society
Admission Vent Discharge/Death
95% VentedOchsner Second Phase: Adjusted Response to
COVID-19 Respiratory Failure
• Introduce alternate modalities with the goal of
delaying/avoiding ventilation
Admission Vent Discharge/Death
70% Vented
Admission NIPPV/HFNC Vent Discharge/Death
40% VentedICU Census, Capacity, Mechanical Ventilator and
Utilization of Mechanical Utilization Model
Ventilators over time In 400
COVID-19 Pandemic 350
• Over 90% of patients admitted to
the ICU required mechanical 300
ventilation in first 2 weeks
250
• Followed current guidelines for
early intubation to facilitate 200
infection control
• Changed practice to HFNC or 150
NIMV per physician late March
100
2020
• Drop in MV utilization prior to 50
peak ICU admissions
• Significant reduction in use of 0
16-Mar
18-Mar
20-Mar
22-Mar
24-Mar
26-Mar
28-Mar
30-Mar
1-Apr
3-Apr
5-Apr
7-Apr
9-Apr
11-Apr
13-Apr
15-Apr
17-Apr
19-Apr
21-Apr
23-Apr
25-Apr
27-Apr
29-Apr
Mechanical Ventilators
OH COVID ICU CAPACITY OH NON-COVID ICU
1.3 ICU 1.3 Vent
0.8 ICU 0.8 Vent
1.1 ICU 1.1 Vent
Actual ICU Actual VentNIMV & HFNC Decrease Risk of Intubation Among
COVID-19 Patients with Respiratory Failure
Therapy (n) # Intubated % Intubated
Standard (542) 433 80%
HFNC (80) 23 29%
NIMV (99) 38 38%
Therapy Hazard Ratio (95% CI) Covariates
HFNC 0.4 (0.29-0.55) Age
NIMV 0.26 (0.18-0.36) Gender
Race
Obesity
SOFA
Seoane et al. Unpublished DataCan non‐invasive positive pressure ventilation prevent endotracheal intubation
in acute lung injury/acute respiratory distress syndrome? A meta‐analysis
Respirology
Volume 19, Issue 8, pages 1149-1157, 10 SEP 2014 DOI: 10.1111/resp.12383
http://onlinelibrary.wiley.com/doi/10.1111/resp.12383/full#resp12383-fig-0004NIMV in COVID-19
Article B Type of Study Number of Results
patients
Am J of Emer Med Retrospective 61 Feasible with 72% of
2021;39:154-57 Cohort patients not requiring
intubation
BJ Anes Case series 103 ½ of NIMV avoided
2020;125:e368-71 intubations
Anest CC Pain Med Retrospective 39 patients 77% avoided intubations
2020;39:579-80 observational
JAMA Systematic Review 3804 Improved survival NIMV
2020;324:57-67 and meta-analysis of Survival benefit loss with
HRF and NIMV paO2/Fio2 less 200
Am J of EM Retrospective cohort 222 Decrease in mortality
2021;43:103-108 No difference in mortality
in early intubation vs failed
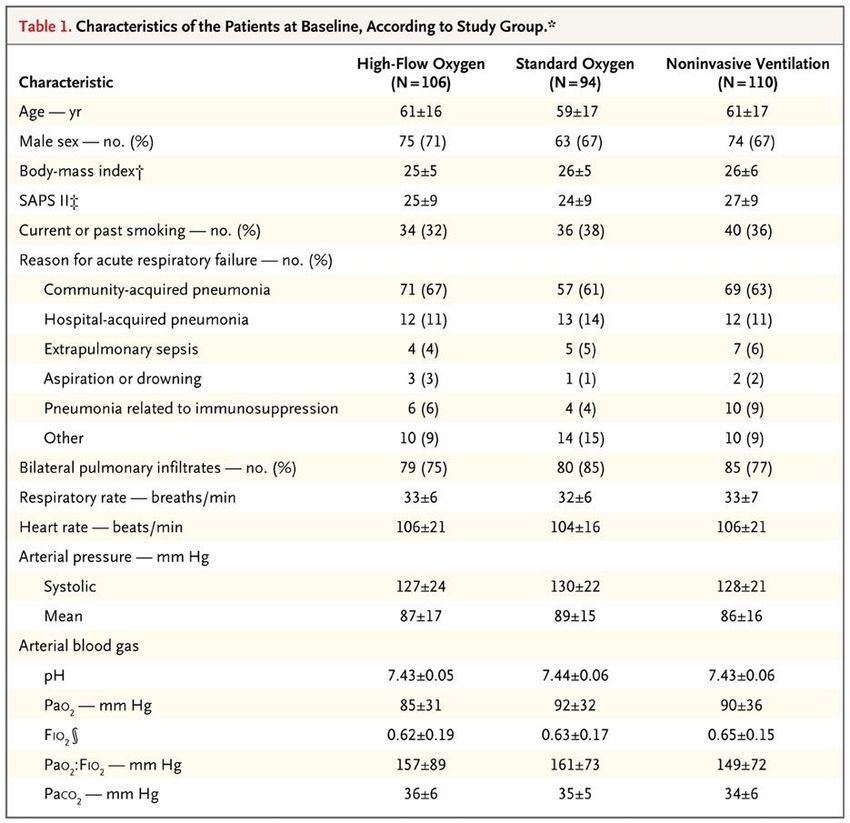
NIMVNasal Pillows Nasal Mask Oronasal Mask Total-Face Mask
Kelly et al. NEJM 2015;372:e30Rationale
• Reduce the need for intubations
– Avoid complications of invasive ventilation
• ETT trauma
• VAP
• Sinusitis
• Interference with upper airway function and
comfort
–Speech
–Eating
• Ventilator induced lung injury?Contraindications • Absolute Contraindications – Hemodynamic instability/cardiac arrest – Respiratory arrest • Relative Contraindications – Inability to tolerate mask (Claustrophobia) – Large volume secretions – Unstable airway – Recurrent emesis – ?Decreased mental status
Complications Associated with NPPV
Kelly et al. NEJM 2015;372e30
Complication Response
Air Leak Ensure correct size and fit of mask
Use mask of a different size or type
Tighten straps
Reduce airway pressures, if possible
Skin irritation or abrasion Apply artificial skin or dressing
Claustrophobia Redirect the patient
Use less obtrusive mask
Light sedation
Nasal congestion or sinus pain Topical decongestants
Humidify inspired air
Reduce airway pressure
Mucosal dryness Humidify inspired air
Mucus plugging Humidify inspired air
Chest percussion during breaks from NPPV
Reduce airway pressure
Pulmonary Barotrauma or pneumothorax Stop ventilation or reduce airway pressures
Aerophagia/gastric distention/ aspiration Use minimal airway pressures
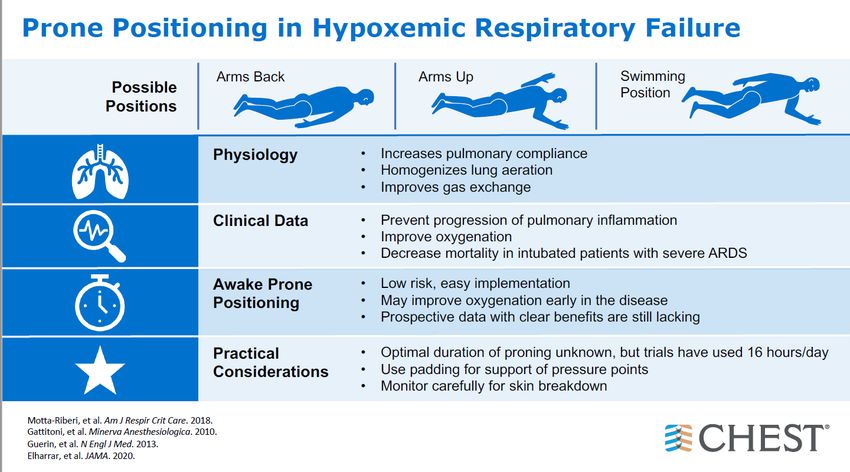
Place nasogastric tubeProning • PROSEVA trial • Prone PaO2/FiO2 ratio < 150 • Target SpO2 92-96% • 16 hours daily
Landmark PROSEVA Trial
Kaplan–Meier Plot of the Probability of Survival from
Randomization to Day 90.
N Engl J Med 2013; 368:2159-2168
DOI: 10.1056/NEJMoa1214103
Guérin C et al. N Engl J Med 2013;368:2159-2168.Prone Position in MV COVID-19 Patients
• Cohort study 702 patients from 68 hospitals across
the U.S.1
– Prone patients within 2 days of ICU had lower adjusted risk
of death
– Hazzard ratio .84 (95% CI, .73- .97)
• Multicentric Study 1000 patients
– No improvement in ICU survival
– Improvement in PaO2
– Responders had improved ICU survival 65% vs 38%
1) Mathews doi: 10.1097/CCM.0000000000004938
2) Langer doi.org/10.1186/s13054-021-03552-2Awake Prone Position
• RR> 30, SpO2 < 93% room air, HR>120
• Conscious and responsive patient
• If no response or can’t tolerate, return to supine
• Feasible and safe with little downside
– HFNC or NIMV
• Awake Prone position and fluid restriction
• Case series reported decrease mortality1
• Associated with averting or delaying MV 2,3
1) Sun Q et. Ann Intensive Care 2020;101(1):33
2) Elharar et al JAMA 2020;323: 2336-38
3) Sartini et al. JAMA 2020;323:2338-40Awake Prone Position in COVID-19 Patients-A
Systematic Review and Meta-analysis
• 25 observational studies including 758 patients
• Improvements:
– PaO2/FiO2 ratio 39 (CI 25-54)
– PaO2 20 mm Hg (CI 14-25)
– SpO2 4.7% (CI 3-6)
– Respiratory Rate -3 breaths (CI -2-5)
• No difference in intubation rates if proned in or out of ICU
Mallikarjuna doi: 10.1097/CCM.000000000000508655 y/o woman with COVID-19 pneumonia and respiratory failure has required mechanical ventilation for pass 3 days. She passed SBT this am and was extubated to NC and initially does well but then develops respiratory distress with hypoxemia and hypercapnea on ABG. At this point you should: A. Immediately re-intubate her B. Apply NIMV via BiPAP C. Apply NIMV via CPAP D. Re-intubate and perform Tracheostomy E. Apply high flow nasal cannula oxygen
NIMV after failing extubation
• Randomized single center controlled study1
– Ineffective in preventing re-intubation once
respiratory failure has occurred
• Randomized multicenter controlled2
– Rate of death higher in NIMV group
– Less than 10% of patients had COPD
1) Keenan et al JAMA 2002;287:3238-44
2) Esteban et al NEJM 2004; 350:2452-60Weaning Adjunct in COPD
• Failed SBT T-piece (50Pts)
• IMV vs. NIPPV
• Decreased days on Vent 16 vs. 10
• Decreased ICU LOS 24 vs. 15
• Survival @ 60 days 92% vs. 72% (p=0.009)
• VAP 7 vs. 0 (4 fatal pneumonia)
Nava et al Ann Int Med 1998;128:721-28NIMV post extubation in hypercapnic patients with chronic
respiratory disorders: randomized controlled trial.
Lancet. 2009 Sep 26;374(9695):1082-8
• Background
– Previous studies have been inconclusive on the benefit
of NIMV post extubation
• Methods
– 106 patients in 3 ICU’s with Chronic respiratory failure
– Passed SBT but had elevated CO2 on ABG
– Randomized to NIMV for 24 hours or O2 therapyNIMV adjunct to extubation
Lancet 2009 Sep 26;374(9695):1082-8
• Results
– 70% patients had COPD
– Decreased post-extubation respiratory failure
• ARR =33%, NNT= 3 OR 5.32 (2.1 to 13.5)
– Reduced 90-day mortality
• ARR=20% NNT= 5
• Conclusion
– Pre-emptive use of NIMV rather than rescue use is
recommended when patients with chronic lung disease
develop hypercapnea during SBTHFNC and NIMV Review • MV may worsen outcomes due to COVID-19 ARDS • High Flow Nasal Cannula & NIMV may avoid intubation in COVID-19 respiratory failure and lead to improved outcomes and preservation of ventilators in a pandemic • NIMV can be an adjunct to extubating patients but not a rescue modality.
Appendix
Lung Protective Strategy • ARDSnet Recommendation • Tidal Volumes 5-6cc/Kg ideal body weight – Goal Plateau pressure 7.25 (not to pCO2) allow permissive hypercapnia • Titrate PEEP/FiO2 to PaO2>55mmHg or SpO2 88-95%
How to Reproduce the Success of
the Trials
• Patient selection
• Equipment
• Familiarity with NIMV
– Nursing, respiratory therapist, physicians
• Commitment to NIMVPractical Points • Use PSV beginning with low settings (5cm H2O/3 PEEP) & most sensitive trigger • Titrate pressure to patient comfort (decrease RR, adequate TV) • Titrate PEEP to trigger effort and sats (4-8) • Start with holding mask to patient; remove mask to allow patient to sense the effort • Make adjustments – Correct mask leaks • Continue to coach and reassure Pts
Practical Points • Inspiratory pressure – Respiratory muscle unloading – Minute ventilation (PaCO2) • Expiratory Pressure – Trigger effort (auto-peep) – Oxygenation – Upper airway obstruction (OSA)
“Best way to reduce VILI is to never
put them on the ventilator”
▪ Early recommendations from Europe were to intubate early to close circuit,
protect healthcare workers
▪ Significant complications from Mechanical Ventilation
▪ Difficult to sedate
▪ Paralytic requirement results in prolonged recovery
▪ VILI Worsening lung compliance over time
• Non-invasive mechanical ventilation and high flow nasal cannula may decrease
MV in COVID respiratory failure.
– Non-intubated prone positioning 1,2
– BiPAP and CPAP
– HFNC (Comfort Flow) 3 1) Elharrar et al JAMA May15,2020.doi10.100
– Accept permissive hypoxemia 2) Ding et al Crit Care 2020;24(1):28
3) Frat et al NEJM 2015;372(23):2185-96You can also read